Today I am presenting the last case of the season. These images belong to a 47-year-old woman with a chronic cough and mild fever. The pulmonary infiltrate has not changed significantly in the last six months.
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
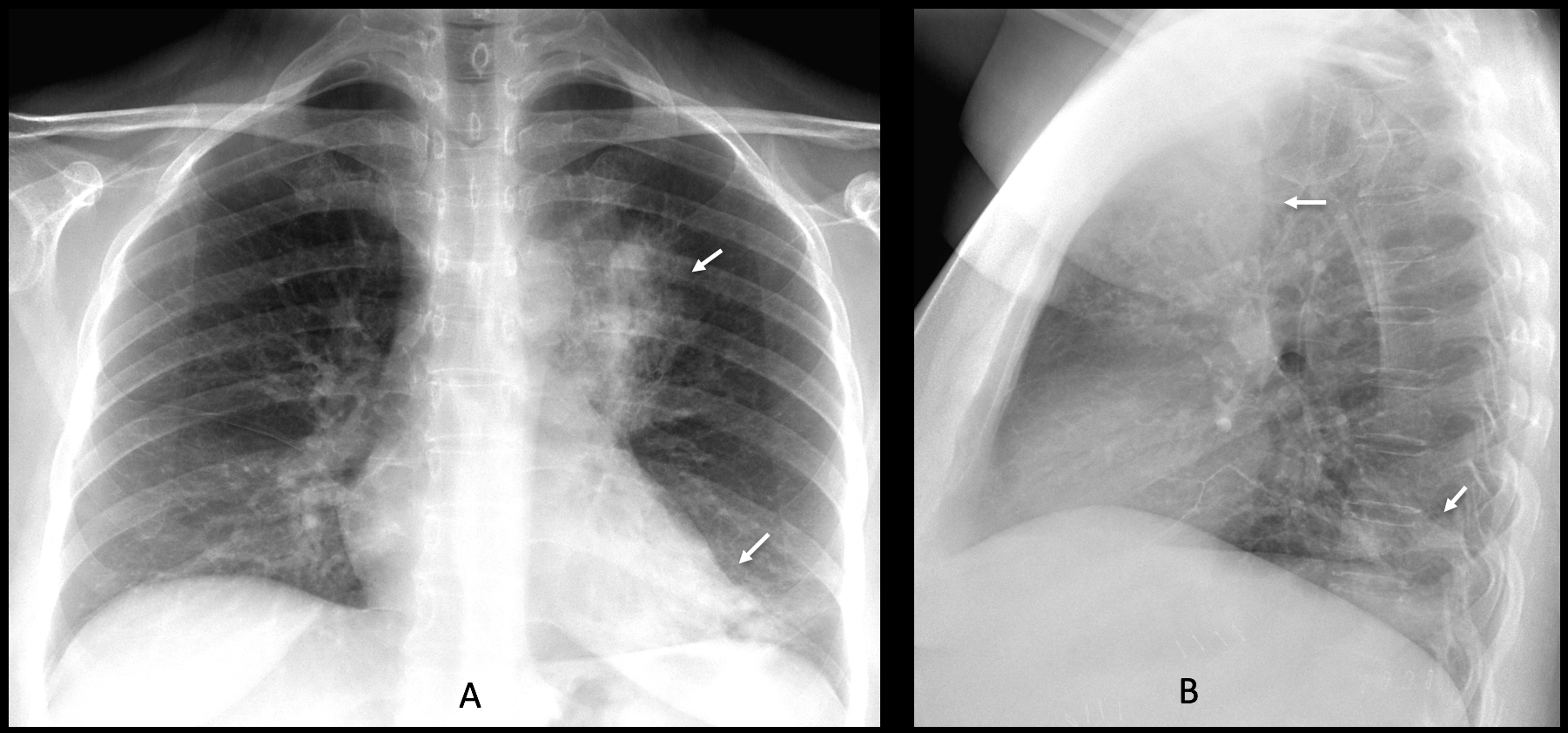
Findings: Chest radiographs show air-space disease in the LUL and LLL (A-B, arrows).
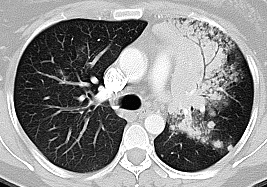
Enhanced axial CT confirms the LUL air-space disease, with an obvious air bronchogram (C-D, red arrows).
