Dr. Pepe’s Diploma Casebook: Case 114 – SOLVED!
Dear Friends,
Today I am presenting radiographs of an 80-year-old man with productive cough and fever. What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
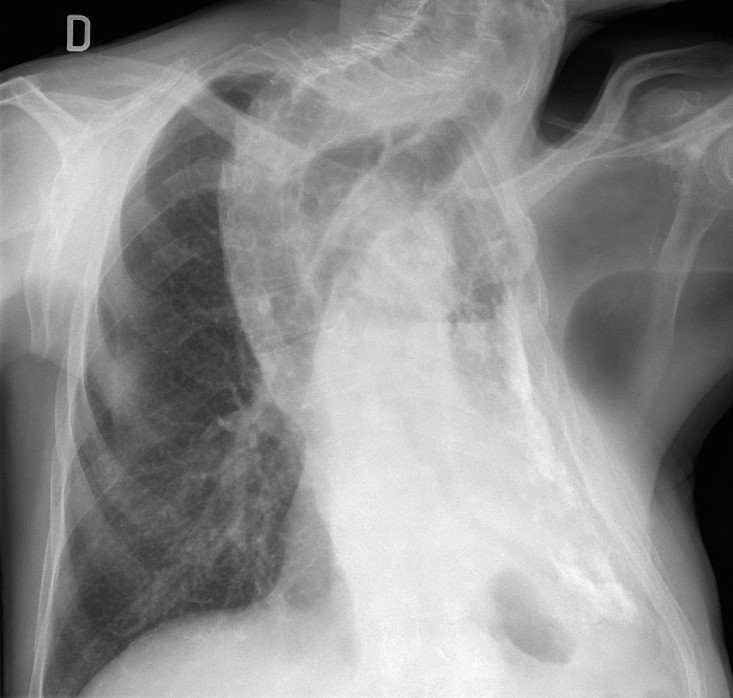
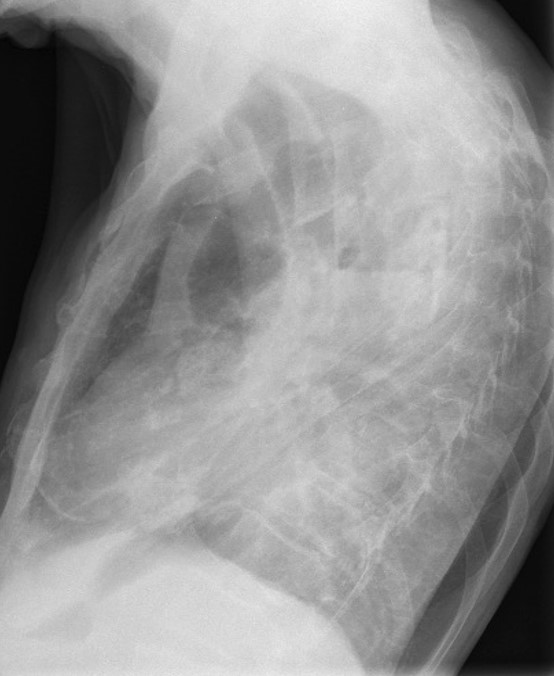
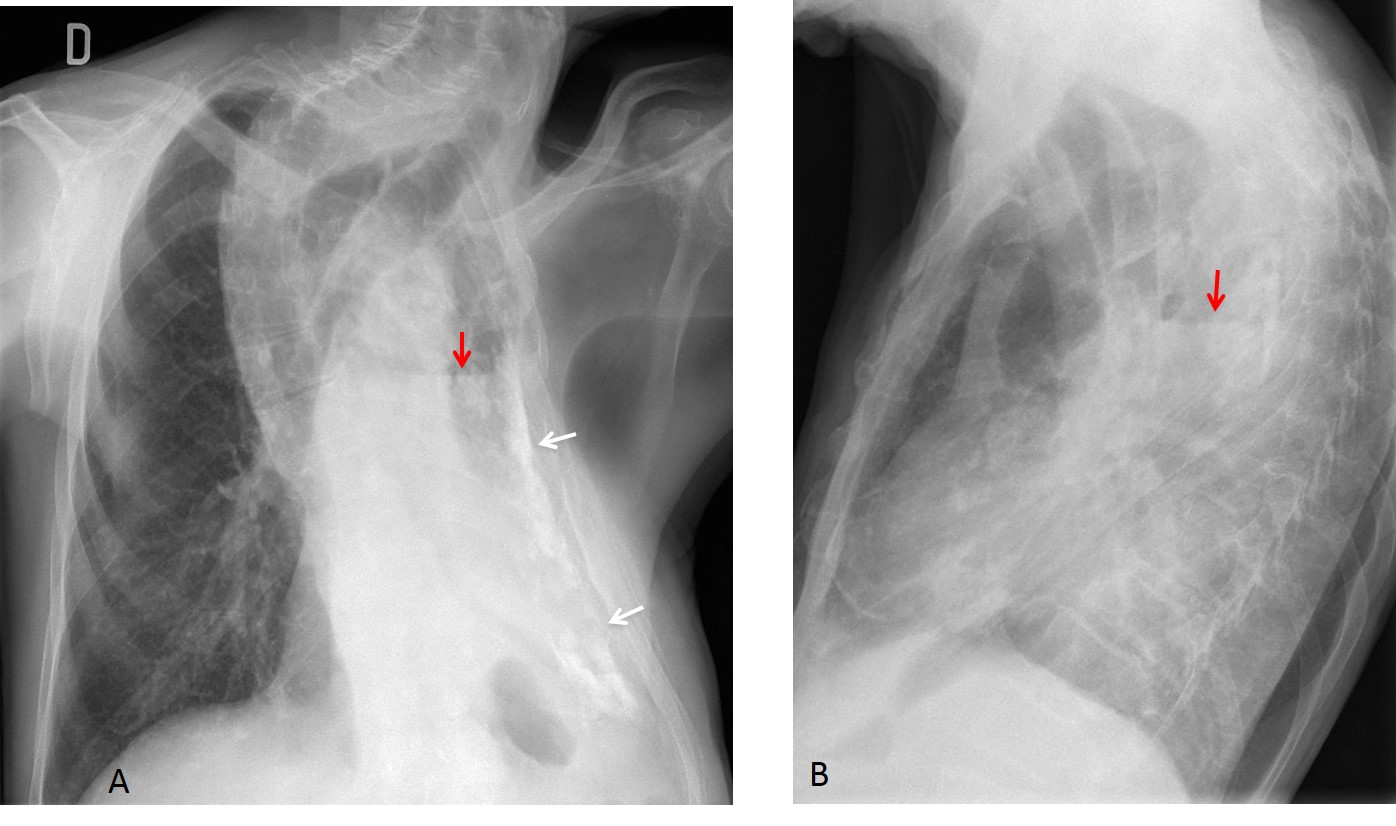
Findings: PA radiograph shows marked scoliosis and a small left hemithorax with pleural calcification (A, white arrows). In addition, there is an air-fluid level within the pleural cavity (A and B, red arrows). This appearance is highly suspicious of bronchopleural fistula.
