Dear Friends,
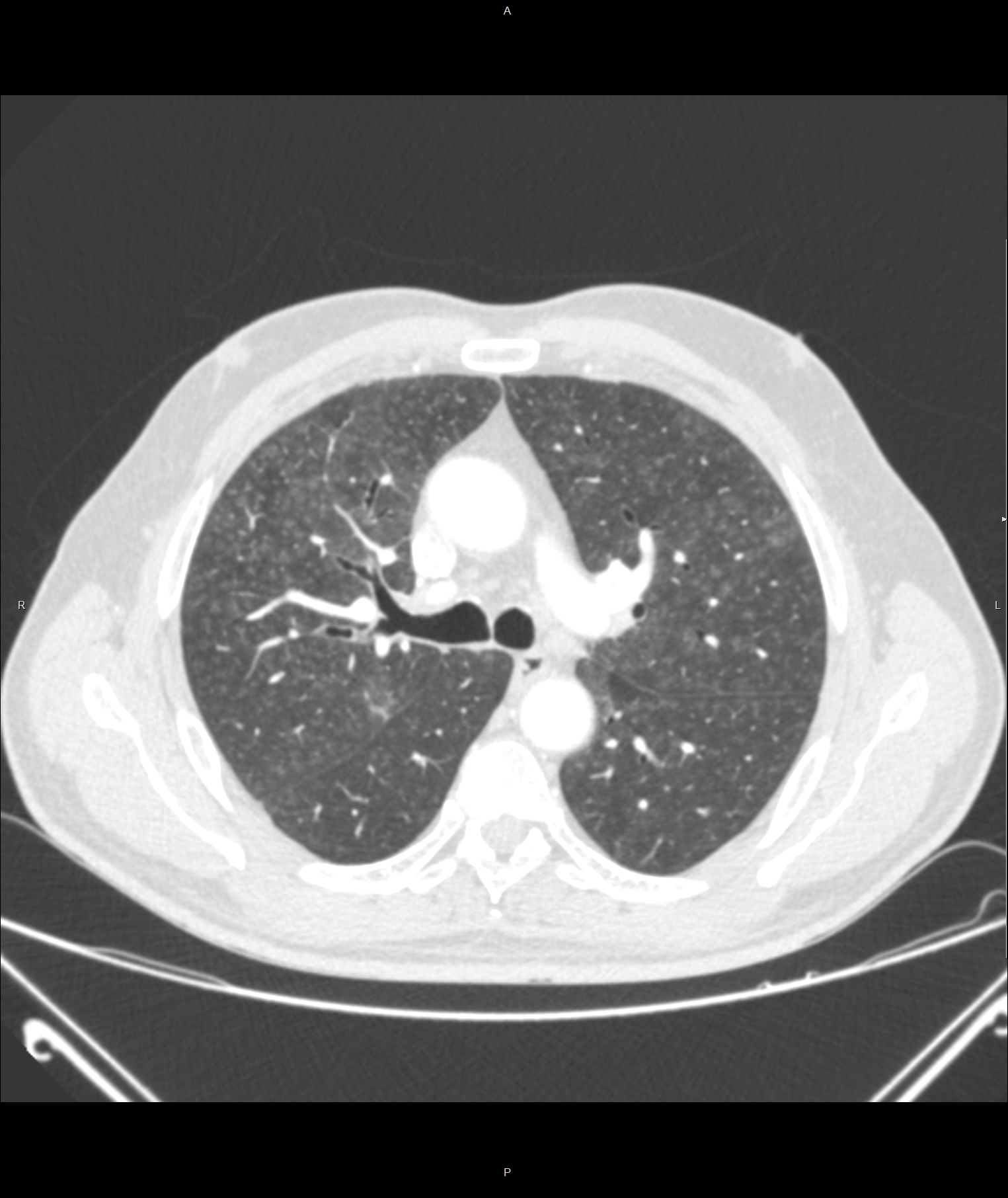
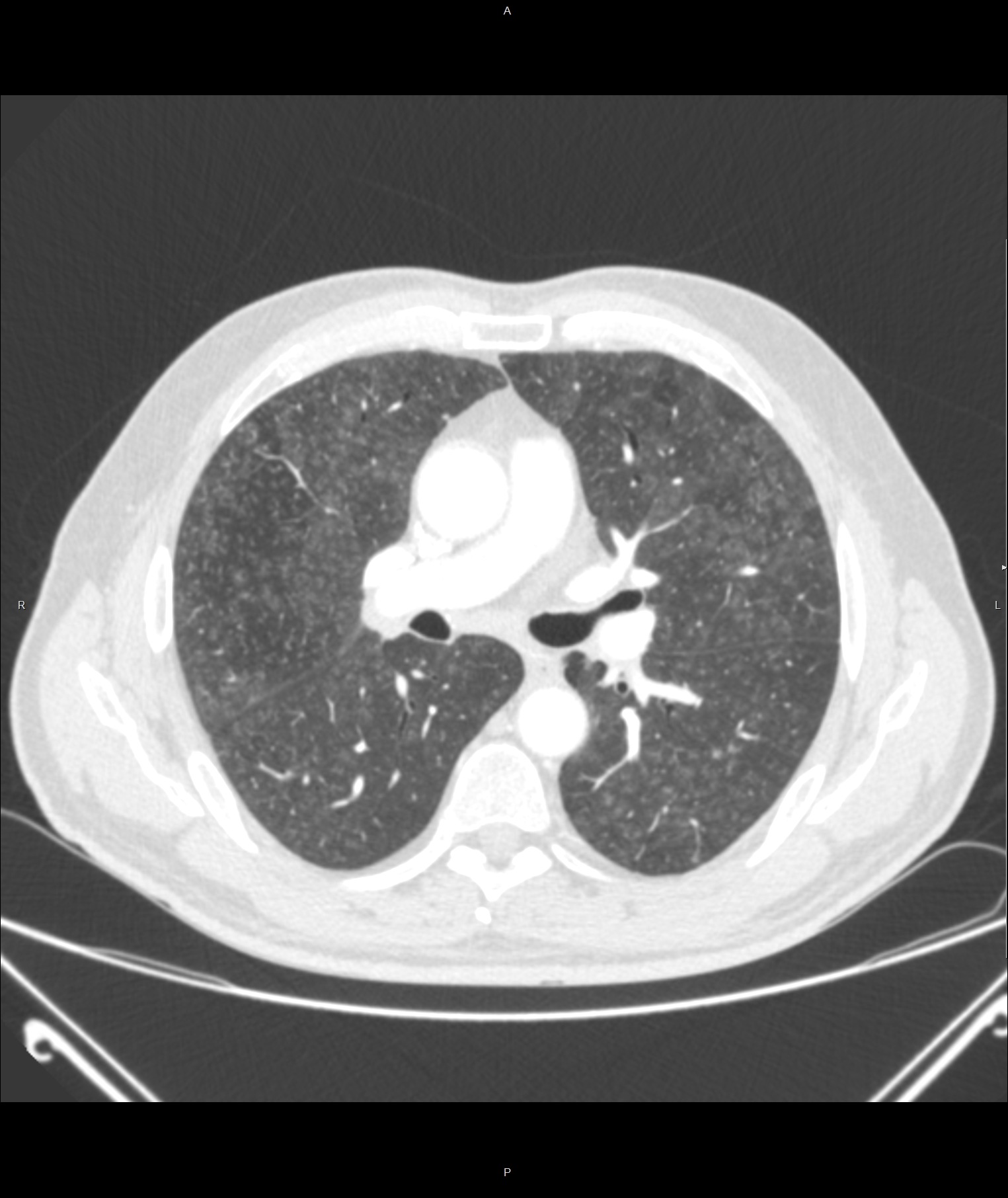
Dr Pepe and I wish you a very happy New Year. To begin 2016 we are showing a warm-up case of a 62-year-old man with cough, dyspnoea and moderate fever of one month duration. Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
Diagnosis:
1. Miliary TB
2. Sarcoid
3. Histoplasmosis
4. None of the above
Click here for the answer to case #127
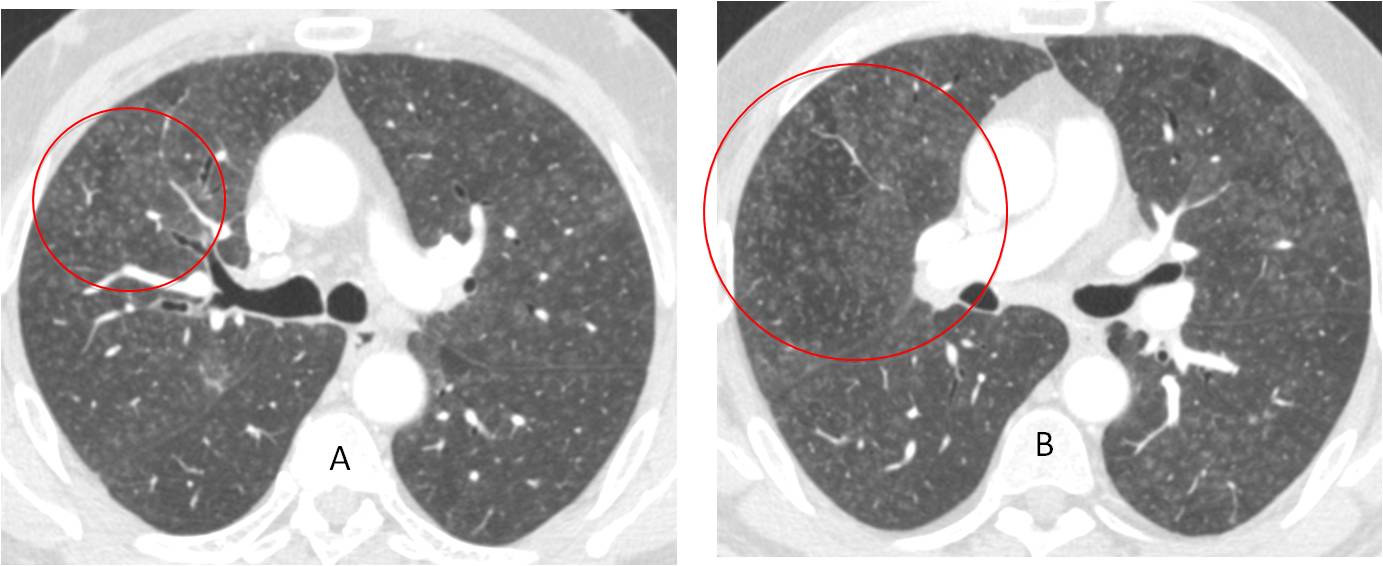
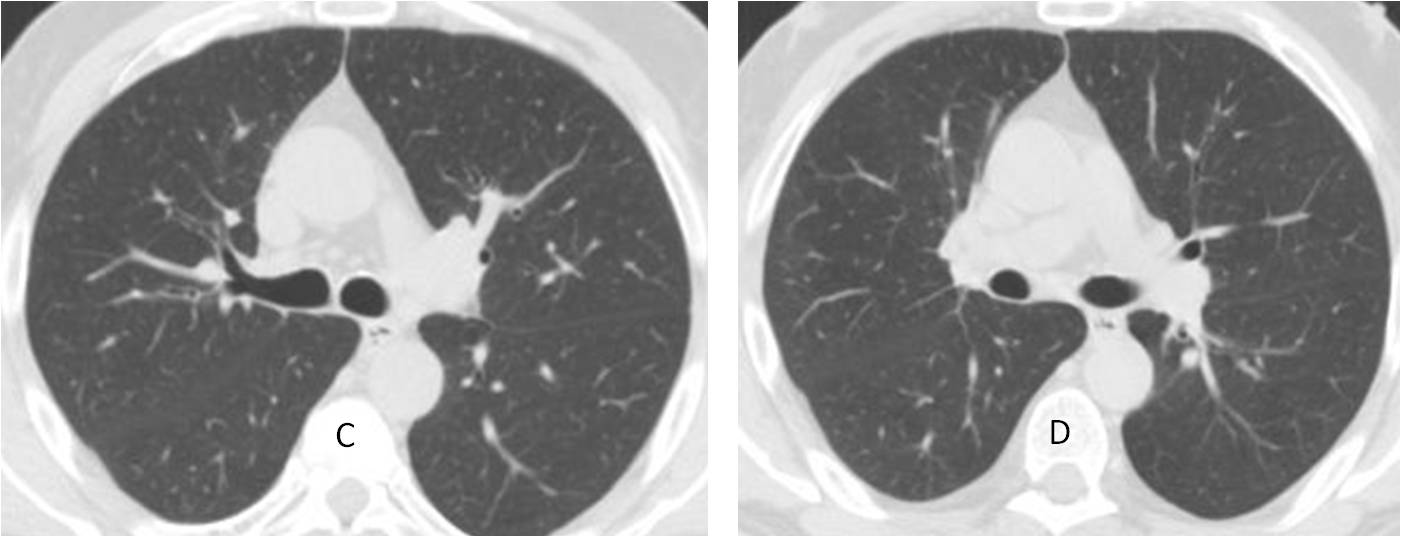
Findings: axial CT shows diffuse centrilobular nodules (A-B, circles) and scattered hyperlucent areas. In the appropriate clinical context, this pattern is