Dear Friends,
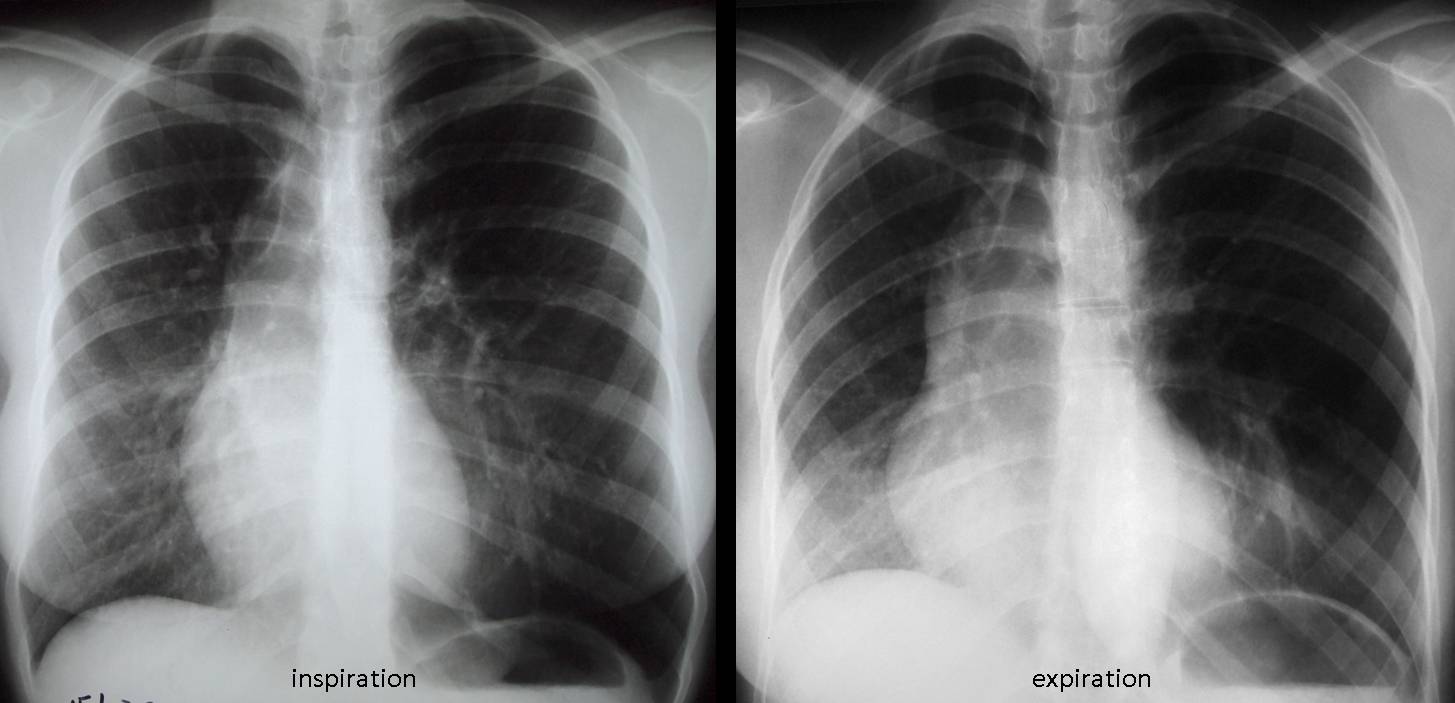
Muppet insists on presenting another case of inspiration/expiration films to test your knowledge. Showing radiographs of a 29-year-old asymptomatic female. What do you think is happening?
