Dr. Pepe’s Diploma Casebook: Case 103 – To err is human: how to avoid slipping up (Chapter 2) – SOLVED!
Dear Friends,
Today I am presenting radiographs of a 30-year-old man. They were taken because an abnormal ECG was found in a routine check-up. What do you see?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.


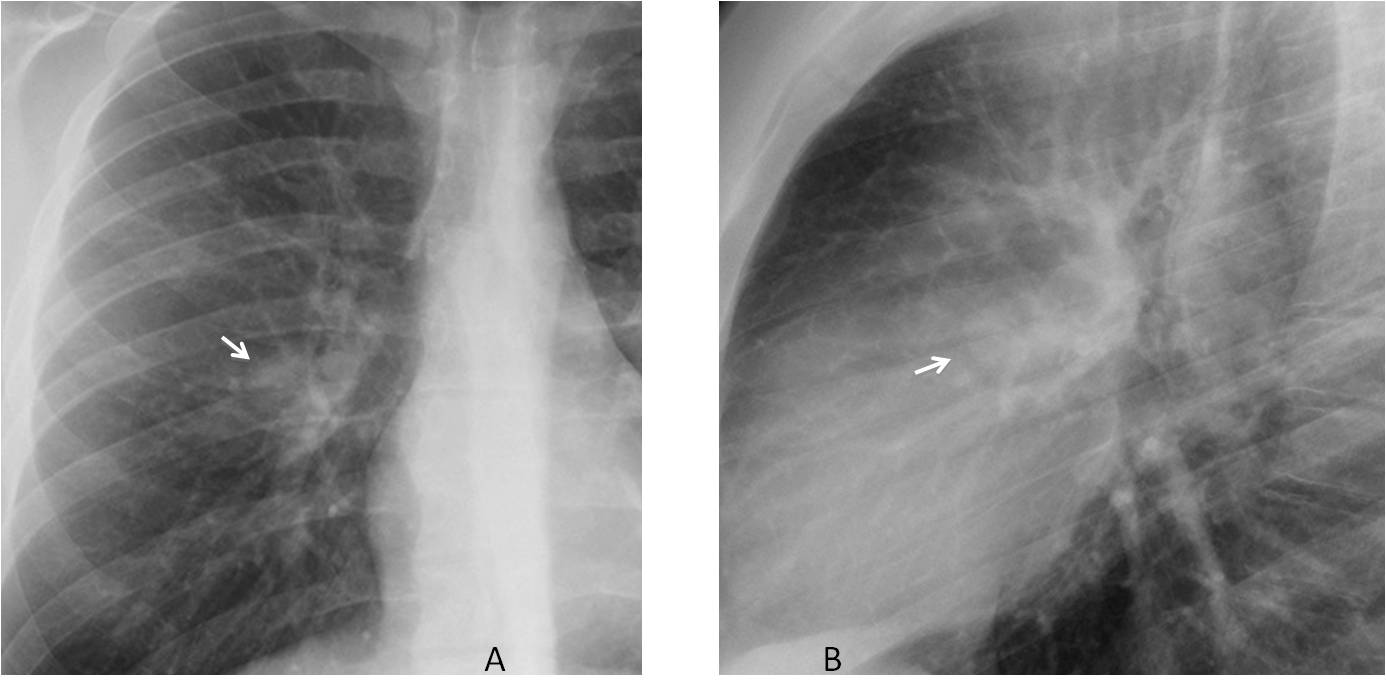
Findings: Chest radiographs show a rounded mass in the right hilum (A and B, arrows), that was overlooked in this examination. Five months later the patient discovered a swelling in his left foot which was diagnosed as malignant mesenchymal tumour.
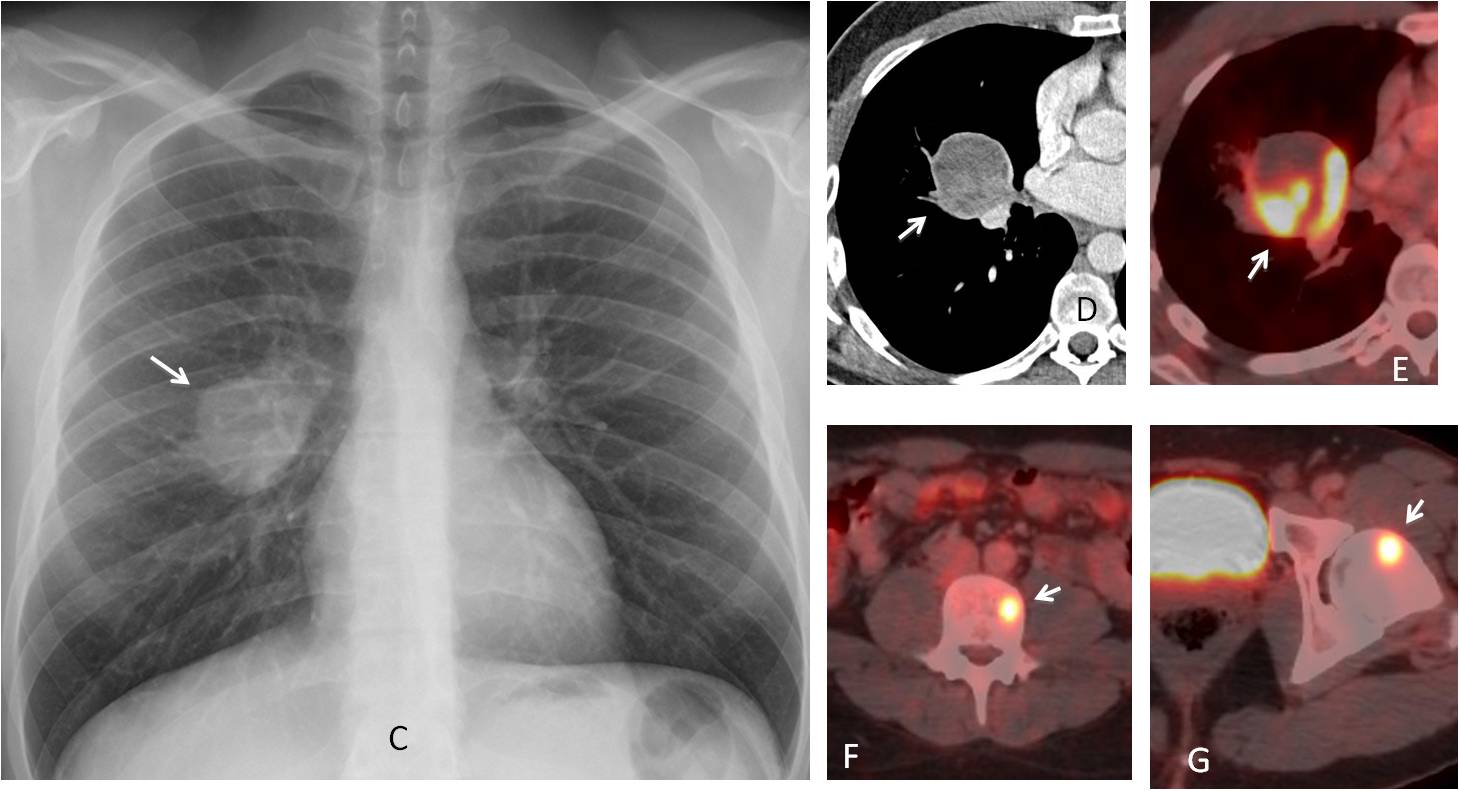
A repeat chest radiograph showed a marked increase in size of the hilar mass (C and D, arrows). PET-CT confirmed increased uptake of the mass and bone metastasis (E-G, arrows).
