Today I’m presenting a 55-year-old male with pain in the right hemithorax.
1. Pulmonary infarction
2. Pneumonia
3. Carcinoma
4. None of the above
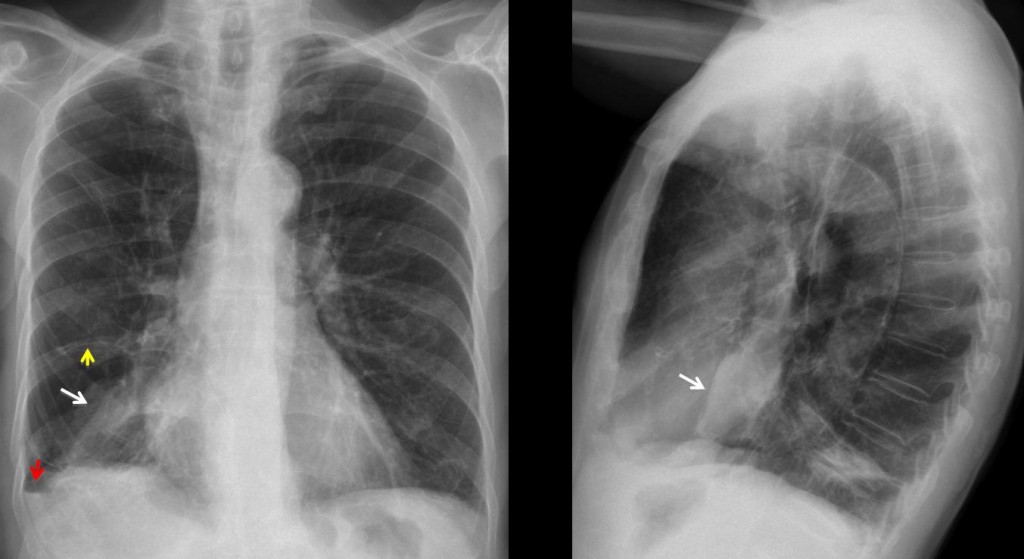
Fig. 1
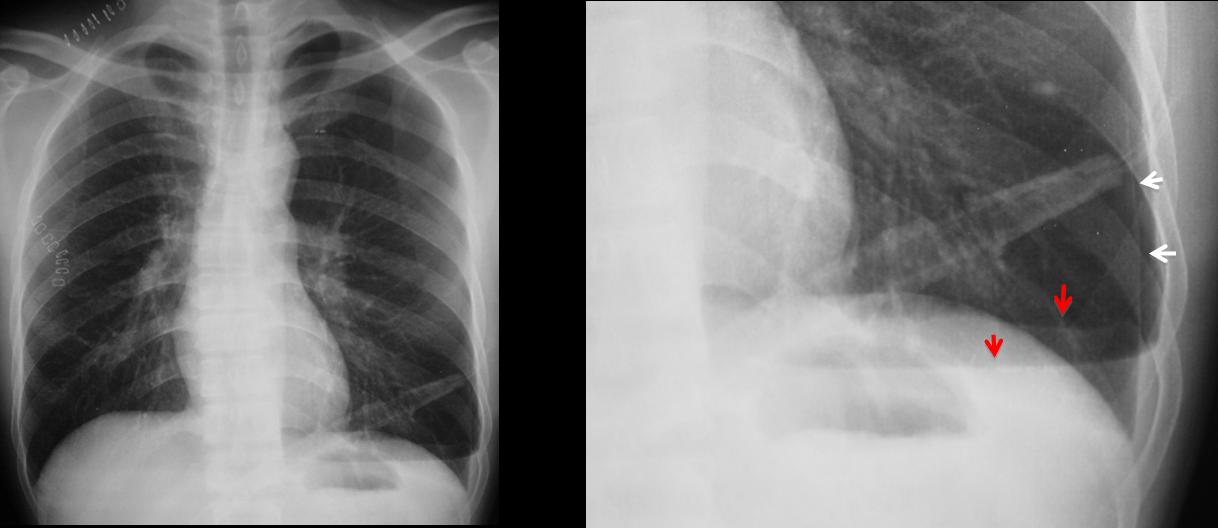
PA and lateral radiographs show an ill-defined opacity at the right lung base (white arrows). The clue to the diagnosis is a small air-fluid level at the costophrenic angle (red arrow). This finding is known as the V line and it is highly suspicious for pneumothorax. A thin line visible in the PA view (yellow arrow) marks the edge of the lung.
