
Dear Friends,
Muppet considers himself a celebrity and, like everybody else, he wants to show you a selfie. Today’s case is provided by my good friend Dr. Fernandez Alarza. Radiographs belong to a 33-year-old woman with moderate dyspnoea. I showed it to Muppet and since he is the smartest guy in the Universe, he made the right diagnosis up to the last finding.
Can you guess Muppet’s diagnosis? What do you see?
Leave your thoughts in the comments section and come back on Friday for the answer.

Click here for the answer to case #88
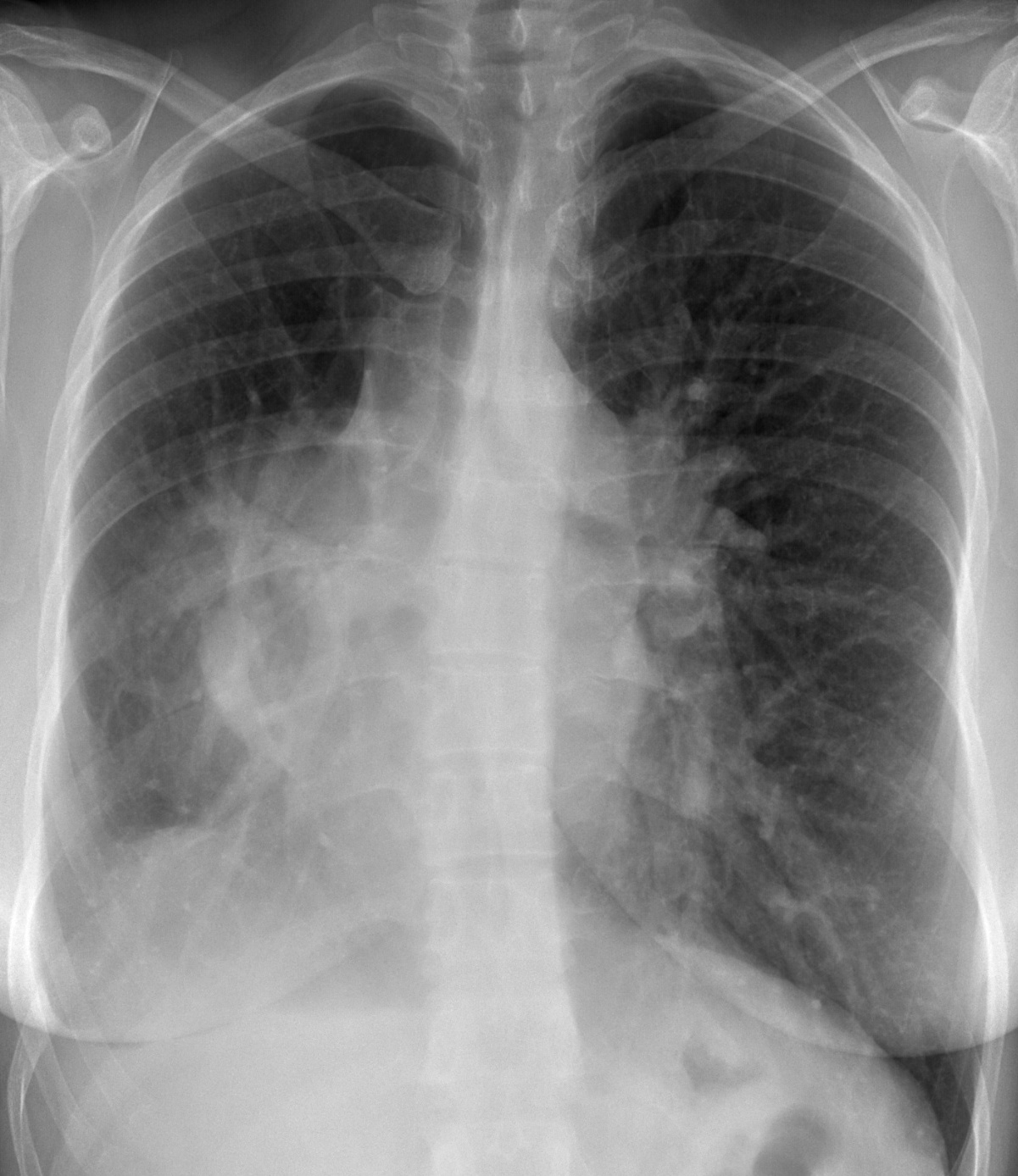
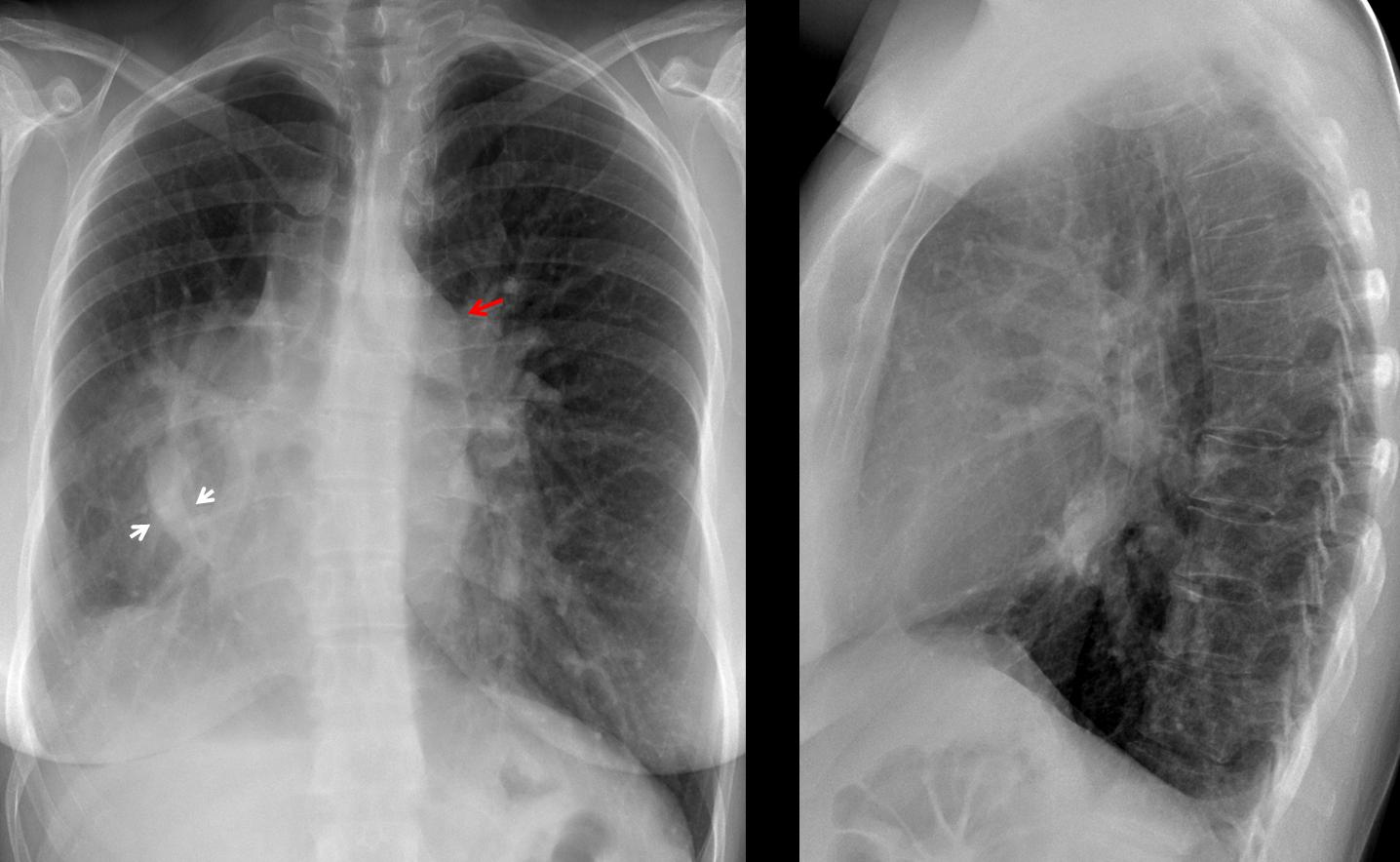
Findings: PA chest shows a small right hemithorax, with displacement of the heart towards rhe right, haziness of the heart border and a scimitar vein (arrows). These findings are characteristic of congenital hypogenetic lung. In addition, there is prominence of the pulmonary trunk (red arrow) and increased pulmonary vascularity. These findings point towards a left-to-right shunt (see Dr. Pepe’s Diploma Casebook case 52).