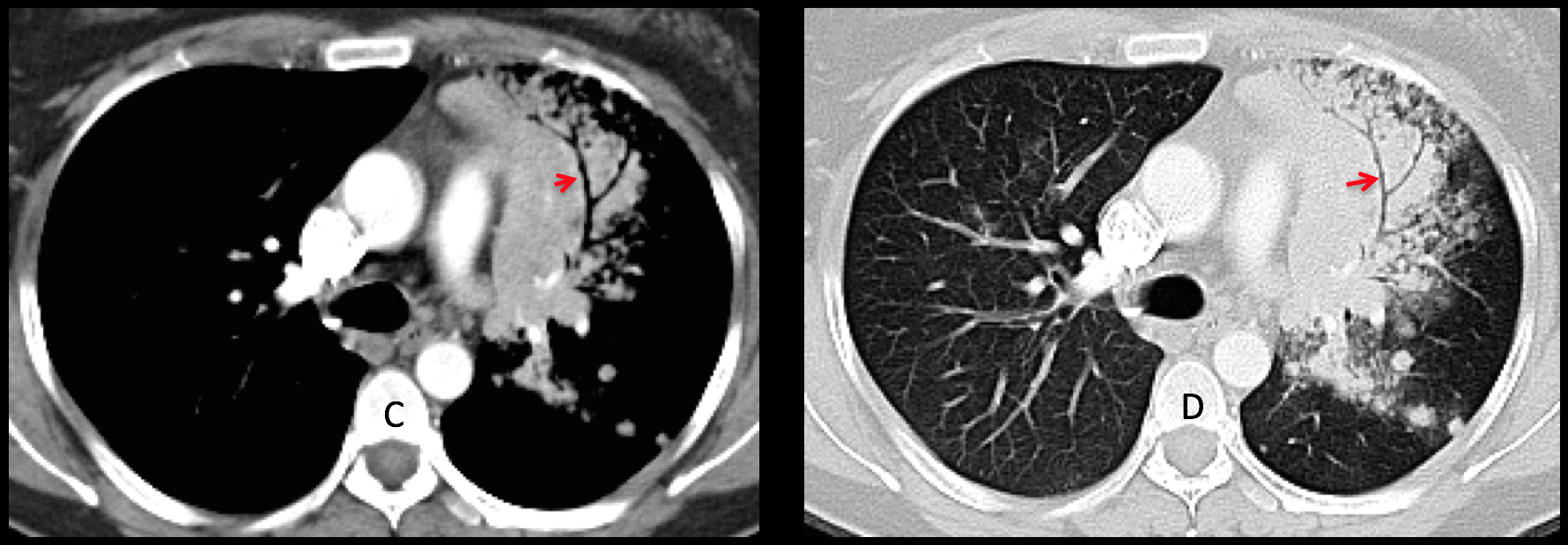
The bronchi are squeezed and scarcely branching. This appearance is highly suggestive of a malignant process that infiltrates the alveolar space, either adenocarcinoma or lymphoma (see Dr. Pepe’s Diploma Casebook Case #62). Biopsy confirmed the diagnosis of adenocarcinoma.
Control radiographs taken one year later show progression of the disease (E-F, arrows).
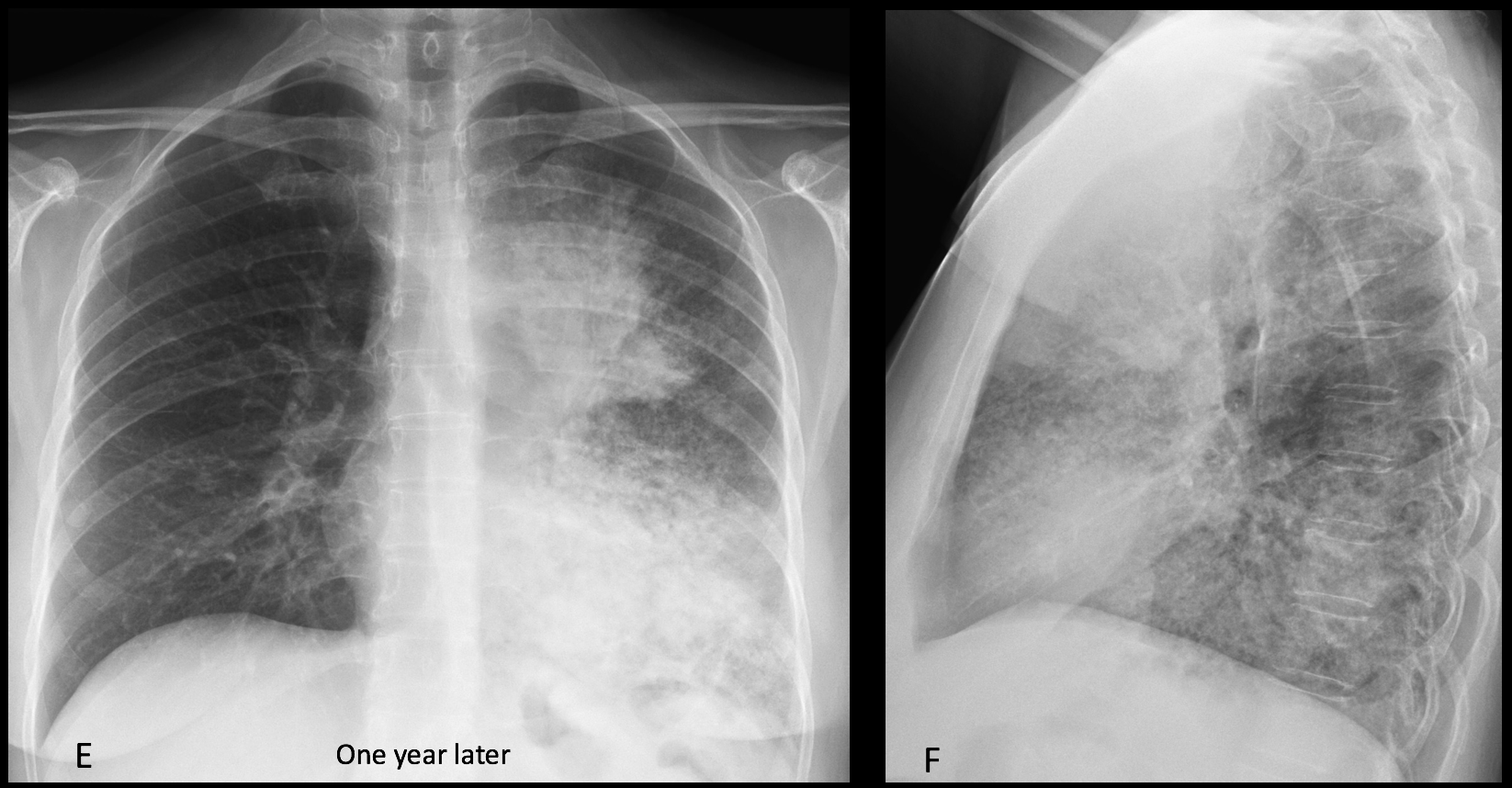
Final diagnosis: adenocarcinoma of the lung (alveolar-cell variant).
