This time I want you to make an easy diagnosis in the case of a 79-year-old woman who was found unconscious at home. Supine chest film obtained on admission. Is the chest abnormal? What do you see?
Examine the image below, leave your thoughts and diagnosis in the comments section and come back on Friday for the answer.
Findings: supine AP film shows a congenital rib malformation with a pseudoarthrosis between the first and the third right ribs (A, B, yellow arrow). The main finding is a line parallel to the right rib cage that raises the possibility of a pneumothorax. Diagnosing a skin fold is easy because vessels are crossing the line (circle in B) and especially because the minor fissure crosses the line and reaches the chest wall (A, B, red arrow). If a pneumothorax were present, the fissure would stop at the border of the lung.
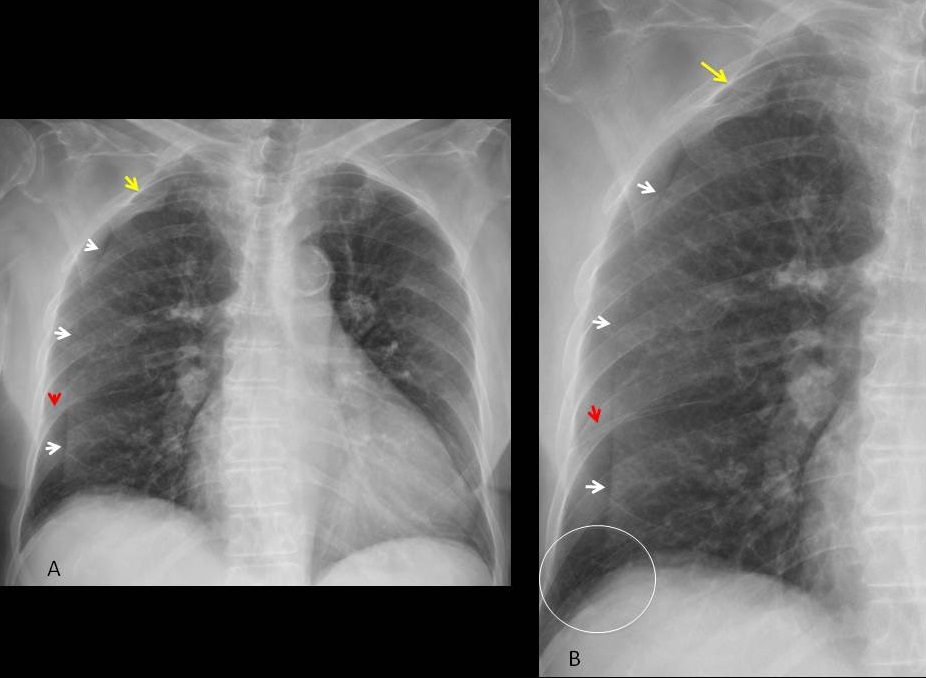
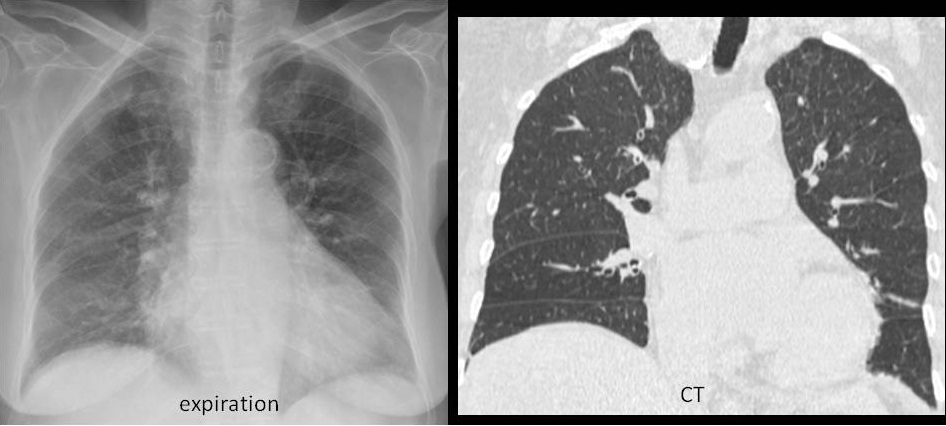
Despite the obvious findings in the AP film, an expiratory film and a CT were performed. Both of them failed to demonstrate a pneumothorax.
