Dr. Pepe’s Diploma Casebook: Case 104 – To err is human: how to avoid slipping up (Chapter 3) – SOLVED!
Dear Friends,
Today I am presenting chest radiographs taken during a routine check-up of a 60-year-old woman. Radiographs were read as normal. What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.


Findings: There is doubtful enlargement of both hila, suggesting enlarged lymph nodes. Confirmation is provided by the convexity of the aorto-pulmonary window in the PA radiograph (A, arrow). Enhanced coronal CT shows a large lymph node at the aorto –pulmonary window (B, arrow). Axial CT confirms the presence of hilar nodes (C, arrows).
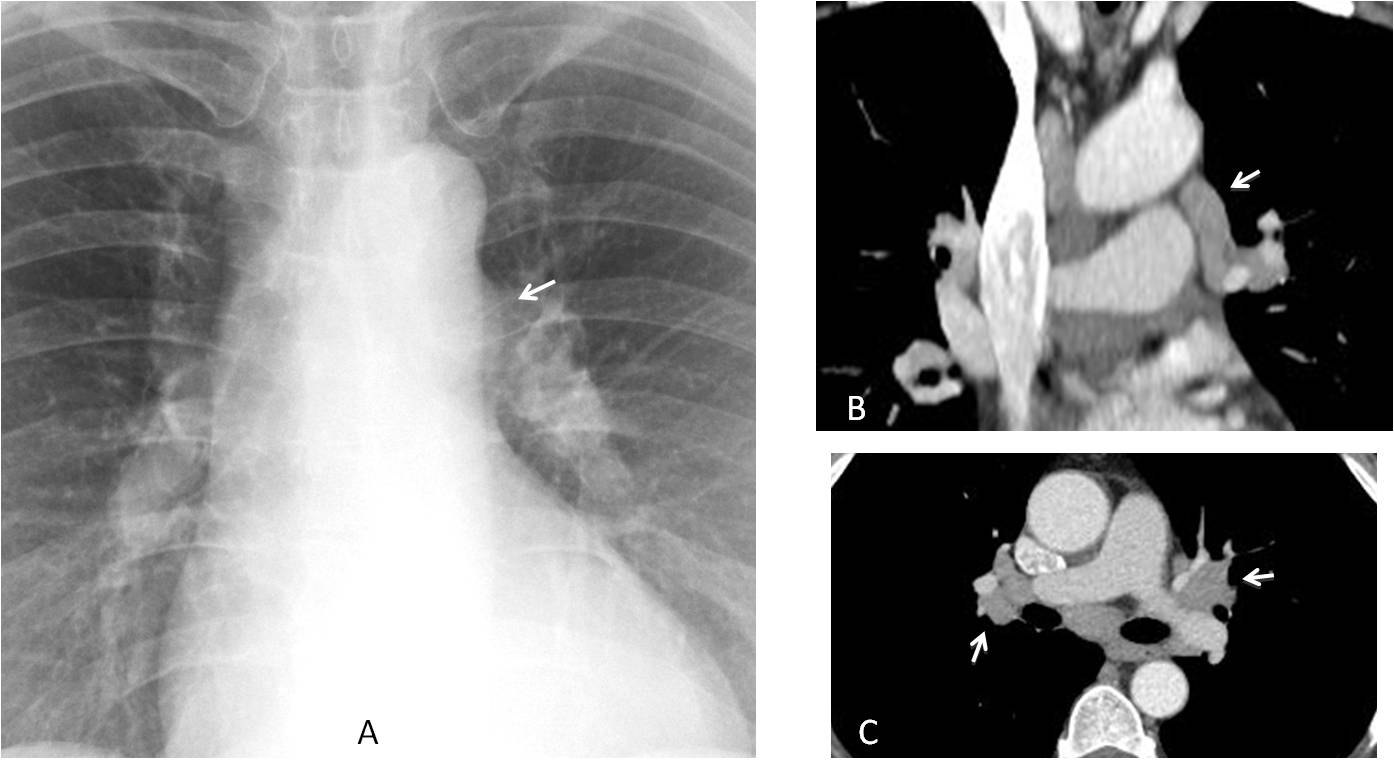
Final diagnosis: sarcoidosis
In the past chapter of “To err is human” I presented perceptual errors, analysing the obvious ones. Today I will discuss missed subtle abnormalities, which are ones that are easily overlooked. This type of error can be avoided if we get into the habit of using checklists.
A basic outline of checklists was described in Diploma cases 98 to 101. In this presentation I want to emphasise the areas where, in my opinion, it is more common to miss subtle abnormalities:
PA radiograph:
Apical regions
Mediastinal borders
Lateral radiograph:
Thoracic spine
It is not uncommon to overlook lesions in the lung apices because the numerous bone structures in this region impede visualisation of the underlying lung. Pulmonary nodules are often missed in the initial chest radiograph; the reported missing rate is as high as 60% (Figs. 1 and 2).
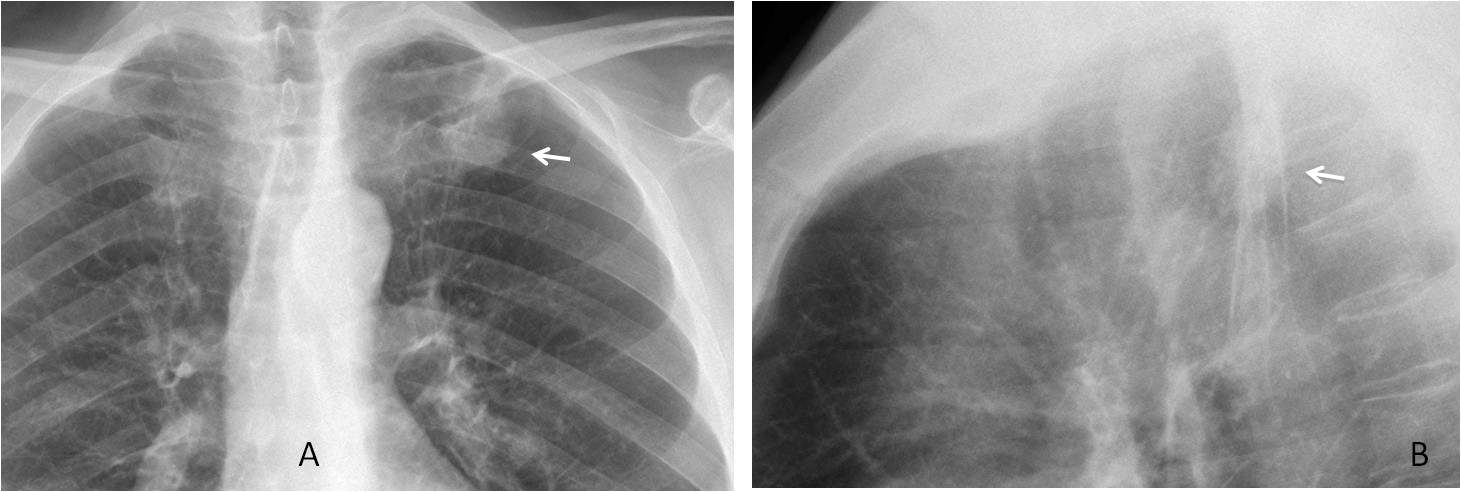
Fig. 1
Fig. 1: 54-year-old man with mild chest complaints. There is nodule over the anterior left rib (A, arrow) that was missed in this exam. The nodule is visible in the lateral film in the Raider triangle (B, arrow). It was also missed in this view.
