While I was in Vienna, Muppet prepared the following case for you: 21-year-old girl with marked dyspnea, no fever. What do you think it’s happening?
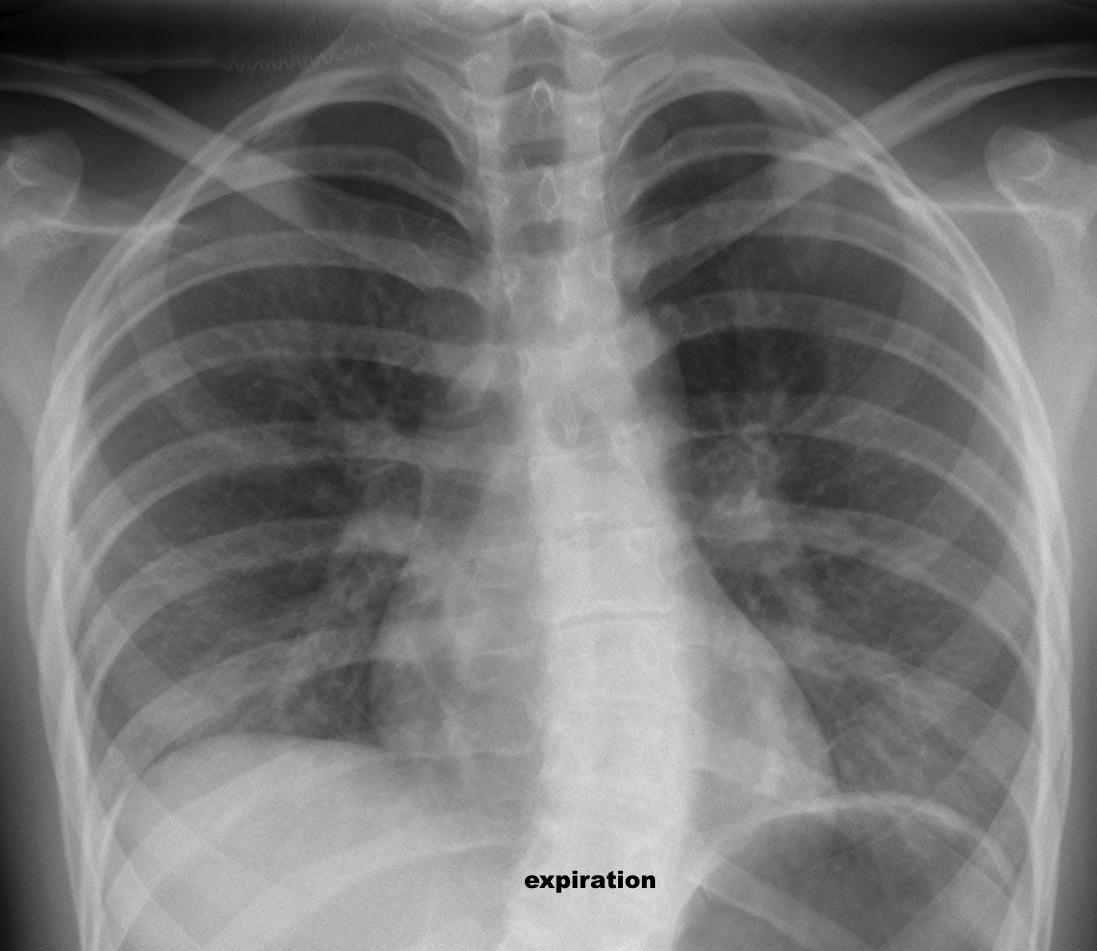
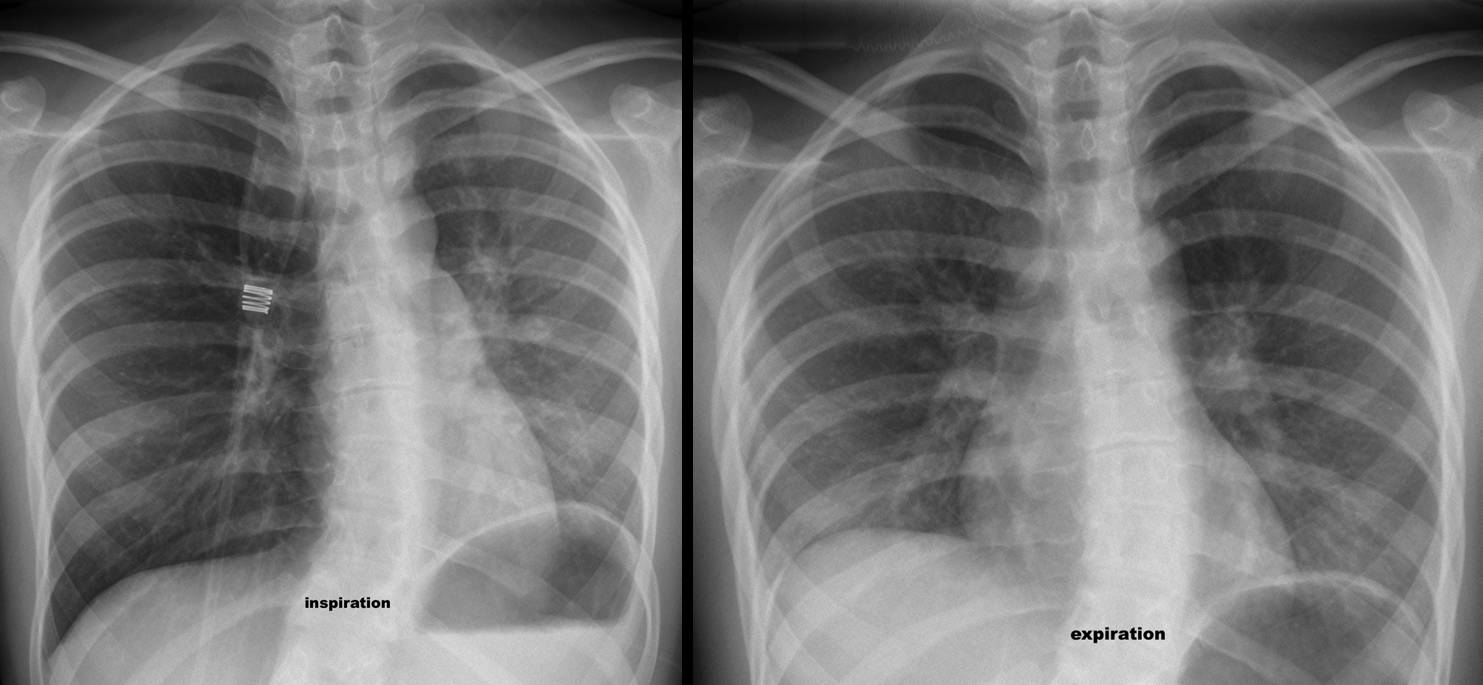
Findings: inspiration film shows increased lucency of right lung, a smaller left lung and displacement of the mediastinum towards the left. Lucency of right lung disappears on expiration and the mediastinum shifts towards the midline. The left hemidiaphragm does not move (it is superposed to the 9th rib in inspiration and expiration).
