Today we are showing radiographs of a 34-year-old man with malaise and chest pain.
What do you see?
Check the images below, leave us your thoughts in the comments section, and come back on Friday for the answer.
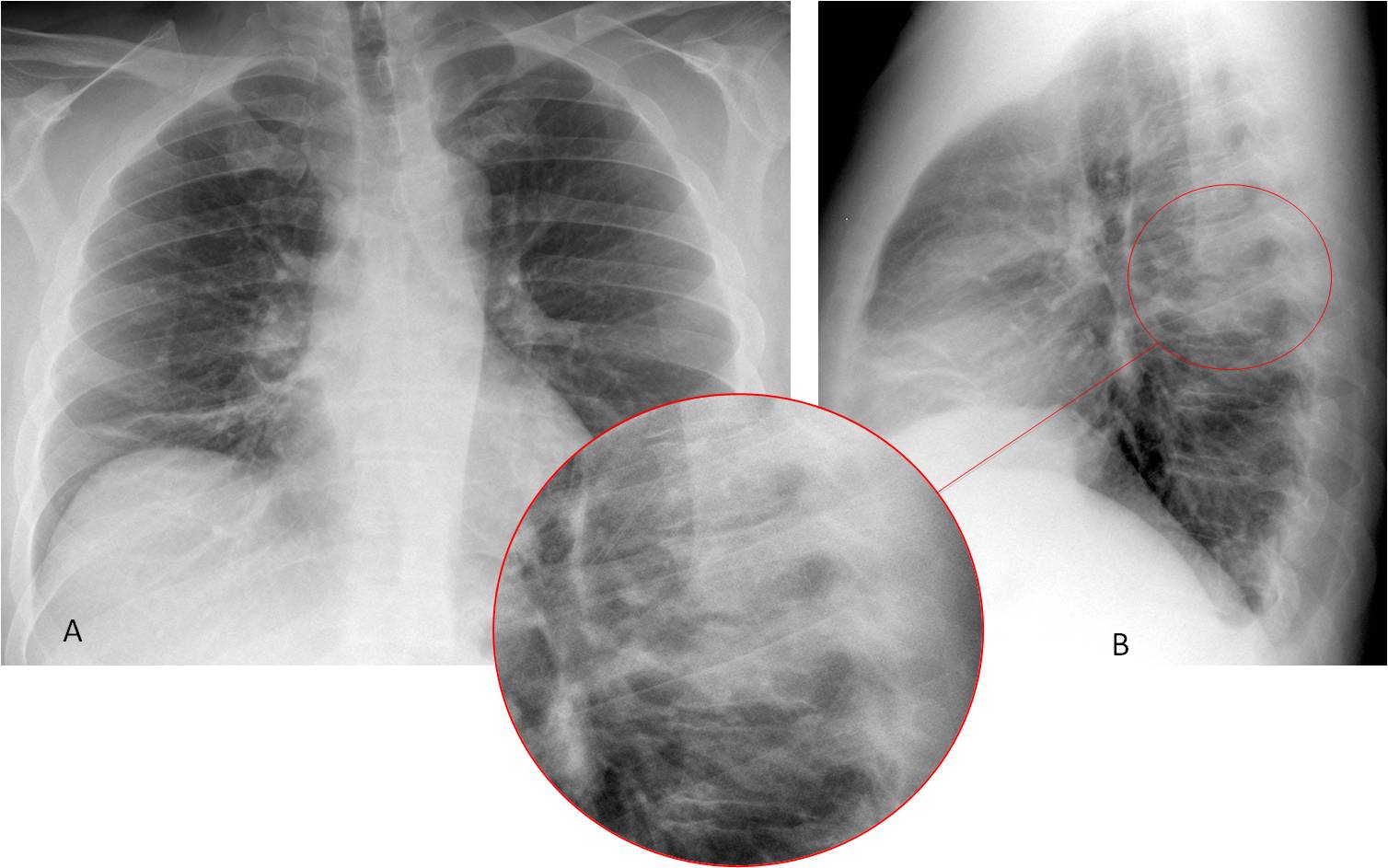
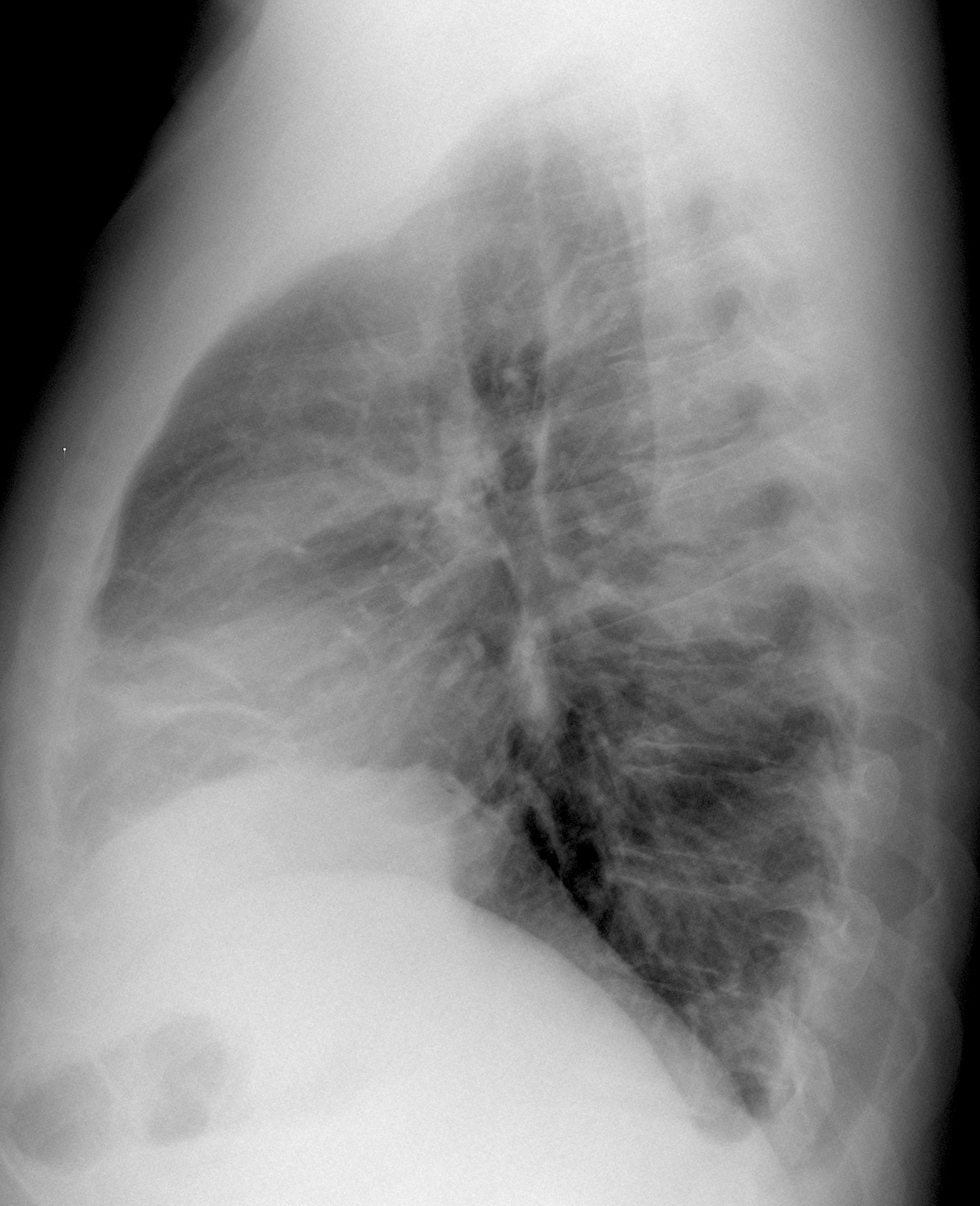
Findings: PA radiograph (A) shows plate-like atelectasis at the right lung base. The right hilum seems increased in density, but it is normal on the lateral projection. The main findings are seen in the lateral view, where the T6-T7 vertebral bodies are more opaque than the ones above or below (B, circle). On close inspection, the intervertebral space is ragged and irregular (insert). These findings are highly suspicious of spinal infection.
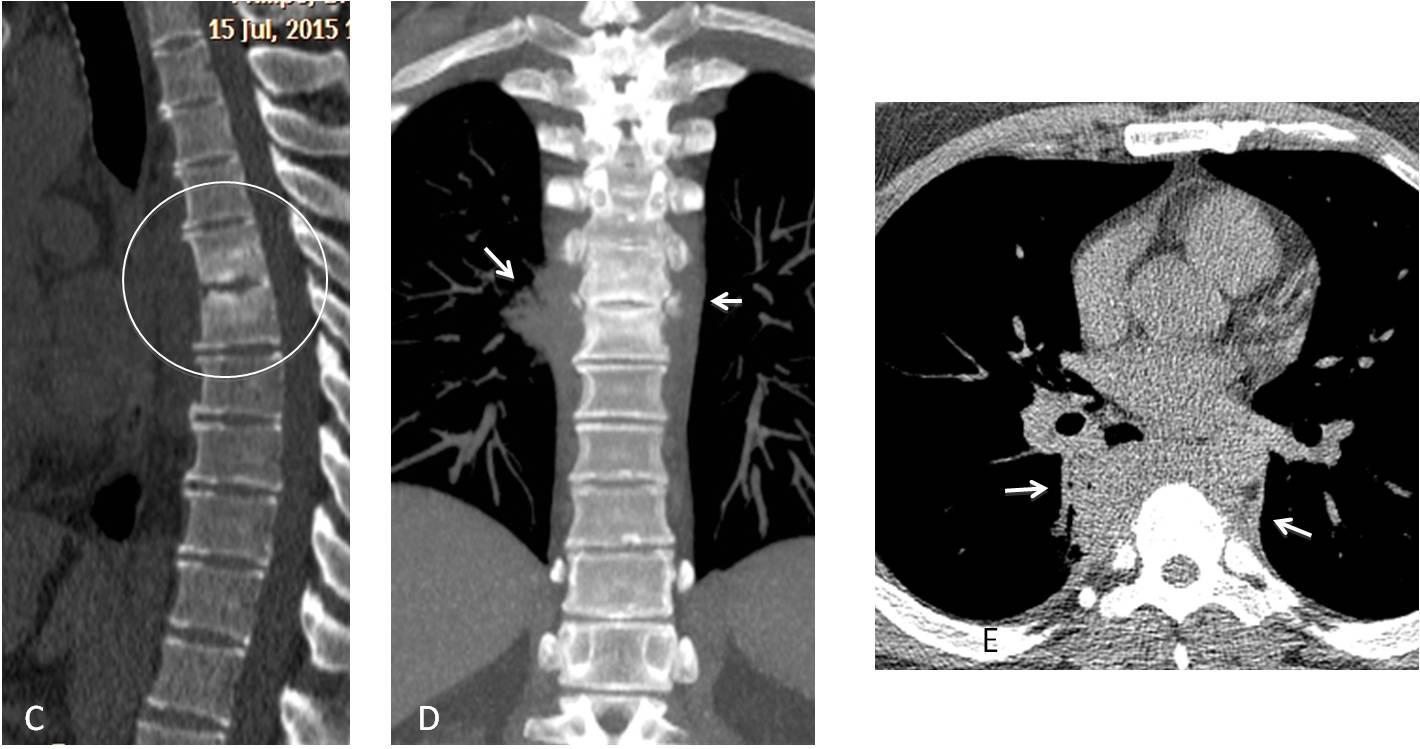
Sagittal CT confirms disk involvement (C, circle). Coronal and axial CT demonstrates swelling of the para-spinal soft tissues (D-E, arrows), which are in part responsible for the increased opacity in the lateral chest radiograph. Biopsy demonstrated inflammatory cells and Staphylococcus aureus grew in the culture.
Final diagnosis: Pyogenic spondylodiscitis of T6-T7
Warm congratulations to Murzin, who made an accurate diagnosis.
Teaching points:
1. Remember the importance of looking at the spine in the lateral view