One year later, the nodule has increased markedly in size (C, white arrow) and a second mass has appeared in the right lung (C, red arrow). Enhanced coronal CT confirms the findings (D, arrows). Final diagnosis: double lung carcinoma
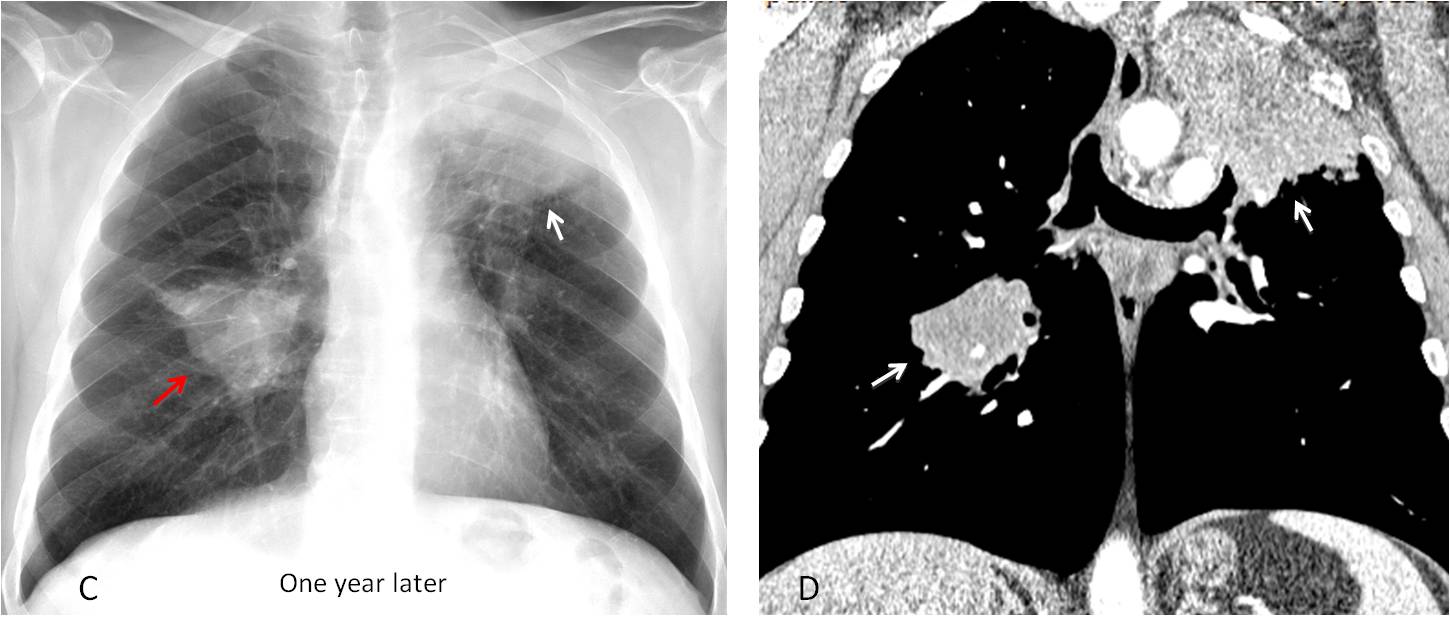
Fig. 1
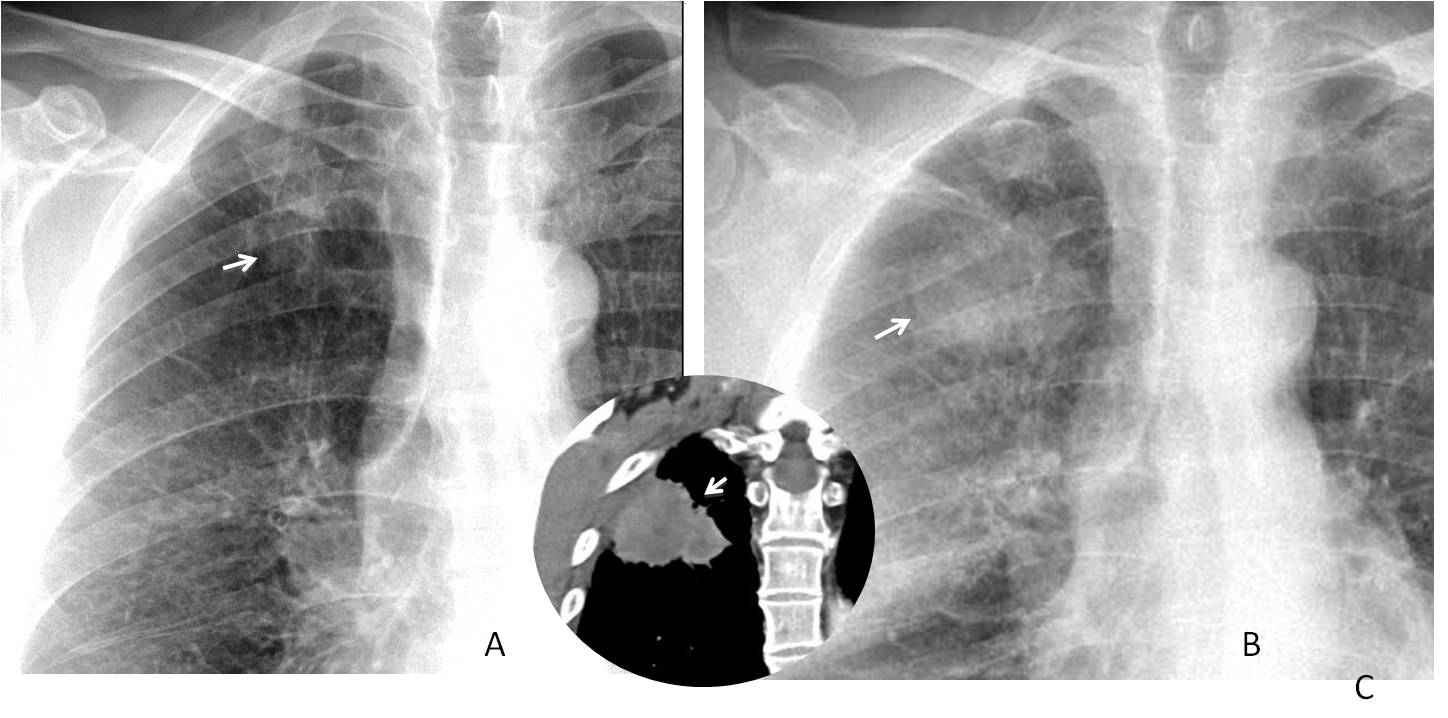
Fig. 2
Fig. 2: 58-year-old man, smoker. Chest radiographs shows a small apical nodule that was missed (A, arrow). Two years later the nodule has grown (B, arrow) and has reached the chest wall (insert, arrow). Diagnosis: adenocarcinoma with chest wall invasion.