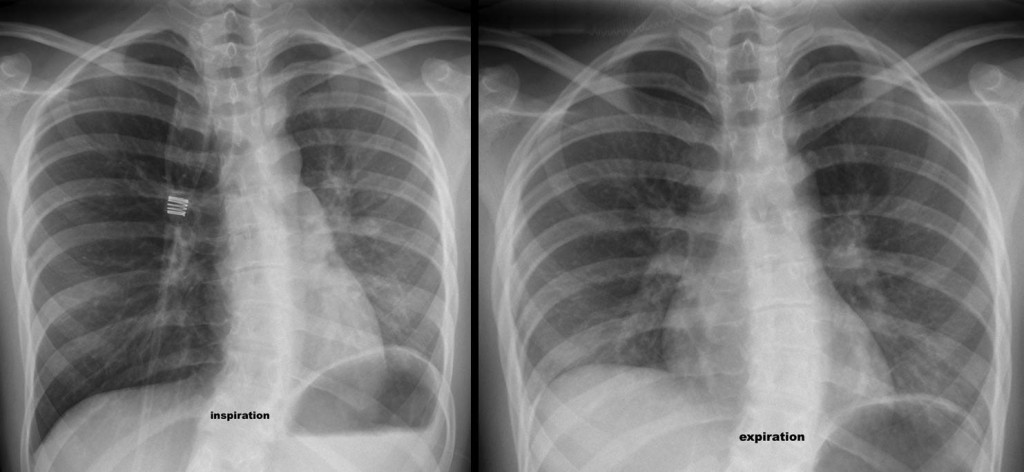
Fig. 1
This appearance is typical of obstruction of the left bronchus: on inspiration air enters in the right (normal) lung, which becomes more lucent and displaces the mediastinum towards the opposite (abnormal) left lung. On expiration, the right lung empties, attracting the mediastinum towards the right side.
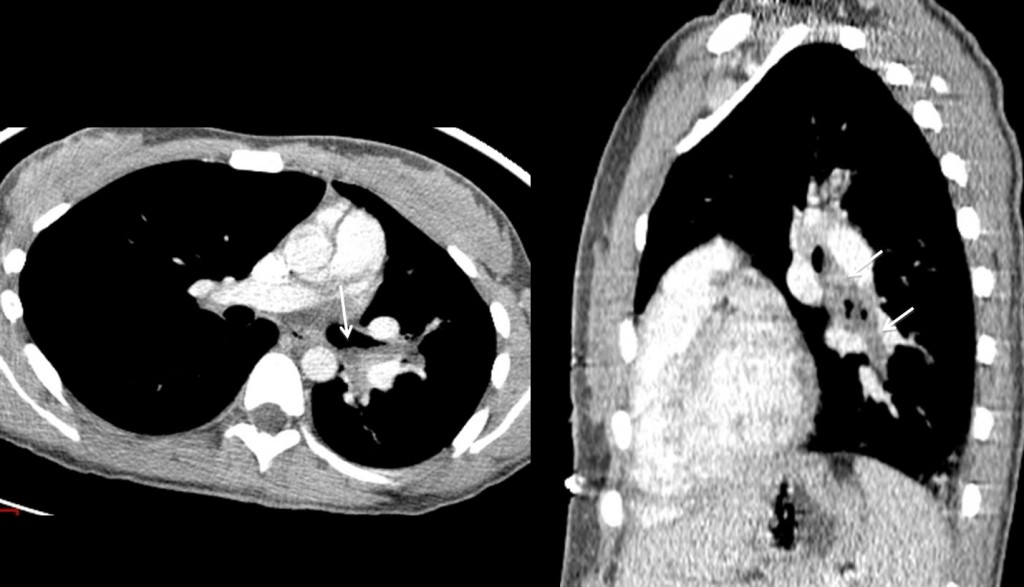
Fig. 2
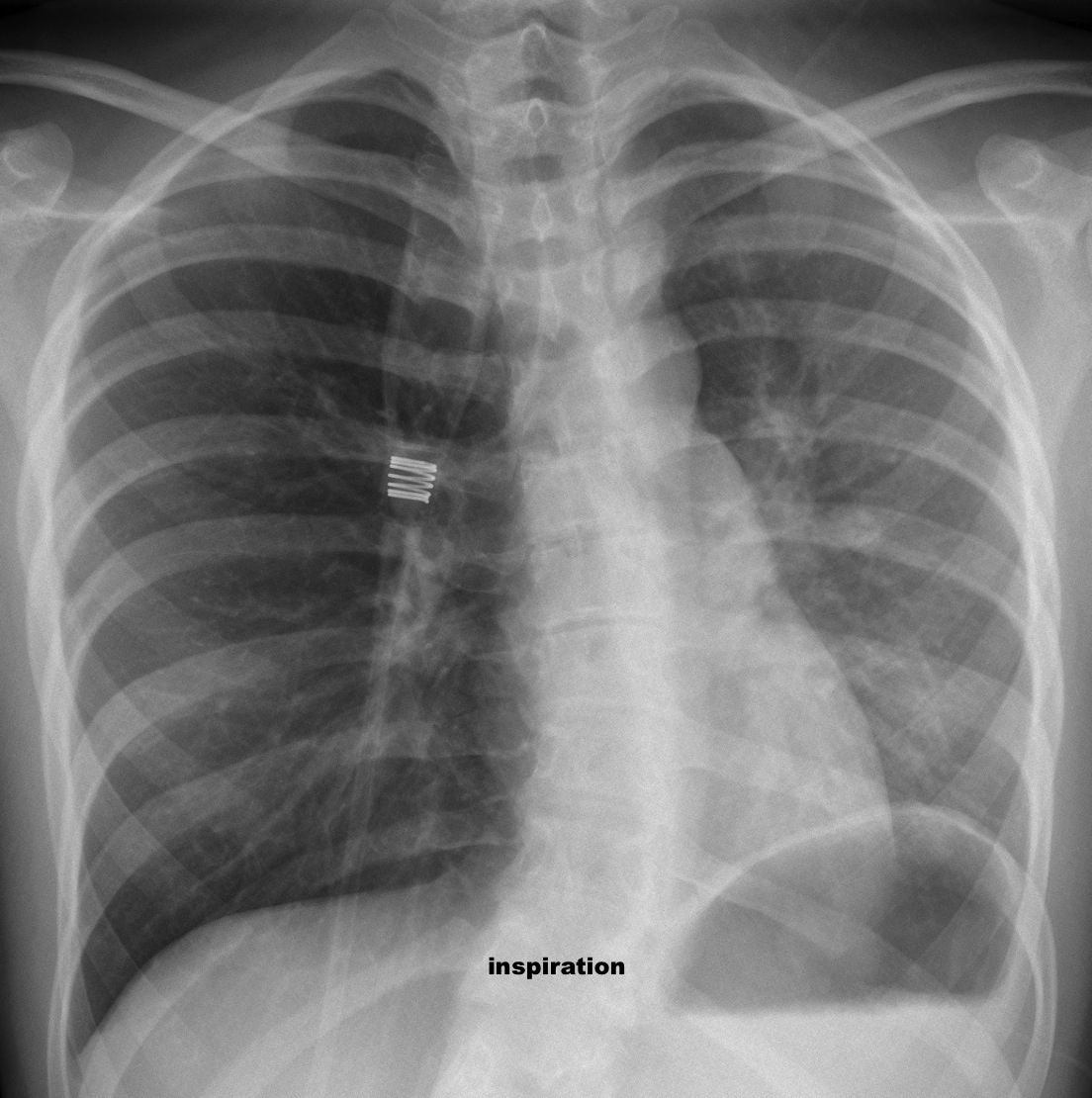
The patient has extrinsic asthma. CT shows obstruction of left bronchus by thick mucus (arrows). She was treated with mucolytics and bronchodilators and the appearance of the chest returned to normal (Fig 3).

Fig. 3
Final diagnosis: obstruction of left bronchus by thick mucus in a patient with extrinsic asthma.
Teaching point: remember that in unilateral bronchial obstruction the mediastinum shifts towards the abnormal lung on inspiration and towards the normal lung on expiration.



something in the left main bronchus
The left lung doesn’t expand during inspiration, probably because of obstruction in the left bronchus. I daresay there is some mucosal thickening which becomes more relevant in the expiration projection, probably because of impairment to the airflow.
Definitely obstruction of the left main bronchus during expiration maybe because of pressure from a vertebra due to scoliosis.
Il problema è a livello della cupola diaframmatica sx che non mostra la normale escursione inspiratoria a causa della sua paralisi.