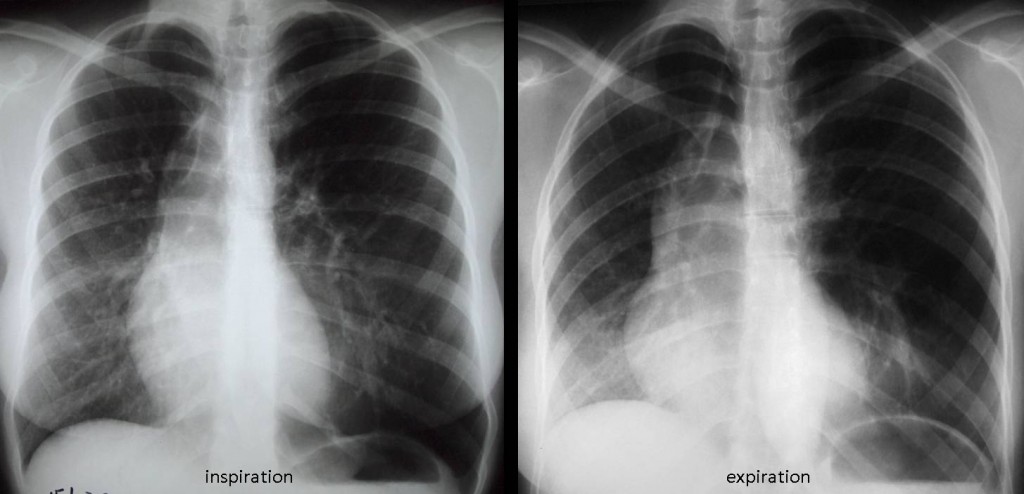
29 y.o. asymptomatic female
Click here for the answer to case #59
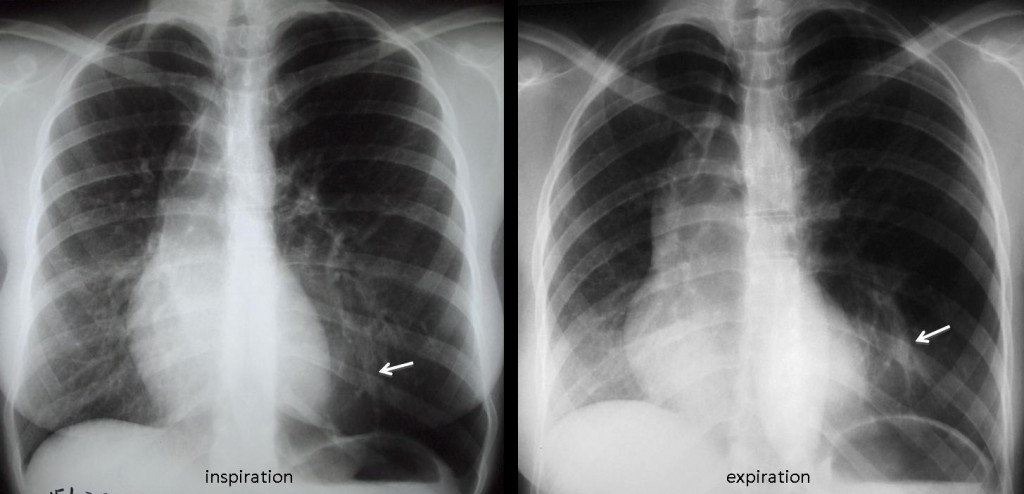
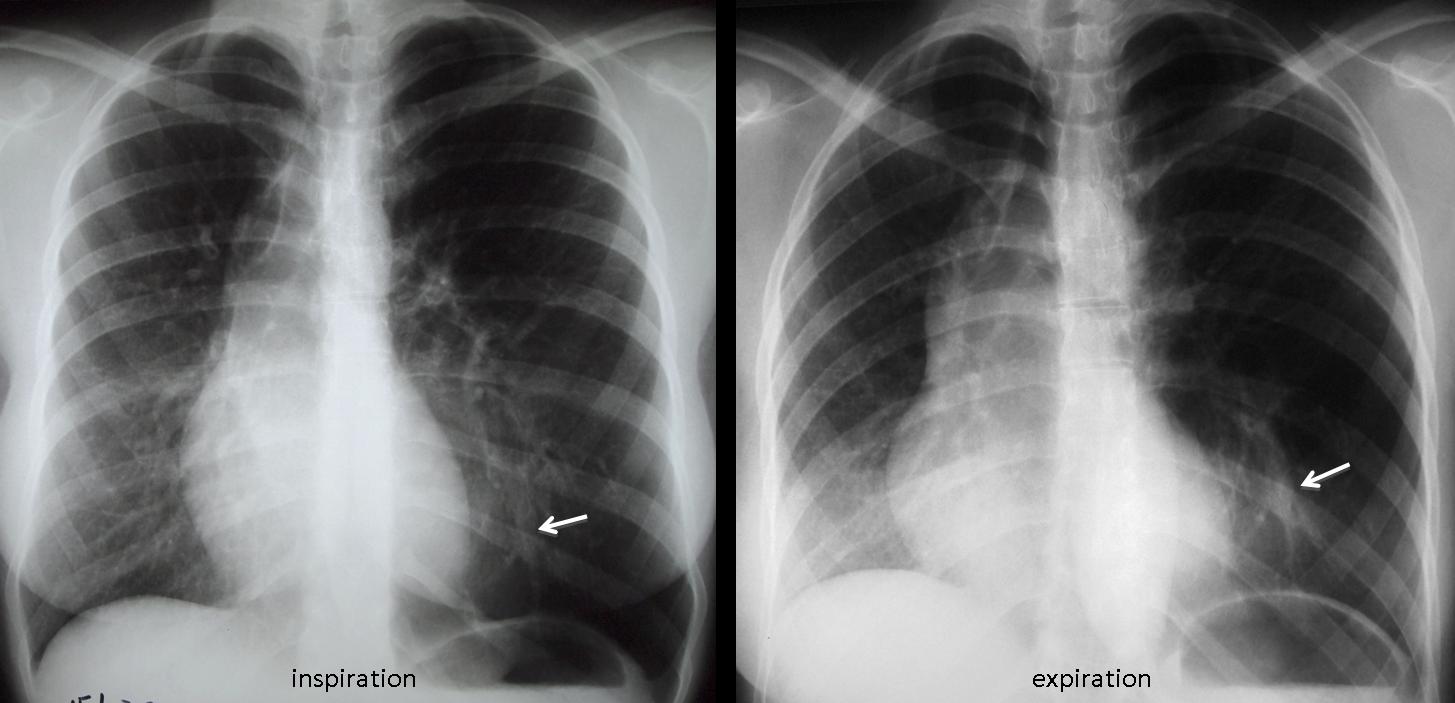
Findings: PA radiographs in inspiration/expiration show hyperlucency of the left lung. The heart is displaced towards the right and