In my experience, many radiologists and just about all clinicians fail to properly look at the mediastinum. Large masses are easily seen, but subtle bulges of the mediastinal contour are missed more often than not. It is our obligation to examine the right and left mediastinal contours to detect subtle abnormalities that may portend serious disease (Figs. 3-5).
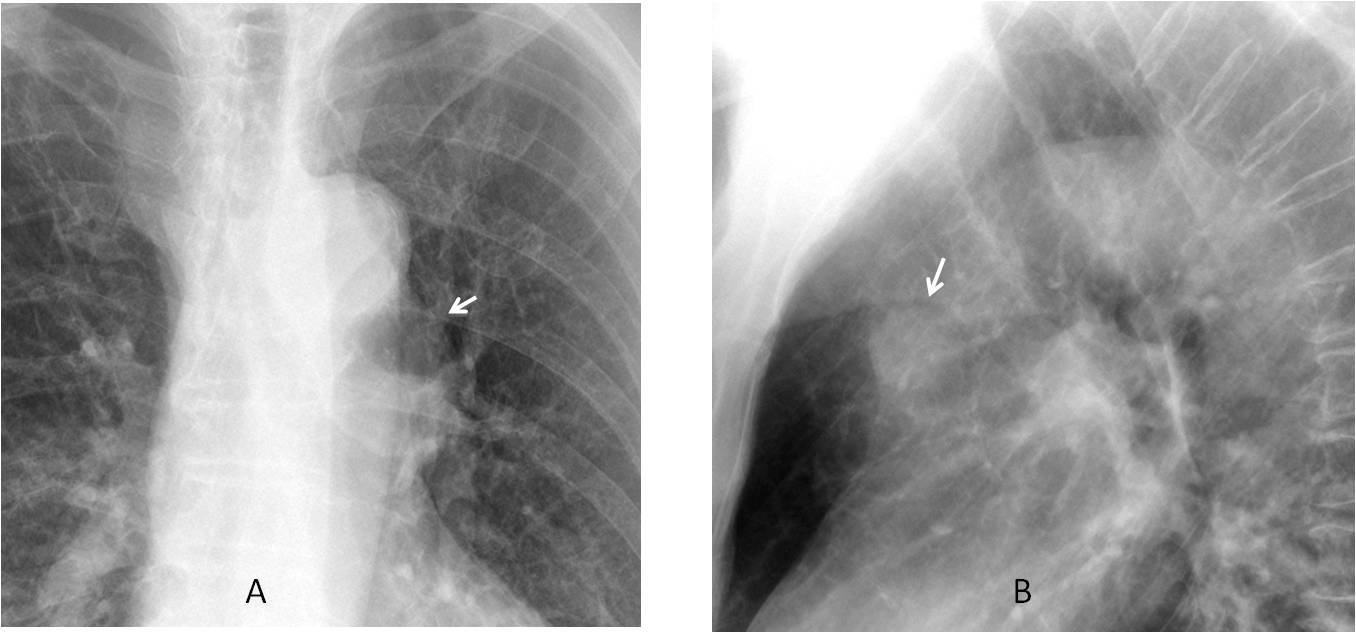
Fig. 3
Fig. 3. Bulging of the aorto-pulmonary window (A, arrow), that was discovered because a nodular shadow was noticed in the lateral view (B, arrow). This finding prompted a CT examination.
Axial and coronal enhanced CT images show that the bulging is secondary to a small, partially thrombosed aneurysm arising from the aortic knob (C and D, arrows).
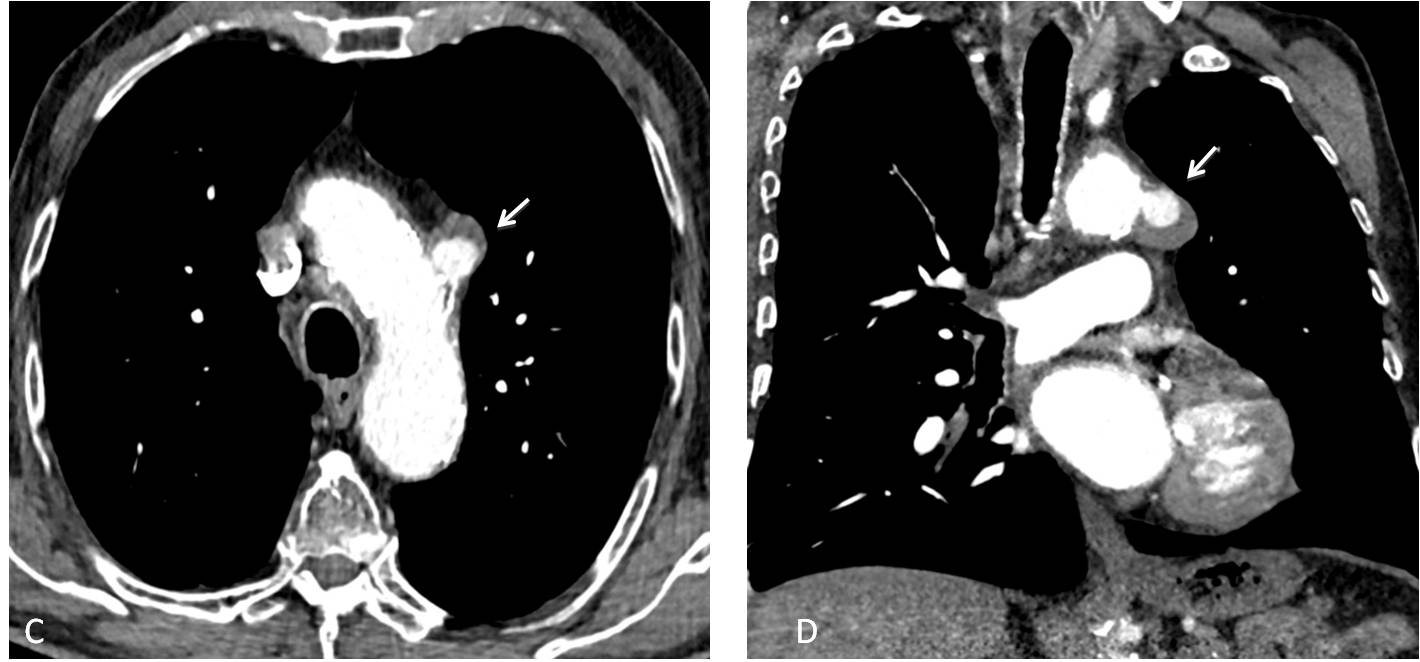
Fig. 3
In daily practice, bulging of the pulmonary artery segment in the PA radiograph is not an infrequent finding. It may herald significant disease, such as pulmonary arterial hypertension, shunts or a mediastinal mass, among others. It should be always investigated (Fig. 4).