Enhanced axial CT confirms the small left hemithorax, pleural calcification (C, white arrows), and the air-fluid level within (C and D, red arrows).
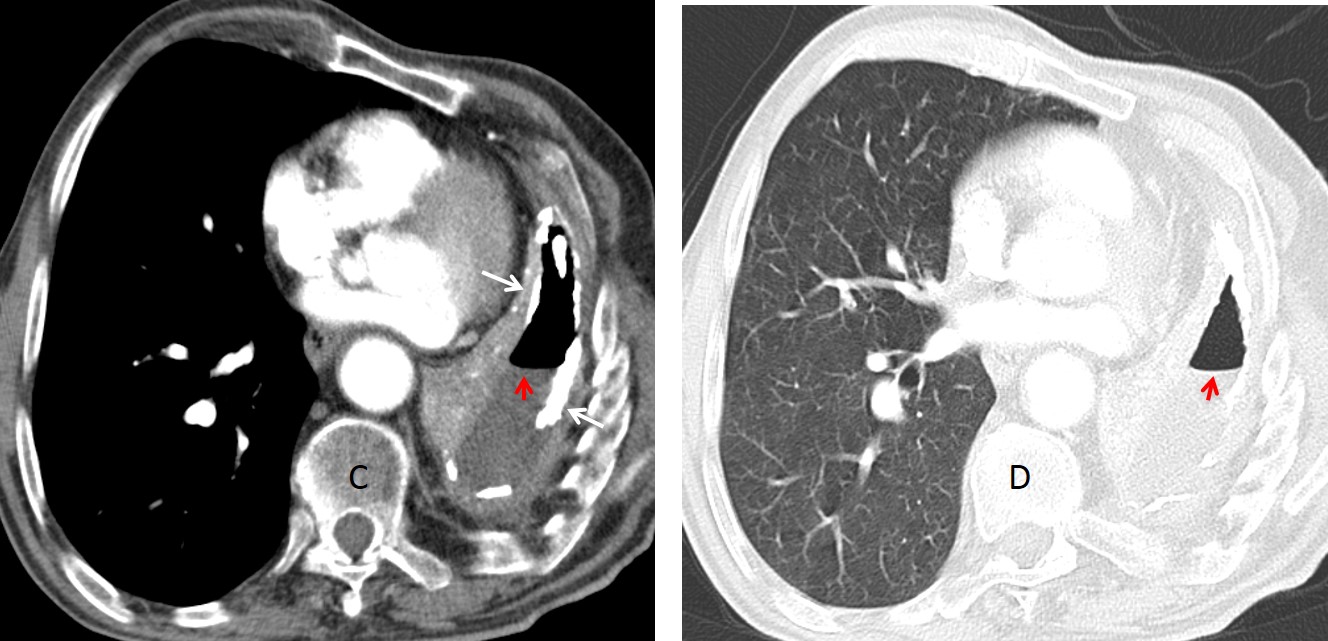
Final diagnosis: bronchopleural fistula in chronic tuberculous pleuritis.
I am presenting this case to discuss the differential diagnosis of a single air-fluid level. This feature is easily recognized in the chest radiograph as a straight horizontal line representing the air-fluid interface.
Detection of air-fluid levels is important because they imply a closed cavity and therefore, active disease.
From the diagnostic viewpoint, air-fluid levels can be found in the lungs, pleura, mediastinum or chest wall. My intention is to describe their specific features in lung and pleura, leaving mediastinum and chest wall for next week.
Air-fluid level in the lung occurs in either cavitated nodules/masses or within pulmonary infiltrates. Air in nodules/masses helps to delineate wall thickness. A thin wall suggests a benign condition (Fig. 1), whereas a thick wall increases the probability of malignancy, although there is significant overlap between different processes (Fig. 2). In my experience, a nodular inner wall is a reliable sign of malignancy (Fig. 3).
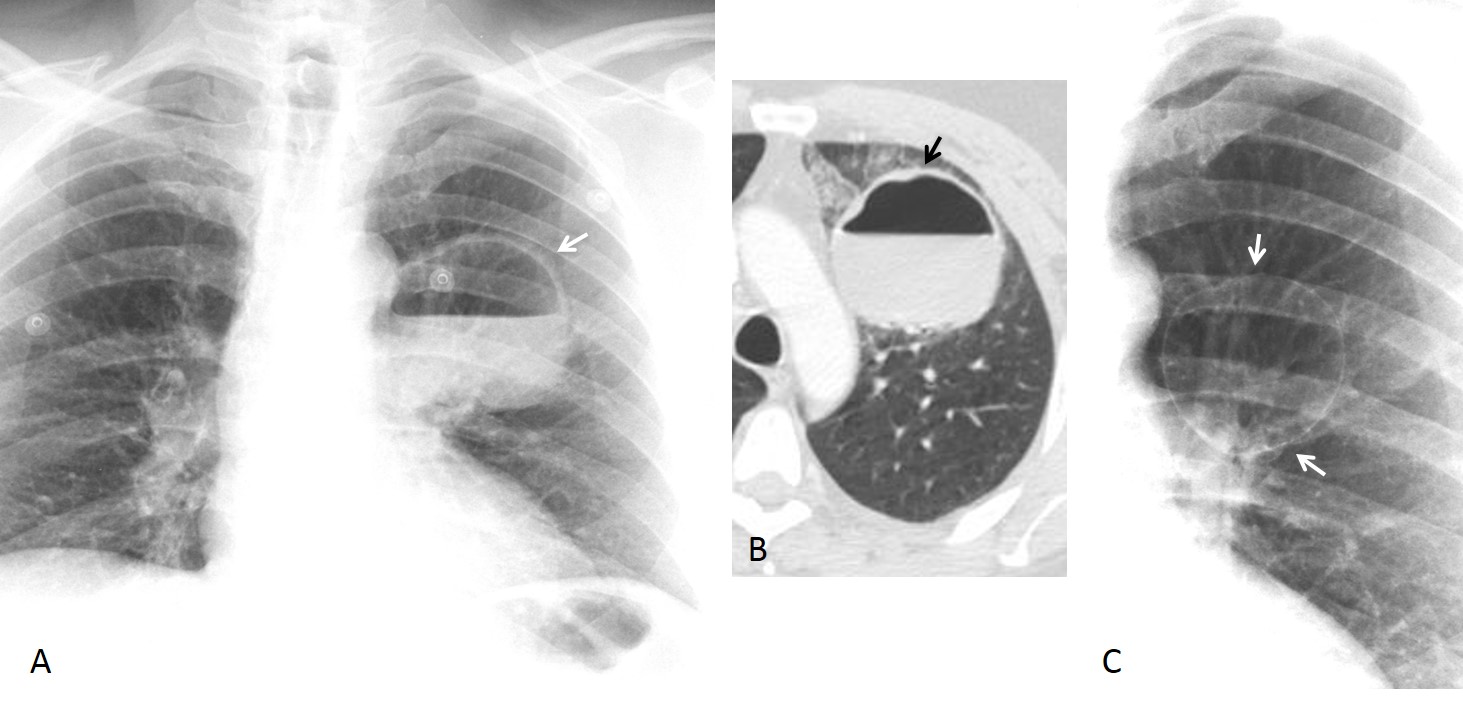
Fig. 1
Fig. 1. 53-year-old man with cough and high fever. PA radiograph and axial CT show a thin-walled cavity with a large air fluid level (A and B, arrows). Radiograph taken three years earlier shows a previous thin-walled lesion in the same location (C, arrow). Diagnosis: infected bulla.