Coronal CT confirms the scimitar vein (arrows), as well as an enlarged right atrium B, arrows), due to a shunt at the atrial level, confirmed at surgery.
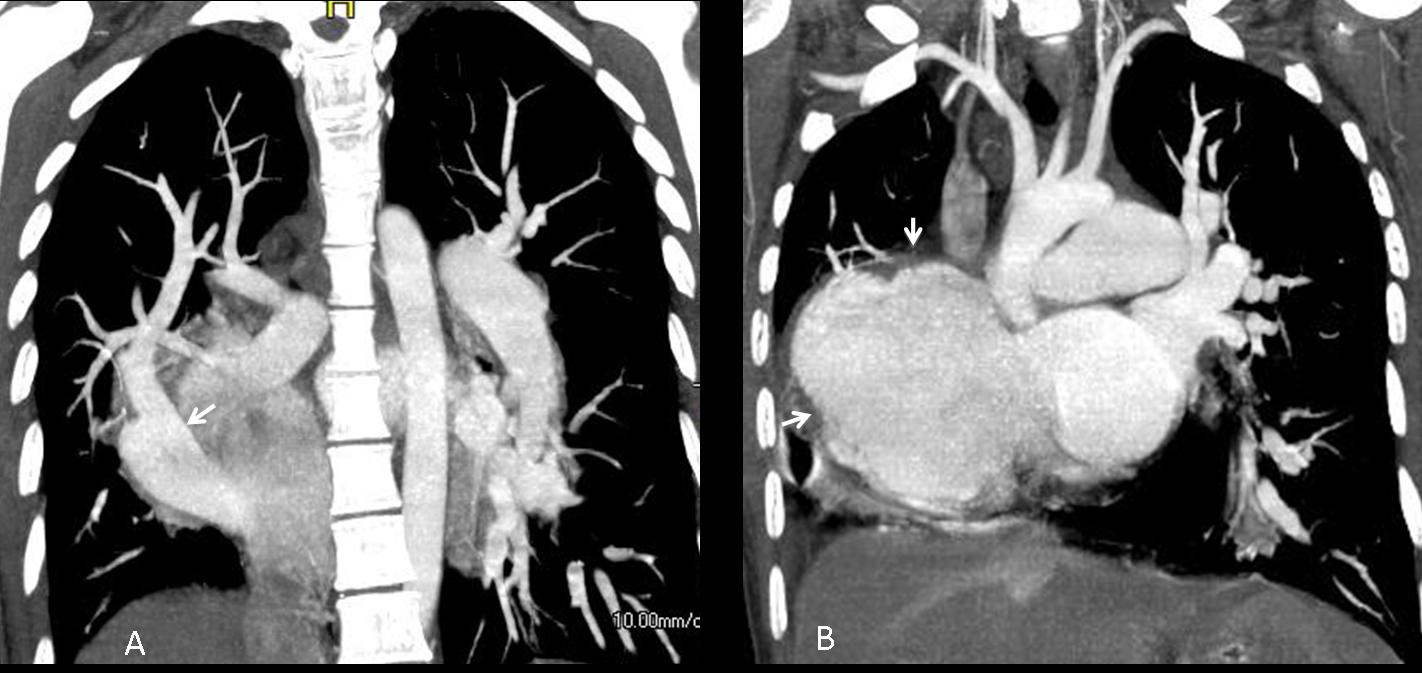
Final diagnosis: hypogenetic lung syndrome, associated to an ostium secundum defect.