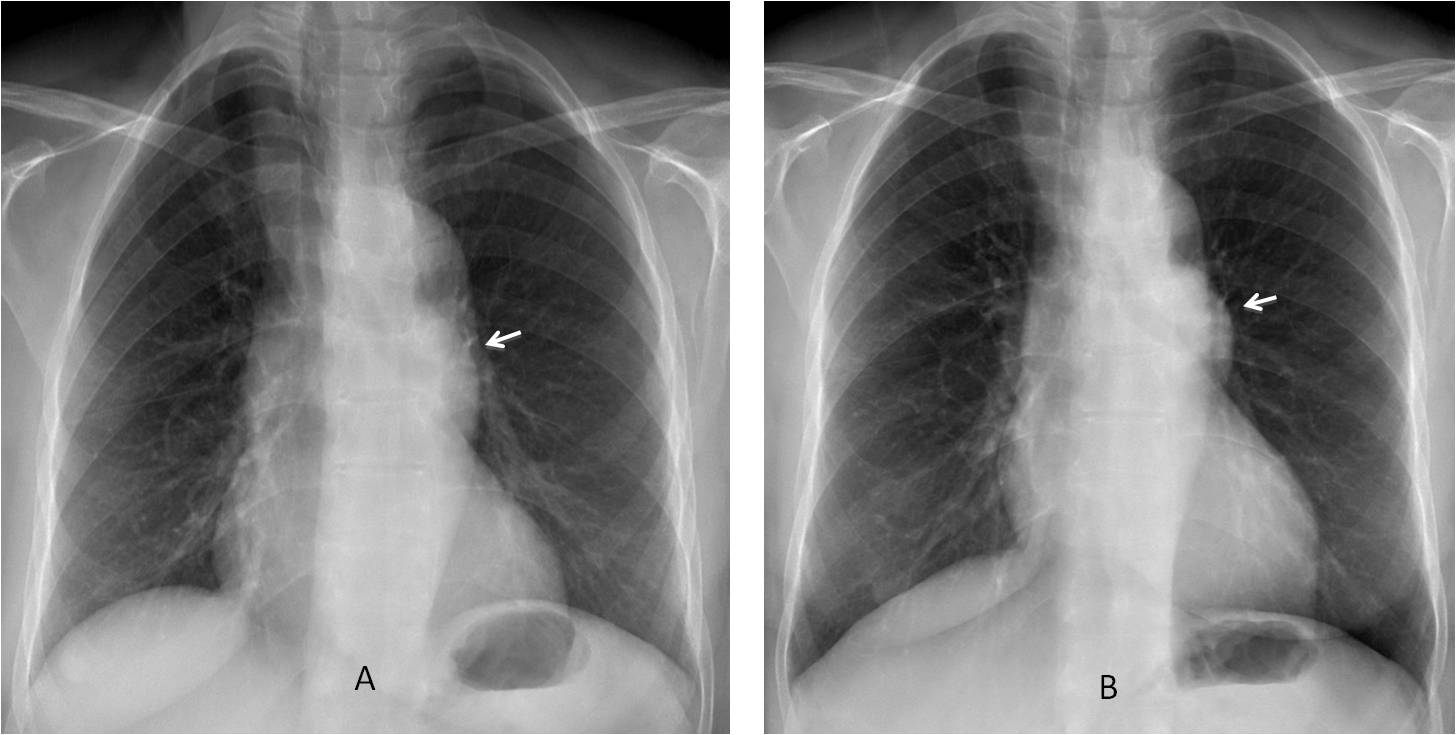
Fig. 4
Fig. 4: 47-year-old woman with asthenia. A bulge in the pulmonary artery segment was missed because of the slight obliquity of the view (A, arrow). A second PA radiograph one month later clearly shows the abnormality (B, arrow).
The lateral view shows a mass in the anterior clear space (C, arrows), confirmed with unenhanced axial and coronal CT (D and E, arrows). Diagnosis: thymoma.
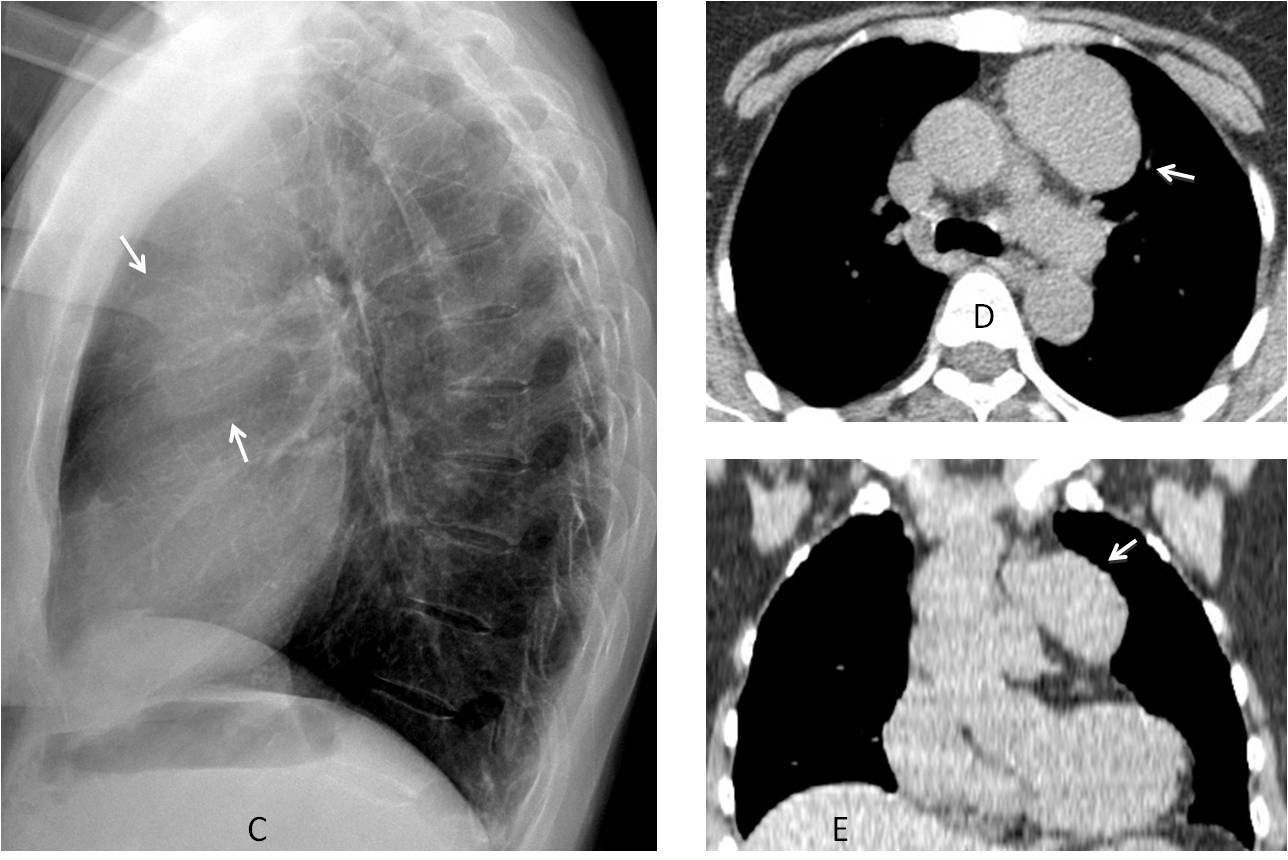
Fig. 4
Careful examination of the heart contour helps to detect changes that may be caused by an aneurysm, mediastinal tumor, or cyst. Failure to do so may result in missed disease (Fig. 5).