Final diagnosis: skin fold mimicking pneumothorax.
Congratulations to Gus, who was the first to give an explanation of the findings.
Teaching point: paying attention to basic findings is crucial to making the correct diagnosis. In this case it would have saved valuable time and money.



….pn-torace dx…..possibile che la diagnosi sia così facile? frattura 3 costa dx ?….
Pneumothorax on the right? or pseudo pneumothorax? Could bed sheet fold mimicking pneumothorax?(Supine chest film )
I am not sure if there is a fracture on the 1-3 ribs on the right or is a displasia of cervical rib (pseudarthrosis).
(Thoracic outlet syndrome)?
You are full of doubts. Too many interrogations.
Should be not? 🙂
Yes, you should be more assertive. Remember: “an expert is someone who make mistakes with confidence”
i think is pseudo pneumothorax!!!!!! It has a lot of confidence that? 🙂
Firsts three ríbs on the right are abnormal. Some of them are forked showing pseudoarticulations. Heart shilouette is enlarged but this finding can be normal on supine. There is a skin fold on the right hemithorax as Gus said.
There are some linear opacities on the lower aspect of the left lung that can be due to linear athelectasis.
Left lung is a bit less dense than the right one. Also there are more vessels on the right lung than on the left. This finding can be due at less partaly to slight rotation of patient. However I think it can be true. I would consider a PE as a pdiagnostic posibility in this patient. Am I wrong?
As you say, probably rotation accounts for the slight diiference in opacity of both lungs. Patient did not have PE.
Now that we have a menage a trois (two against and one in favour).
would you do expiration film to prove/disprove your diagnosis? And/or CT?
Should inform you that the patient was awake at the time that the AP film was taken.
No…. is pseudo pneumothorax.
If the patient has pneumothorax symptoms the best method to see a small pneumothorax is CT but that hyperlucent part on the right is not.
Supine pneumothorax has different distribution plus the minor fissure extended through hyperlucent area to thoracic wall
I wouldn´t do any other imaging test. I would go to see her chest trying to found out for example if he is very thin.
As you say the patient was awake at the time of taking the PA view I would ask him about any chest pain or dyspnea.
Maybe it is a combination of pseudo pneumothorax and pneumothorax. I agree that the vertical line near the lateral chest wall on the right is a skin fold. I suspect pneumothorax because of possible double diaphragm sign on the right.
As for ribs -I would say there is articulation between first and second rib (which are bifid).
…la domanda del professore è chiara…cosa farei in caso di sospetto pn-torace? il problema si pone ovviamente x “piccoli” pn-toraci in cui la radiografia tradizionale può essere “muta”…farei l’ecografia “beside ultrasound” ricercando i segni ecografici del Pntorace: Perdita dello “silding” pleurico e presenza del “double sign”…
…la paziente è stata mastectomizzata a dx !
Firstly I was sure that it is a skin fold mimicked a pneumothorax in the right lung and nothing abnormal except an enlarged heart is not seen. But this “skin fold” is strange, it is too much similar to the lung shape and in the right lung apex it is detected additional line of the possible pneumothorax. But in the lung’s bases pulmonary vascularity is good seen, what I’m not expecting to see in pneumothorax. So, I don’t know. In my report I would recommend chest CT for exclusion of right sided pneumothorax.
There is a finding that helps to eliminate neumothorax and therefore eliminates doing CT.
Yes, it’s obvious now, interlobular fissure is seen, no pneumothorax. “Easy case” as you said at the beginning 🙂
…but in real life I’d like perform control chest film in few hours …
See? Once we pay attention to the basics, diagnosis is easy. Congratulations
Lung vasculature extends beyond the line of the skin fold.
Not only the lung vasculature.
Horizontal fissure as well.
Good. You passed the test.
Thank you. 🙂 Very interesting case to analyze, loved it.
Cardimegaly
Aortic calcification
Intravertebral disc heights are decreased in thoracic region