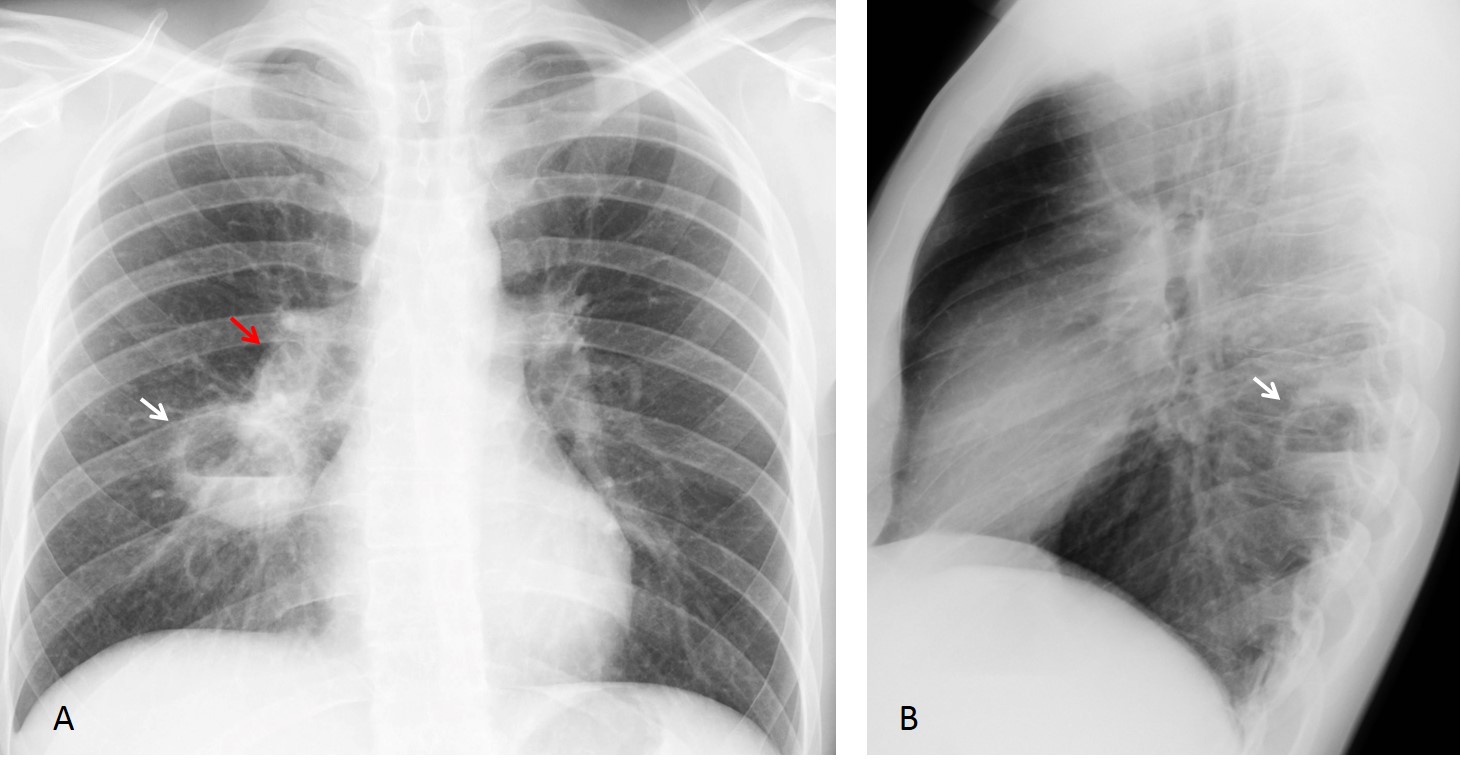
Fig. 2
Fig 2. 25-year-old man with fever and copious sputum. PA an lateral adiographs show a cavity with an air-fluid level in the apical segment of the RLL (A and B, white arrows). The right hilum shows increased opacity compared to the left (A, red arrow).
Coronal and axial CT images confirm the cavitation (C and D, white arrows) as well as enlarged lymph nodes in the right hilum (D, red arrow). My initial diagnosis was TB. Clinicians suspected aspiration and treated the patient with antibiotics. The chest radiograph three weeks later (E) shows that the cavity has disappeared. Note that the right hilum has returned to normal. Final diagnosis: pulmonary abscess secondary to aspiration

Fig. 2
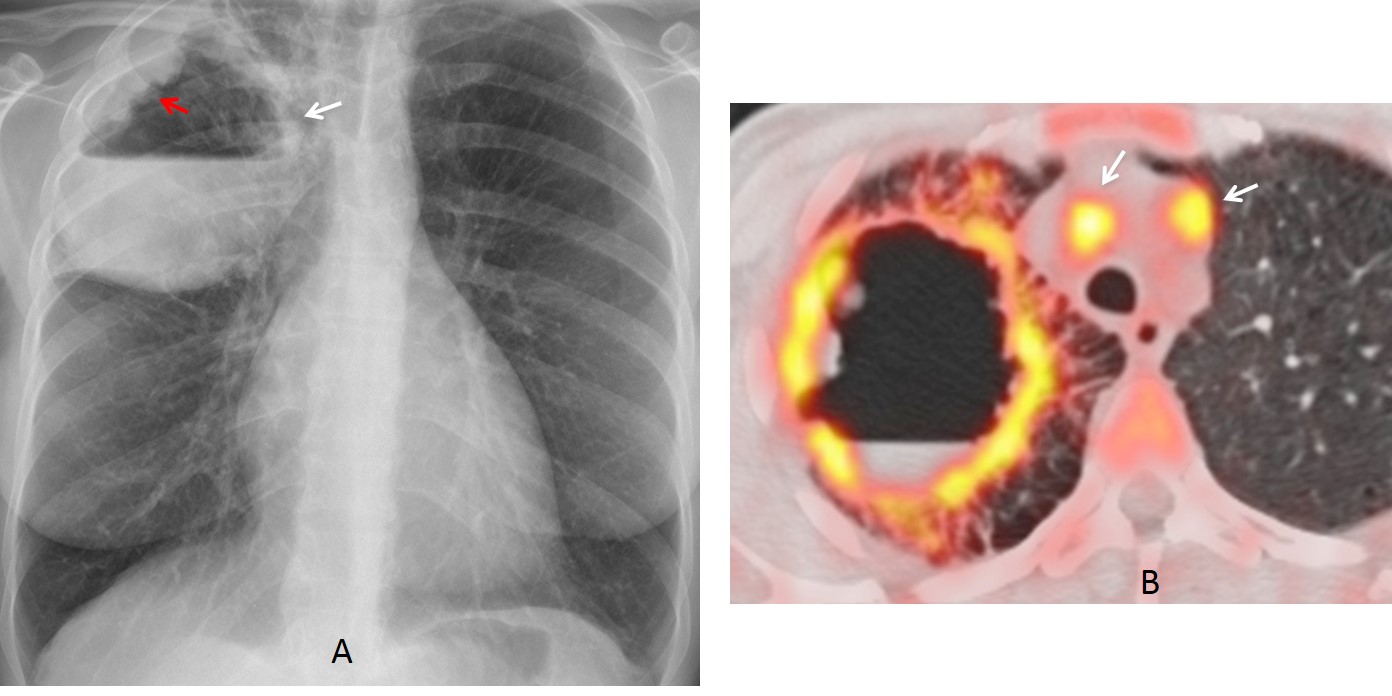
Fig. 3
Fig. 3. 43-year-old woman with fever and hemoptysis. PA radiograph shows a RUL cavity with an air-fluid level (A, white arrow). Irregular nodularity protrudes from the lateral wall (A, red arrow). This finding strongly suggests malignant disease. PET-CT shows enhancement of the wall and mediastinal lymph nodes (B, arrows). Final diagnosis: infected squamous-cell carcinoma.