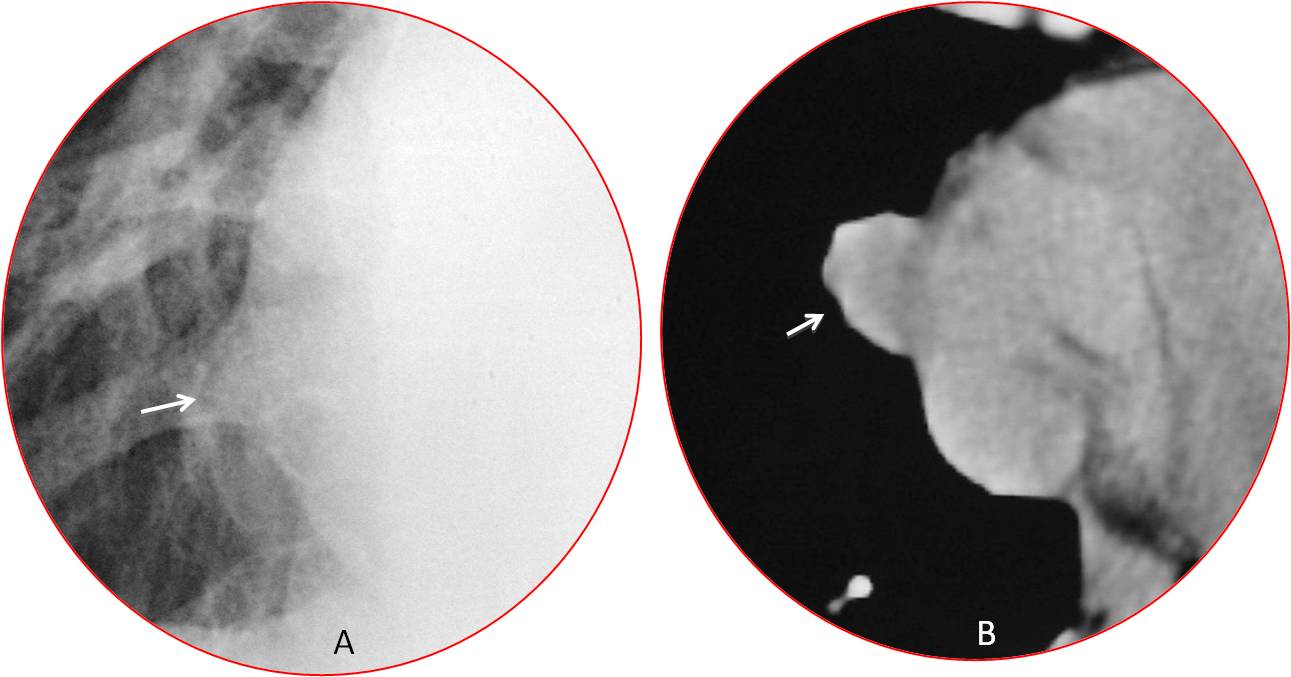
Fig. 5
Fig. 5: Slight protrusion of the right heart border (A, arrow). Unenhanced CT shows a rounded mass (B, arrow) measuring -10 HU. Diagnosis: pericardial cyst.
In my experience, examining the thoracic spine in the lateral view can be very rewarding. It is a good way to discover intrinsic spinal conditions (Fig. 6) or, more commonly, superimposed pulmonary entities that are not seen in the PA view (Figs. 7 and 8).
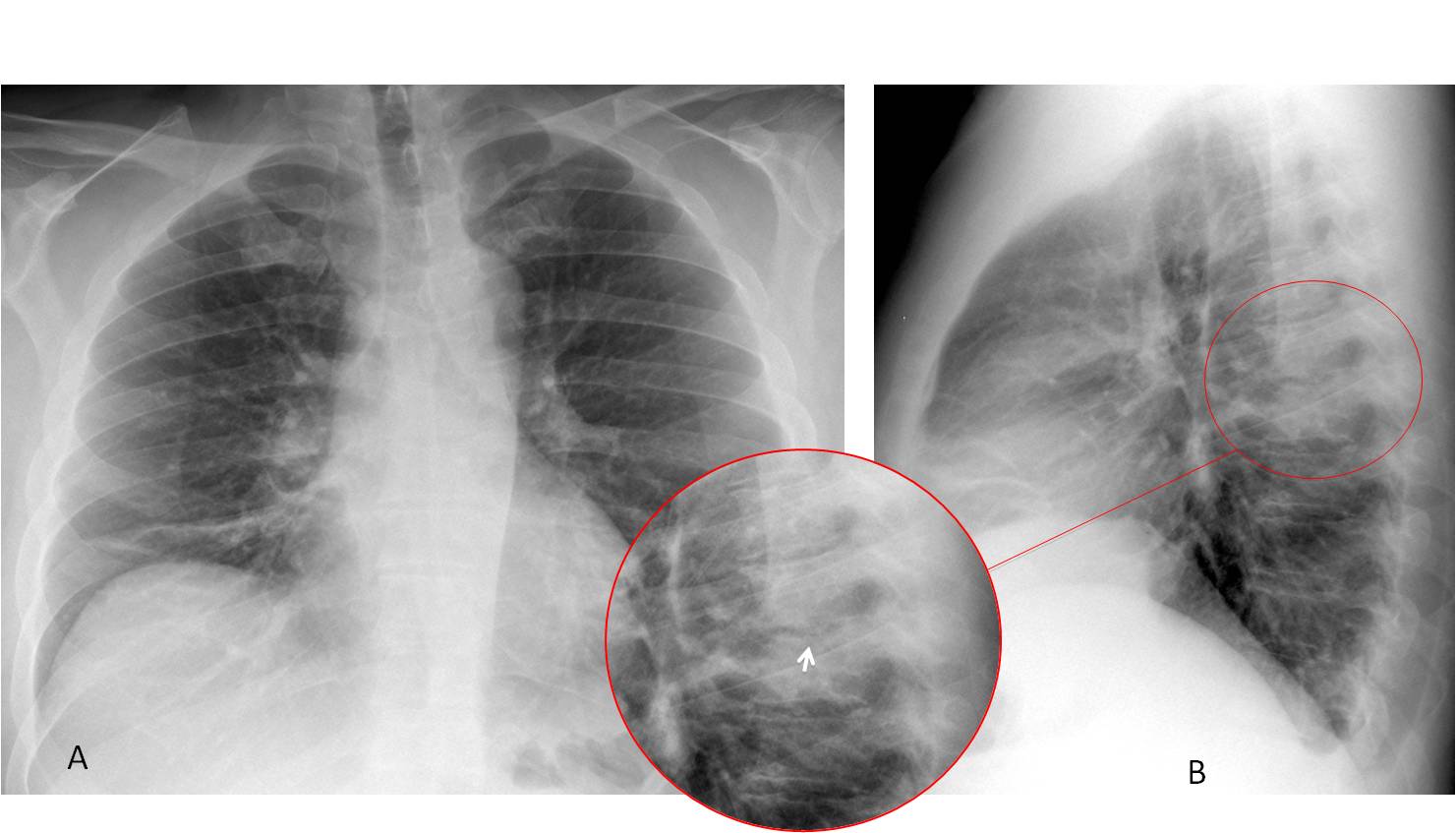
Fig. 6
Fig. 6: 47-year-old man with fever and back pain. PA radiograph (A) shows plate-like atelectasis at the right lung base. In the lateral view, the T6-T7 vertebral bodies are more opaque that the ones above or below (B, circle). On close inspection, the intervertebral space is ragged and irregular (insert, arrow). These findings are highly suggestive of spinal infection.