2. Remember that the spine becomes gradually darker as it reaches the lower thorax because there is more lung air superimposed. Seeing a local increased whiteness is suspicious of spinal disease or superimposed lung pathology. It helped to suggest the diagnosis in this case.



Hello!
opacification of the posterior sinus – pleural effusion. Subsegmental atelectasis.
hello.
On the PA radiograph is regular rounded upper mediastinal mass connected with aortic arch.
I suppose saccular aortic aneurysm.
Also right diaphragm is elevated and small atelectasis plaque is seen in lower part of right lobe.
Later view is unremarkable.
Spondylodiscitis Th6-Th7…
Atelectatic platelet in the right lower pole…
I Think the rounded opacification in the superior mediastinum is caused by sternal manubrium because of patient’s rotation during the exposition…
Subpleural effusion on the right
….sollevamento della cupola diaframmmatica dx, strie disatelettasiche alla base polmonare corrispondente , ilo vascolare non ben rappresentato,….clinica(dolore)….laboratorio( aumento D-Dimeri)….la prima ipotesi diagnostica è tronbo-embolismo polmonare…..
Left pleural effusion and right sub segmental atelectasis. Consider PE when u see left sub segmental atelectasis
Right subpulmonar effusion with partial ML attelectasis
The right hemidiaphragm is elevated and there is a small atelectasis that involves the medial segment of the middle lobe. An hepatic abscess could be the cause, I don’t know if the patient has a fever.
Many different diagnosis. The answer is easy if you remember the basic approach of where to look in the PA view ( hila, apices, trachea, costophrenic angles) and lateral view (anterior and posterior clear spaces, sternum and spine and middle mediastinum)
Right hilum in the PA view( there is an opacity there). Small focal hiperlucency adjacent to the upper part of the right hila.
The right hemidiaphragm is elevated secondary to atelectasis in the right lower lobe.
I see splenic flexure of colon under the left hemidiaphragm.
Sorry, wrong answer
Atelectasis of the ML + right pleural effusion + left pneumothorax
Did you look at the lateral view?
Pneumonia in the posterior clear space.
Getting closer…
Both hemidiaphragms are clearly visible on lateral view , right is higher.RML with athelectatic plates. On lat.view at the level of The Th7 there is an opacification, that on PA view probably represents thickening of right paravertebral line.
opacity in the posterior clear space that extends to diaphragmatic contour.
I stil don’t like the spine so spondylodiscitis but perhaps with reactive fluid in posterior costodiaphragmatic recess on the left?
You did very well. Don’t push your luck. Answer tomorrow.
I hope it wasn’t just about luck…
Thank You for your contribution in teaching. ..
You were the only one making the diagnosis. Should be proud of yourself.