there is shifting of the mediastinum towards the right on expiration, confirming air trapping of the left lung. In addition, a tubular structure is visible in the left lower lung (arrow).
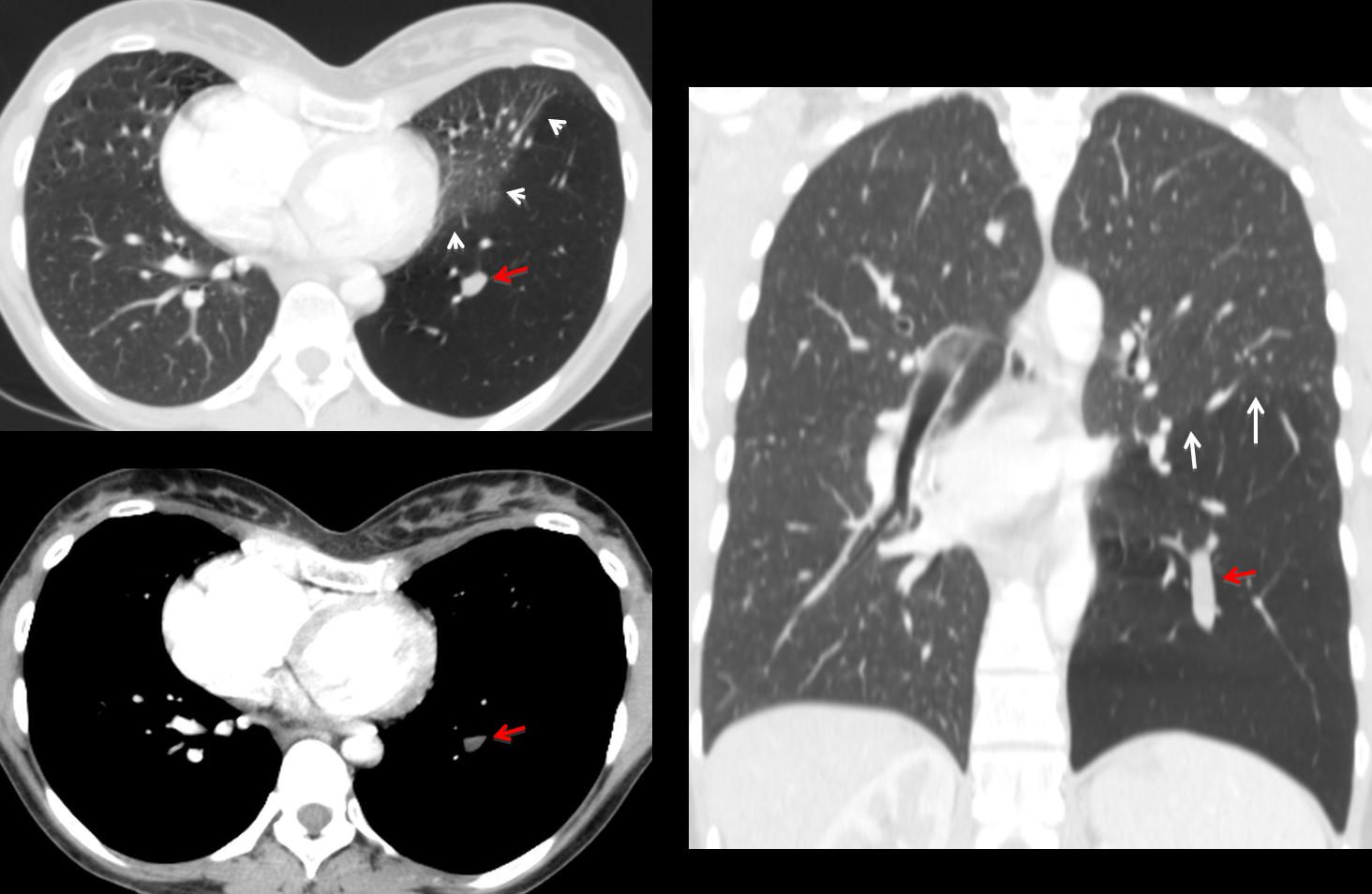
Axial and coronal CT show hyperlucency of the left lower lung, limited by normal upper lung (white