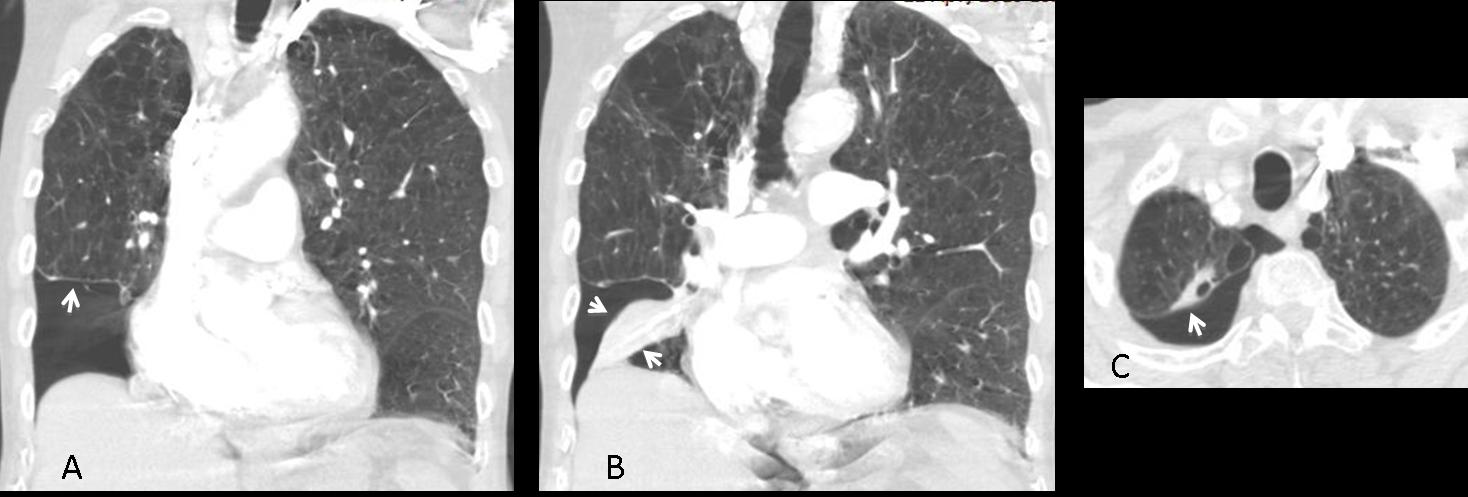
CT confirms the basal pneumothorax (A, arrow), which has caused segmental collapse of the right lower lobe (B, arrows). In the axial view, the pneumothorax is seen to extend to the lung apex (C, arrow). There are bullae throughout both lungs.
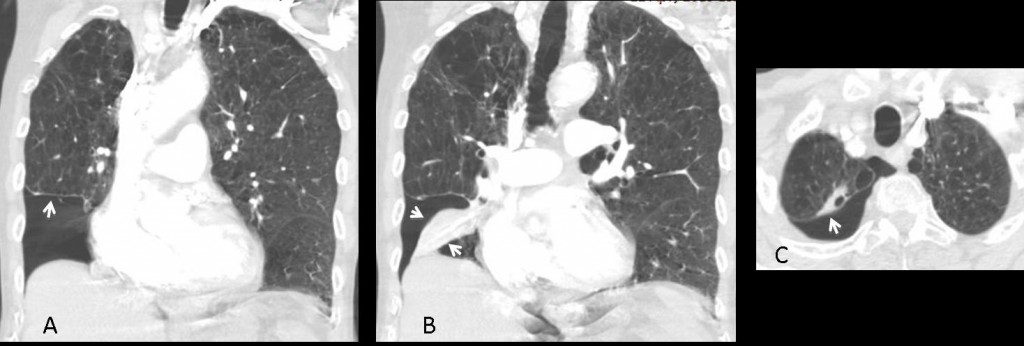
Fig. 2
Final diagnosis: basal pneumothorax with secondary segmental lung collapse
The V line is described as two intersecting lines forming a V, with the apex pointing laterally. It represents a small amount of pleural bleeding secondary to separation of the two pleural layers. One of the lines of the V is sometimes absent, as in the case presented.
