Muppet is afraid of losing our audience and insists on showing easy cases. Here we are presenting radiographs belonging to a 54-year-old man with skin lesions.
What do you see? Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
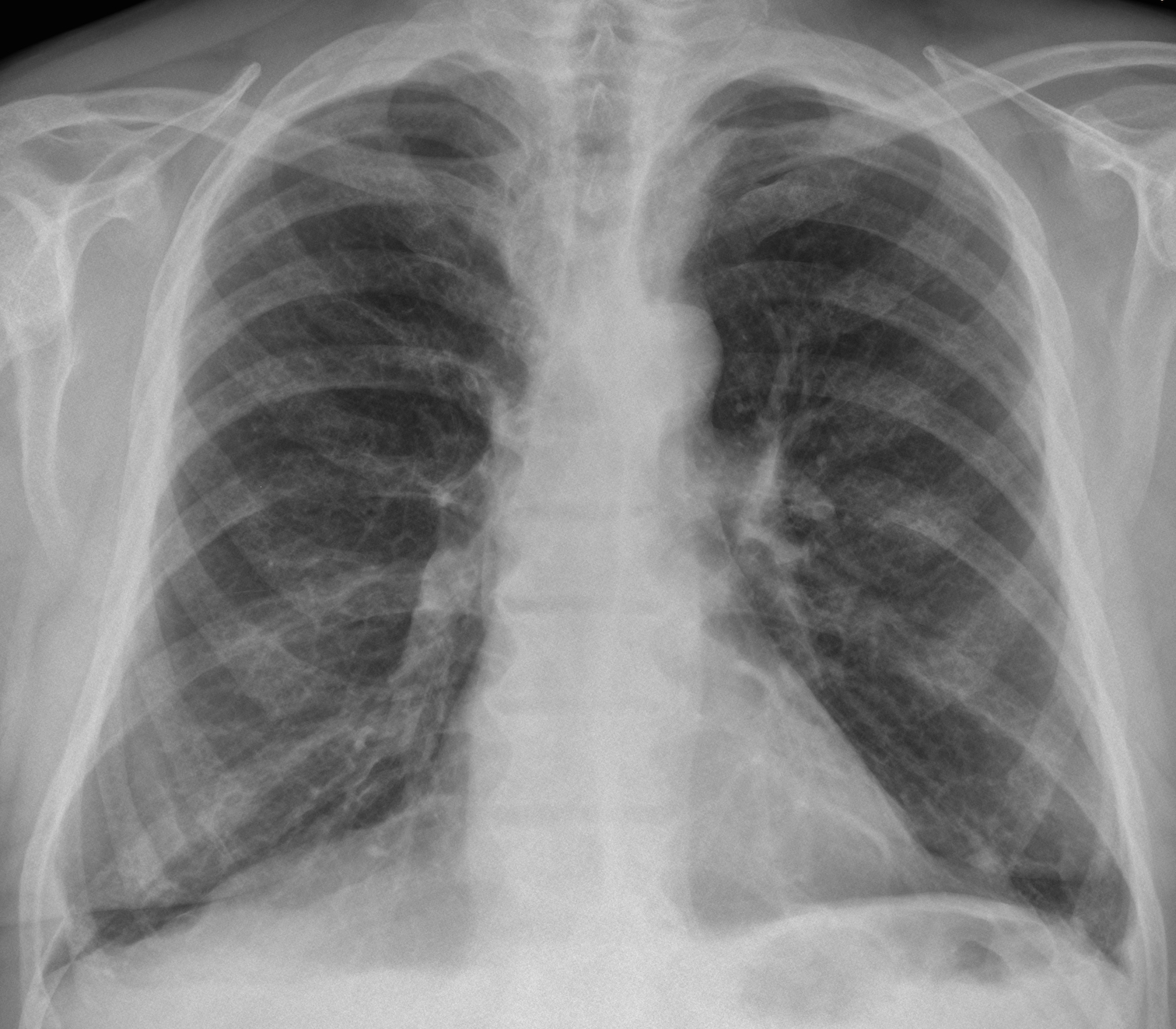
Findings: chest radiographs show a generalised increase in bone density, more obvious in the dorsal spine in the lateral view.