Congratulations to Amjad Ramzanali, who suggested the correct diagnosis.
Teaching point: remember that dilated bronchi are usually seen in inflammatory opacities, where the volume loss makes the bronchi shorter and wider. Narrowed bronchi, the so-called leafless tree appearance, occur in neoplastic infiltration of the alveolar space surrounding the bronchi.
This is the last case of the season. See you again in September.
Enjoy your vacation!





Good morning!!
Alveolar consolidation at lingula with air bronchogram. Also in the lateral view there is an increased density in the LLL.
Abdominal surgical staples.
In CT there is a left paramediastinal solid hyperdense mass with bronchogram and peripheral tree in bud and nodules.
We have to rule out malignancy but perhaphs it could be superinfected.
Good morning
I can choose any of above 4
There is patchy opacity at LUL zone and LLL zone. Surgical clips are also noted.
On CT, there is focal consolidation, surrounding with GGO, centrilobular nodules, possibly with TIB pattern, and some small nodules in left lung, some mediastinal nodes, also suspected some GGO in right lung
Differential diagnosis are chronic infection, and malignancy
Hello! The chest xray shows alveolar infiltrations in the left upper and lower lung field. On ct there is consolidation with air-bronchogram and many surrounding nodules, which could be suggesting a granulomatous disease. There may also be some left hilar lymph nodes with calcification. Given that the findings did not change in the last 6 months, the malignancy may be less likely. So this could be tubeculosis or a fungal infection, especially if there is immunosuppresion?
Wish you a nice summer vacation!
Have to disagree with you about the lack of change. Adenocarcinomas may be very indolent. In this particular case, the leafless tree appearance of the bronchogram is a strong indication of malignancy and trumps all the other findings.
Invasive Mucinous Adenocarcinoma
Yes. Good!
İt could be post primer tbc
There is no obvious adenophaty at pa and lateral view
Nodal engalarhment can’t seen 2/3 of postprimer tbc
BAL Must be done rule olur for malignancy
Answer: any of the above.
Air bronchogram sign 🙂
There is a consolidation in the left upper lung. Ddx: TB
Good afternoon sir. Cxr pa view shows increased left perihilar non homogenous opacity with air bronchogram within. No cavitation or calcification seen.aortic knuckle silhouette also not lost. Patchy opacity seen along left paracardiac border with no loss of silhouette suggestive of posterior basal segment involvement seen
On ct scan there is well defined perihilar opacity abutting the mediastinum with consolidation of apical segment of LLL and associated opacities with halo sign , suggestive of :
1. Fungal angioinvasive aspergilloma .
2.central bronchoalveolar carcinoma with lung consolidation.
On ct scan there is well defined perihilar opacity abutting the mediastinum with consolidation of apical segment of LLL and associated opacities with halo sign , suggestive of :
1. Fungal angioinvasive aspergilloma .
2.central bronchoalveolar carcinoma with lung consolidation.
radiograph show left upper zone consolidation
CT show non-segmental consolidation with GGO suggestive of associated haemorrhage, infiltration of the mediastinal fat and left pulmonary veins
multiple nodules alonge the left oblique feutrues
features strongly suggestive of Adenocarcinoma
I believe you all can refine your diagnosis by looking at Diploma case 62 🙂
Adenocarcinoma. Lepid growth pattern. Un abrazo
Good diagnosis.
Dr Pepe manda un abrazo de vuelta
I believe this is fungal infection.
On CT scan, according to thin stretched bronchi within LUL consolidation, suggest lung malignancy.
Good! Somebody is reading/remembering the previous Diploma cases!