The V line is not always seen in pneumothorax, but when it is present, it is a useful indicator of a small or overlooked pneumothorax. A confirmatory expiration film should then be performed.
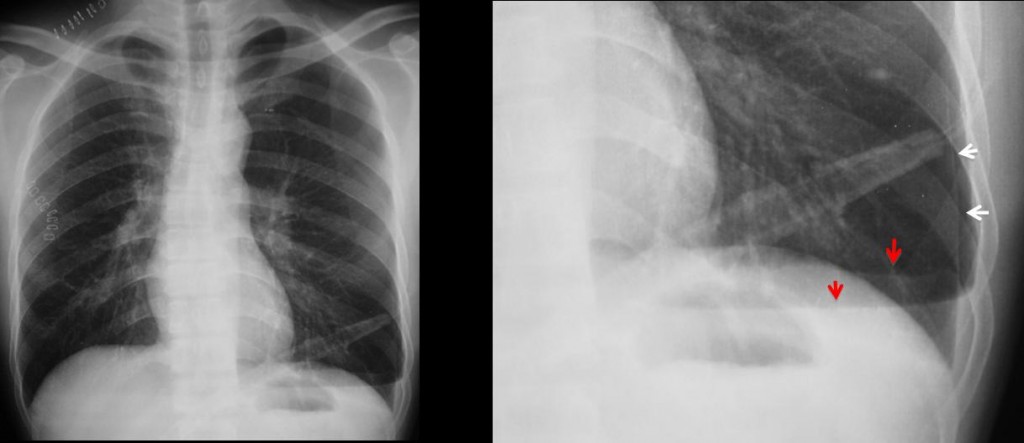
Fig. 3
Typical V line. Note the two branches of the V, better seen in the cone