I would like to begin a new subspecialty with the case of a 58-year-old male with a palpable nodule in the left breast.
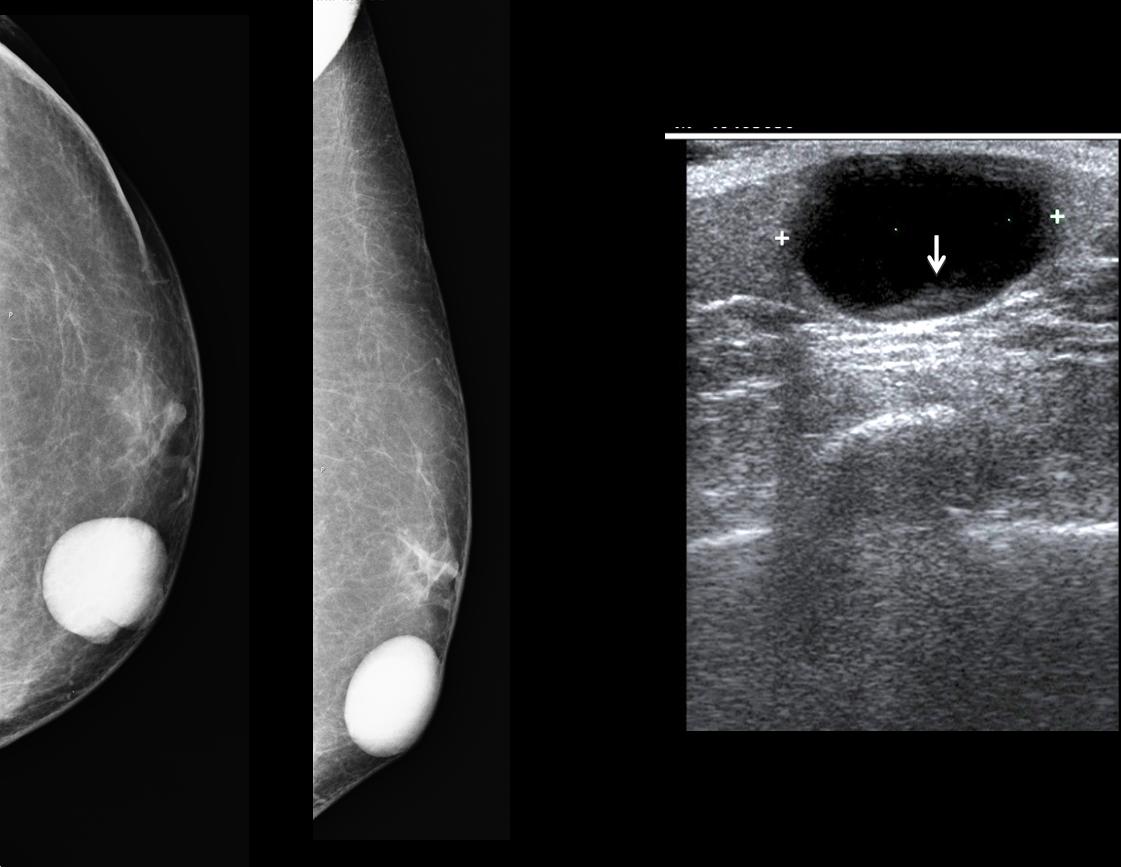
Findings: Mammograms show a rounded nodule in left breast (arrows), reasonably well defined but with contour irregularities.