arrows). There is a non-enhancing tubular structure in the centre of the left lower lung (red arrows). The displacement of the heart towards the right is due to the expanded left lung plus a marked pectus excavatum.
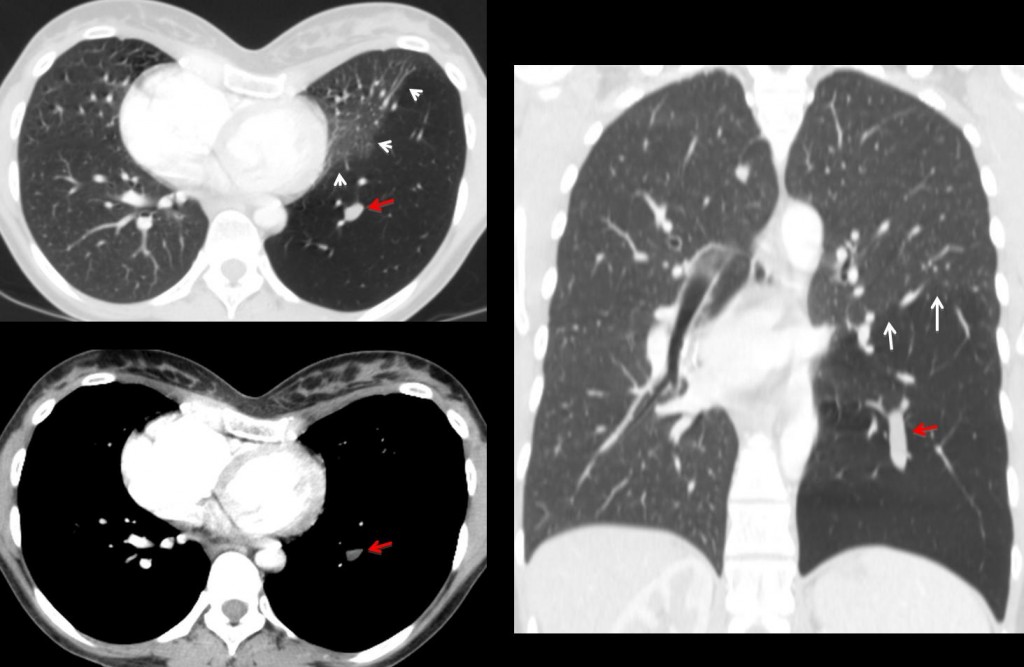
Final diagnosis: Congenital bronchial atresia, left lower lobe.
