Muppet is very excited because he has seen many interesting cases in the last two months. He has decided to show them during December and January to make me jealous.
The first patient is a 42-year-old woman with a moderate cough, seen on the 19th of November. What would be your diagnosis? Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
Findings: PA film shows a branching shadow in the right lower lung (A, arrow).
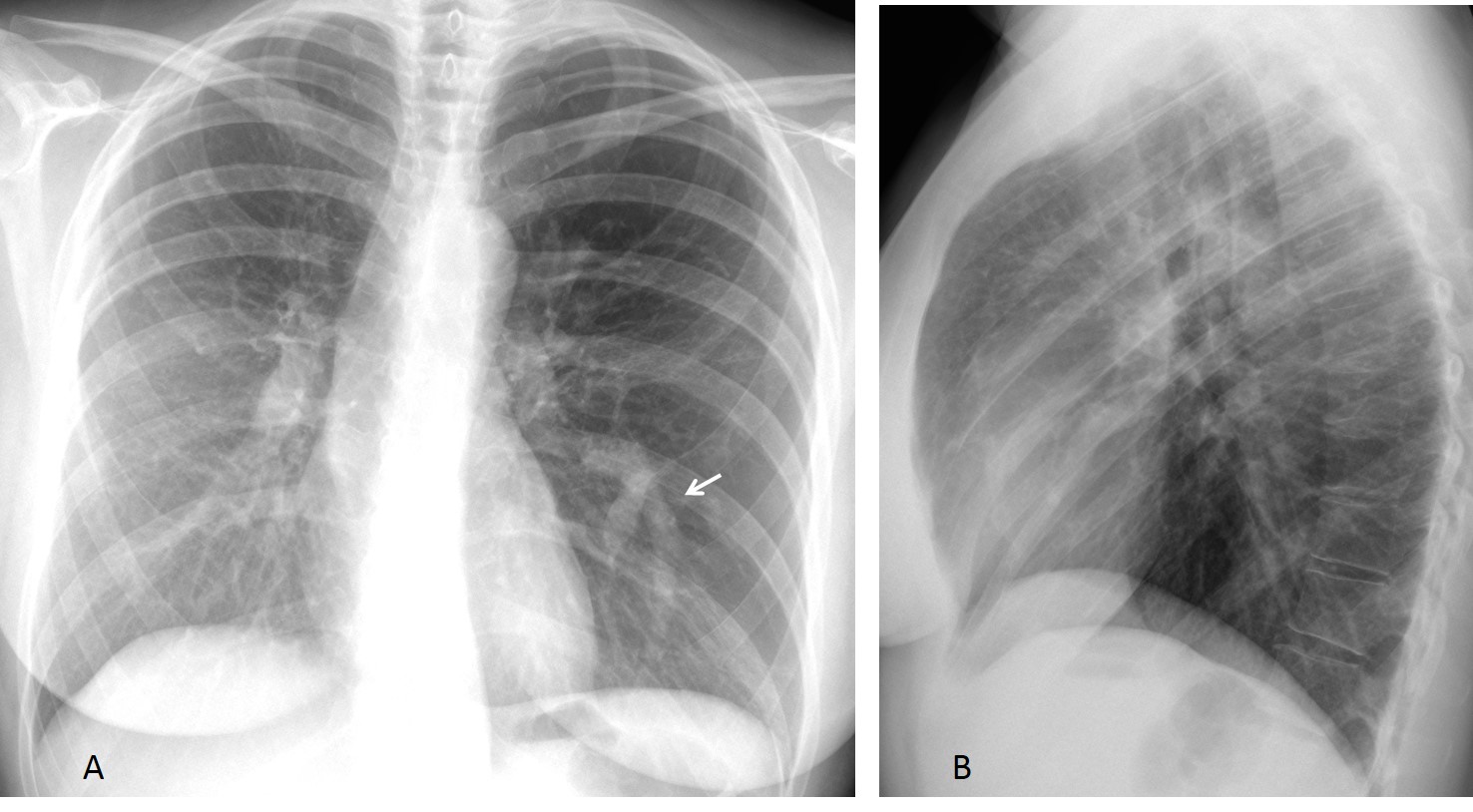
There is also hyperlucency of the left lung with slight mediastinal shift. The combination of hyperlucent lung plus a branching shadow is highly suggestive of mucus impaction and secondary air trapping.
