to celebrate the coming year Muppet wants to finish the chapter of air-fluid levels by showing you two patients with fever and malaise.
1. A in a pleural cavity and B in a lung cavity
2. B in a pleural cavity and A in a lung cavity
3. Both in a lung cavity
4. Both in a pleural cavity
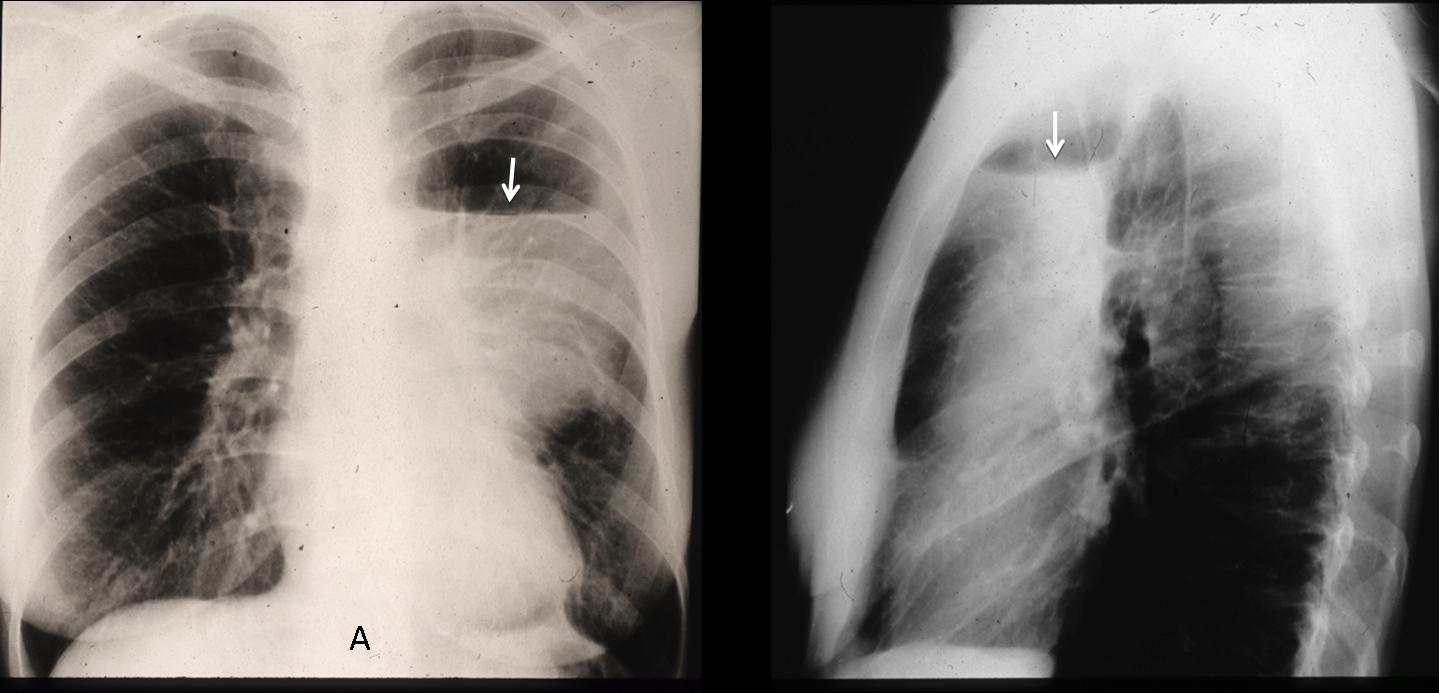
Case A findings: chest films show an air-fluid level (arrows) in the left hemithorax which follows the requisites for hydropneumothorax: the length of air-fluid level is different in PA and lateral projections, has no superior wall and goes across the whole hemithorax in the PA projection.