In the second chapter of “To err is human” I plan to analyse perceptual errors, the most common ones, accounting for up to 50% of errors committed by radiologists. For a variety of reasons, in this type of error the radiologist does not see the abnormality, which may be obvious or subtle.
In this presentation I will discuss missed obvious abnormalities. They are defined as those that are clearly visible in the chest radiograph in retrospect. Distraction, fatigue, multitasking, etc. are some of the causes of this type of error. They can be summarised in the vernacular as: “shit happens”.
Although obvious errors cannot be avoided completely because they depend on circumstances beyond our control, they may be minimised by carefully examining certain areas:
1, The hilar regions
2. The cardiac shadow
3. Visible lung included in images of adjacent chest organs
The hilar regions are a conflictive area and they may hide significant pathology, as demonstrated in the initial case. They should be scrutinised in the PA view. The lateral view is of great help, not only discovering intrinsic hilar pathology, but detecting lesions in front or behind them (Figs 1-2)
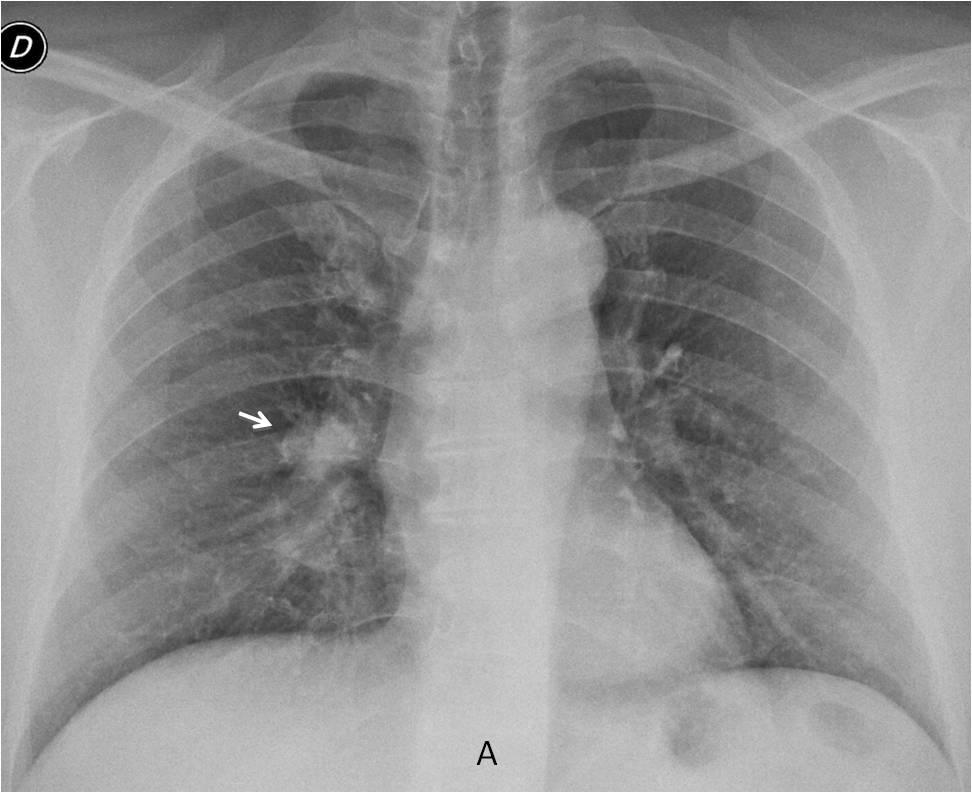
Fig. 1
Fig 1. Preoperative PA radiograph for hernia in a 64.year-old man. There is a nodule in the right hilum that was overlooked (A, arrow).
