Muppet wants to test your diagnostics skills with the following case of a 39-year-old smoker with dyspnea. Check the images below, leave your diagnosis in the comments, and come back on Friday for the answer.
1. Bronchogenic carcinoma
2. Endobronchial TB
3. Benign endobronchial tumour
4. None of the above
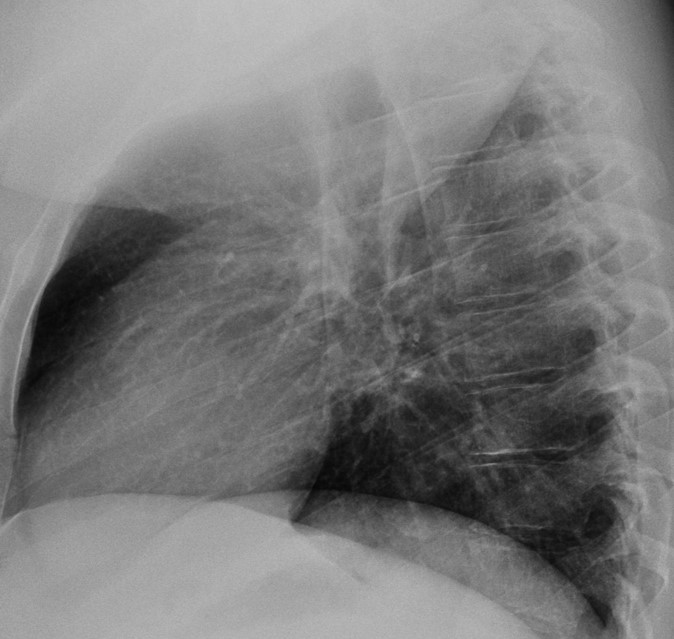
Findings: the chest radiograph shows a typical RUL collapse, confirmed with unenhanced coronal CT, which shows occlusion of the RUL bronchus (Fig. 1B, arrow).