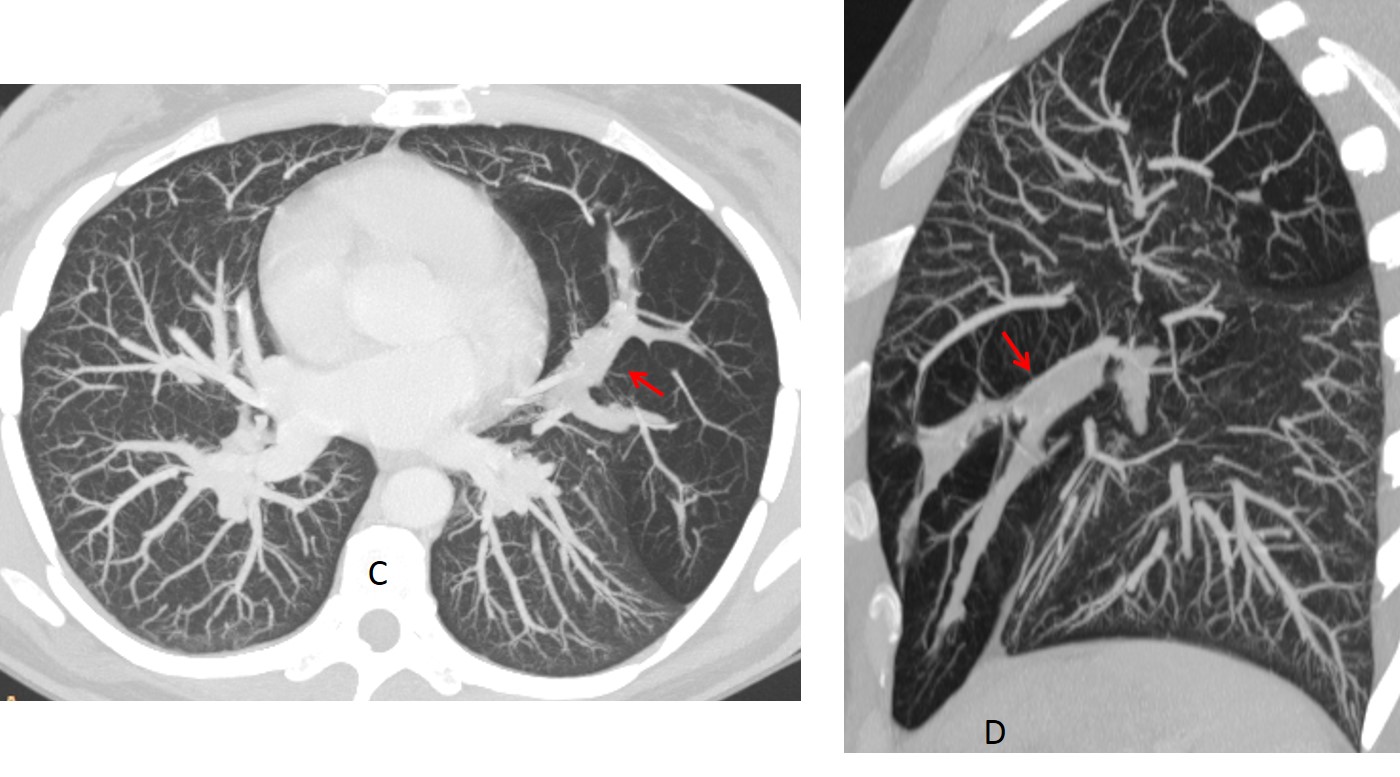
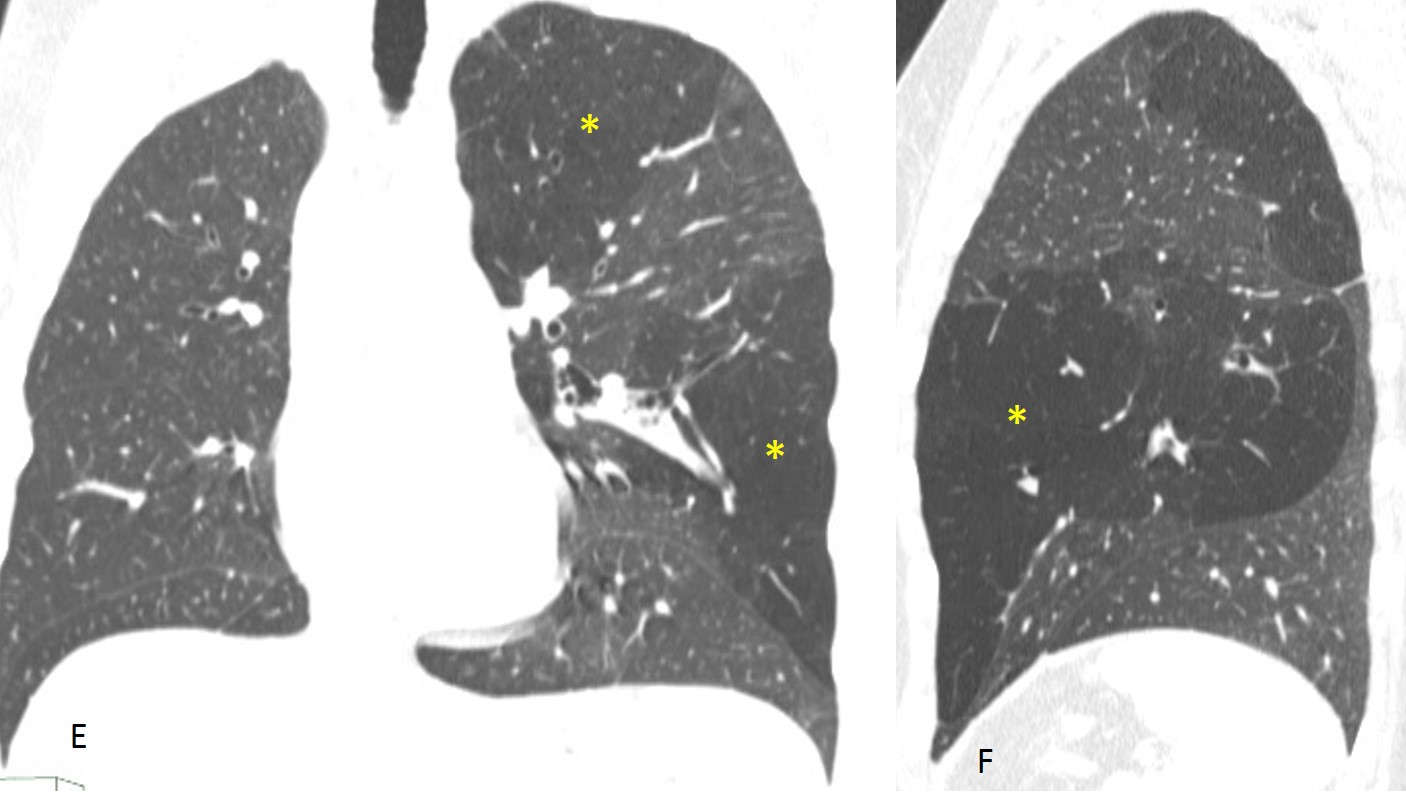
CT confirms the mucus plug (C,D arrows) and the hyperlucency involving the whole left upper lobe, including the lingula (E,F asterisks).
For those of you that diagnosed AVM, remember that this malformation is not accompanied by lung changes.
Final diagnosis: congenital bronchial atresia.
Congratulations to Fernando, who made the right diagnosis
Teaching point: focal hyperlucent lung and mucus impaction are very suggestive of bronchial atresia. In my experience, it one of the most common congenital malformations in the adult. I saw this case only three weeks ago.



Will give it a go…
Radiopacity over left mid-lower zone with branching pattern, giving finger-in-glove appearance.