Review of the initial chest film prompted a repeat examination, including a lateral view, which confirmed a nodule behind the right hilum (B and C, arrows). Diagnosis: carcinoma
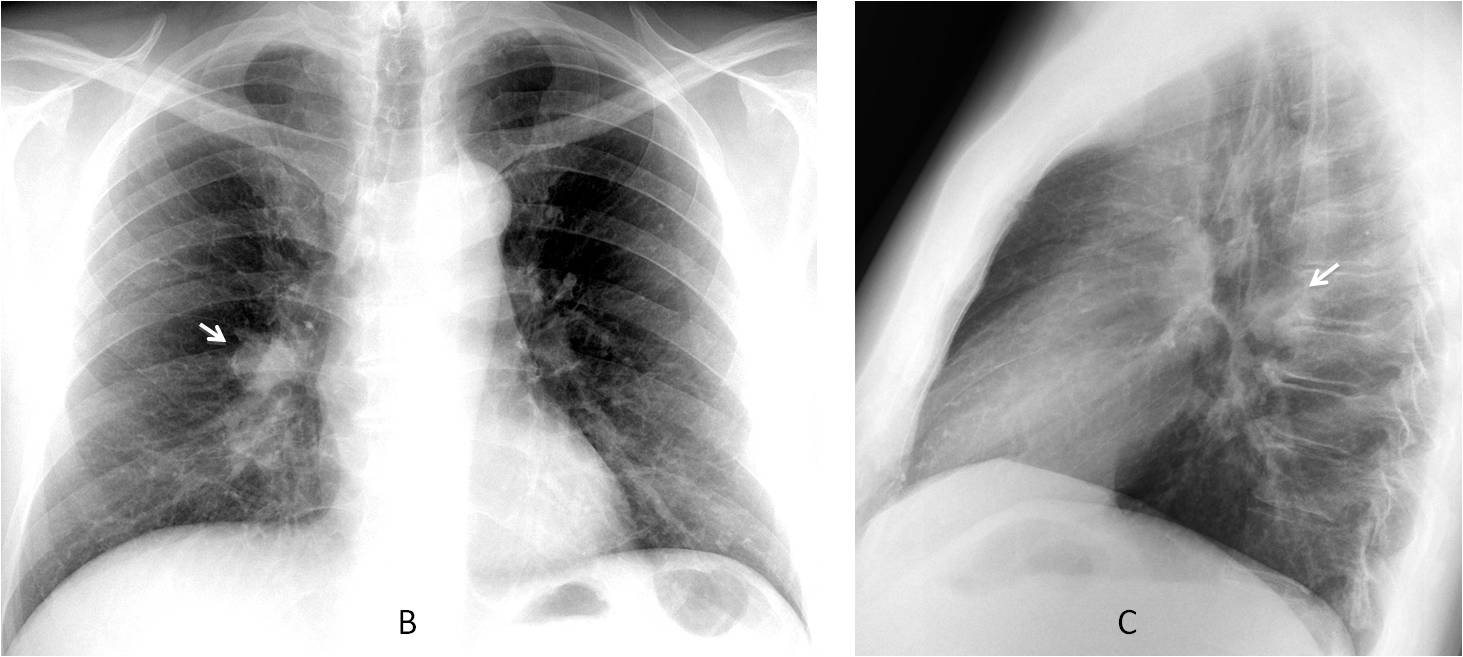
Fig. 1
Perceptual errors affect all of us. I saw the case below one month ago and noticed the abnormality in the lower part of the left hilum (Fig. 2). As usual, I checked with previous examinations and discovered that it was not mentioned in previous reports, one of which was mine. So whoever is free from error may cast the first stone!
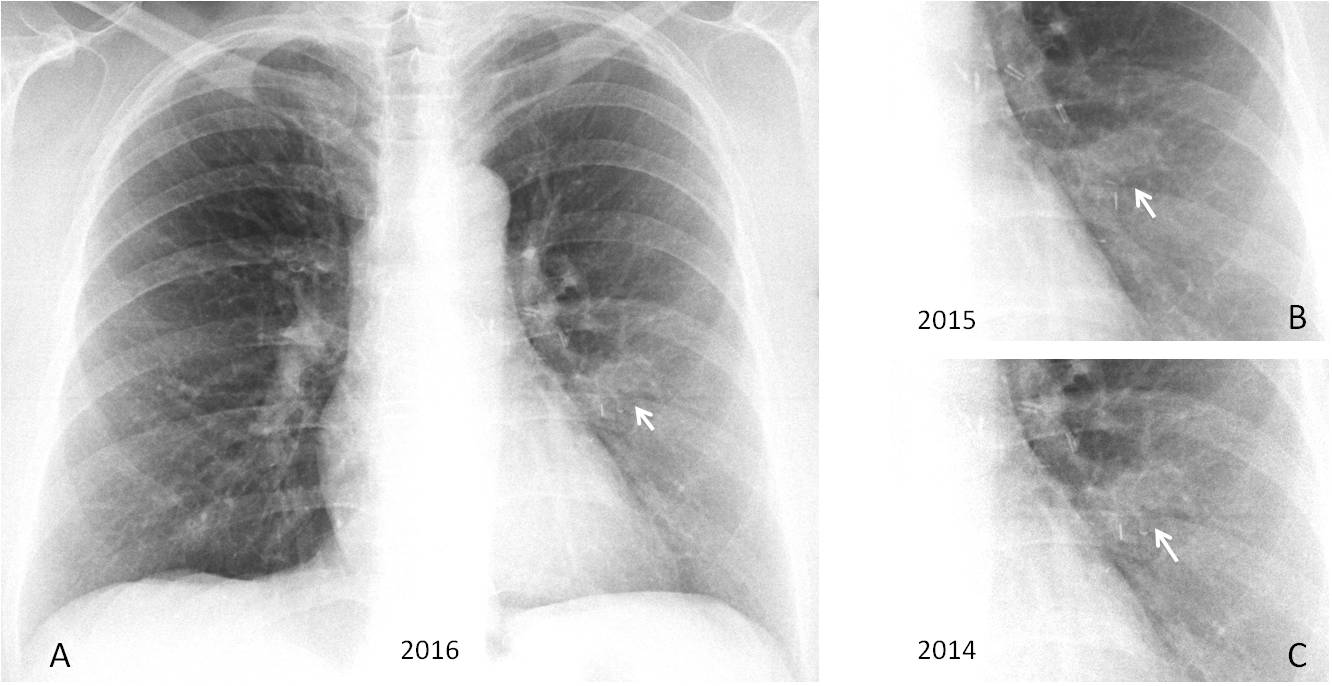
Fig. 2
Fig. 2. 53-year-old woman. Routine follow-up radiography for breast carcinoma. There is an elongated opacity adjacent to the left hilum (A, arrow) that was not mentioned in previous reports (B and C, arrows).
Axial and coronal CT show that the opacity represents an elongated calcification in the left mid field (D and E, arrow). The branching suggest a calcified mucus impaction (unproved).
