Today we are showing radiographs of a 61-year-old man who has had several pulmonary infections during recent years.
What do you see? Leave your thoughts in the comments section and come back for the answer on Friday.
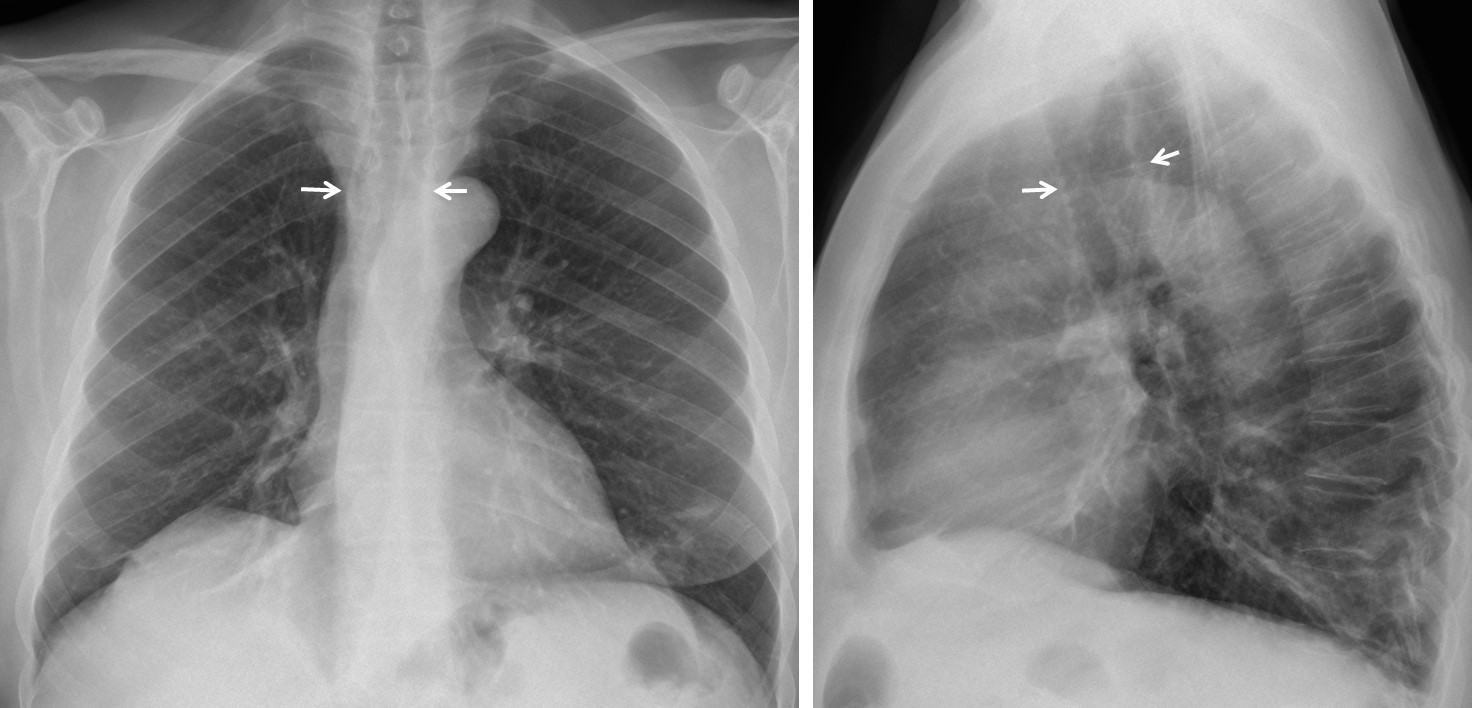
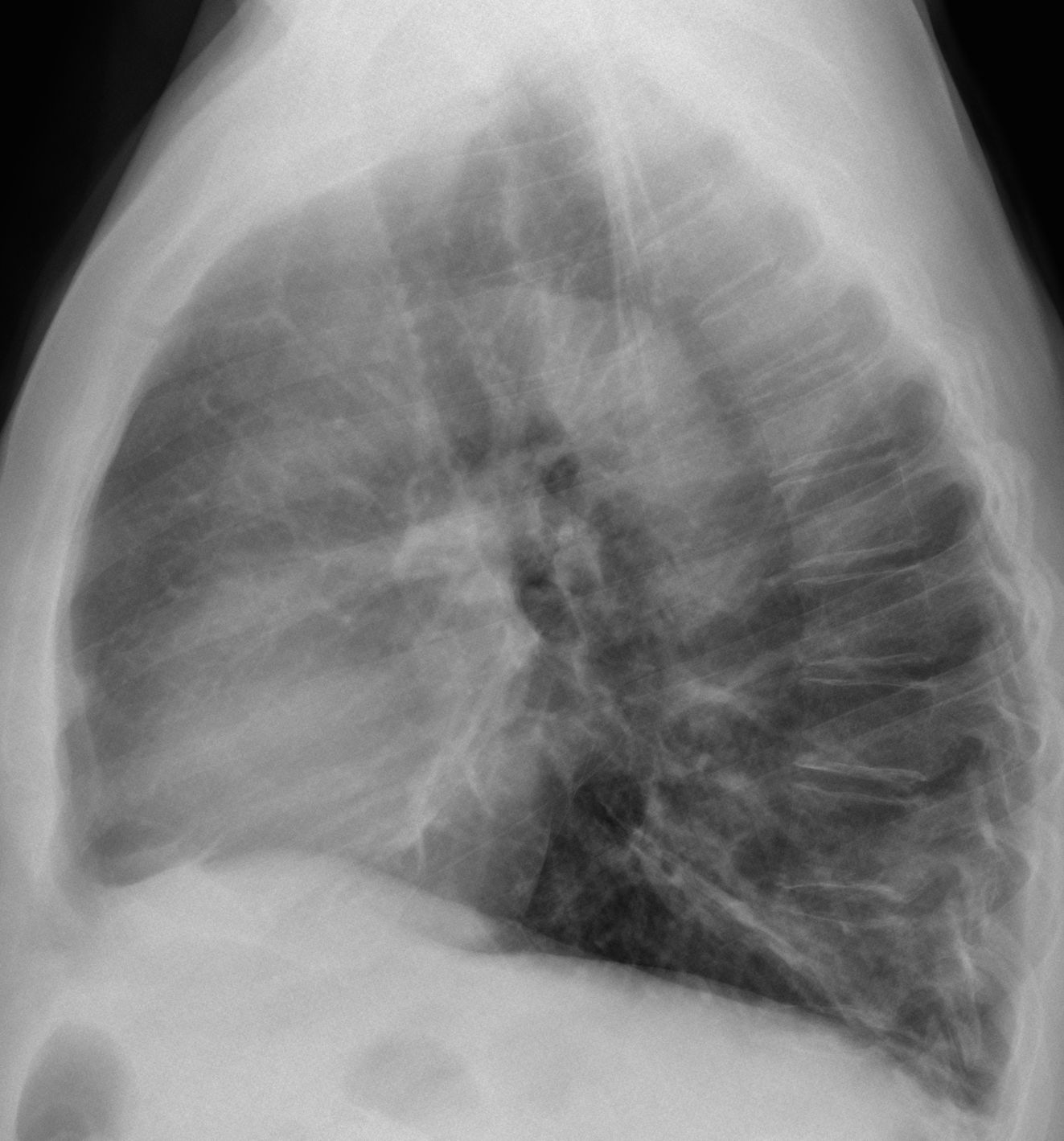
Findings: Chest radiographs show a marked increase of the tracheal diameter, both in PA and lateral views (arrows). Lineal infiltrates in both bases are seen, probably secondary to previous infections.
Unenhanced coronal and sagittal CT confirm the findings, showing a corrugated appearance of the tracheal wall and dilatation of the main bronchi. These findings are very characteristic of tracheobronchomegaly.