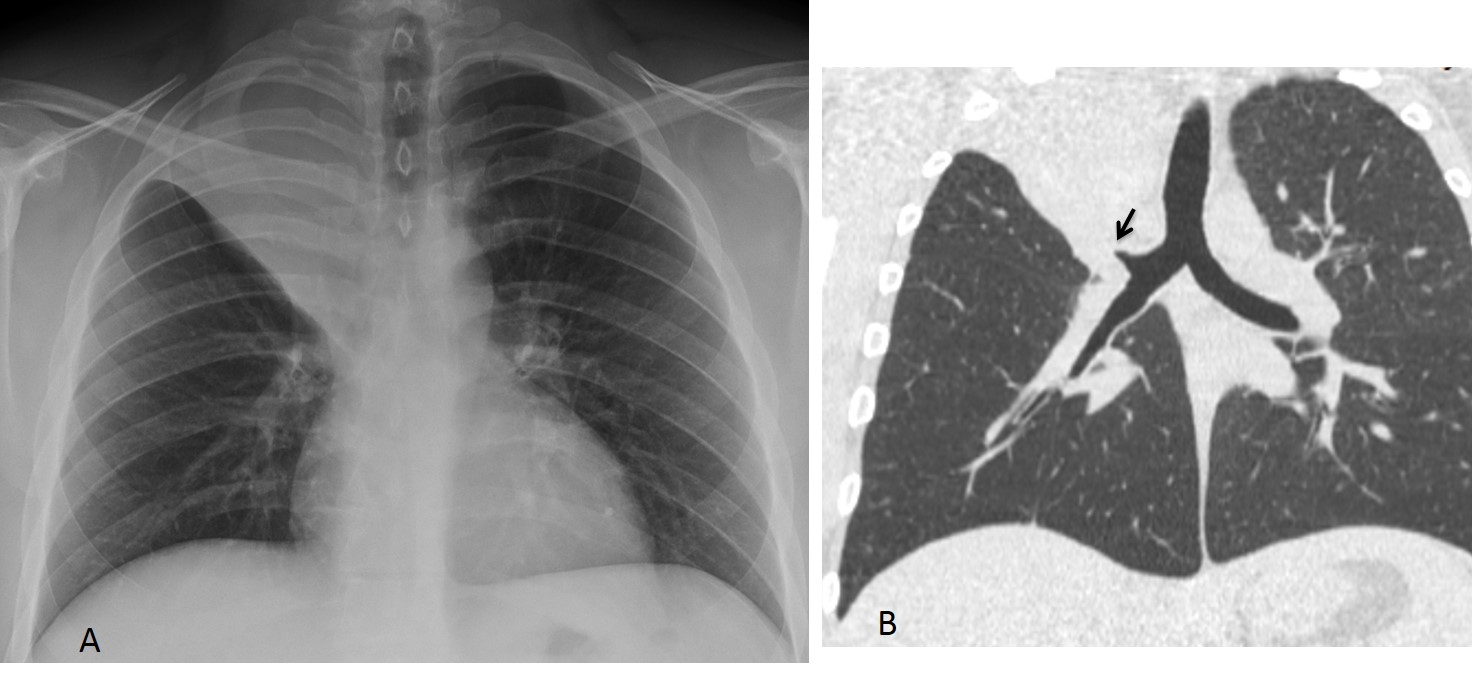
Fig. 1
The clue to the diagnosis lies in identifying high-opacity branching structures within the collapsed lobe (Fig. 2 A-C, arrows).
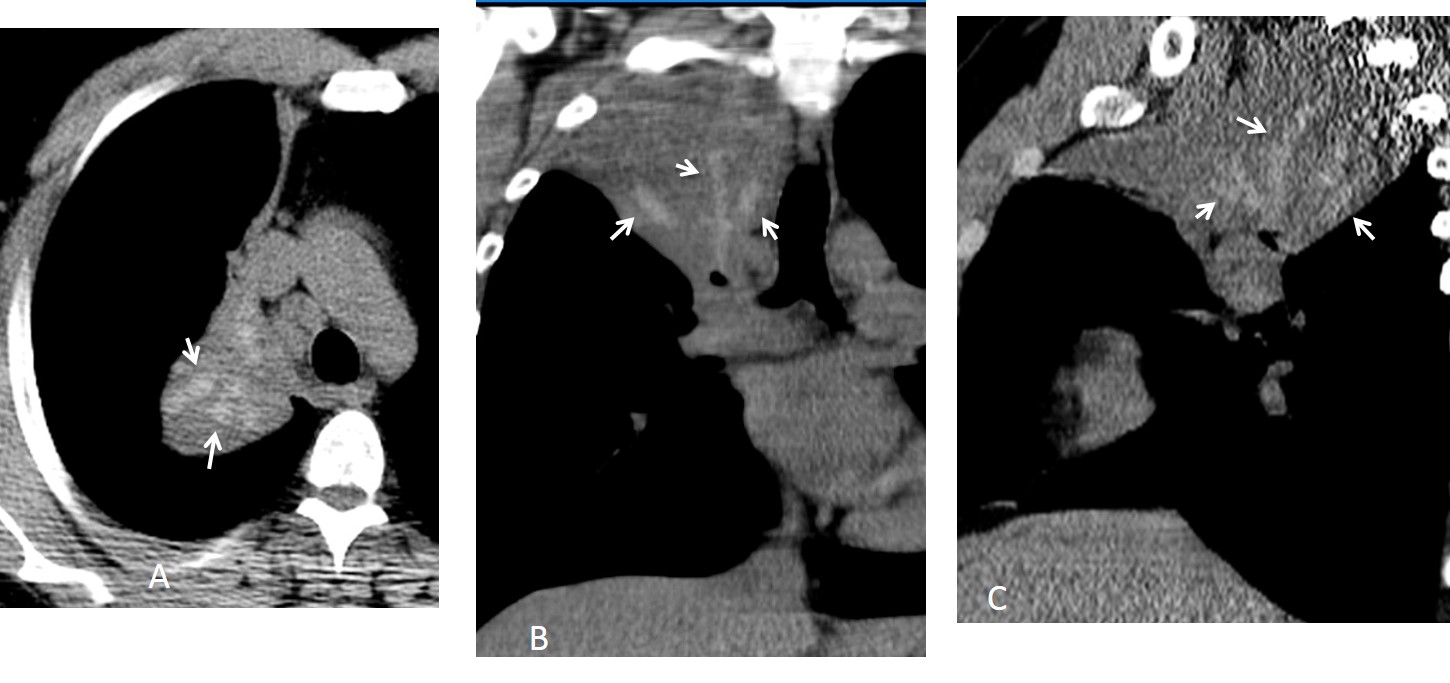
Fig. 2
Since the RUL is obstructed, they most likely represent mucous impaction. As the main cause of dense mucous impaction is allergic bronchopulmonary aspergilosis, this is the most likely diagnosis. This suspicion was confirmed at bronchoscopy. After removal of the plugs, the chest showed marked improvement (Fig. 3).