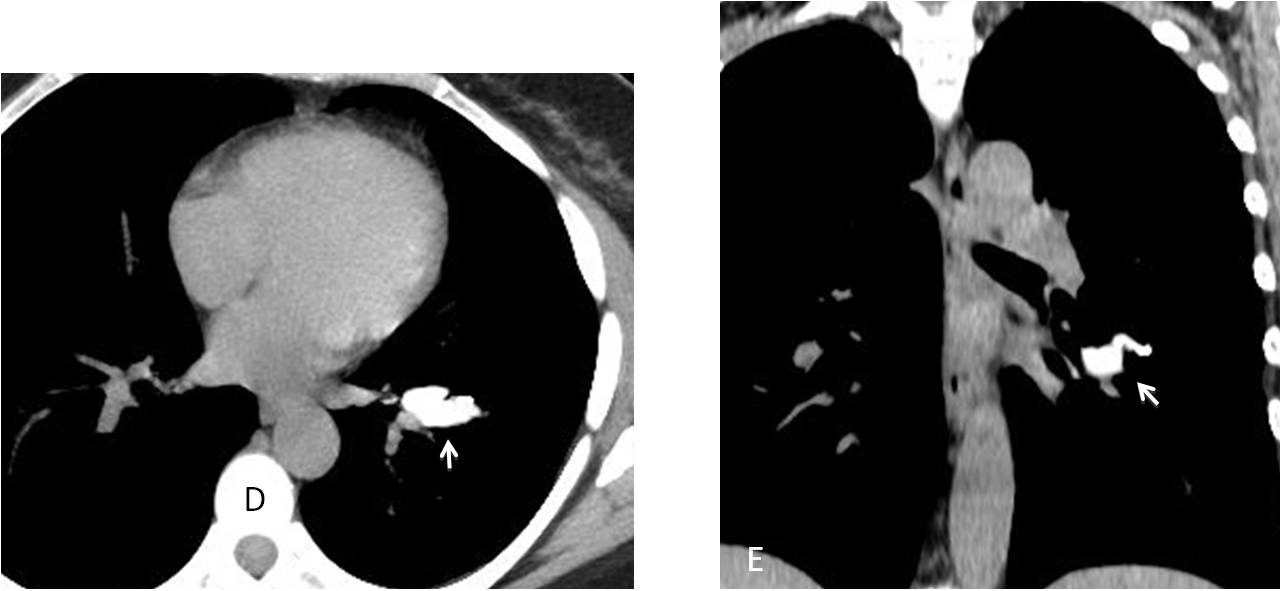
Fig. 2
The heart covers a significant area of the chest radiograph. A careful examination of the entire silhouette facilitates discovery of lesions around or behind the cardiac shadow (Figs. 3 and 4).
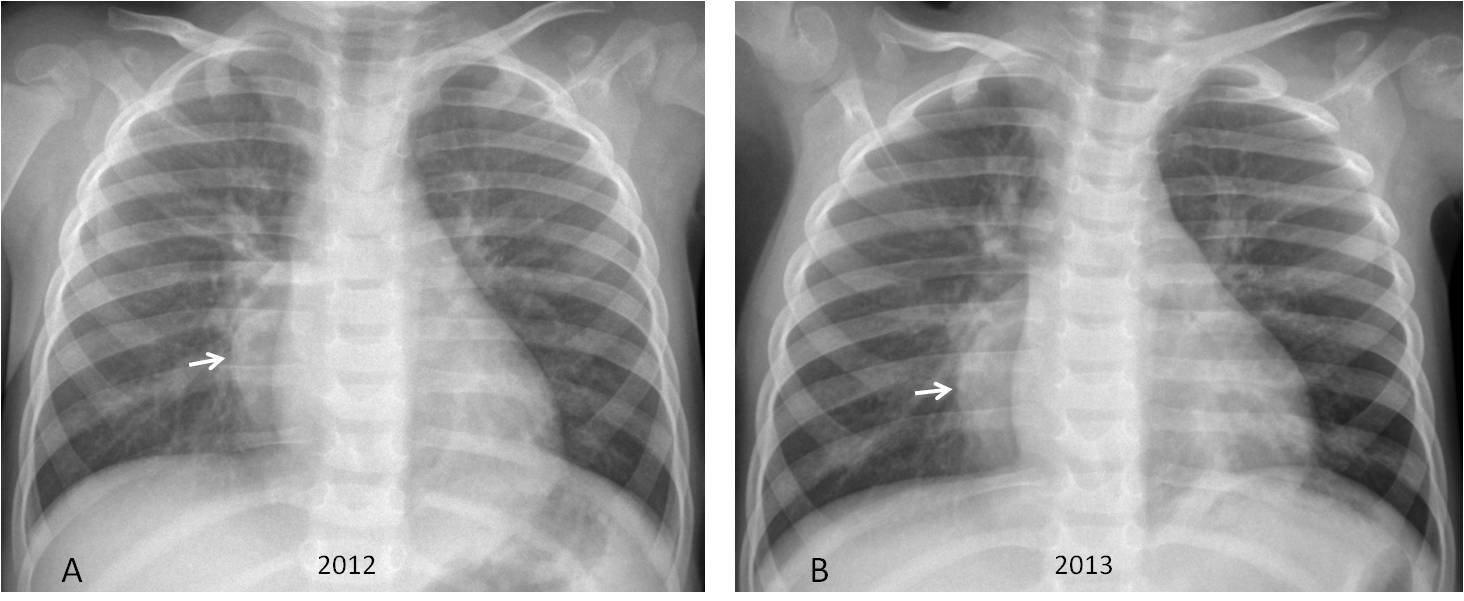
Fig. 3
Fig. 3. Seven-year-old boy with a history of pneumonia in two consecutive years. The radiologist missed a right posterior mediastinal mass paralleling the right heart border (A and B, arrows).