down view (red arrows), where the pneumothorax is more evident (white arrows).
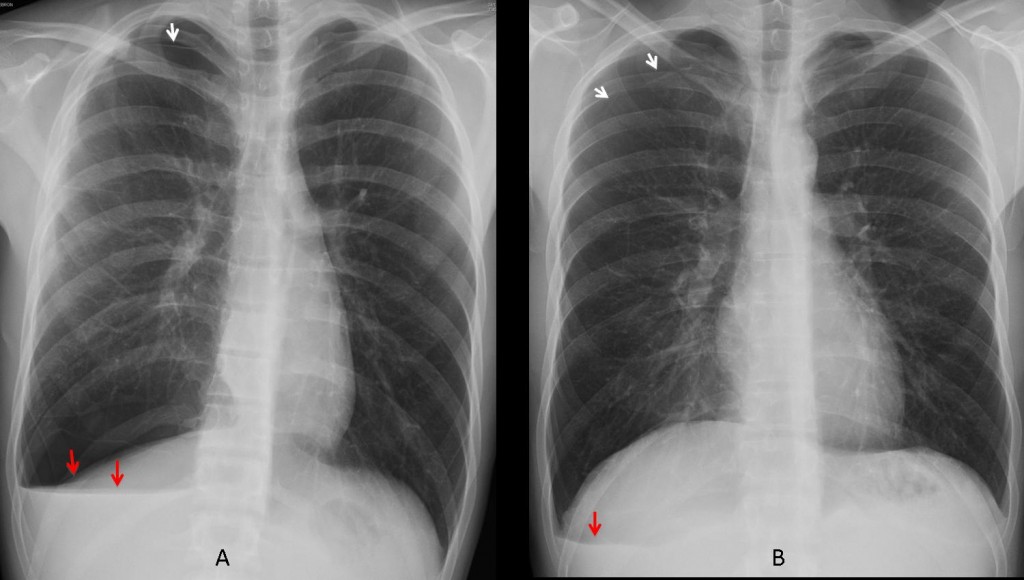
Fig. 4
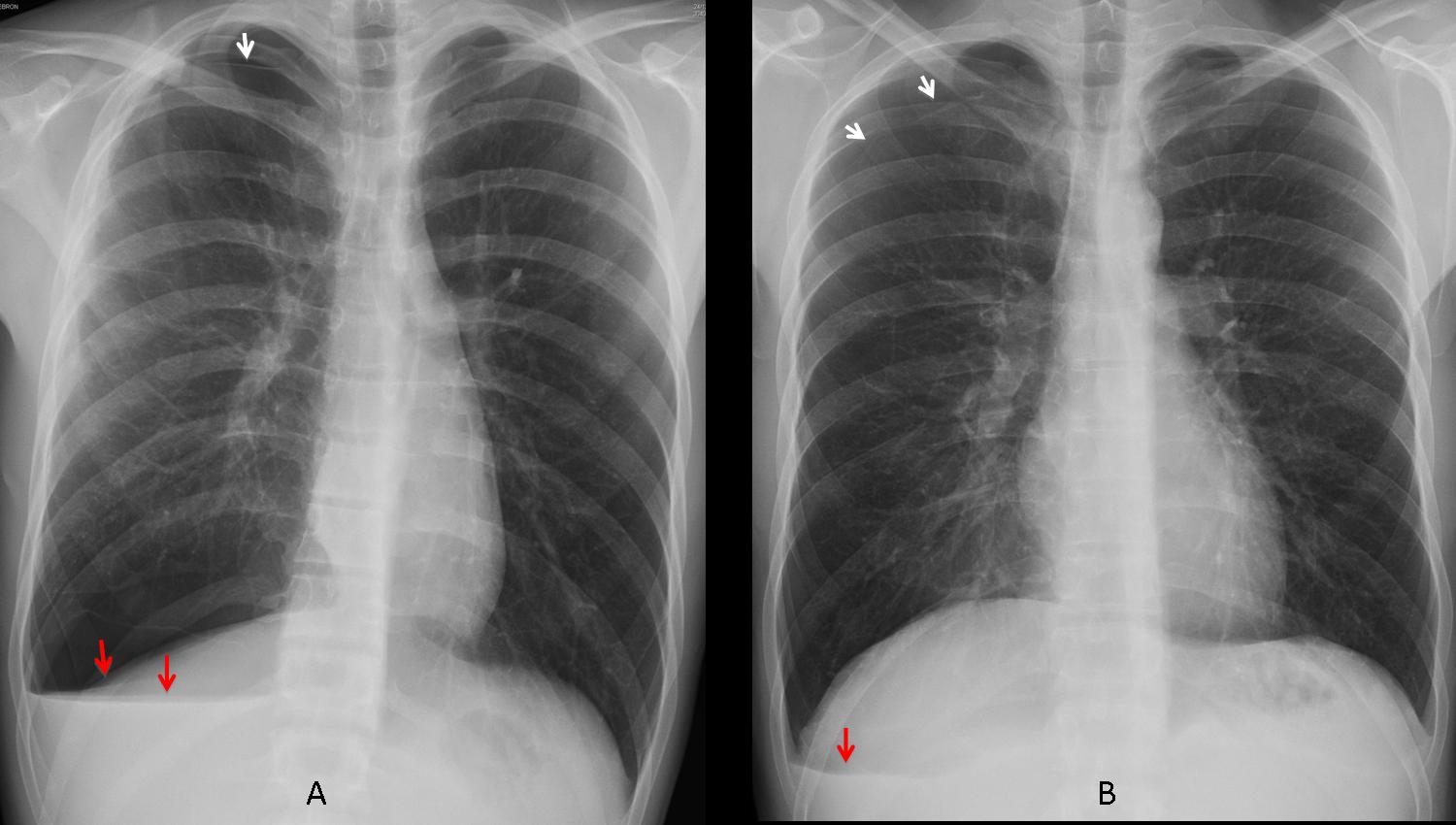
Two cases in which the V line alerts to a small pneumothorax (A, B arrows). The V line has two branches in A (arrows) and only one in B (arrow).