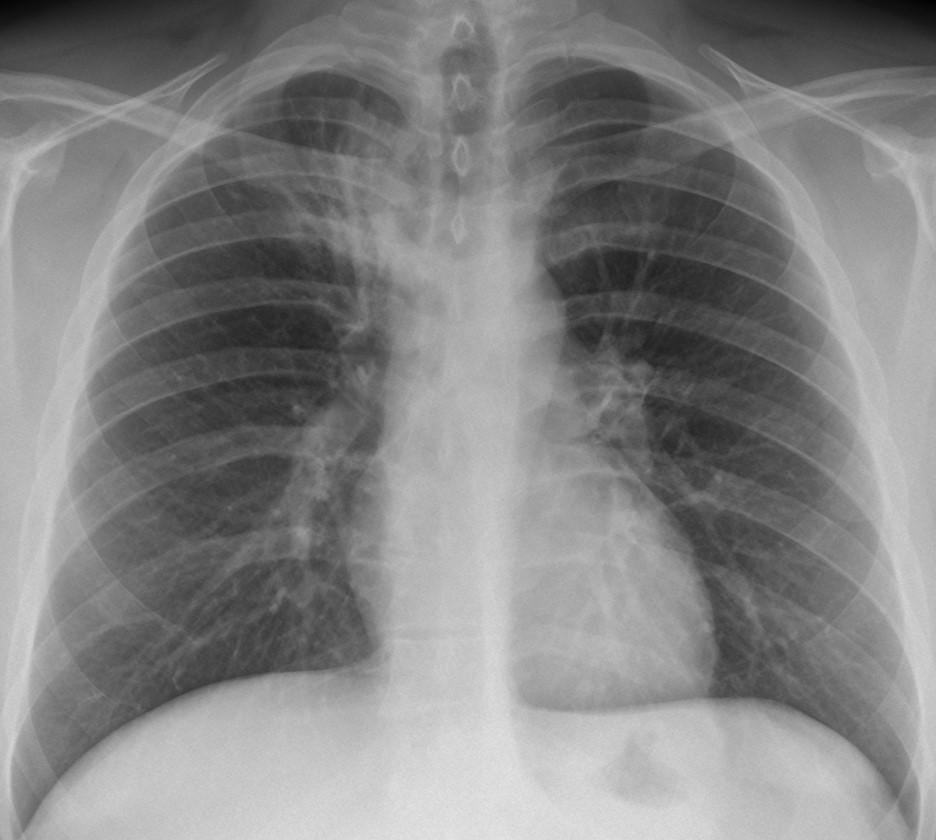
Fig. 3
Final diagnosis: ABPA, causing RUL collapse.
Congratulations to Gaborini and Laurens who made back-to-back diagnoses.
Teaching point: it is important to know useful signs, because you never know when they are going to help. I have made brilliant diagnoses by recognising the dense mucous plugs … except in this particular case, in which I overlooked them! Nobody is perfect!