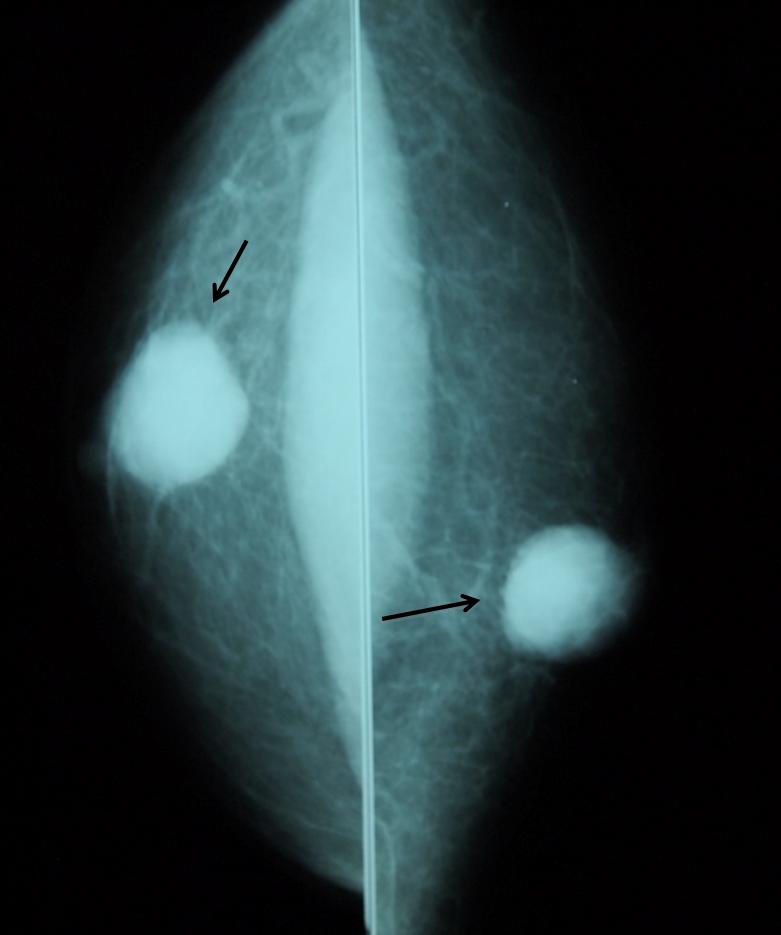
Fig. 2
The most common cause of a palpable lesion in the male breast is gynecomastia. However, in men older than 45 years, the uncommon malignant nodule should always be excluded. When the mammogram shows a nodule, an ultrasound examination should be done. In this particular patient, US confirmed a solid lesion (arrows), and biopsy yielded malignant tissue.
Final diagnosis: intraductal carcinoma of male breast.
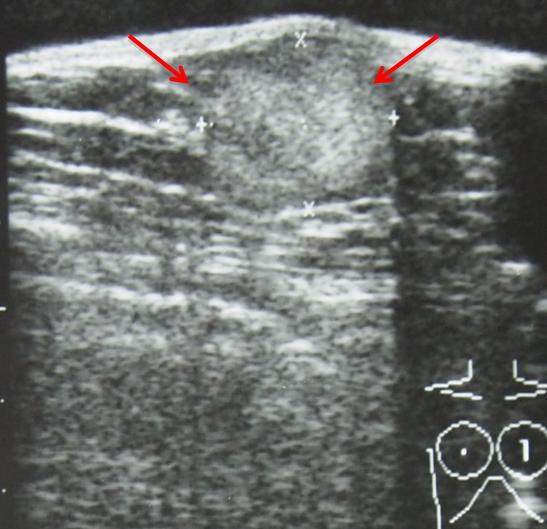
Fig. 3
Carcinoma of the male breast represents less than 1% of all breast neoplasms.
The lesions have the same mammographic and sonographic characteristics as those in females. As occurs in women, the incidence increases with age.
It has been said that their prognosis is poorer than in women, but this is due to the fact that they are often detected at higher stage than women, owing to delay in diagnosis (no screening programs in men).
All histologic types occur; papillary carcinoma is more common in men than in women.