An air-fluid level within a pulmonary infiltrate is the hallmark of necrotizing pneumonia (Fig. 4), although it can occasionally occur in a malignant infiltrate (Fig. 5).
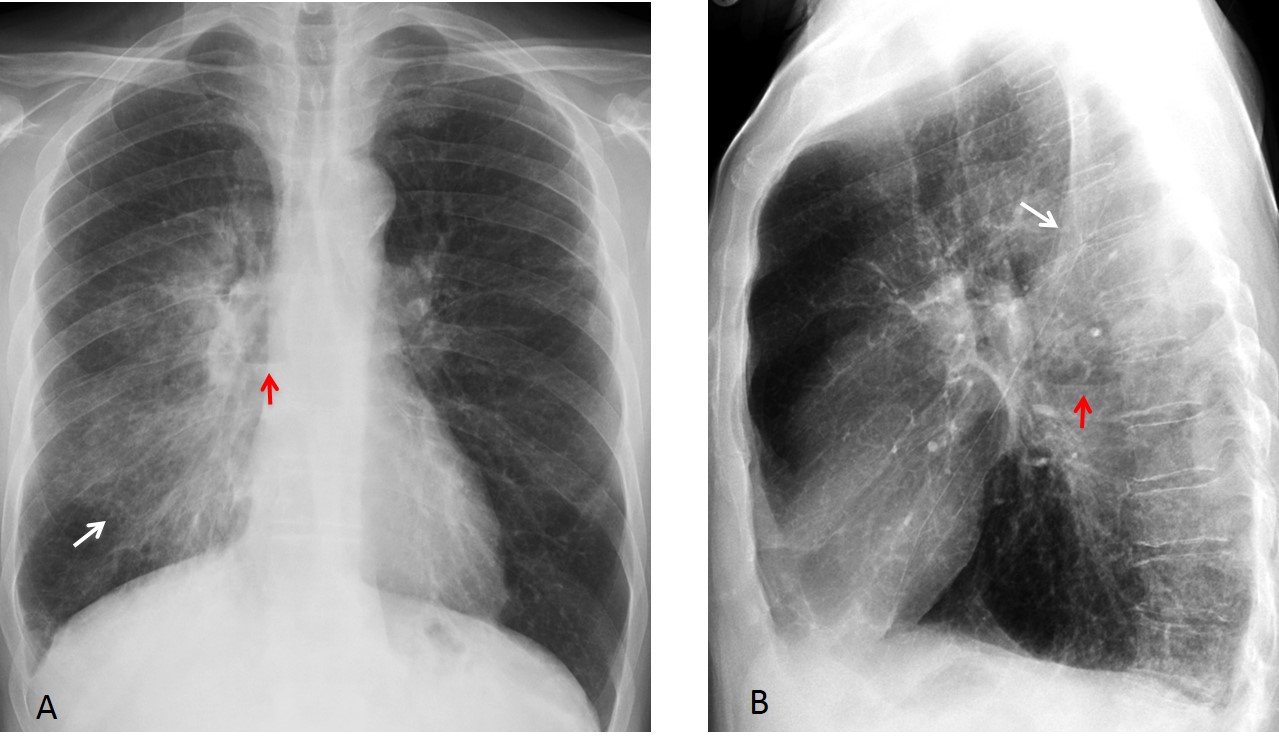
Fig. 4
Fig. 4. 62-year-old man with fever. Chest radiographs show airspace disease (A and B, white arrows) with a centrally located air-fluid level (A and B, red arrows).
Coronal and axial CT confirm the airspace disease and the central cavity (C and D, arrows). Diagnosis: necrotizing pneumonia.