No bronchial obstruction because no signs of impaired left hemithorax ventilation.
It is as you said Genchi Bari difragmática unilateral paralysis.
Well, three for bronchial obstruction and two for diaphragmatic paralysis!
I would like to join the group in favor of unilateral diaphragmatic paralysis.
There is no air trapping in expiration and the left diaphragm moves upwards in inspiration.
Are you sure that the left hemidiaphragm moves?
If you ask like that I am no longer sure. 😉
Unfortunately I don’t speak Italian. However I read about Holzknecht-Jacobson sign mentioned by Genchi Bari.
Acoording to the literature in bronchial obstruction (foreign body, tumor etc) mediastinum shifts to the healthy side in expiration whereas the abnormal side remains hyperlucent. In Inspiration it will be central.
Only in complete obstruction will the mediastinum shift to the abnormal side in inspiration and remain central in expiration.
A complete obstruction seems unlikely here – the left lung is not atelectatic.
This is confusing. I even considered that the inspiration is actually the expiration but when counting the ribs, this can be ruled out (or not???)
I am looking forward to your explanation – why the mediastinum seems to shift to the wrong side.
The left hemidiaphragm is proyected over the 9th rib in ispiration and expiration. Therefore, it’s not moving. Will talk about inspiration/expiration later (Muppet wants to go out)
OK, a few words about inspiration/expiration. When in the standard PA view (inspiration) one of the lungs is expanded and the other is smaller, we don’t know whether there is air-trapping in the expanded one or bronchial obstruction in the smaller one. The answer is easy by taking an expiratory film: if the expanded lung empties, the abnormal one is the other. If not, the expanded lung is air-trapping.
This is accompanied by mediastinal shift: in expiration, the “good lung” empties and the mediastinum shifts towards it.
To summarize: in inspiration, the mediastinum shifts towards the sick lung (the good lung fills out and displaces the mediastinum). In expiration, the mediastinum shifts away from the sick lung (the good lung empties and attracts the mediastinum). Actually, it is very simple.
Apply this rule to the present case.
Scusami “galactico” ma penso di avere sbagliato con la prima risposta:” senectus ipsa morbus est” (Cicerone).E’ la vecchiaia! Non ho considerato lo “spostamento” del mediastino durante l’inspirazione: esso si sposta a sx.Questo è il segno del “pendolamento” del mediastino o segno diHolznect-Iacobson.Esso indica una insufficiente ventilazione del polmone a causa di una ostruzione bronchiale( adenoma?).Il diaframma omolaterale naturalmente non si abbassa durante la stessa fase inspiratoria!
Good. Wise men know when to change their opinion.
Peccato che il mio inglese è pessimo:avrei così risposto direttamente, alla “dear” Alice.Il segno di H-J è probabilmente riferito ad una condizione di ostruzione “cronica” del bronco principale, mentre gli aspetti che tu, giustamente, menzioni sono riferibili ad un ad condizione di ostruzione acuta.Sentiamo cosa dice il “galactico-blaugrana”!
In inspiration left main bronchus is clearly visible, in expiration only proximal part. Some kind of valve mechanism?
Bronchi tend to narrow their lumen in expiration.
I think the very first answer was right: “something in the left main bronchus”, I men literally: foreing body. This is an acute case of left main bronchus obstruction, because of the clinical presentation (requiring oxygen) and because there is not (yet) hyperlucent left lung (hypoxic vasoconstriction). So, tumor (carcinoid would fit patient´s age) is unlikely.
Mediastinal shift (bamboleo mediastinico), which is intense in this case is not a prominent feature in diaphragmatic paralysis. Here you have a beautiful description of mediastinal shift in these historical articles by McLeod and Swyer and James
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1019360/pdf/thorax00034-0063.pdf
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1019253/pdf/thorax00030-0048.pdf
I like your discussion, except the foreign body part. They usually go to the right lower lobe. Otherwise, well done!
Thanks for the vintage articles