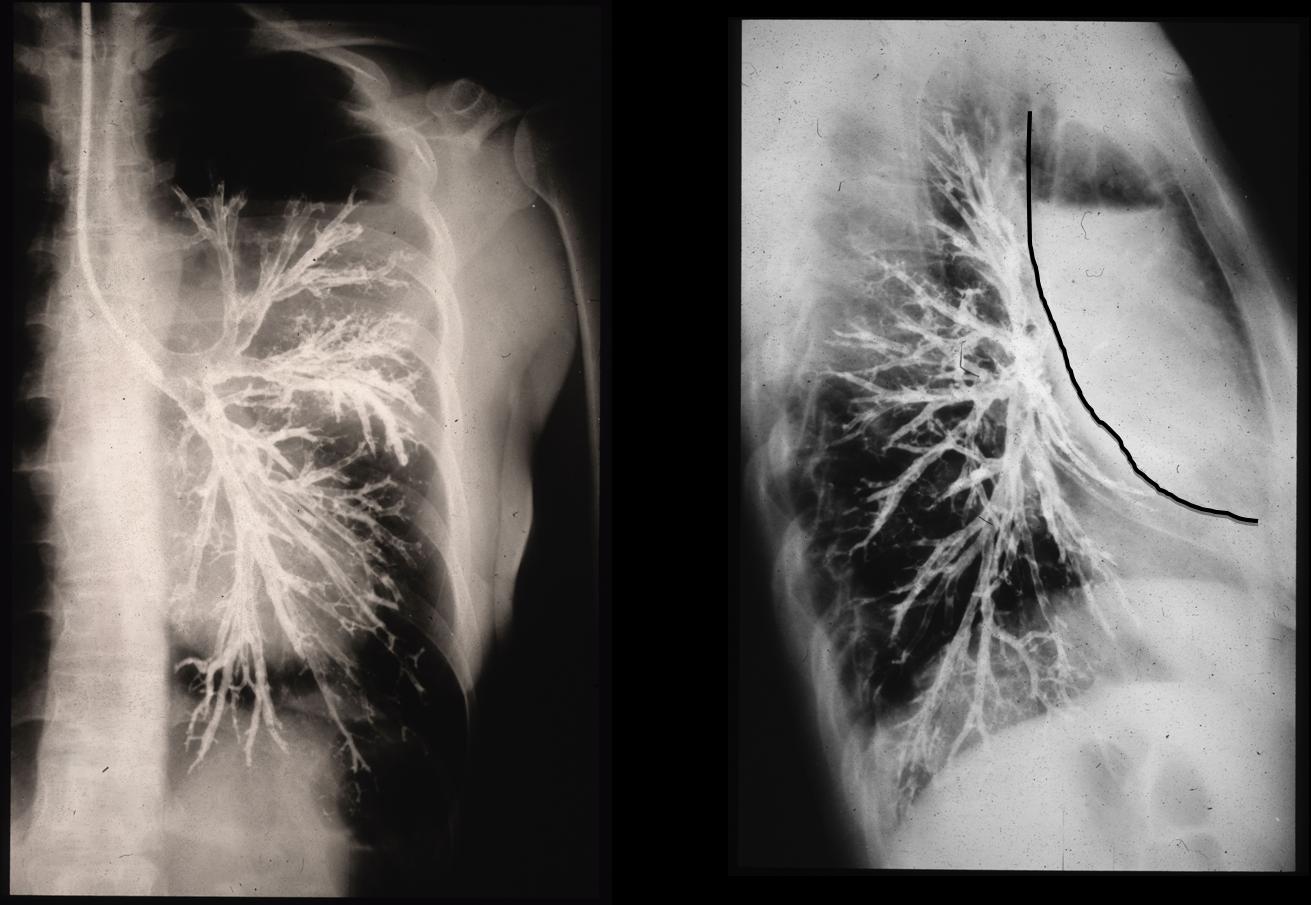
The case is from the pre-CT era and diagnosis was confirmed with broncography, which shows an extrapulmonary lesion displacing the bronchial tree without involvement of bronchi (Muppet performed the study and is very proud of his technique).
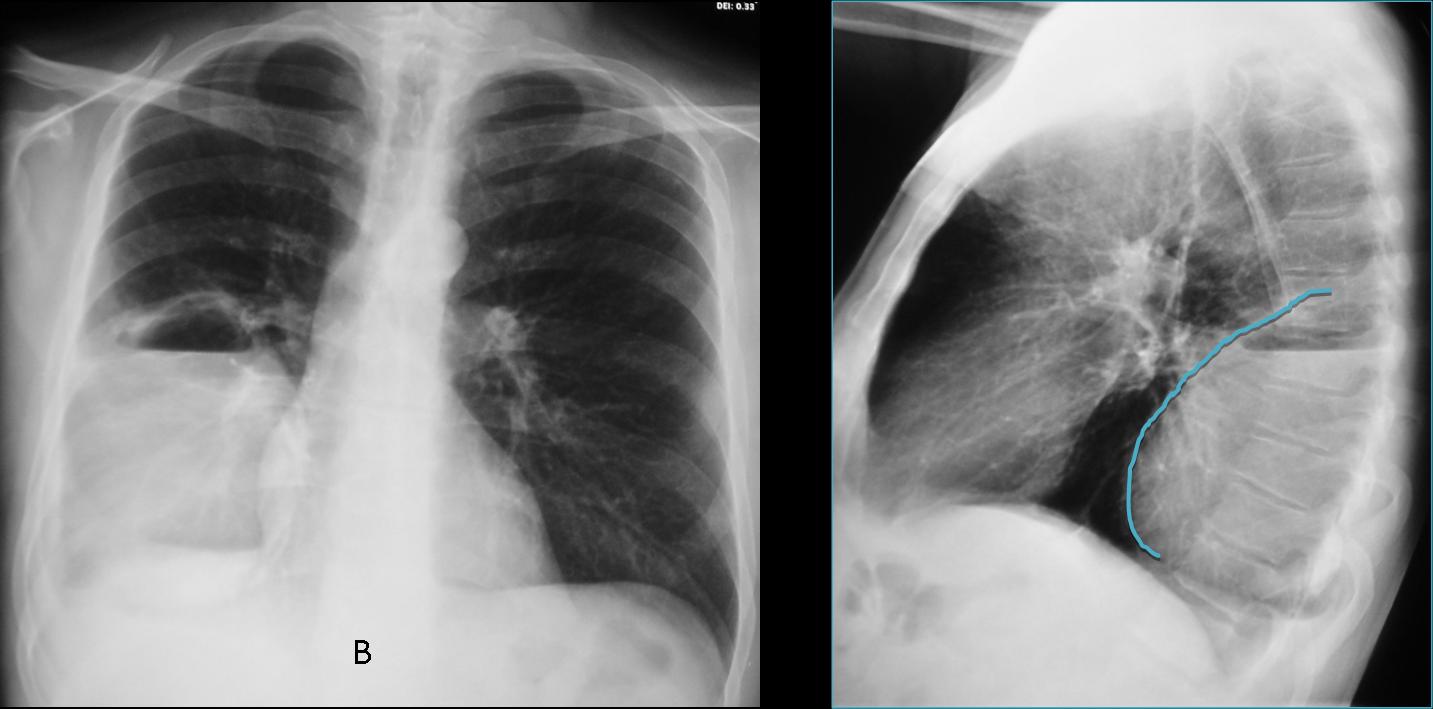
Case B shows a right lower peripheral lesion with air-fluid level and a superior wall. At first glance, it seems intrapulmonary. However, there is blunting of the costophrenic angle (arrow) and the lateral view shows a superior obtuse angle, suggestive of an extrapulmonary lesion.
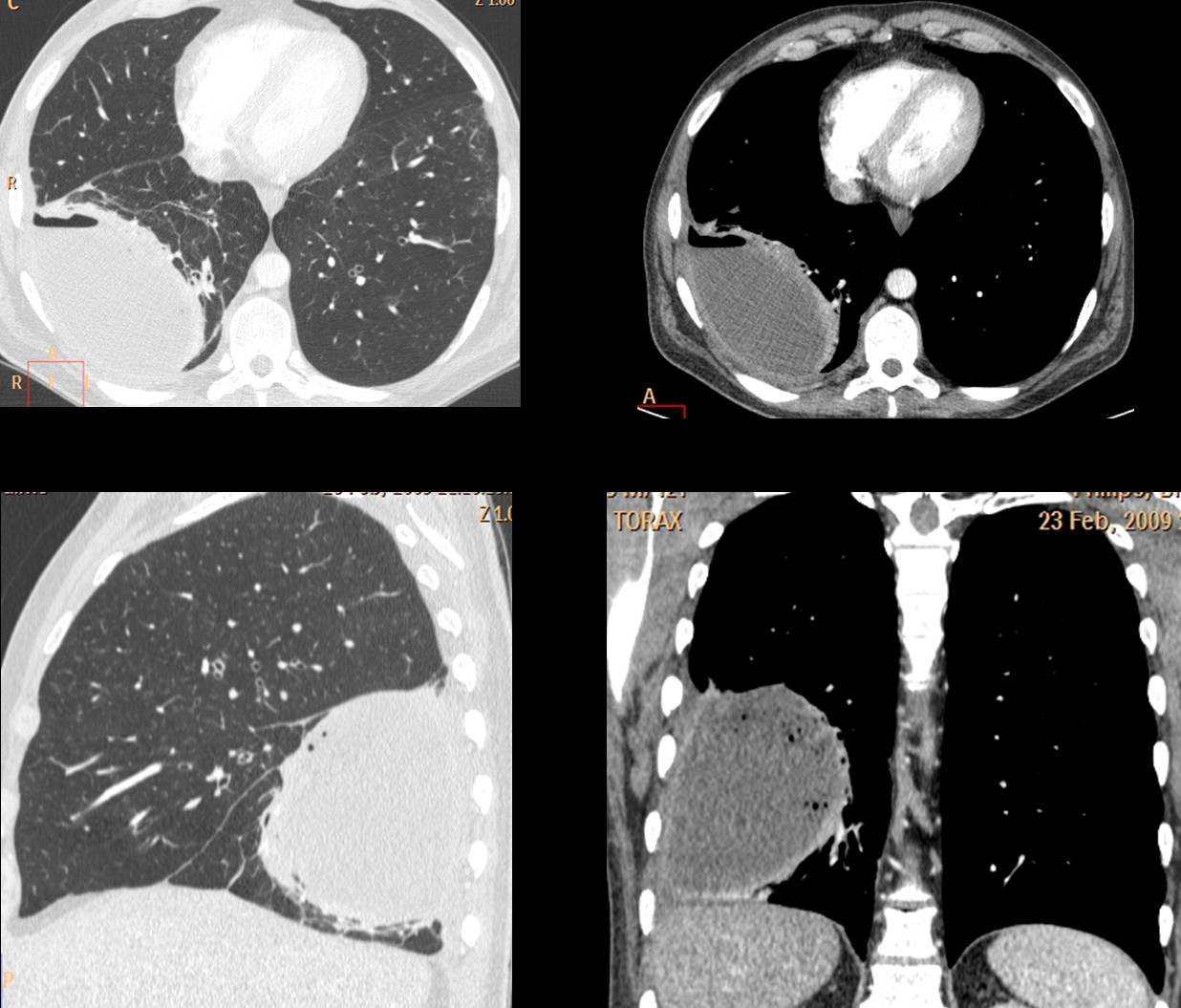
The findings suggest loculated pleural fluid. CT confirms the loculated fluid and the intact lung. Final diagnosis: loculated empyema.
So, the final answer is # 4: both air-fluid levels are in the pleural space
Teaching point: loculated fluid may sometimes simulate a pulmonary cavity because the levels are of equal length and they may have a superior wall. Clues to the correct diagnosis are: peripheral location, blunted costophrenic angle and extrapulmonary contour.





Bella lezione di semeiotica radiologica classica del Professore che ringrazio.I criteri per stabilirne la sede sono tre( in AP e LL).Sede della lesione, margini della lesione ed angoli di raccordo con la parete toracica. In A : la sede( in LL) è mediana;i margini( in LL ), sono indistinti e gli angoli di