Sagittal CT confirms disk involvement (C, circle). Coronal and axial CT shows swelling of the para-spinal soft tissues (D and E, arrows), which are partially responsible for the increased opacity in the lateral chest radiograph. Culture of needle biopsy material grew Staphylococcus aureus. Final diagnosis: Pyogenic spondylodiscitis of T6-T7.
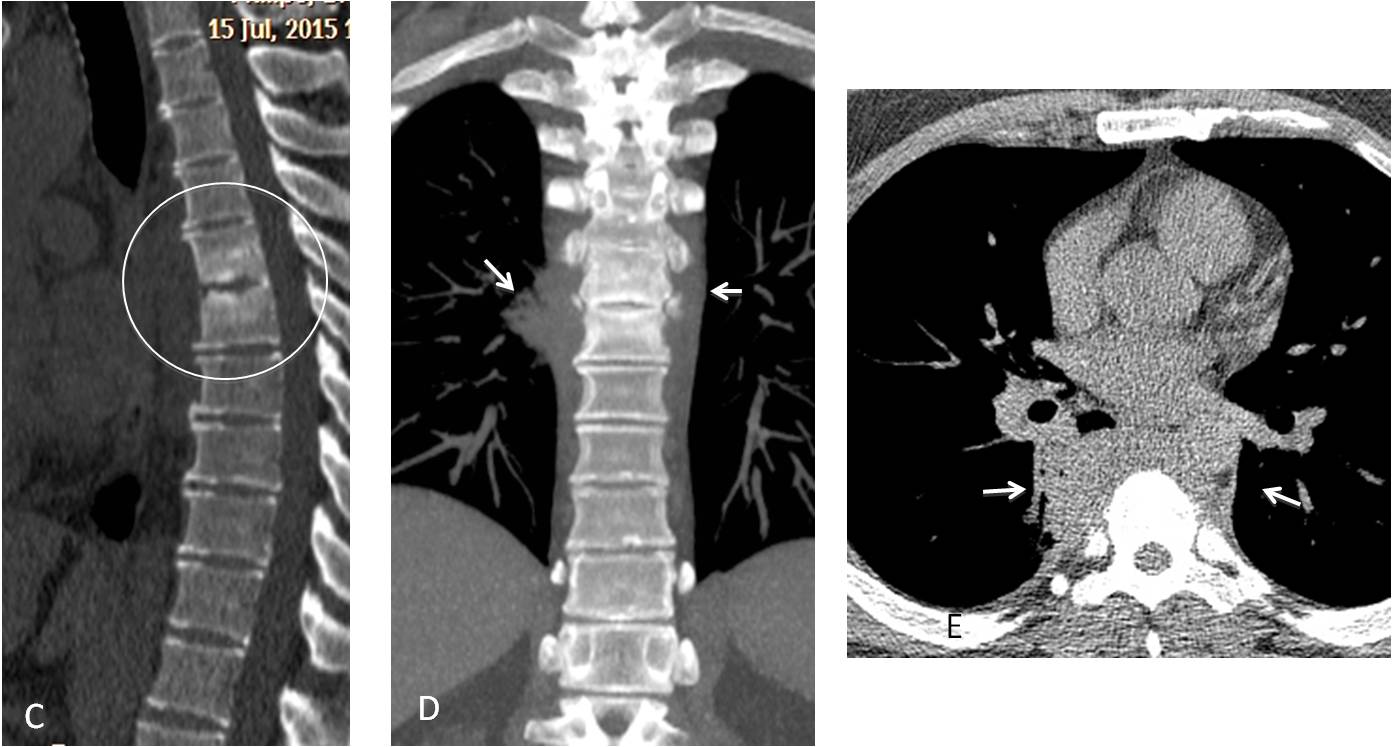
Fig. 6
As we all know, the opacity of the vertebral bodies decreases in the caudal direction, because the superimposed lung is larger. Any change in this decreasing opacity suggests a lung abnormality and should be investigated (Fig. 7).
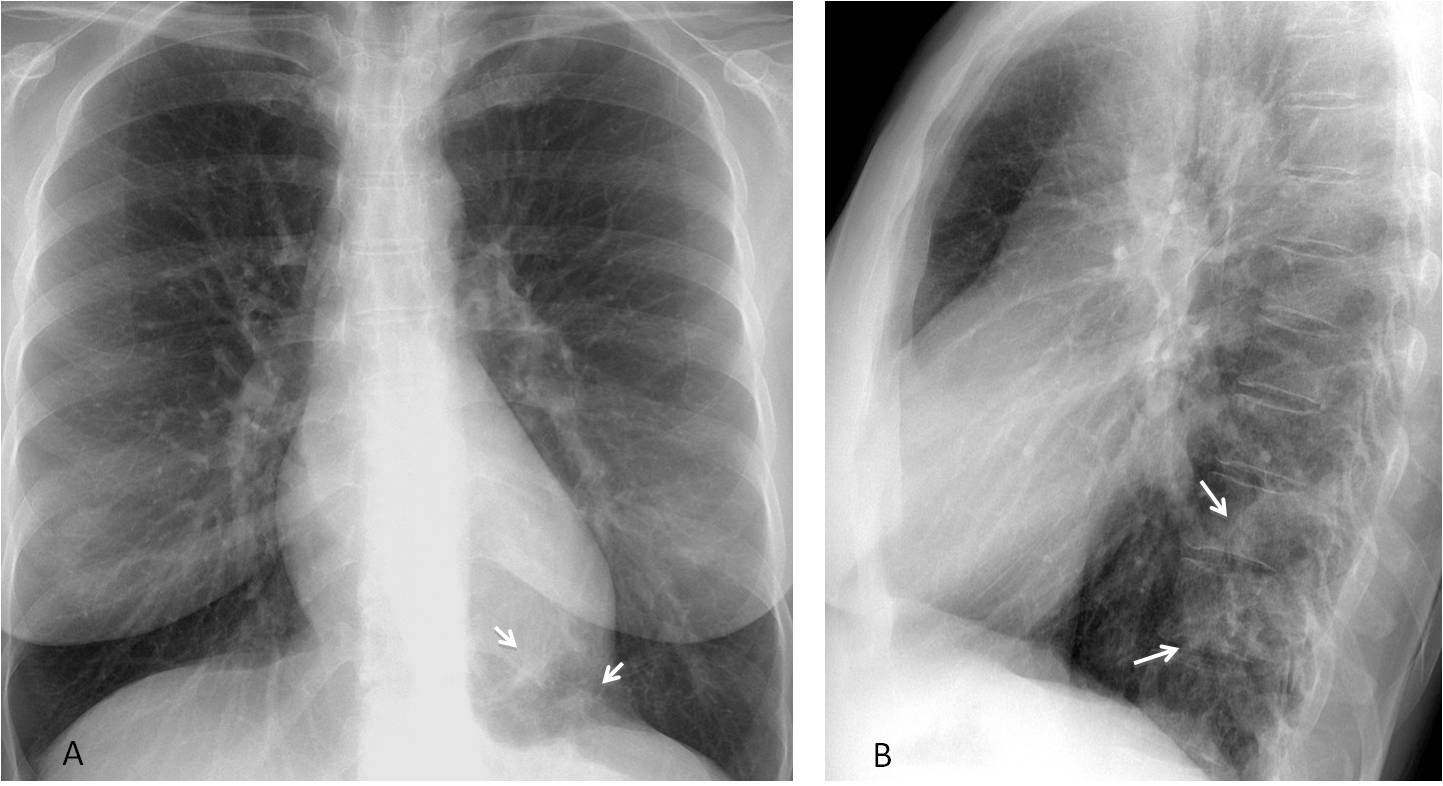
Fig. 7
Fig. 7: 44-year-old woman with renal colic. Lateral radiograph shows an increased opacity at the level of the lower thoracic spine (B, arrows), barely visible at the left lung base in the PA view (A, arrows).