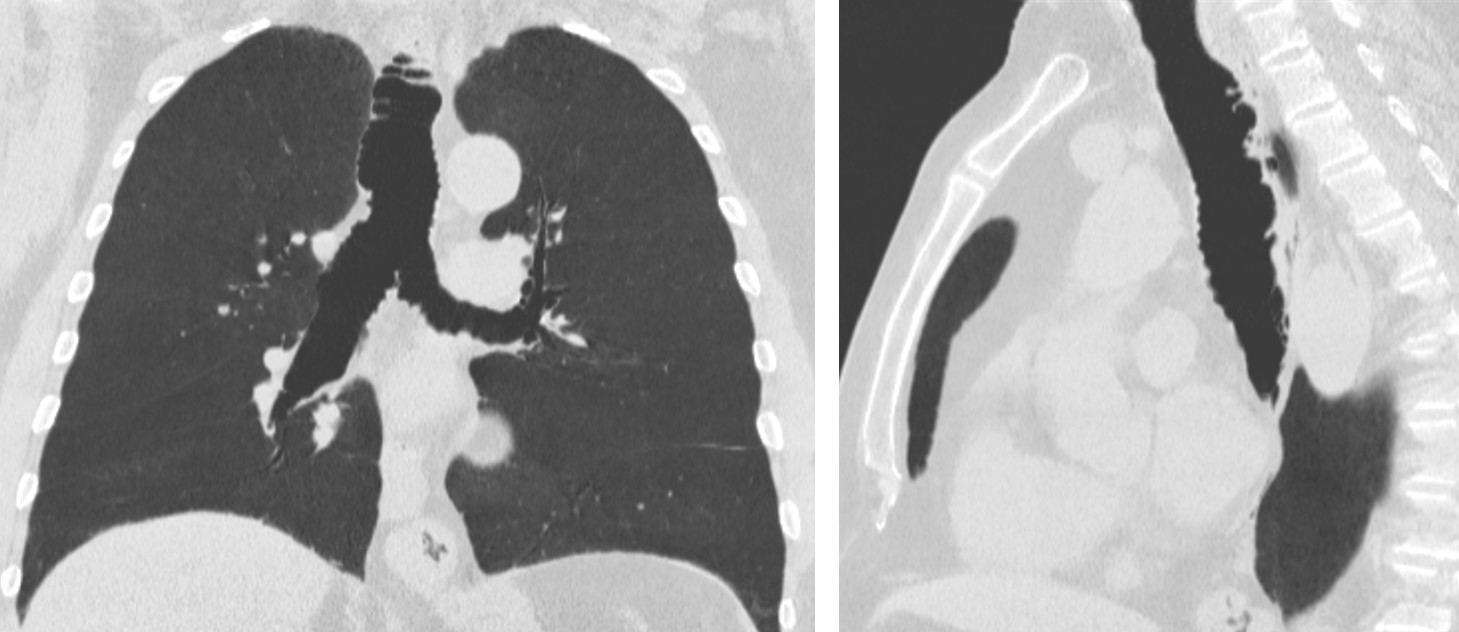
Final diagnosis: tracheobronchomegaly (Mounier-Kuhn syndrome)
Contratulations to Stanko, who was the first to suggest the diagnosis.
Teaching point: remember to look at the trachea when examining a chest film. Important findings can be discovered. Although tracheobronchomegaly is an unusual disease, the present case was seen in October of this year and the diagnosis was suggested in the plain film.



pleural thickening,decreased volume of rt lung, ., mesothelioma should be excluded by CT
Dear Dr Caceres and Dr Pepe, I’ve recently discovered this excellent case demo and discussion. I will just have a go with this…
Bilateral lower lung fibrotic changes as evident with diaphargmatic tenting and peripheral linear opacities.
Also pleural thickening, including calcified portion over the right hemidiaphragm.
There is also slight reduced lung volume.
No focal lung mass.
Normal heart size and cardiomediastinal outline.
Features are of chronic lung changes from asbestosis exposure.
Welcome to our humble abode! Sorry, I don’t agree with you about the diaphragmatic calcification.
I’d say Mounier-Kuhn (elderly man, common infections).
The bronchus and bronchi look enlarged.
one more for Mounier-Kuhn syndrome
Couldn’t agree more
In case you are all right, only the first one gets credit!
It doesn’t matter if you are first….the teaching point is to learn from the mistake.
i hope we are right… please my god!!!! 🙂
I agree with you. Making mistakes is the best path to knowledge.
Atelectasias laminares en ambas bases junto con opacidades nodulares de morfología alargada en campo pulmonar inferior izquierdo, a descartar bronquiectasias (en el contexto clínico referido)
Dilated and corrugated trachea
Central airway bronchomegaly more on left side
Left lower zone branching opacities
Right lower zone opacities
Lateral chest showing posterior basal segment opacities
Suggest Tracheobronchomegaly – Mounier Kuhn syndrome with changes of recurrent infections
??? Posterior displacement of lower portion of major fissure on ? left with diaphragmatic tenting – is there partial collapse Dr. Caceres or Dr.Pepe
Good discussion. No partial collapse was found at CT.
Final answer on Friday.
….carissimo professore, non posso lasciarti!….ci sono delle immagini bronchiectasiche alle basi polmonari con “mucoid-impact”….l’ilo di dx è mal visibile e notevolmente “più basso” del sx anche in LL … mentre l’arco cardiaco inferiore di dx è “anomalo .la tc, venerdì, stabilirà il perche’…..