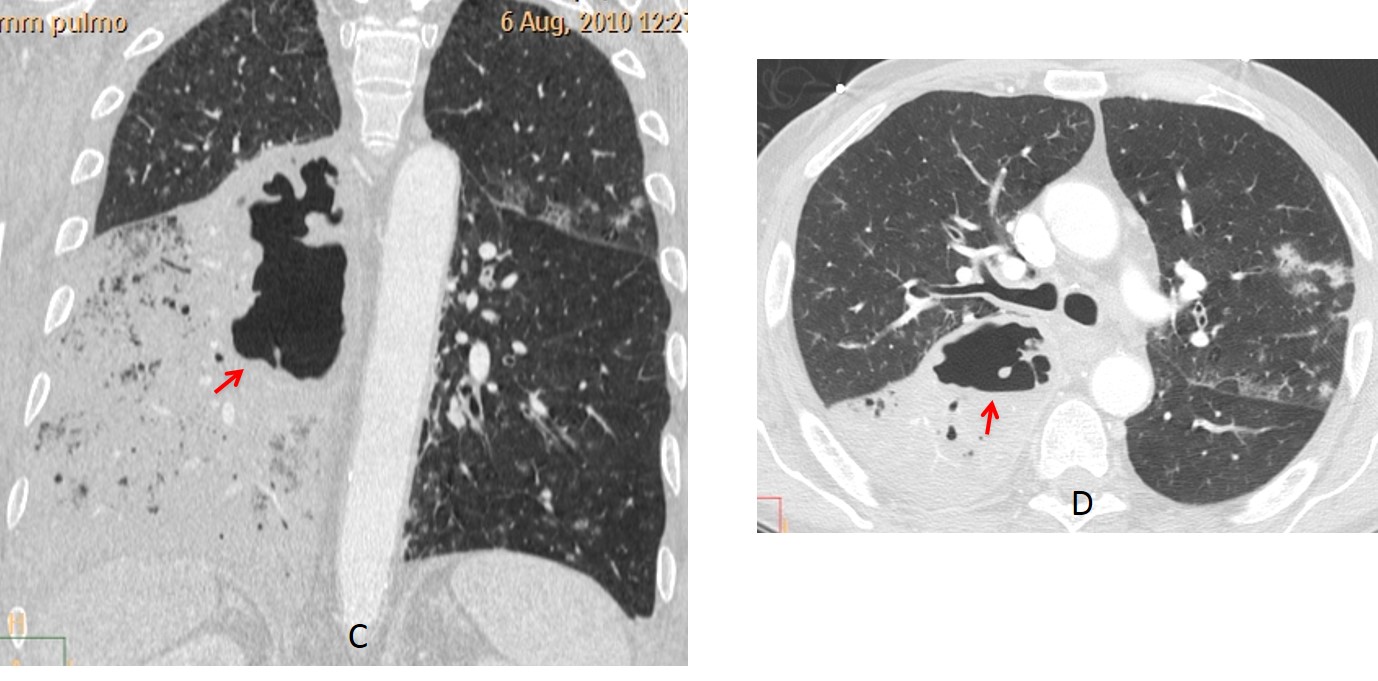
Fig. 4
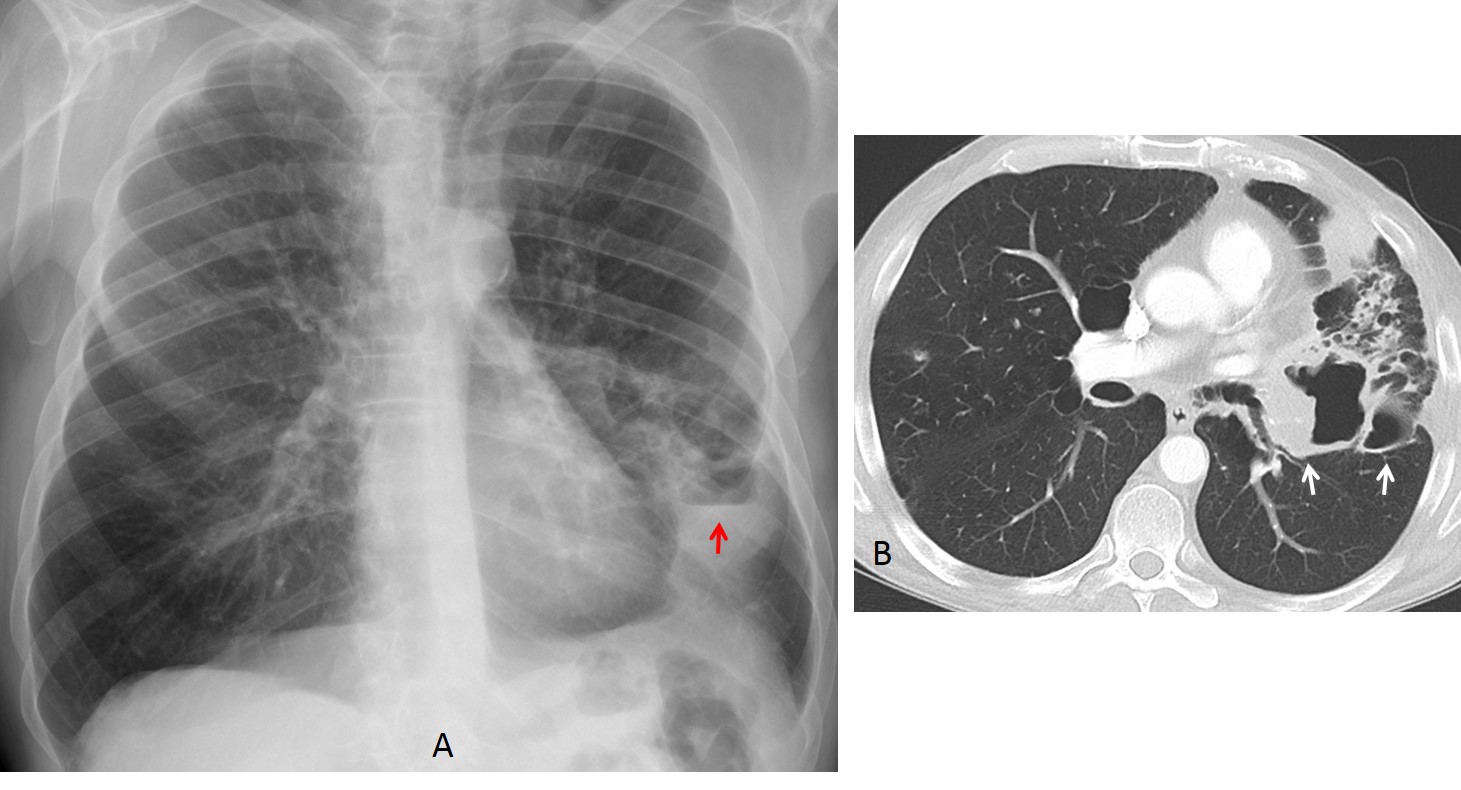
Fig. 5
Fig 5. 60-year-old man with hemoptysis. PA radiograph shows airspace disease with an air-fluid level (A, red arrow). Enhanced axial CT confirms a part-solid carcinoma with cavities (B, arrows).
An air-fluid level in the pleura has a different appearance than in the lung. It is usually very obvious, and contrary to what occurs in the lung, the length of the level is different in the PA and lateral projections. Also, the level lacks a roof above (see diagram below and Figs. 6 and 7). Most common causes are: infection or trauma, and occasionally, bronchopleural fistula. Surgery and other types of invasive procedures should be excluded.