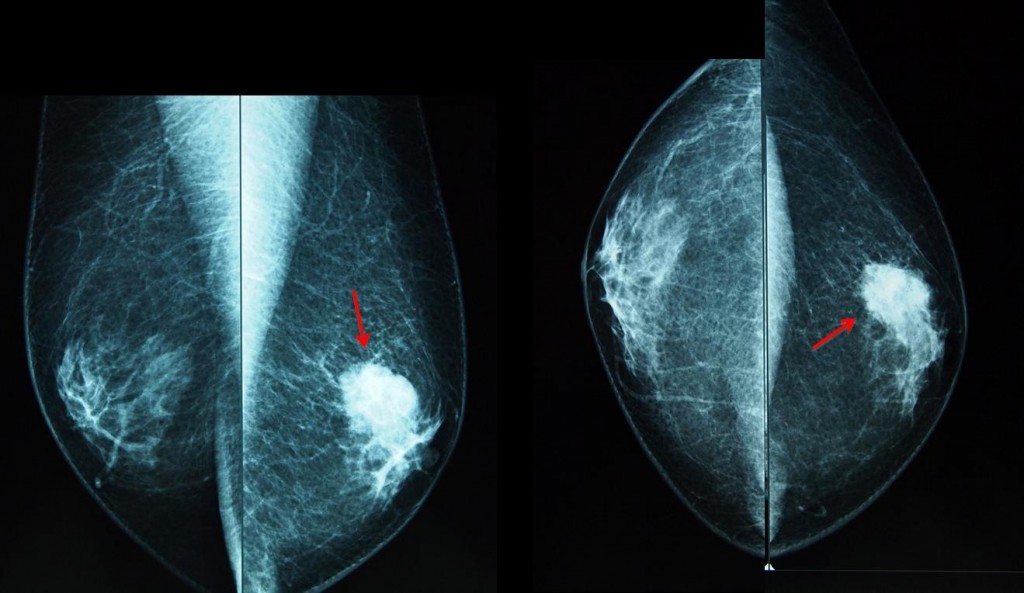
Fig. 4
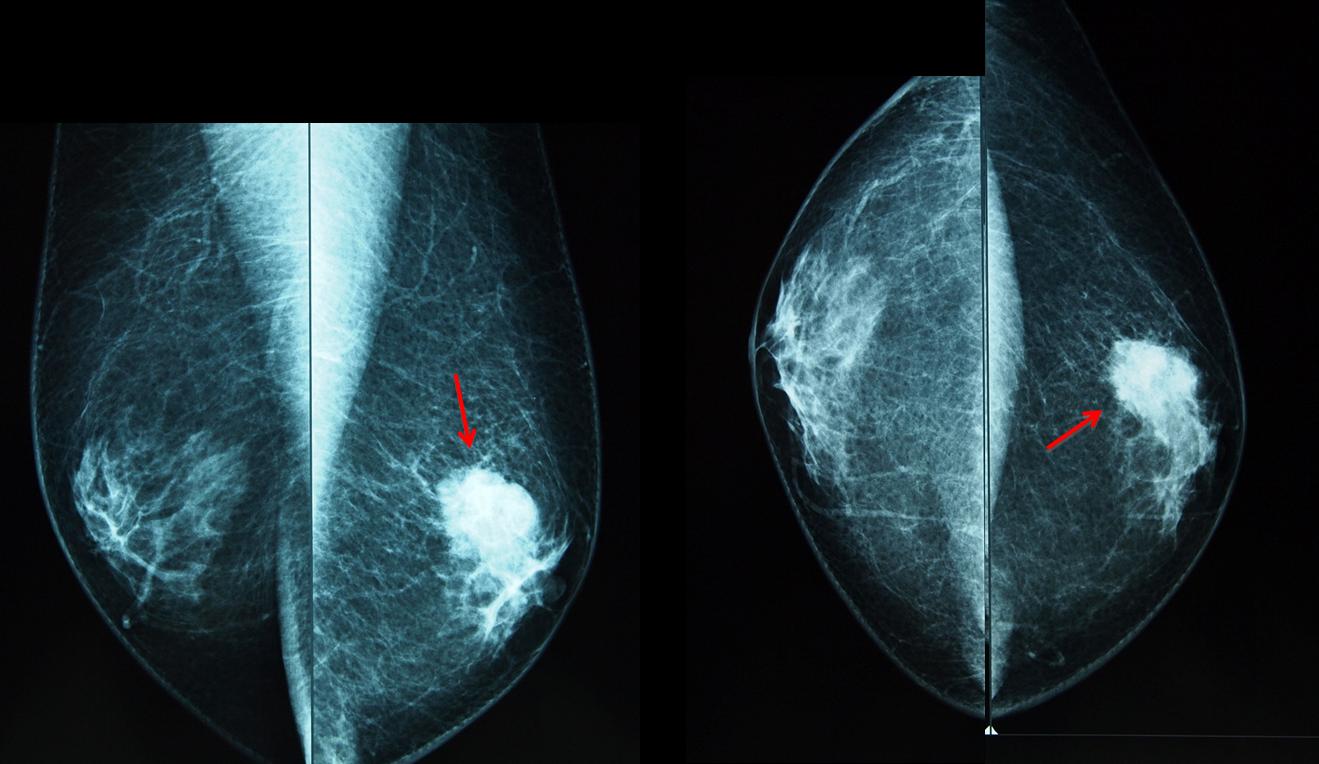
Fig. 4 is a 53-year-old man with gynecomastia and a palpable left breast nodule (arrows). Note the irregular contours of the nodule, which is located eccentrically from the nipple. Histologic diagnosis: ductal carcinoma.
