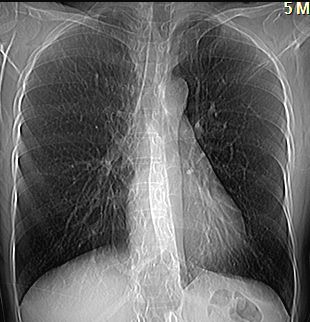
Today we are showing PA radiographs of a 55-year-old woman, asymptomatic. The image presented is a reconstruction of a CT examination (no radiograph available). Muppet believes it is worth showing because it is an unusual disease and has teaching value. What do you see?
Check the image below, leave your thoughts in the comments section and come back on Friday for the answer.
Findings: the AP chest reconstruction shows a tubular structure in the right lower lung (A,B arrows), which suggests a blood vessel. The first possibility that comes to mind is a scimitar vein, although there are no signs of pulmonary hypoplasia, a common finding in scimitar syndrome.
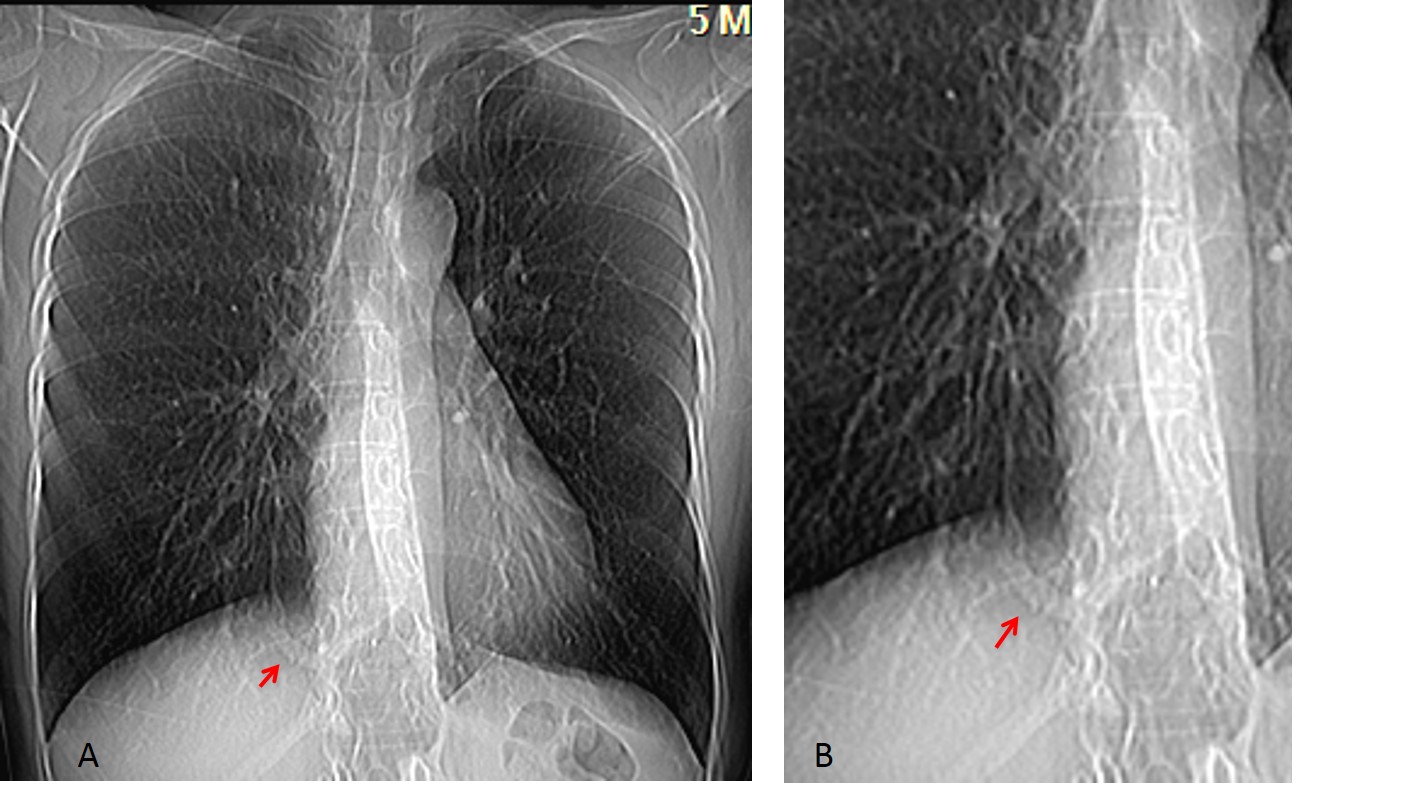
CT shows that the abnormal vessel is an artery arising from the descending aorta (C,D arrows). With lung window, no abnormalities are seen in the RLL; calcium is seen in the wall of the artery (E, arrow).