Three years later the mass has grown considerably (C and D, arrows). Diagnosis: neuroblastoma
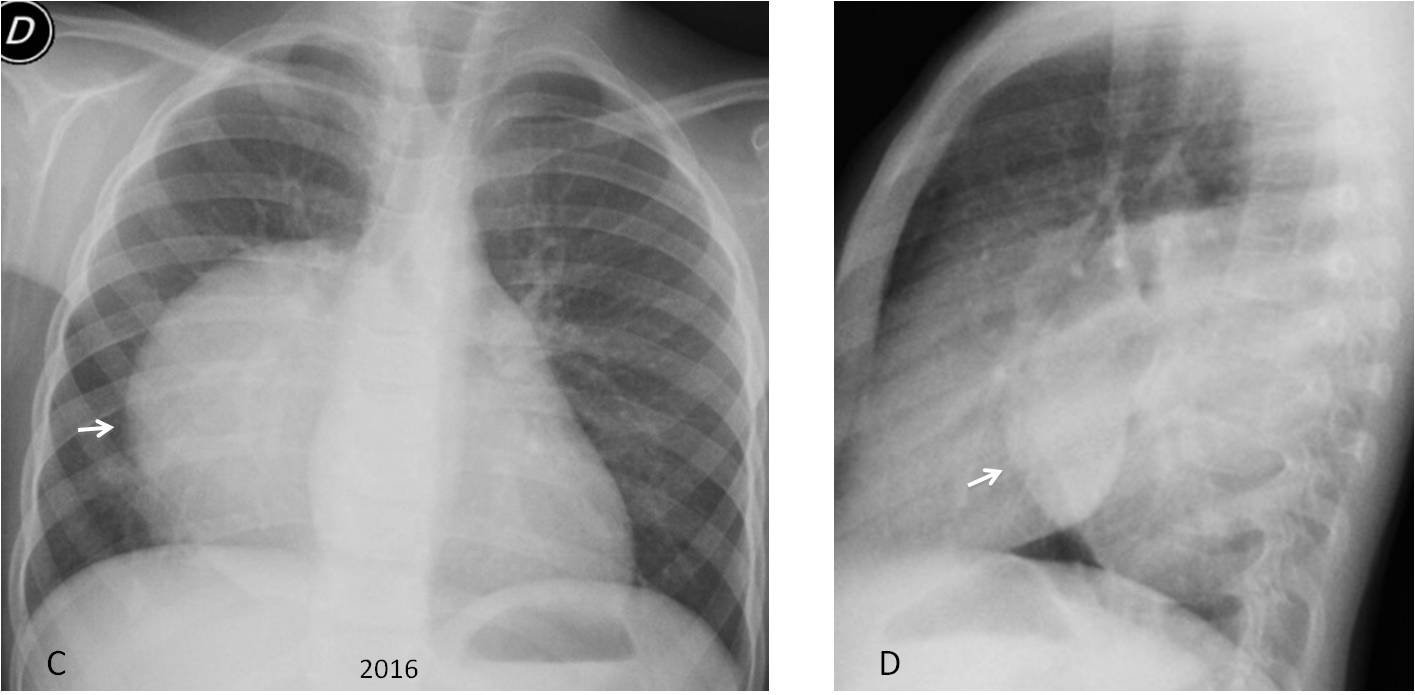
Fig. 3
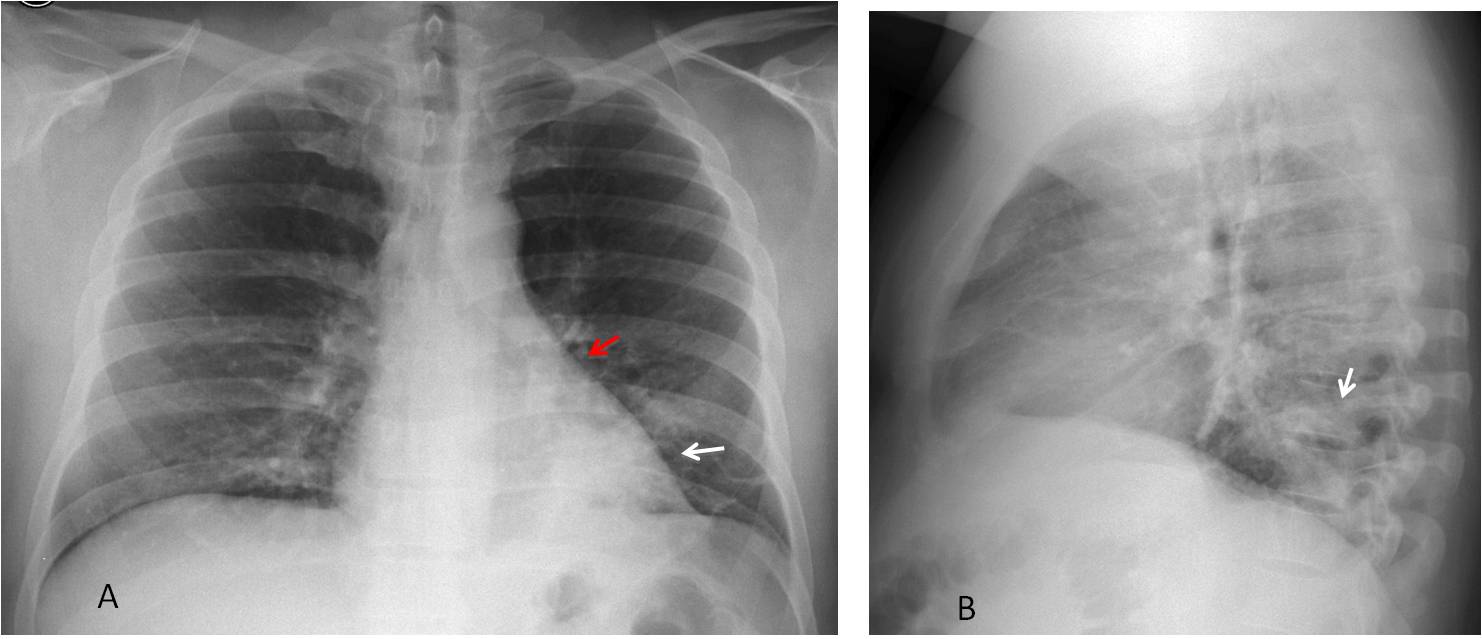
Fig. 4
Fig. 4. 41-year-old man with cough and mild fever. Chest radiographs taken in 2009 show a peripheral opacity in the RLL (A and B, white arrows). There is marked downward displacement of the left hilum (A, red arrow), indicating volume loss.