Differential diagnosis
Gynecomastia is the most common abnormality of the male breast. Nodular gynecomastia should not be confused with a real nodule. Mammography and ultrasound examination will demonstrate the typical appearance of mammary tissue (arrows), excluding further work-up.
There is no evidence that gynecomastia increases the likelihood of malignancy
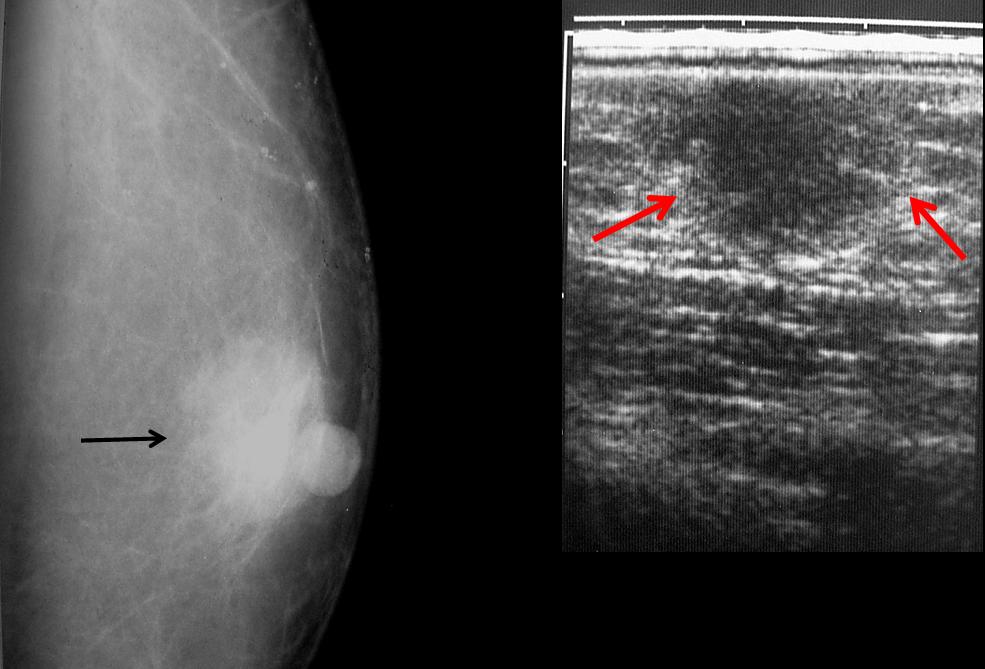
Fig. 5
Epidermal inclusion cyst is a dermic tumour that is well-defined and adherent to the skin. Ultrasound confirms the typical cystic appearance, with some debris in the dependent area (arrow).