Unenhanced abdominal CT to study renal colic discovered a multicystic lesion in the left lung (C, white arrow), with a possibly abnormal vessel arising from the abdominal aorta (C, red arrow), confirmed with enhanced chest CT (D, arrow). Diagnosis: cystic sequestration. The patient denied a previous episode of pulmonary infection.
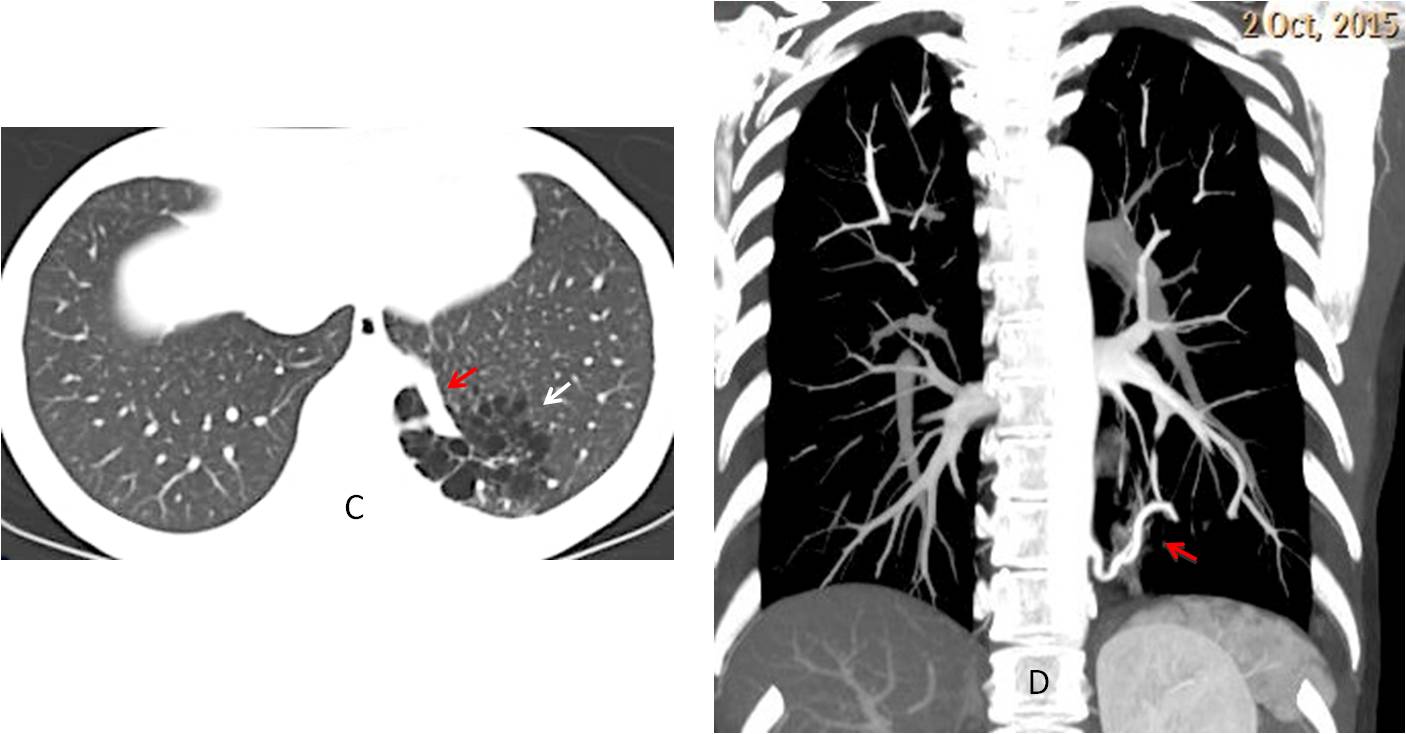
Fig. 7
This final case is a good example of a missed nodule in the lateral radiograph that ended with the demise of the patient two years later. It clearly emphasizes the importance of examinaing the thoracic spine in the lateral view (Fig. 8).
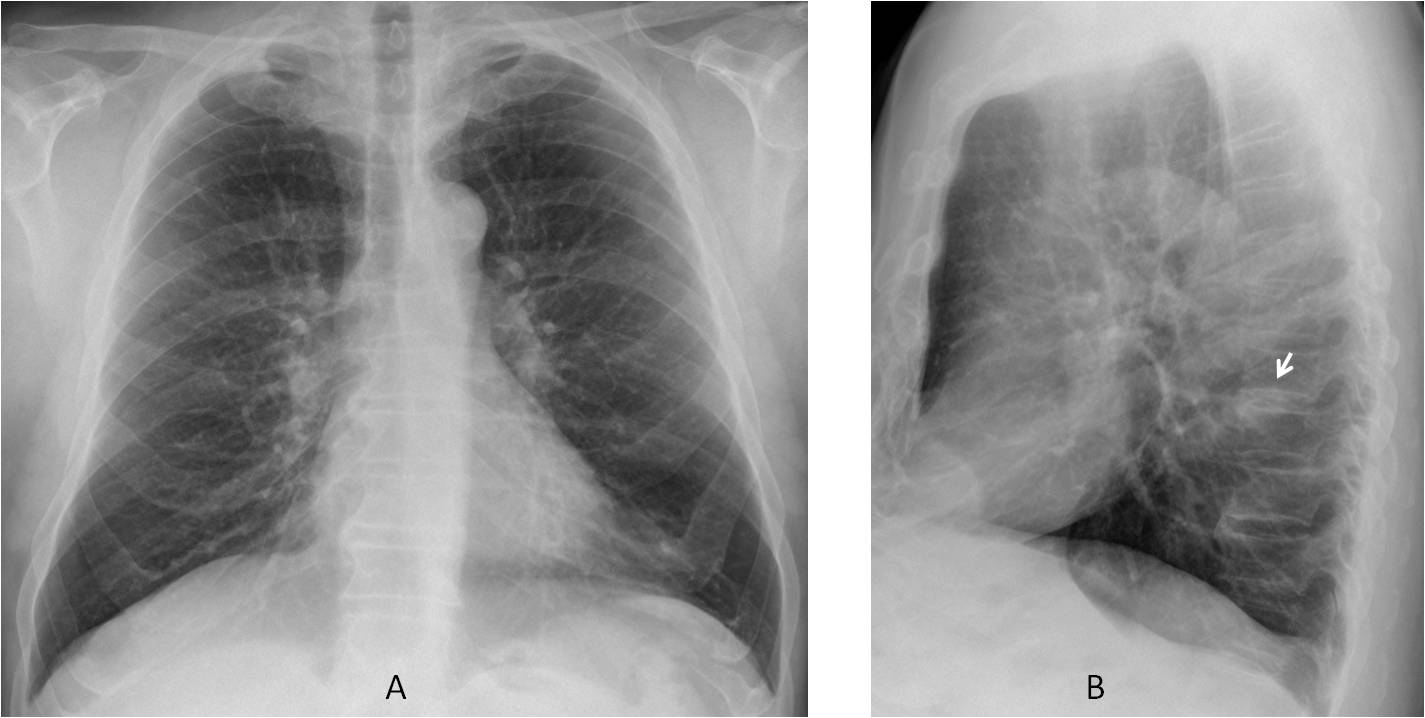
Fig. 8
Fig. 8: 58-year-old male, with mild cough. PA radiograph (A) is unremarkable. There is a small nodule projected over the thoracic spine in the lateral view (B, arrow) that was overlooked by the radiologist.