Hilar displacement was overlooked and the patient did not have new radiographs until February 2013, which showed obvious LLL collapse (C, arrows). CT confirms marked collapse of the LLL (D and E, white arrows) secondary to an endobronchial lesion (D, red arrow), with fat in the center (E, red arrow). Diagnosis: endobronchial hamartoma resulting in lobectomy.
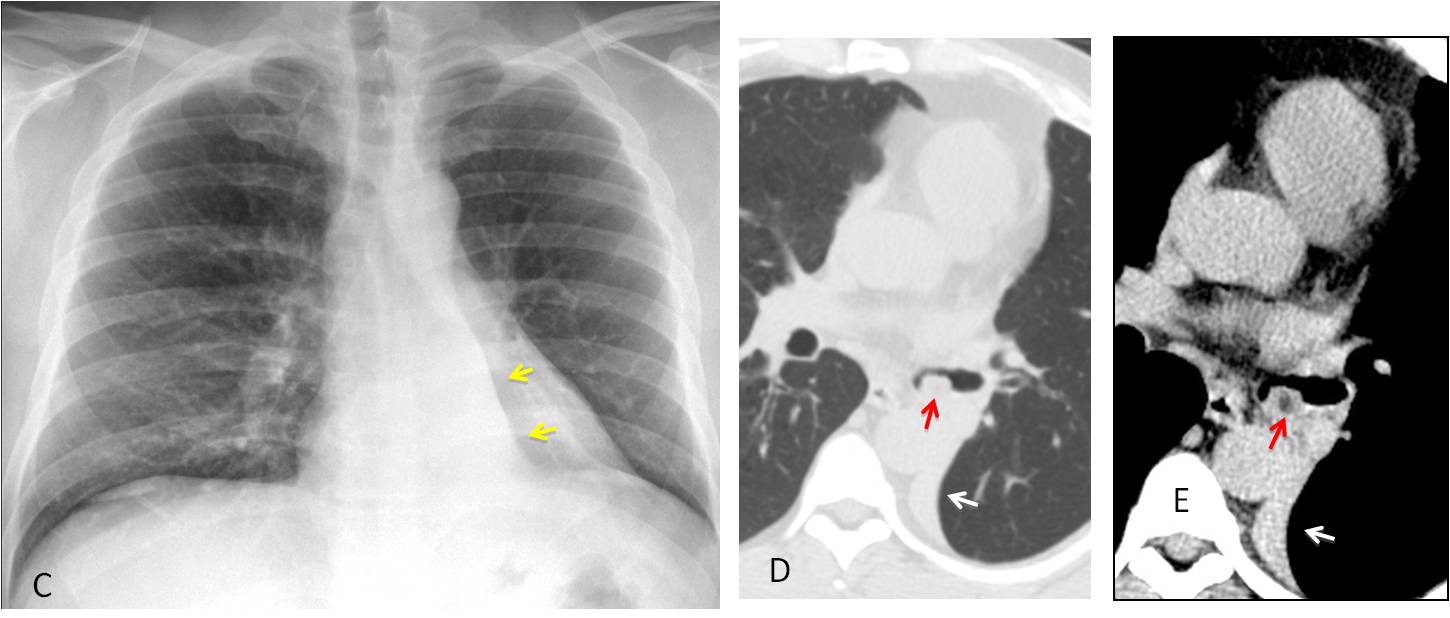
Fig. 4
A common cause of missing obvious lesions results from overlooking the lung included in radiographs of peripheral chest organs (neck, upper extremities, abdomen). A well-known example is missing a Pancoast tumor in cervical spine radiographs for neck or shoulder pain, but it may occur in other areas as well (Figs. 5 and 6).
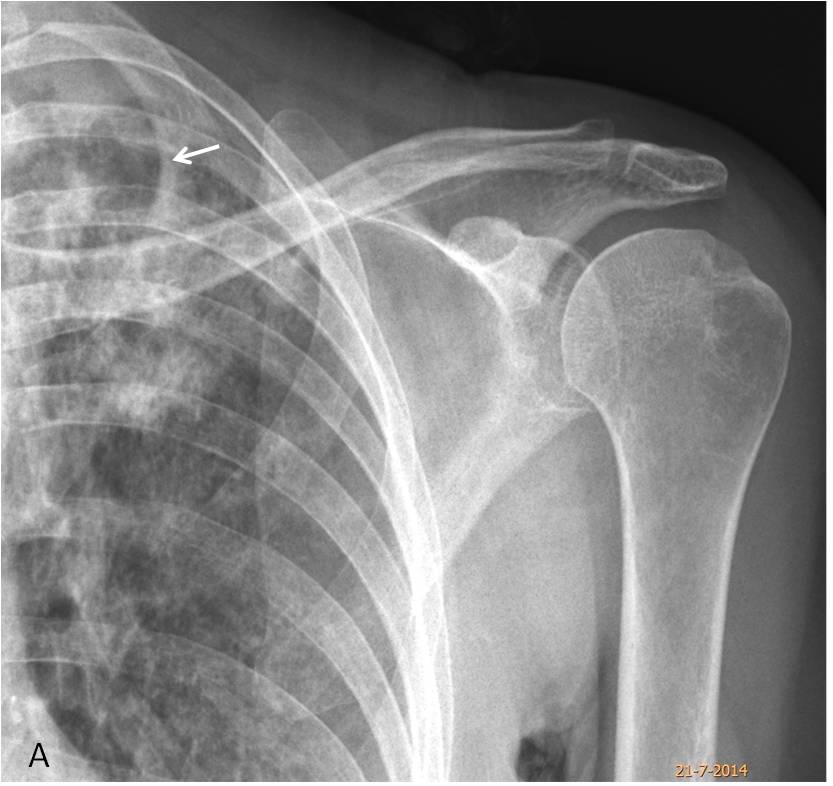
Fig. 5
Fig. 5. 71-year-old woman with shoulder pain. The cavitated infiltrate in the RUL went undetected in the shoulder radiograph (A, arrow).