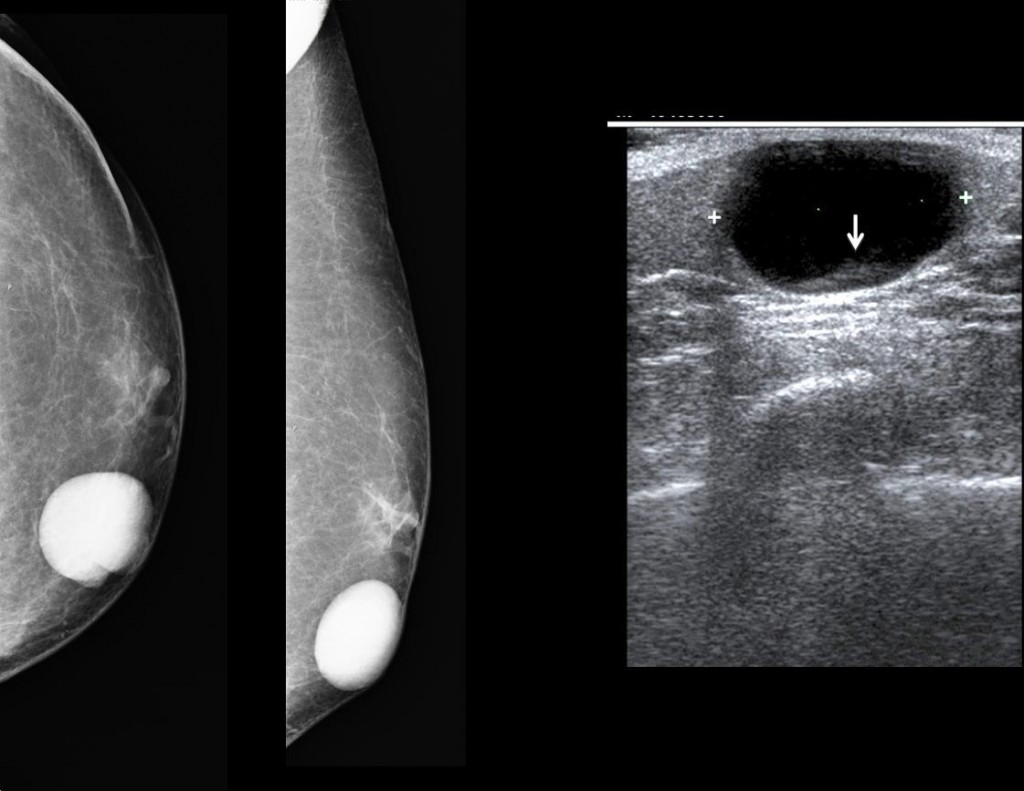
Fig. 6
Fibradenomas are extremely rare in men. The male breast is composed of fat and remnants of ductal tissue; lobular tissue does not develop. Therefore, lesions that originate from the lobules such as fibroadenomas are practically non-existent in the male breast.

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
Gynecomastia is the most common abnormality of the male breast
A solid breast nodule in a man older than 45 years should be investigated to rule out malignancy
Imaging manifestations of breast carcinoma in men are the same as in women
Suggested reading: Imaging characteristics of malignant lesions of the male breast. RadioGraphics 26:993-1006, 2006
Case prepared by Elena Rabanal, MD




There is a superficial well-defined dense mass which is clinically palpable with coarse calcifications. Invasive ductal carcinoma is an important differential. However, it raises the skin and thus, is most likely in keeping with an epidermal inclusion cyst.
CC and MLO views showing a dense mass with relatively well defined/circumscribed margins.
No surrounding architectural distortion, no associated skin thickening, no coarse calcifications are evident (however given the low resolution of this image, we cannot exclude fine pleiomorphic branching type of micro-calcifications).
Fatty composition of the remaining breast parenchyma.
Axillary lymph nodes are not visualised in the field of view.
With regards to the differential diagnoses:
1. Fibroadenomas should have a long axis oriented along the chest wall, with a lobulared margin and low short axis ratio – in this case the lesion is circular.
2. Carcinoma is also not probable – given the very well defined borders. A carcinoma this large would most probably have an irregular border…with associated architectural distortion and skin thickening.