Congratulations to Murzin, who made the right diagnosis.
Teaching point: this is a nice case of satisfaction of search. Discovering the obvious alteration (hypogenetic lung) leads us to stop investigating and miss the left-to-right shunt, which is more important in the management of the patient.


Chest radiograph frontal projection
I’ll defined radio opacity overlying the right heart border & silouettbing with extension into right hilum.
Right dome is ill defined with overlying uniform radio density and blunting of right costophrenic angle
Shift of mediastinum and trachea to the right
Lateral chest radiograph
Loss of retrosternal lucency with prominent hilar shadow
Collapse of lung with effusion
…mitico Professore, il Bari è in serie B ed è fallito…..speriamo di “risalire a vedere le stelle”….intanto “pariamo ” il colpo dei “blaugrana”….quello che fai vedere è la “S. della scimitarra”, esempio di ritorno venoso anomalo “parziale” con ipogenesia del polmone dx e destrocardia….è inutile pertanto che elenchi la semeiotica elementare presente in questo caso…con stima!
I think You are right…
so: right venolobar syndrome with partial anomalous venous return…
I think atrial septal defect should be also considered…
Hi Professor Caceres, we miss u so much at the ECR this year!
The X ray show a sligh shift of the mediastinum to the right, increase of the size of the pulmonar vascular structures giving the image of a prominents hilum, bilaterally,with enlarged pulmonary arteries. I see a tubular structure in the right lower hemithorax and a probably hipoplastic lower lobe, very suspicious for a vascular anomaly as a vein (could represent a partial anomalous venous drainaje ?? ). The heart show very blurred margins, as well as the aortic silhuette, which I can not identify properly. Giving the age of the patient this findings might be related with a kind of congenital cardiac/vascular malformation, which I have to think about it 😉
Hi, interesting case.
The film is slightly rotated and there is also a thoracic scoliosis.
There is tracheal deviation to the right and plethoric lung fields. There is a right silhoutte sign with an ill-defined opacity and an air bronchogram. I see an ill-defined circular radioopaque shadow in the right lower zone along the 9th right with an ill-defined margin, which seems to be in the hilar region on the lateral view. There is also blunting of the right costodiaphragmatic recess indicative of a pleural effusion.
I’m not sure if there is also a mass in the right hilum..
my dx would be right lower lobe collapse-consildation with a right pleural effusion with possibly ca bronchus.
as the alias i’m still in medical school so excuse me if my description and dx is way off. what advice would you give to an aspiring radiologist?
thank you.
….cosa succede Professore? Poche risposte…tu che non commenti…..li hai spaventati tutti….se la risposta esatta non è la mia,dacci qualche suggerimento prima del fischio finale al 90!
Sorry, your answer was correct, but incomplete. See answer by Murzin.
I think that we have few answers because the ECR virus: people get tired during and after the Congress (not unlike the FIFA virus in Barça players!)
….è chiaro che vi sia ipertensione polmonare…ma essa può essere sostenuta oltre che da una DIA od un DIV( come appunto si può associare nella sindrome della scimitarra) , anche da un semplice sovraccarico del piccolo circolo determinato dal vaso anomalo che drena nella VCI: non l’ho menzionato perchè il quadro era evidente…Per il Barca, auguro il TRIPLETE( ma il Real di quest’anno è veramente molto forte!!!!!)
ECR virus is good ….but dr pepe is addictive drug 🙂
nice case!!!!