highly suggestive of hypersensitivity pneumonitis. Further investigation discovered that the patient owned a Jacuzzi, in which Mycobacterium avium was found. Lung biopsy yielded MAC.
Symptoms disappeared after avoidance of the Jacuzzi and a follow-up CT confirmed the disappearance of the lung changes.
Two months later
Final diagnosis: hot tub lung (hypersensitivity pneumonitis due to MAC).
Congratulations to Pio, Gaborini and Vilma who suggested the right diagnosis
Wanted to show you this case because of the typical CT findings and because it is my first personal case of hot tub lung.
Teaching point: recognising a typical pattern and correlating it with the clinical findings considerably narrows the diagnostic options.


centrilobular pattern of nodules, with ground glass attenuation. I chose number 4, my type is extrinsic alveolitis or maybe RBILD
hypersensitive pneumonitis
I think, none of the above ..
ill-defined nodules in centrilobular distribution, air trapping and diffuse groundglass opacities – hypersensitive pneumonitis.
…patologia diffusa a patter micro nodulare : tali micro noduli sono uniformemente diffusi, ” indifferenti” alla pleura, a non elevata densità’ e margini ” flou” . Non adenopatie ilo- mediastiniche….si esclude pertanto la tbc miliare, la sarcodiosi, le metastasi….non capisco l’istoplasmosi….dovrebbe trattarsi di una LIP( linfocitaria interstiziopatia polmonare)….. Come risponde al cortisone?…..Buon anno , mitico professore !!!!!
4.Faint ill-defined centrilobular nodularity, ground-glass opacities, air trapping, mid/lower zone predominance
Subacute hypersensitivity pneumonitis.
Centrilobular nodules, ground glass opacification, air trapping , no hilar lymphadenopathy -pattern atypical for sarcoidosis. Miliary tb – patient usually in very poor clinical condition. Pulmonary histiocytosis early stage – patient is rather too old. The most probable is hypersensitivity pneumonitis subacute phase. We don’t have any clinical information about exsposition to alergic factors.