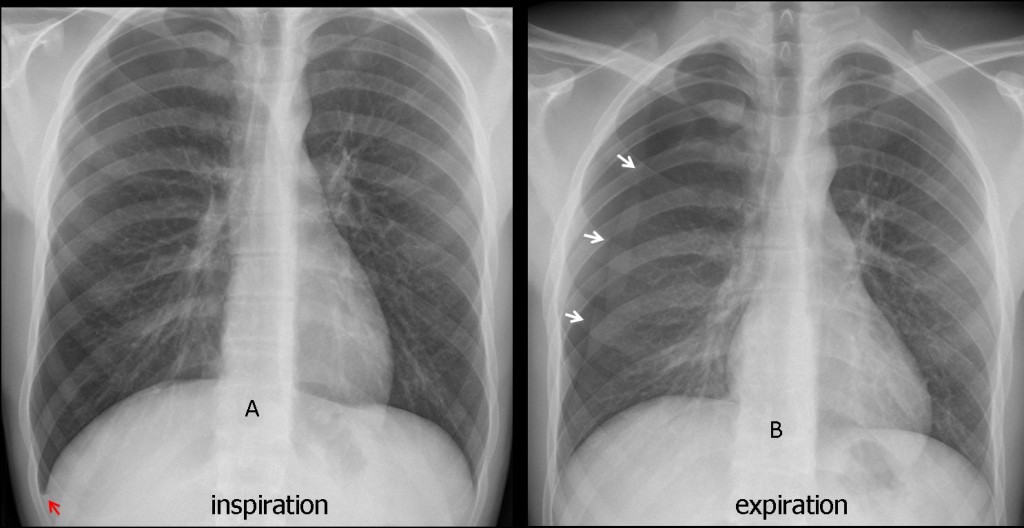
Fig. 5
Pneumothorax poorly seen in the inspiration film, but suspected because of a tiny V line (A, red arrow). Expiration film shows the pneumothorax to better advantage (B, white arrows).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- A small pneumothorax may be missed because the free lung edge is barely discernible.
- The V line is a useful ancillary finding to suspect a pneumothorax. Confirm with an expiratory film.
Case prepared by Dr. Pepe







There are some fibrotic changes in the right lung, pleural fluid, and irregular (not smooth ) border of right hemidiaphragm ( maybe some subpneumonic fluid collection ). there is also a RL cystic lesion with solid part (maybe crescent sign) and atelectasis of a part of RLL. Finally i do not like the right first rib . I would not be surprised if the cystic lesion is a diaphragmatic hernia.
Pulmonary infarction
round atelectasis
Atelektasis.
Gobba di Hampton,Area di consolidamento,non visibilità arteria polmonare nelle diramazioni periferiche + clinica( dolore acuto base toracica) , se anche i D-dimeri alti = tromboembolismo con infarto polmonare.
So far, the diagnosis has not be mentioned. Keep trying, before tomorrow’s answer!
Il quadro radiologico di base è una BCO, con grossa bolla aerea alla base polmonare dx ove coesistono aree di consolidamento parenchimale: se pensiamo alle complicanze di una BCO , in questo caso, potremmo ipotizzare aree di consoldamento sub-atelettasico da tappi di muco e/o una sovrainfezione da aspergillosi polmonare.Terapia antibiotica e mucolitici , con controllo dopo 8gg e rivalutazione del quadro, se non risolto, con una TAC( cosa che Voi avete certamente fatto).
Right lung base shows:
1- Peripheral round opacity.
2- Loss of volume in the form of elevation of right hemidiaphragm and downward displacement of right hilum.
3- pleural thickening.
So, I think that the principle diagnosis is round atelectasis
4.None of the above.Вероятно- Перфорирала тънкостенна киста в 3/0, с дренирано към плеврална кухина съдържимо и ограничен хидропневмоторакс.Седментна ателектаза в дясна основа.
Necrosis of pericardial fat?