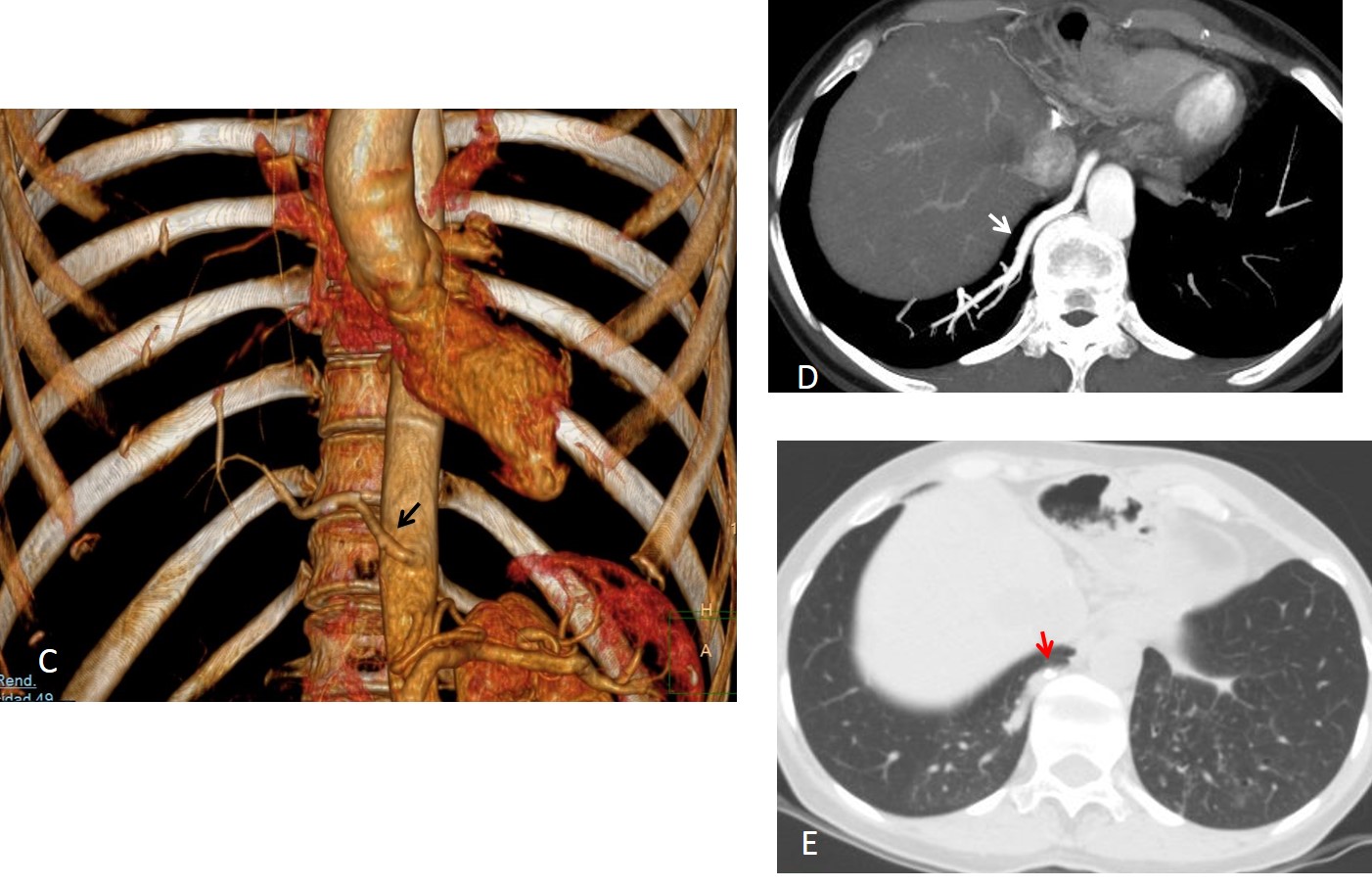
Final diagnosis: isolated systemic supply to normal lung (pseudo sequestration)
Congratulations to Aleksander Marin, who was the first to see the abnormal vessels.