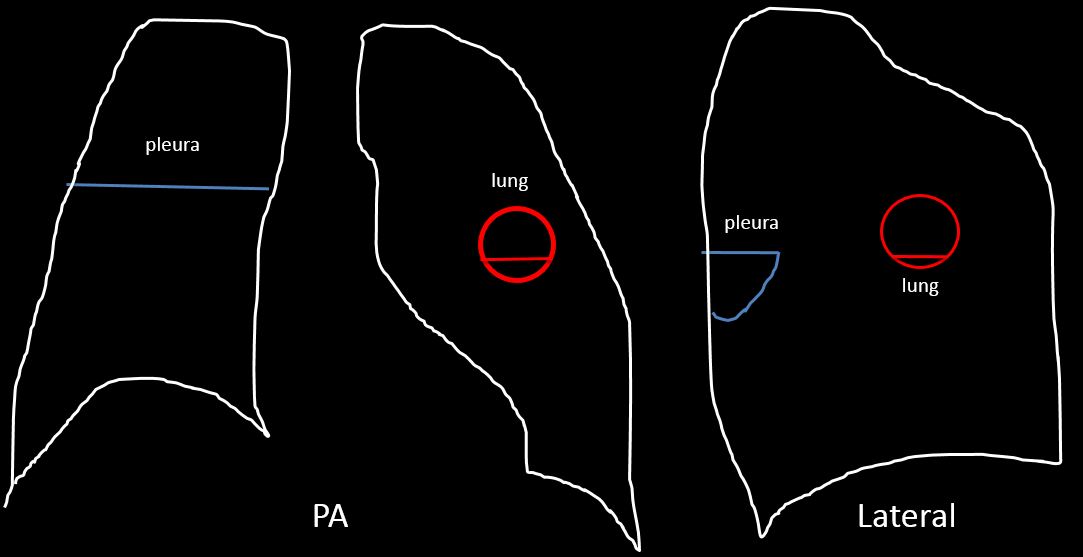
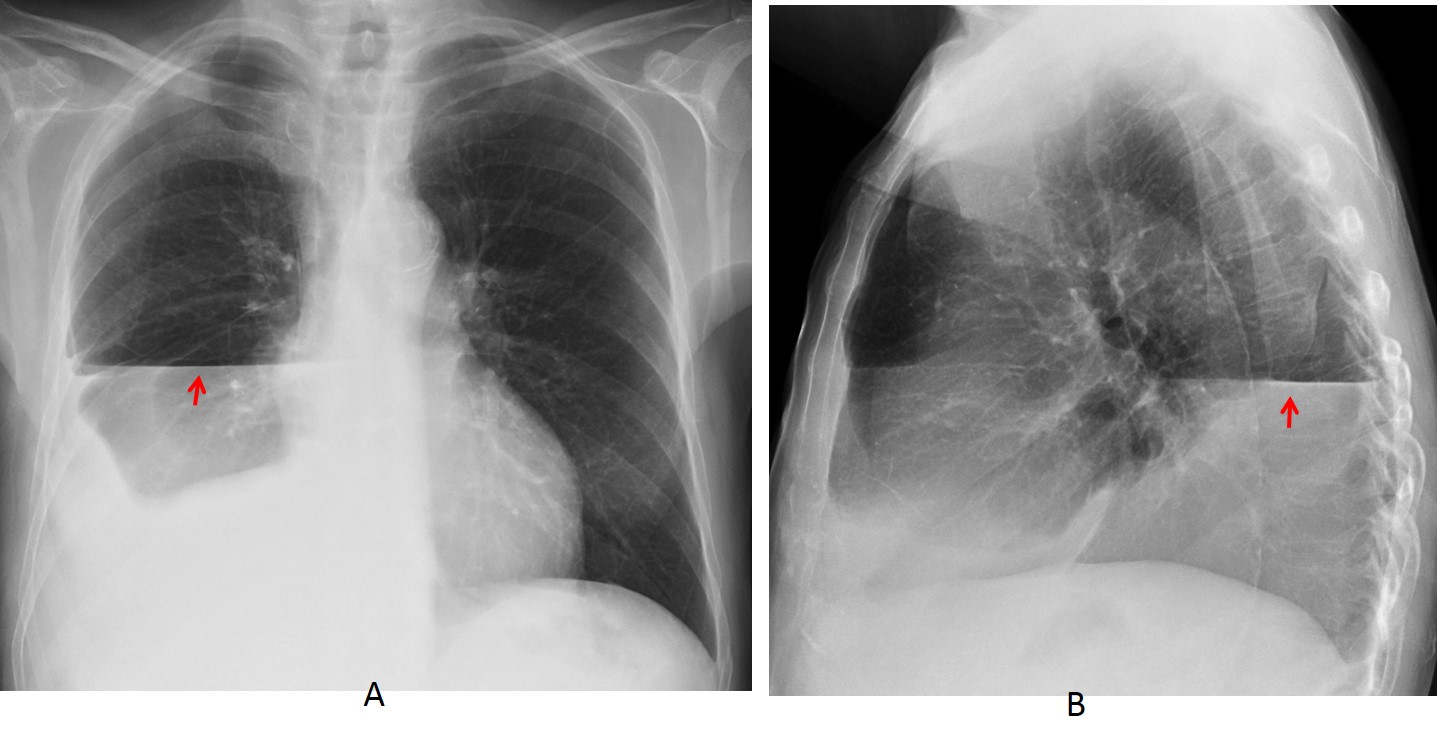
Fig. 6
Fig. 6. 45-year-old man with hydropneumothorax. Note the different length of the air-fluid level in the PA and lateral views (A and B, arrows) and the absence of a visible wall above the level.
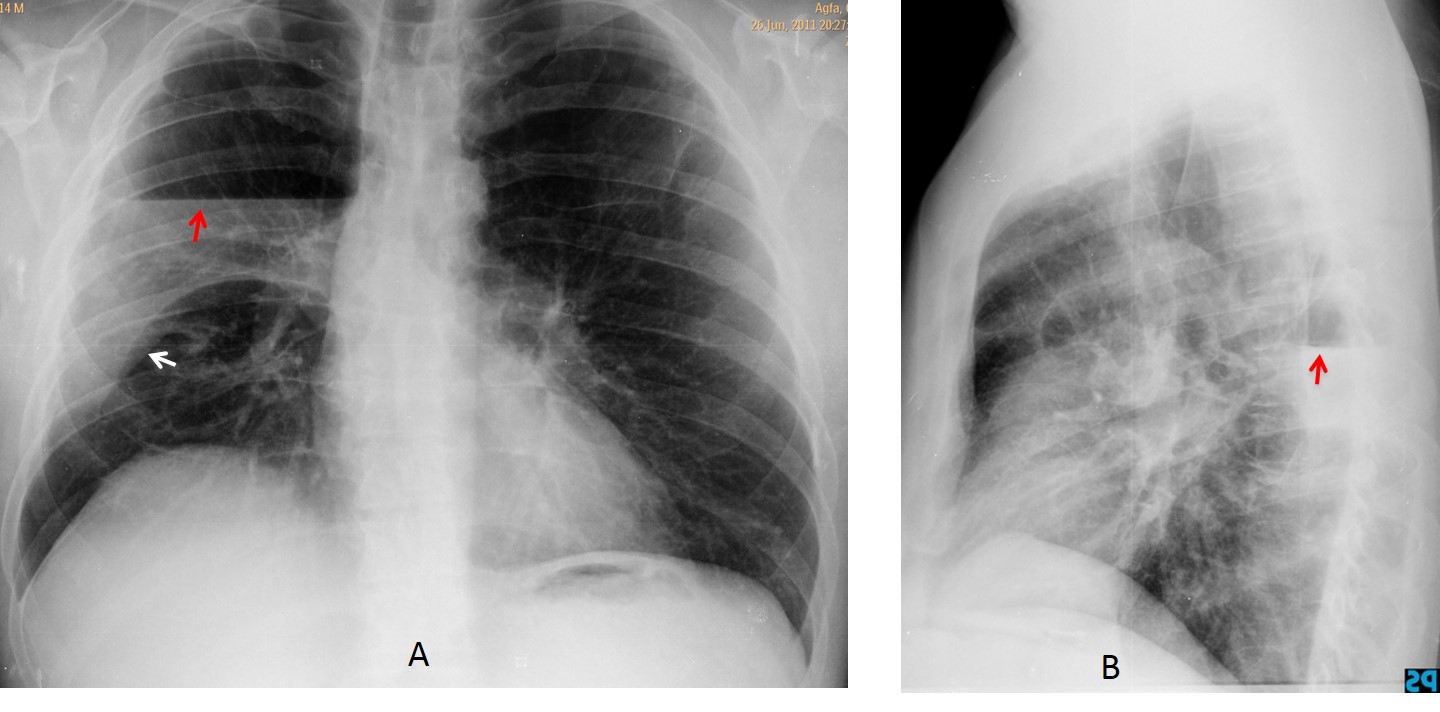
Fig. 7
Fig. 7. 48-year-old man with neurofibromatosis and fever. Chest radiographs show a central air-fluid level (A and B, red arrows), which should be in the pleura because of the different lengths of the level and the lack of a roof. The lower margin of the fluid rests on the major fissure (A, white arrow).