One year later the nodule has grown and is visible in the PA and lateral radiographs (C and D, arrows). Needle biopsy confirmed a carcinoma of the lung with a small metastatic nodule to the liver. Two years after the initial radiograph, PET-CT demonstrates innumerable metastases in the liver (E, arrows). The patient died shortly afterwards.
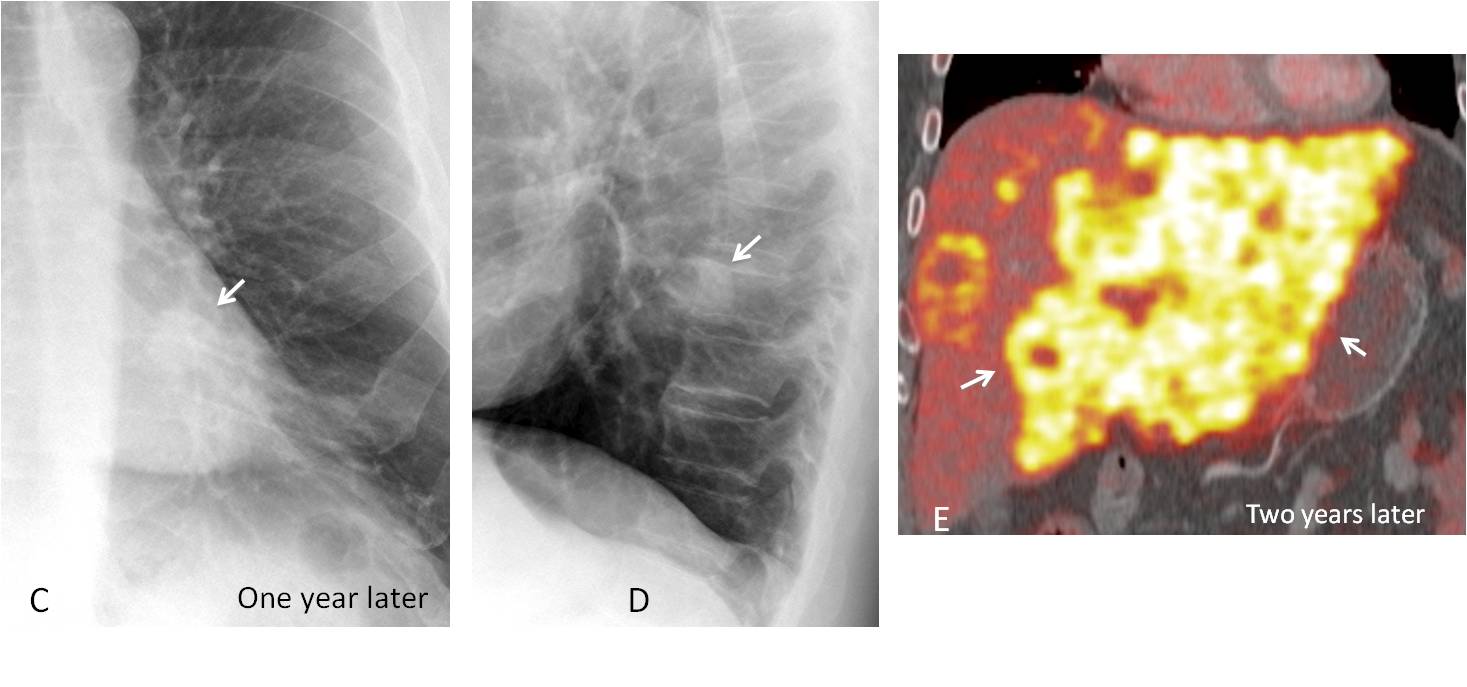
Fig. 8

Follow Dr. Pepe’s advice:
Subtle errors of perception are avoided by using checklists
Specific areas that should be scrutinised are:
– In the PA view: the lung apices and the mediastinal borders
– In the lateral view: the thoracic spine


Hi,
i can see bulging of the aorto-pulmonary stripe on the AP view with a small correspondent ovoid density on the lateral view.
Impression: aorto-pulmonary window lesion.
Good morning!
There is an increased density in the apical portion of the left hemithorax compared to the right one.
The hilum are prominent. Both have a well defined inferior margin, and in the lateral view I think there is a nodular lesion with center high density (calcium?), perhaps adenopathy?
Sarcoidosis?
Why not?
I see an ovoid hilar region in left hilum which shows a focus of calcification
Adenopathy?
Agreed with MK – I see the same changes, but calcium in “nodular lesion” suggesting calcified limph node after tuberculosis and the slightly increased density in left apex due to fibrous changes of the lung parenchyma after healed TB.
Besides, there is pleural thickening on lateral view in the main fissure which slightly deformes the diaphragmal contour
Changes after lymphatic nodules and lung tuberculosis
The bulging on left mediastinal contour just below the arcus aortae suggesting – “conus pulmonalis” due to hypertension
Cardiologist consultation needed
Hi!
Fat pad sign on profile pic.suggests small perikardial effusion
No pericardial effusion visisble at CT. Sorry 😉
Anterior mediastinum mass.
Older people tend to have an elongated ascending aorta, that impinges in the anterior clear space. No anterior mass was found at CT.
Hi,
i think it is hard to tell if the lesion is in the anterior or middle mediastinum because of the close relationship between the AP stripe and AP window. but I favored the AP window/middle mediastinal lesion because I imagined a small nodule there on the lateral view!.
Usually, lesions in the aorto-pulmonary window are in the middle mediastinum
Hello,
There is prominent pulmonary artery with prominent vascular hilas probably with cut-off – I think about pulmonary hipertension.
I believe the pulmonary artery arch is lower than the bulging seen in the PA view
…il Bari sta scivolando verso ….l’alto….ma quello che vedo è verso il ….basso…..ampliamento del forame di coniugazione intervertebrale tra D10 e D11…
Hi,
Bilateral hilar nodal enlargement.
Possible diagnosis: Sarcoidosis.
Back from ECR Congress. Congratulations to all of you who saw the bulge in the aorto-pulmonary window, with special mention to
tr, who was the first