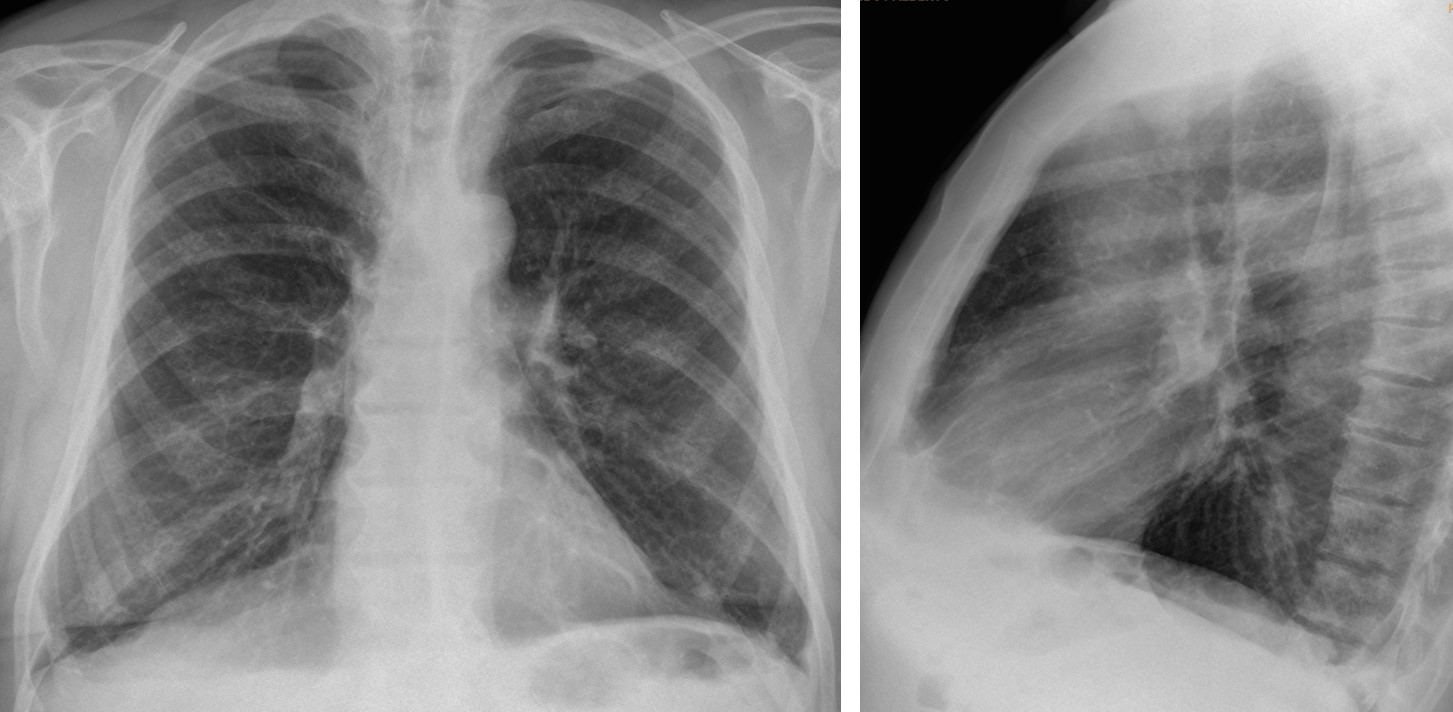
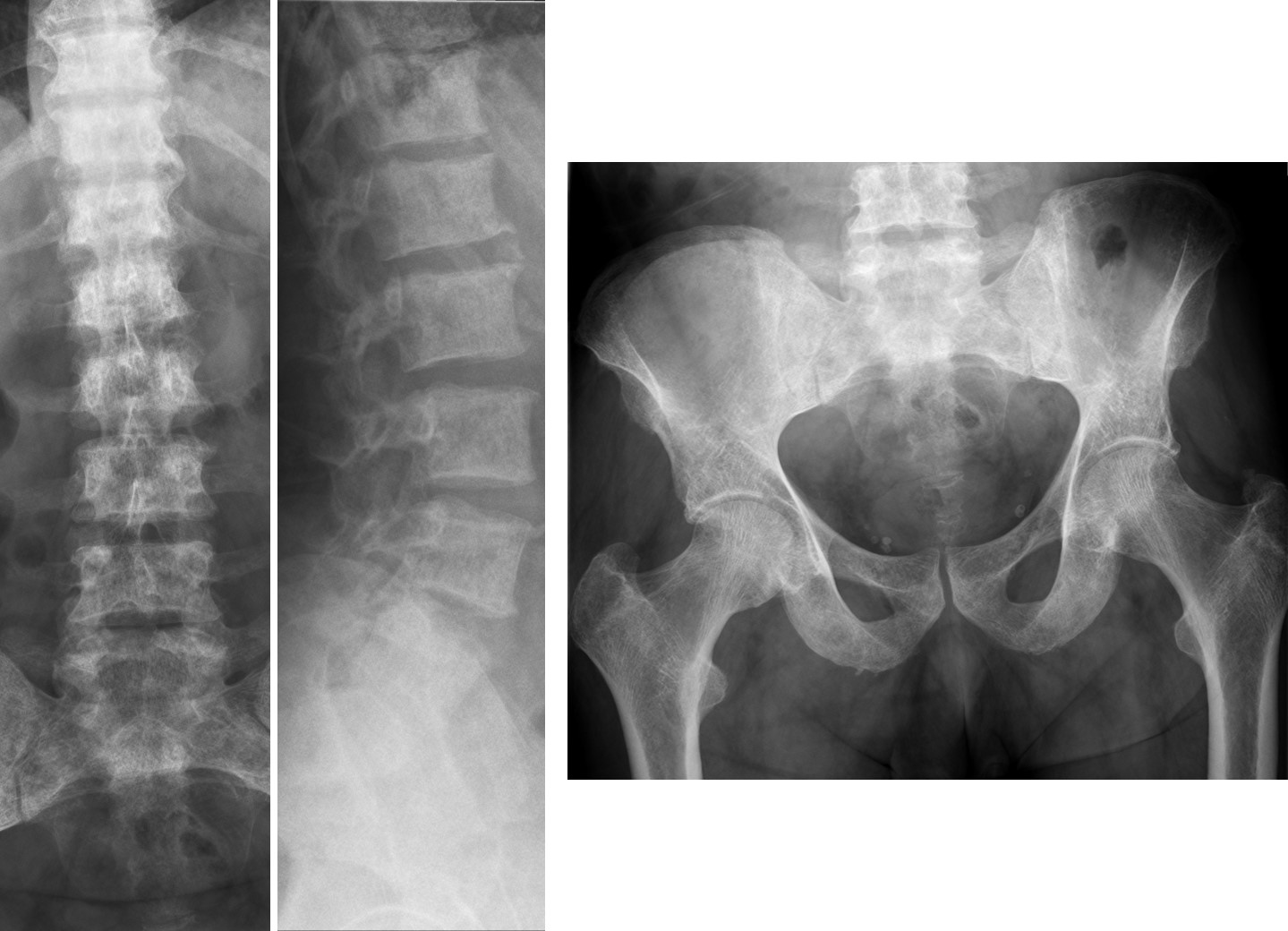
There also unspecific lineal shadows in both lungs. Radiographs of pelvis and lumbar spine confirm the widespread increased bone density.
The most common condition to produce this appearance is renal osteodystrophy, which can be excluded because of normal renal function. A good possibility is myelosclerosis, unlikely because the spleen is not enlarged in the PA film.
Diagnosis was made because the patient had urticarial lesions with pruritus, suggesting the diagnosis or urticaria pigmentosa, confirmed by biopsy.
Final diagnosis: systemic mastocytosis.