raccordo non sono ben valutabili. In B , la lesione è periferica, i margini sono distinti, la sua morfologia è simile in AP e LL ed ,infine gli angoli di raccodo sono ottusi( segno della gravidanza).Pertanto se il mio ragionamento è esatto, la risposta corretta è 2.
Happy new year to the Muppet and to you professor !!! Hope you will continue to intrigue us with your exciting cases in 2013 and in the years to come !!! Personnaly, I think that I have learned a lot from your lectures and your cases during last year so I will give it a try with these cases.
In the first case there is an air-fluid level in a cavity with indistinct margins in the AP projection especially in its upper part(incomplete border sign) and distinct borbers in the lateral projection, which indicate a loculated pleural effusion with an air-fluid level. Moreover, the diameter of the air-fluid level is smaller in the lateral than in the AP projection (oval shape) and the angles with the thoracic wall are obtuse, suggesting that the cavity is situated in the pleura in the anterior thoracic wall (extending maybe in the anterior mediastinum).
In the second case the air-fluid level is located in a cavity with distinct borders in both projections which abuts the posterior thoraric wall and the right major fissure in the lateral projection. There is a negative silhouette sign with the right hemidiaphragm in the AP projection. The diameter of the air-fluid level is the same in both projections (round shape). Despite, the obtuse angle of the lesion with the thoracic wall(in the lateral projection), I think that all indications suggest that it is located in the RLL.
So the right answer is 1 (A. in a pleural cavity and B. in a lung cavity).
I hope I didn’t disappointed you and the Muppet. I tried my best !!
I think you are right.
Muppet is not dissapointed and is very happy with your discussion. But…
Muppet wants to give a hand: so far, nobody has made the correct diagnosis.
La morfologia del livello idro-aereo, nelle 2 proiezioni rx è diversa a seconda che essa sia in una cavità acquisita(intrapolmonare) o preesistente ( extrapolmonare).Nel 1° caso essa si comporta come un palloncino elastico che riempiamo di liquido: allora avrà una morfologia e volumetria “identica” nei 3 piani dello spazio.In B si osserva questa condizione ed il livello è intrapolmonare( cisti infetta?). In A la morfolofgia e volumetria è differente nelle 2 proiezioni e nulla sembra limitare la parte gassosa cranialmente, per cui dovrebbe essere extra-polmonare….ma in LL sembra osservarsi una opacità triangoliforme con apice all’ilo, come da atelettasia e pertanto di natura non liquida.Pntorace con atelettasia inziale del lobo polmonare superiore( falso livello idroaereo).
quale è la soluzione finale del caso 48?
I think 3 both are in the lung cavity
Thanks
both are loculated pleural effusion