Axial CT confirms the hydropneumothorax (C and D, arrows) and the partially collapsed right lung. There are numerous blebs in both lungs secondary to neurofibromatosis.
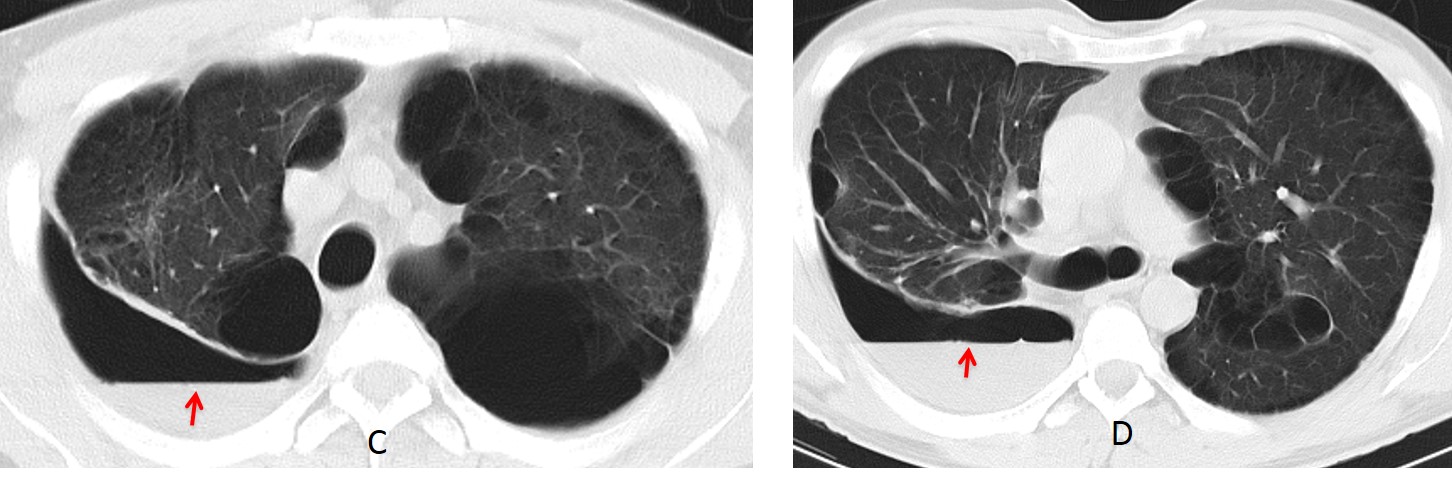
Fig. 7
An atypical presentation of an air-fluid level in the pleura occurs in pneumothorax. About 20% are associated with a small amount of pleural fluid that appears as a double horizontal line (V line) or, more commonly, as a single line in the costophrenic angle (Fig. 8). This is a helpful clue to suspecting pneumothorax when the classic findings are not obvious.
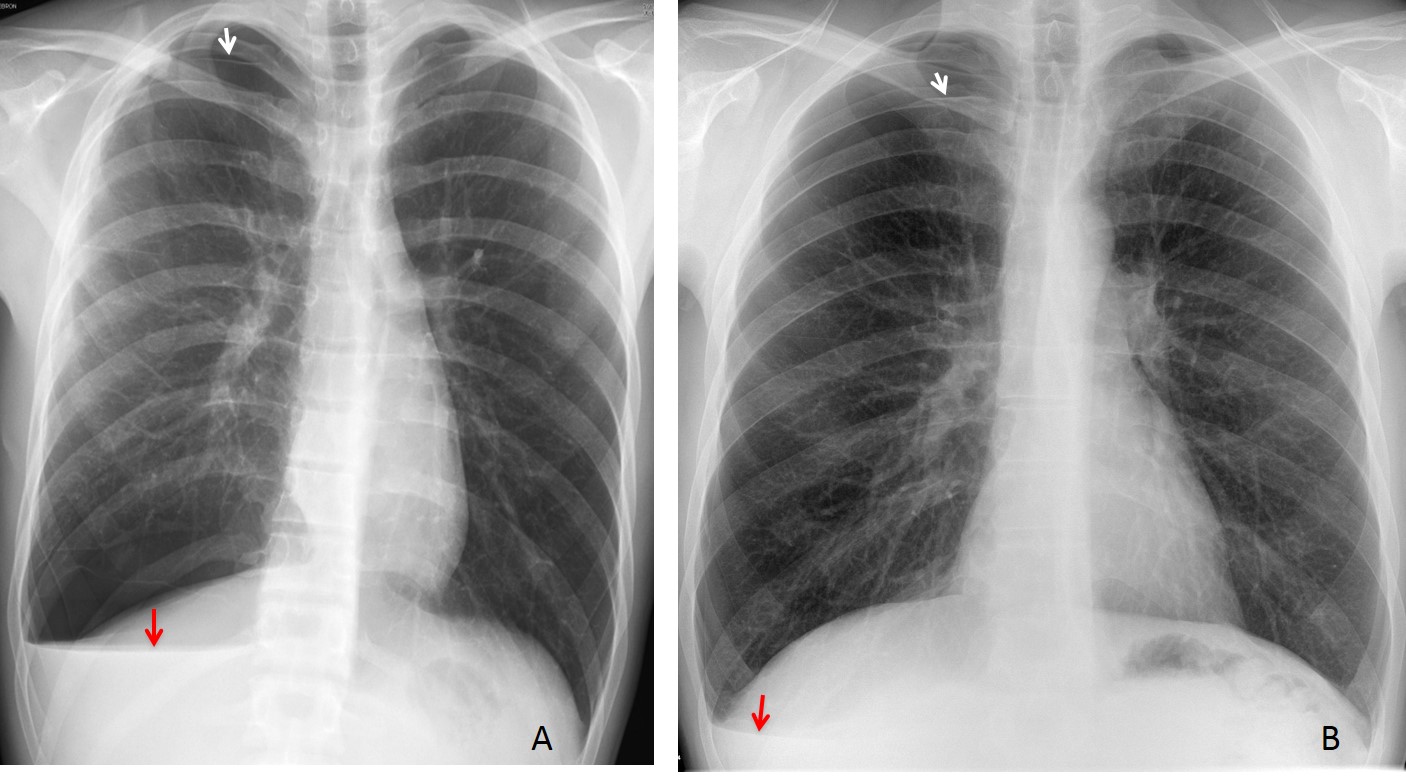
Fig. 8
Fig. 8. Two patients with pneumothorax and a V line (A and B, red arrows). The pneumothorax is barely visible in both cases (A and B, white arrows).