Teaching point: Congenital lung lesions are not rare in adults. Focal hyperlucent lungs with air trapping and mucous impaction are findings highly suggestive of bronchial atresia.


Probably an Aneurysm of the superior Vena Cava, maybe saccular type. uncommon, but the image in expiration shows the enlargement of right paratraqueal band.
Il polmone patologico è il sx: in inspirazione-espirazione esso si mantiene iperventilato( air-trapping), com mediastino che rimane deviato a dx.L’emidiaframma sx rimane immobile a livello della X costa, posteriormente.Il bronco principale di sx sembra avere un calibro inferiore al controlaterale:broncomalacia?
CXR frontal views in inspiration and expiration of asymptomtic 29 years old female revealed :
unilateral hyperlucent left sided lung that is persistent during both inspiration and expiration , with contralateral shift of the mediastinum to the right side .
the left hilar vessels are abnormal , replaced with multiple dispersed vessels .
so there is no air trapping causing left lung hyperlucency but abnormal decreased vascularity may be the cause .
so swyer James McLeod syndrome is diagnosis .
so
.
there is some mediastinum shifting on inspiration which is getting larger in expiration. moreover there is air in both sides of trachea wall (maybe some mediastinum air). air trapping and fistula?
air trapping Swyer and James?:)
but there is not hipoplastic lung sorry….
mediastinal shift towards right in inspiration can be explained by a tension pneumothorax (there is not clear vascular marking in the left base as far as i can see), but if patient is asymptomatic then this is very unlikely.
Moreover the aortic arch is strikingly right sided and i wonder if there is any associated bronchial anomaly to explain the airtrapping in the left lung during expiration.
Look carefully at the left lung
Both lungs are hyperinflated. Very reduced vascular shadows in most of left lung (there is only a small paracardiac sound portion of lung) and in RUL. Left hilum is small. At expiration both diaphragms go upwards, but very little (one intercostal space) so there is some bilateral air trapping. Mediastinal shift increases a little to the right (the less affected lung). I think Gus is right and we have a McLeod-Swyer-James syndrome (bronchiolitis obliterates). Somewhat tricky because both lung are involved although in different proportion. The only differential I can imaging is antitrypsin deficiency panlobular emphysema, but you should expect enlarged hila.
Rml atelectasis, the trachea and the midline is pulled to the rigt in both inspiration and expiration.
mediastinal shift towards right during expiration represents air trapping in left lung.
Paucity of bronchovascular markings and hyper-lucent left upper lobe along with some mediastinal shift towards right seen in inspiration phase. There is increase in mediastinal shift towards right more marked in upper half of mediastinum along with hyper-lucent left upper lobe noted during expiration most likely represents congenital lobar emphysema.
Thank you for clarifying the last case. I really appreciated your response and Genchis response, too!
In this New case the Sick lung Seems to be on the left, with Diminished vascularity and Hyperinflation. The right lung Is larger in Inspiration and smaller in expiration, explaining the mediastinal shifting. I really Hope i got it right this time.
In Swyer James the affected lung Is supposedly the smaller one (although the above mentioned criteria are otherwise a good fit).
How about Congenital lobar emphysema (rare in adults)?
Yes, you got it right this time. Congratulations. But you are missing one finding. As I said above, look carefully at the left lung
i cannot identify the left pulmonary artery
on the other hand if it was missing i would expect the left lung to be smaller.
but a congenital problem is most likely – patient is asymptomatic.
You are right about the congenital problem. Answer next Tuesday
Following your advice (look to the left lung) and advances made by Alice, there is a tubular structure at left base on expiration. Could that be a bronchocele (bronchial atresia) ?
Yes. Congratulations
Quindi l’air-trapping del polmone sx è dovuto alla ventilazione secondaria attraverso i pori di Khon , dai territori normalmente ventilati.Grazie, mitico!PS. il Bari si sta salvando dalla retrocessione in C.
great case profesor Caceres…
Muppet is the mastermind. I just follow his orders