3. Nodular gynaecomastia is more lucent, and shows an internal preserved pattern of breast fatty-glandular tissue.
4. Given the size, high density of this lesion, together with the well marginated borders, it is mostly compatible with an epidermal inclusion (sebaceous) cyst.
The next step would be an ultrasound.
epidural inclusion cyst
Formazione omogeneamente rx-opaca, a margini regolari , al di , sotto del piano epidermico, “senza” distorsione dell’archiettura ghiandolare e “senza” distorsione del capezzolo che è “in situ”.Si esclude per prima cosa il CR mammario.Si può escludere anche il fibro-adenoma che è tipicamente “giovanile ” e piu’ profondo. Si può escludere la ginecomastia nodulare, perchè unilaterale ed inoltre a questa età dovrebbe essere indotta da squilibri ormonali e-o terapie farmacologiche,non riferite nell’anamnesi. La diagnosi è pertanto di cisti, da inclusione di sebo e cheratina :cisti epidermoide. Un bravo ecografista, con sonde opportune è in grado altresì di individuare il sottile tramite ipoecogeno di collegamento all’esterno: a volte basta “spremerle” per fare uscire il contenuto, tipicamente biancastro e maleodorante.
epidermal inclusion cyst but for exact diagnosis needs sonography
Only five responses and all of them in favor of epidermal inclusion cyst! No doubts?
I think that these are the CC projection of both breasts. Gynecomastia is usually bilateral.
On mammography, gynecomastia can be nodular, dendritic or diffuse. In nodular gynecomastia, a nodular, mass-like lesion is seen in the retro-areolar region.
4. Nodular gynecomastia.
There are views of the left breast (CC and lateral). Sorry about the misunderstanding
Gentile collega,” sicuramente” una ecografia ha “preceduto” la Mammografia: allora perche’ far vedere “Solo” la mammografia? La Vostra diagnosi definitiva è certamente frutto di una diagnostica integrata( Eco+Mammo).Vedendo la “sola” mammografia l’ipotesi più plausibile è la cisti epidermoide.Sbaglio?
Sorry, I disagree. Epidermoid cysts are very well defined (an example will be shown in the discussion), whereas the case shown has irregularity and spiculation of the borders. Diagnosis of carcinoma was suggested in the mammogram, which was the initial examination. And confirmed with echography and biopsy.
Teaching point is that any nodule in a male over 45 y.o. should be suspicious of carcinoma until proven otherwise. As you well know, fibroadenomas are very unusual in males.
Dr. Pepe is no strange to mammography. He presented his PhD thesis in carcinoma of the breast.
From here, the borders are well defined…very well defined.
That explains the 5 answers favouring epidermal inclusion cysts :).
Ultrasound is also mandatory.
Sono d’accordo con Kelvin: i contorni si vedono ben deniti, in piu’ non c’è distorsione della struttura ghiandolare nè compromissione dello strato cutaneo sovrastante nè del capizzolo, che sono tutte “vicine” alla opacità. Molto probabilmente ciò che rende “interessante” il caso è appunto ” l’apparente” benignità della massa alla mammografia, ma sono è tutta disattesa la semeiotica radiografica classica!
I will go with nodular gynecomastia even though it is not a typical position. But we have a male patient!
Although gynecomastia is the most common lesion in males, it looks like breast tissue. In this case, the appearence is nodular.
Views showing a dense mass with relatively well defined/circumscribed margins.
With regards to the differential diagnoses:
– Nodular ginecomastia, mass-like lesion is seen in the retro-areolar region in patient male over 50 years old with hormonal prostate hyperplasia.
– High density of this lesion, together with the well marginated borders, it is mostly compatible with an epidermal inclusion.
-Diagnosis of carcinoma was suggested in the mammogram.
– fibroadenomas are very unusual in males.
Option 4 Nodular ginecomastia
PD: I apologise about my English ,not so good…
Don’t worry about your English. Mine is worse. The important thing is a correct approach to the case. See answer to Maria, above.