Another atypical presentation of a pleural air-fluid level occurs in the fissures. It is uncommon, but when present, it may simulate a thin-walled pulmonary cavity. The diagnosis is easily made by noting the spindle shape and the anatomic location within the fissure (Fig. 9).
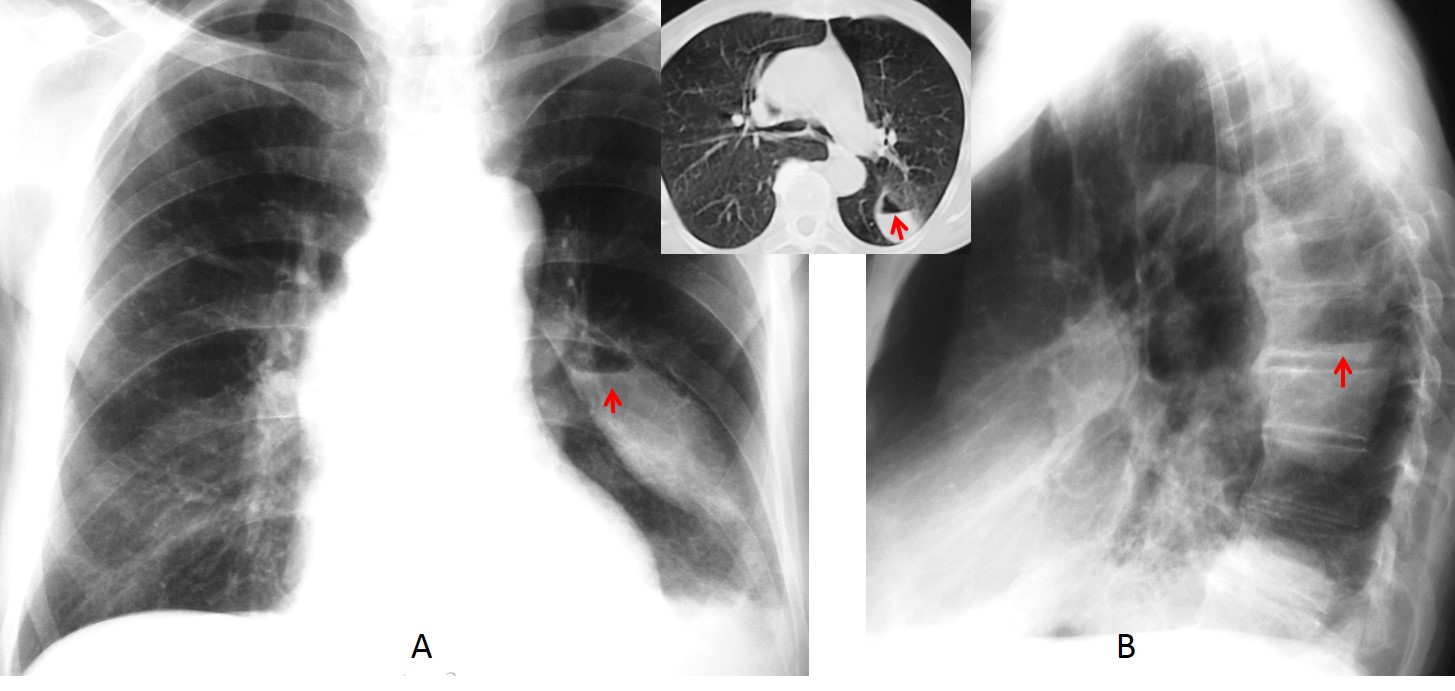
Fig. 9
Fig. 9. 75-year-old man after pneumonia. There is a residual air-fluid level in the left major fissure, visible in both radiographic views (A and B, arrows) and confirmed with CT (insert, arrow). Note the typical spindle shape of the fissure in the PA view.

Follow Dr. Pepe’s advice:
1. An air-fluid level implies a cavity and therefore, an active process.
2. The most reliable sign of malignancy in lung cavities is a nodular inner wall.
3. Air-fluid levels in pleura are asymmetrical in the PA and lateral views.


There is thorax cavity deformation due to IV stage scoliosis. This leads to abnormal visualization of all intrathorasic structures – trachea, mediastinum are shifted to the left.
Left lung seems to be decreased in volume.
There is pleural calcification seen on the left and the horizontal line – air-fluid level in the cavity.
1. necrotizing neumonia
2. lung abscesse
3. Pleural empyema
4. Cavitary lung cancer/squamous cell ca
Are there any information about thoracoplasty?
No previous thoracoplasty
Is there any information about sputum analysis, bronchoscopy?
And how many years this patient has this scoliosis?
Are there any previous plain films?
The right lung looks normal, but this mild ground glass opacity on the level of IVth rib – this is summation?
(Seems this is the case with trick?)
It could be also the patient after lobeectomy (lll?) or pulmonectomy – is there any information abour previous surgeries?
Those pleural calcification commonly associated with asbestosis exposure
Too many questions 😉
No previous surgery
Scoliosis since youth
Pleural calcium associated to asbestos is usually bilateral
Severe scoliosis.
Loss of volume of the left hemithorax (previous lobectomy?).Diffuse left pleural calcifications and rectification of the left bronchus. Hidroaereal level. If personal history of TBC, we have to think on sobreinfected bronchopleural fistula…
I agree with stated findings of Olena and MK.
Severe dextroscoliosis, decreased left lung volume, left-sided pleural effusion with pleural calcifications.
If this is recurring, neoplasm is possible. Bronchopleural fistula may be present if there is a history of TB.
In addition to the above mentioned statements I would add asbestosis-related disease and keep in mind probably diffuse pleural mesothelioma if there is known inhalational exposure to asbestos fibres.
Unilateral pleural calcification is usually associated to previous infection.
Fistola bronco pleura per la presenza di livello idro-aereo, nella cavità’ pleurica..
Greetings,
– marked deformity in the chest wall due to the severe thoracocervical rotatory dextroscoliosis.
– extensive pleural calcification in the left chest (DDX: hx of tuberculous pleural disease, hx of hemothorax/empyema, hx of talc pleurodesis).
– ill-defined peripheral opacity over the right middle zone (true lung lesion vs. chest wall lesion/breast tissue shadow), and if its a true lung lesion, then it might represent an infection or a neoplasm.
thanks
At this stage, it is obvious that the most likely diagnosis is broncho-pleural fistula. Congratulations to MK, who was the first to state unequivocally that the patient had a BPF.