Six months later a preoperative film for a vocal cord nodule discovered extensive bilateral
infiltrates with cavitation, confirmed with CT (B and C, arrows). Diagnosis: paucisymptomatic TB affecting the lungs and vocal cord.
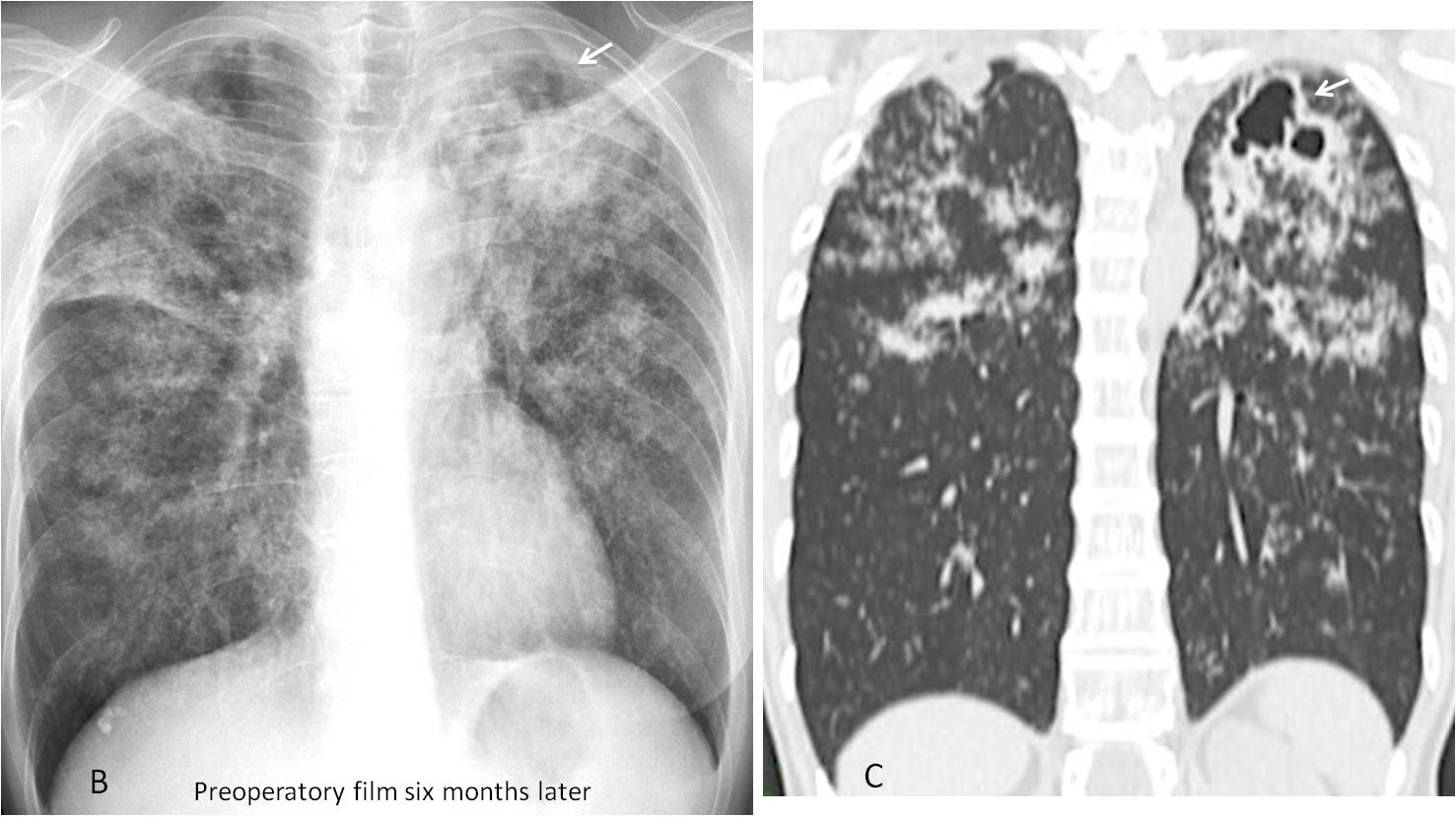
Fig. 5
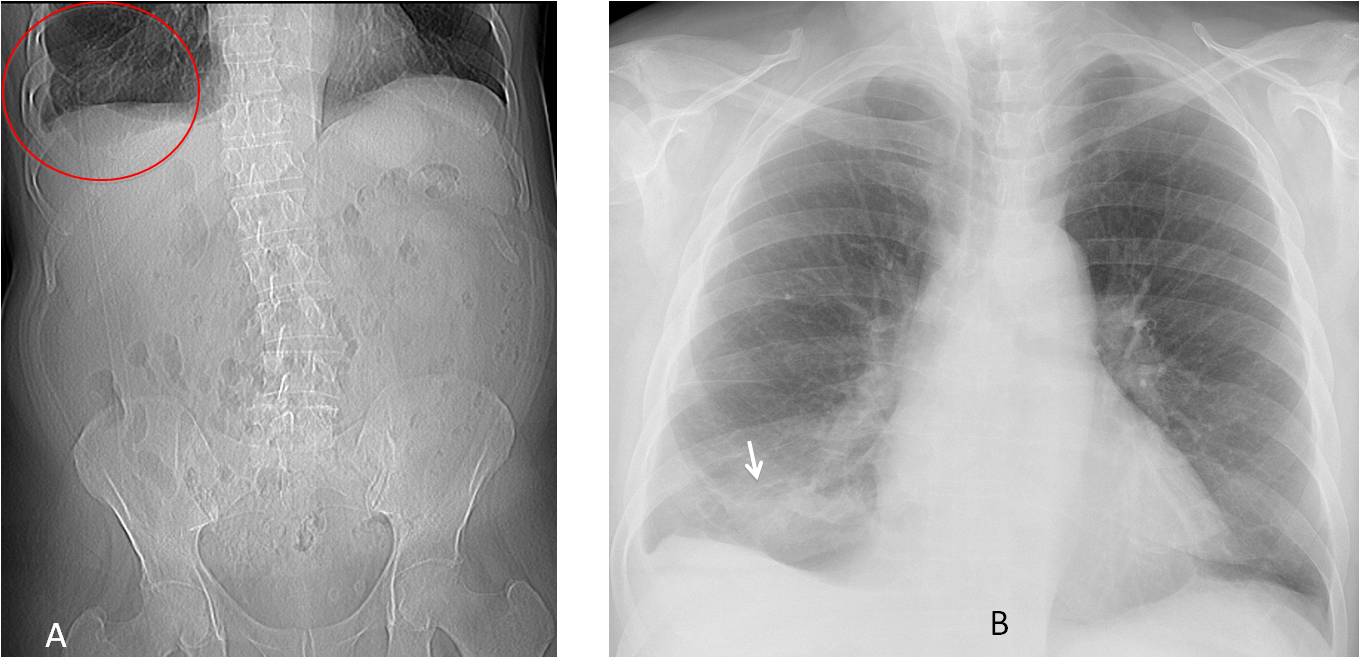
Fig. 6
Fig. 6. 75-year-old man with a history of renal calculi. An abdominal radiograph (which was lost and is replaced here by a scout film), showed changes in the lower right lung (A, circle). A chest radiograph was taken, confirming a basal pulmonary infiltrate (B, arrow) and small pleural effusion.