Teaching point: pseudo sequestration is a rare disease and I just wanted to show you a new case, seen a few weeks ago. We published two cases many years ago and an interesting fact is that the abnormal artery is seen most of the time in the plain film.


Pectus excavatum
The oesophagus appears diffusely dense?
Also the position of gas in the stomach is displaced higher and to the midline is unusual.
The fact she is asymptomatic makes me consider this has to be something chronic.
Or is there something in her history for a CT scan.
Calcified wall of lower thirds of the oesophagus. Considerations: Leomioma, old intramural hepatoma of the oesophagus.
Would love to see the CT images.
Will show the CT on Friday. The esophagus is OK. Look carefully.
Thank you. There is a smal vessel like structure in the medial right lung base. Scimitar syndrome?
Hmmm…oesophagus showing stent outline…could be post malignancy stricture oesophagus
Middle and lower third of oesophagus is dilated with irregular narrowing at the esophageal-cardiac junction. I would go with scleroderma .
Figure of 7 ribs, heart slightly diaplaced to left allowing on mild rotated hest position. This is pectus excavatum.
Lining of oesophagus probably due to oral contrast ingestion on CT table, the distal part at relaxation phase. No lung changes to supposrt acleroderma.
???
Do not waste your time with the esophagus. remember this is a reconstruction of a CT examination.
Look carefully. The abnormality is visible.
Left hemithorax is hyperlucent. Poland syndrome maybe?
No. Sorry
is a women? no trace of breasts…
ther is increased broncho vascular marking viz. on rt side,if im not wrong ther is either central line or pt is intubated n tube is in rt bronchus…increase B-V marking suggest either br.asthma or pul. edema…
hiatal hernia
Nice to see your face. Sorry, wrong diagnosis
Midline stomach. Could it be some kind of situs ambiguous?
Lt hemidiaphragm
I see a vessel like structure behind the medial right hemidiaphragm – Scimitar syndrome?
I think left sterno clavivular joint or internal end of lt clavicle is abnormal ,mybe stefnoclavicular syndrom,,,
Small caliber pulmonary vessels, especially right-sided…curved tubular opacity in the base of the lung on the right, would agree to what Aleksander proposes…suggestive of Scimitar.
swyer james syndrome?
11th rib absence?
the left sternoclavicular joint its ok?
Is it change of left clavicule near sternum? Variant of anatomy?
….pazza, pazza, pazza idea……migrazione endotoracica di una protesi endovascolare dall’ aorta addominale…..ottimo BARCA!!!!!!
Yes it is a crazy idea. Look at the answer by Aleksander
Scimitar sy.
Bilateral hyperluce lungs barrell chest .?COPD
Scimitar !
…l’anomalia potrebbe essere la congenita occlusione delle due vene polmonari: esse non sono rappresentate ed al loro posto ci sono sottili diramazioni vascolari, che rappresentano il circolo collaterale di scarico….
could that be an intrathoracic rib?
It could be but it is pointing the wrong way
Fracture of acromial part of the right clavicula.
Alexander Marin is very smart. The more you know, the more you know 🙂
Prof. thanks for the case, can’t wait to see CT!