on Rx partial – segmental opacity with out air bronchogram of the right upper lobe B2.no tracheal shifting. no juxtaphrenic peak . a small elevation of the minor fissure.
on the ct we can see a small lost of volume of the right uper lung and a mass like lesion above the right hilum.
The right sternoclavicular joint it s ok?
Posterior sternoclavicular joint dislocation?
This is a straightforward case. The answer is in the films.
Sternoclavicular joints are OK.
….faccio pre-tattica….il goal al 90’…..
OK, I will wait for the right answer in the last minute!
plain film and Ct demonstrate uniform opacity of the right upper lobe.The right minor interlobar fissure is displaced upwards indicating right upper lobe atelectasis. CT shows that right upper lobe bronchus is filled with soft tisue opacities.There is mediastinal lymphadenopathy.
Diagnosis: Bronchogenic carcinoma.
Nice description, but the diagnosis is incorrect.
I think that suspected mass like lesion on CT above right hilum is actually collapsed lung – upper right lobe atelectasis.
Upper lobe atelectasis can also be seen on chest radiographs
(triangular RUL homogenous opacity, cranial displacement of horizontal fissure).
If I am correct I ask myself what are these hyperdense opacities inside the collapsed lung on last CT picture. If they are hyperdense vessels on non-enhanced scan could this be pulmonary embolism?
Yes, you are right, the dense opacities are the clue to the diagnosis.
Poststenotic (resorptive) atelectasis due to mucoid impaction. Possible cause Allergic bronchopulmonary aspergillosis?
melanoma? carcinoid?
mucus plug? or maybe a mucus producing tumor?
and if those dense opacities correspond to bronchial structures, then ABPA could at least be considered as well
congrats, you are 10 mins earlier, we were on the same track 🙂
Shall we consider it a team effort?
Absolutely, team work is great. Gaborini deseves first place though, i was stuck reading differentials for a little bit too long. 🙂
it’s a split first place
Ca bronchus causing rt. upper lobe collapse.
Hi!
I guess, it is a RUL atelectasis due to a benign endobronchial tumor. There is no malignant mass seen, no expancity, no lymph node involvement, RUL-bronchus is smoothly cuting off.
I believe , I’ve seen the same appearance once in my practice : young woman with bronchial cut off.
Endobronchial benign tumor ? (Non expansive athelectasic and no bone infiltración)
Hiperintensity it’s due to a mucus producing tumor ?
So, “endobronchial benign neoplasm mucinoid ” ?
(Sorry due to my poor english)
Usually, with a lot of mucus you have a “mucinous bronchogram sign” in which the bronchi are less dense that the surrounding parenchyma. The case presented shows the opposite: high-density mucus. This sign is highly suspicious of allergic aspergillosis.
Stenosi bronco superiore dx da K, con atelettasia lobare superiore ed enfisema secondario dei due lobi restanti.
Last try – Mucoepidermoid carcinoma of lung?
Sorry,no. See the answer by Gaborini and Laurens
lobectomy.
Is not my round 🙂
It was not mine, either. I missed the diagnosis!
….complimenti “galactico”….il numero di risposte indica l’interesse suscitato da questo caso!…io penso, che la diagnosi esatta l’abbia proposta tu, quando tra le opzioni diagnostiche hai suggerito la TBC endobronchiale: le calcificazioni, alla TC senza mdc, possono corrispondere a granulomi di necrosi caseosa, calcificati, che a sede endobronchiale, hanno determinato la successiva atelettasia del lobo superiore…..alcune delle immagini adenopatiche sembrano avere le stesse calcificazioni….pensare ad una Aspergillosi(invasiva e/allergica) avrebbe dovuto sottendere un deficit immuninatario.e-o asma o fibrosi cistica, che non sono state riportate…..se ho sbagliato allora dico che anche i grandi , a volte piangono(il Barca di quest’anno)…..
Barça may still win the championship. We will see in two wooe’s time.