Axial CT shows an endobronchial lesion in a segmental bronchus of RLL (C, arrow). The lesion has fat density (-89 HU) (D and E, arrows). Final diagnosis: endobronchial lipoma, discovered accidentally and confirmed by biopsy. The patient had no significant respiratory symptoms.
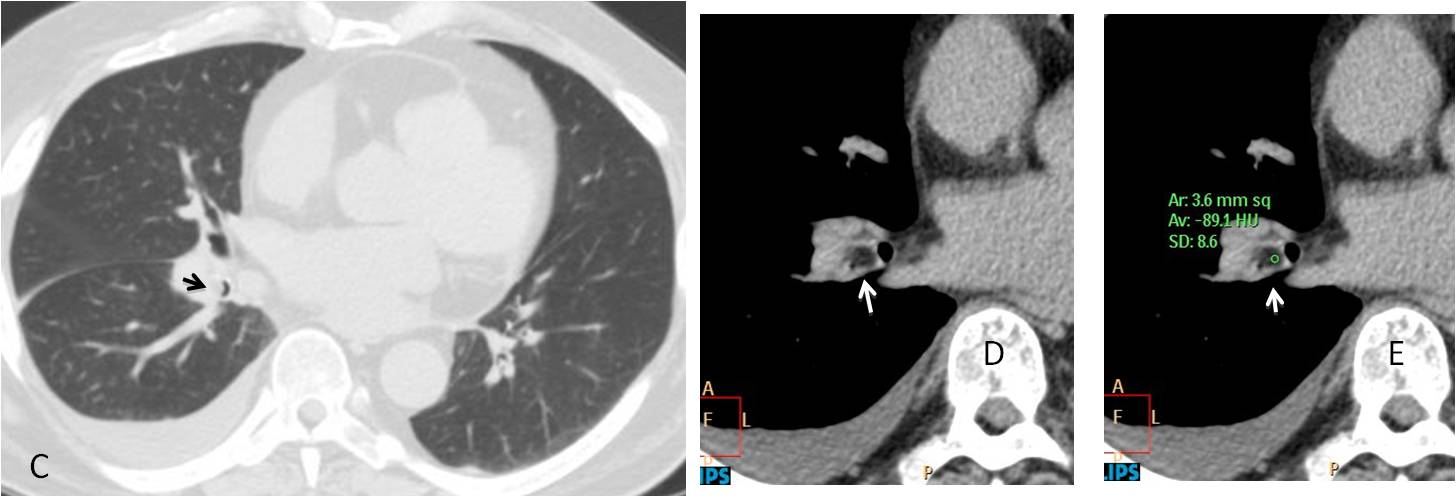
Fig. 6

Follow Dr. Pepe’s advice:
Obvious errors of perception are difficult to avoid
They can be minimised by :
- Paying special attention to the hilar regions
- Looking behind and around the heart shadow
- Examining the lung in radiographs of peripheral chest organs


Good morning!!!
In the lateral view there is an extrinsic compresion of the inferior trachea/left principal bronchus.
There is a flatened of the left hemidiaghram with a traction of its anterior portion.
Juxtaphrenic peak or diaphragmatic tetin sign
Second look:
Enlarged right hilum with a nodular appearence in the lateral view and loss of volume of this hemithorax with right juxtaphrenic peak sign?
Hi! in my opinion there is a defect with the big vessels of the heart and their contours. I mean I cannot really separate the borders of aortopneumonic winndow, of the aortic arch and furtheremore I cannot define the whole margin of right pulmonary artery. So, maybe there a displastic aortic arch? or a misposition of vessels and their origin? I would like to see a CT with contrast medium.
Hi!
I think there is an enlarged right hilum compared to the left one.
Good morning, professor! Could we say there is an enlargement of right paraspinal line in PA x ray? We think right hilum is not well defined in PA and lateral view. Pulmonary artery anomaly?
Good evening professor.
Figure of 3 indentation of aorta and subtle rib notching, suggestive of aortic coarcitation.
Coarctation of aorta with rib notching
….l’insegnamento del Professore è quello della DD tra opacità parenchimale o vascolare , alla lettura del radiogramma standard….opacità in sede ilare dx…
Congratulations to all of you who said that the right hilum was enlarged, especially Y.E. and UFTM radiogroup, who were the first ones.
Final answer tomorrow
Interesting case and interpretations
Hi,
a faint round density anterior to the right hilum can be seen on the lateral view, in the mentioned clinical context, i suggest a vascular malformation.
thanks
So, maybe there a displastic aortic arch? or a misposition of vessels and their origin?