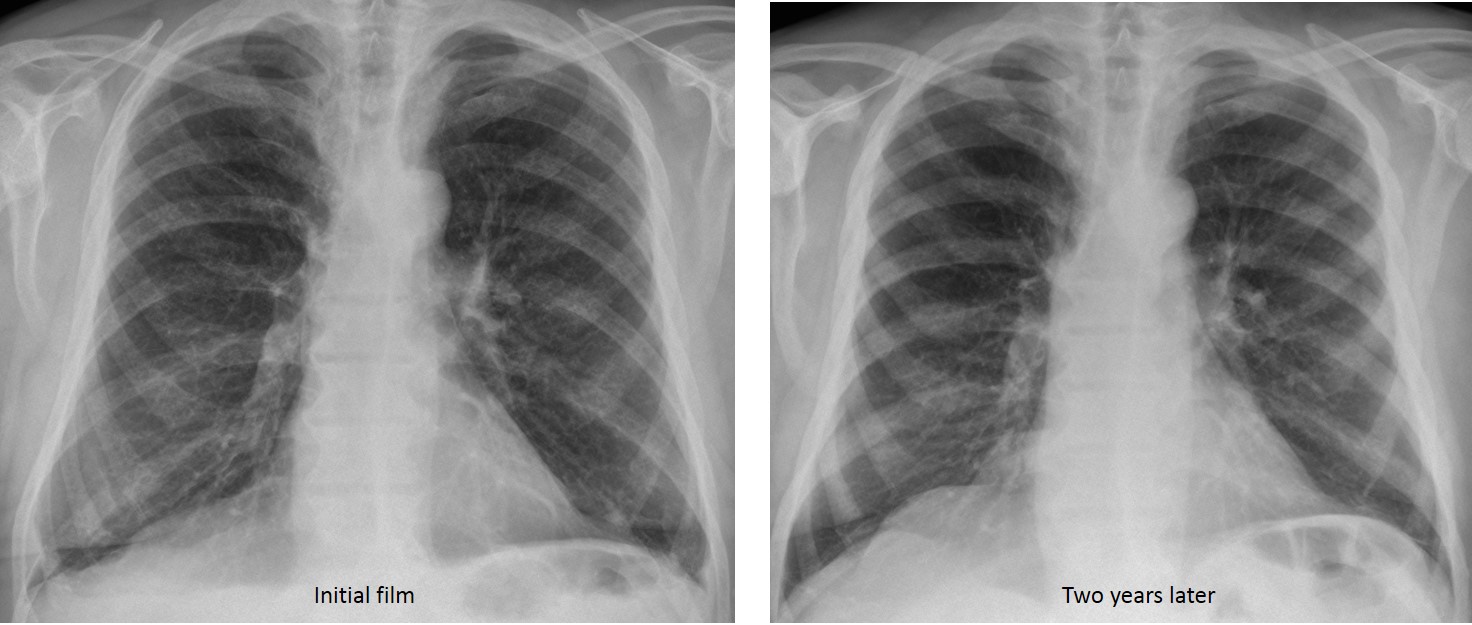
Lung involvement has been described in this condition. I am no expert in mastocytosis and lung biopsy was not done, but there is improvement in the lineal shadows in a PA radiograph taken two years later.
Congratulations to Fernando, who made the correct diagnosis.
Teaching point: radiographs were shown to emphasise that the majority of us don’t look at the chest bones and may miss important diseases, as proved by this case.



Interstitial opacities, increased lung volume, skin lesions and an easy case – could it be NF1?
Don’t believe everything the Muppet says! He is a tricky
fellow.
rugger jersey spine?
Myelofibrosis and cutaneous extramedullary hematopoiesis
Good guess. Is the spleen enlarged?
Langerhans Cell Histiocytosis would explain the interstitial parenchymal changes, the rash and the destruction of the 8th rib on the right side, with my first differential being a tumor with metastasis in the rib and paraneoplastic rash.
Lungs appears “dirty” to me.
Interstitial opacities with reticulo-nodular pattern.
Can’t tell if it’s only due to my monitor: there is permeative pattern in few ribs/verterbra.
and those skin lesions..
Dear proffesor can You provide us with picture of that lesion(s).
My guess:
– Mycosis fungoides or
– HIV (+): kaposi’s sarcoma & Opportunistic pneumonia & lymphoma
Sorry, I don’t have pictures of the skin lesions. But the patient had pruritus
…Churg-Strauss syndrome…?
Increased interstitial markings, especially bibasal + dilated esophagus on lateral view + skin lesions = Scleroderma is the first diagnosis.
Small amount of pleural effusion, egg-shell cacified mediastinal lymph nodes and signs of pulmonary hypertension may be found in cases of scleroderma.
I disagree with you about the dilated esophagus in the lateral view. And the retrotracheal line has a normal thickness.
Did the patient smoke?
No, to my knowledge
Sarcoidosis?
The other hypothesis is Superior vena cava syndrome.
There is widening on the frontal view of the upper mediastinum on the right, and i think there is swelling of the right hilum too.
….io penso che la patologia sia a carico del “contenente ” e non del “contenuto”….i corpi vertebrali sono addensati con sindesmofiti ….e nello spazio intercostale dx tra 7 ed 8 costa si vede una tenue e disomogenea opacità che potrebbe essere a carico delle parti molli della parete, sede della patologia cutanea…..la diagnosi? Psoriasi e rachide di tipo infiammatorio….
Diffuse lytic and sclerotic bony lesions. Mastocitosis.
Finally!