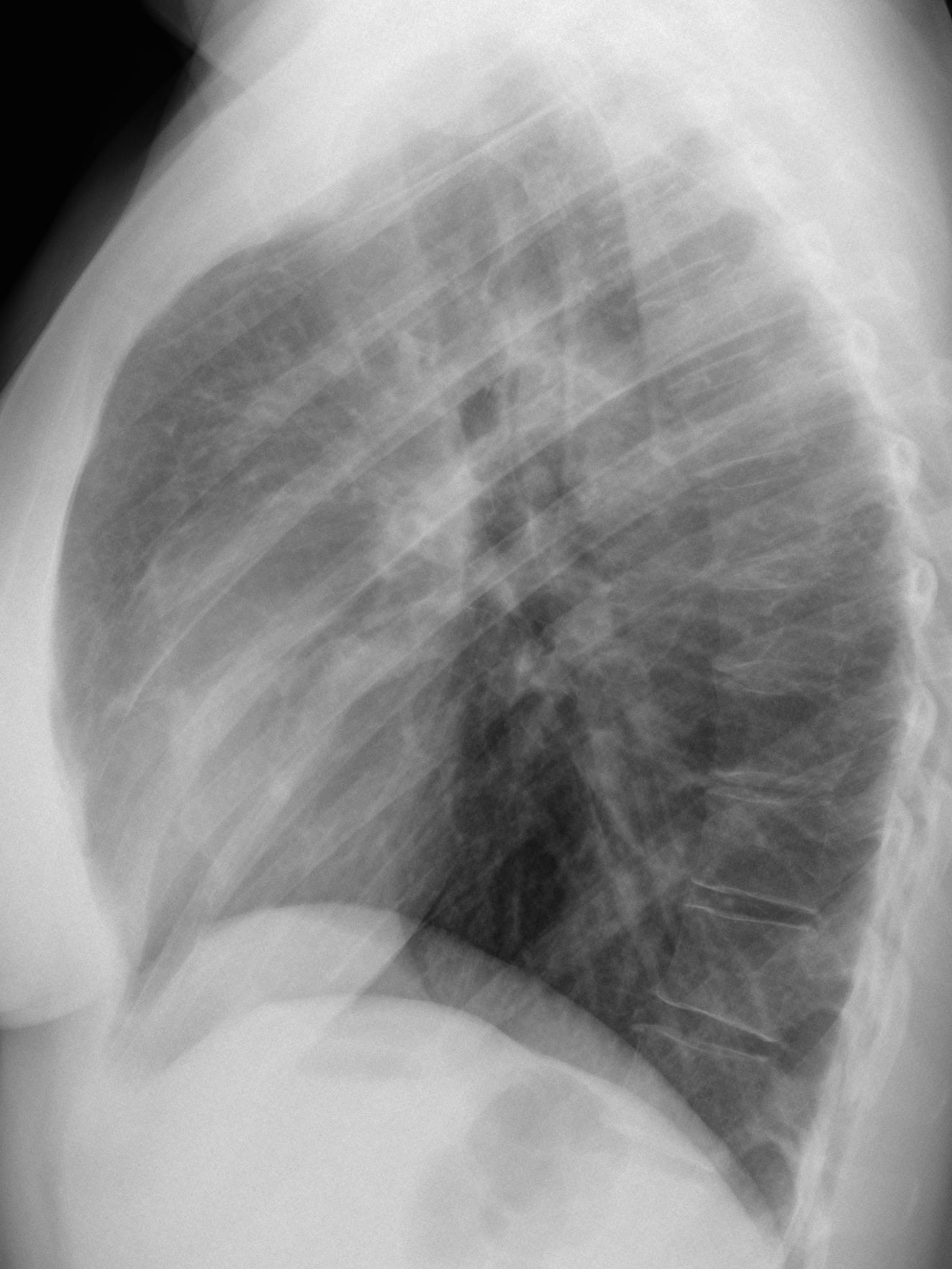
In association with hyperinflated left hemithorax, contralateral mediastinal deviation and barrel-chest configuration as appreciated on the lateral projection.
Features are suggestive for a patient with underlying chronic lung disease such as asthma, complicated by ABPA. Other causes of bronchocele to be considered. CT for further evaluation is advised.
DDX:
-mucoid impaction (several reasons)
– arterio-venous malformation
-air- filled pulmonary sequestration
And the winner is?
Arterio-venous malformation
Y-shaped tubular opacity and distal vascular amputation. Bronchial atresia.
avm ?
Tubular opacity seen in left lower lung zone with extension to the left hilum mostly representing an arterio-venous malformation.
scimitar syndrome?
From a practical point of view, scimitar syndrome accurs nearly always on the right side.
There is double lined tubular opacity within left mid lung zone downwards … Mild hyperinflation of left lung field … For HRCT chest
DD: – bronchial impaction
– asthma or avm
Bronchial atresia
…sarà l’angio-tc , con le ricostruzioni in VR a definire l’anomalia “vascolare” che non mi sembra tuttavia una MAV….l’ilo vascolare di sx è ” tronco” e sembra continuarsi distalmente con l’immagine rx-opaca ad y invertita….mi sembra inoltre di osservare una povertà della trama vascolare a sx….penso pertanto ad una anomalia dell’arteria polmonare sx( atresia), con iperplasia vascolare del circolo di compenso sottostante….
lingular avm
….l’opacità a dito di guanto è indicativa di “mucoid.impact” da ostruzione…..la causa della ostruzione può essere congenita(atresia bronchiale) od acquisita( Tumore,TBC,Asma,aspergillosi…)
Better late than never!
Merry Christmas
Feliz Navidad ….da S. Domingo !!!!!Grazie PROFESSORE !!!!!
left lower lobe bronchial atresia with compenssatory upper lobar inflation;
differential may be mucoid impaction