Dr. Pepe’s Diploma Casebook: Case 42 – SOLVED!
Dear Friends,
To continue reviewing basic chest patterns, I present the case of a 52-year-old man with a solitary pulmonary nodule.
Diagnosis:
1. Probably malignant
2. Probably benign
3. Indeterminate
4. Need previous films
Check the images below, leave your thoughts and conclusion in the comments section and come back on Friday for the answer.

52-year-old man with a solitary pulmonary nodule
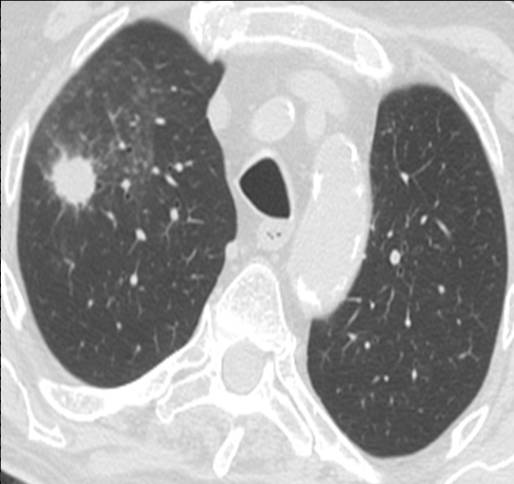
52-year-old man with a solitary pulmonary nodule
Case 42 – solution
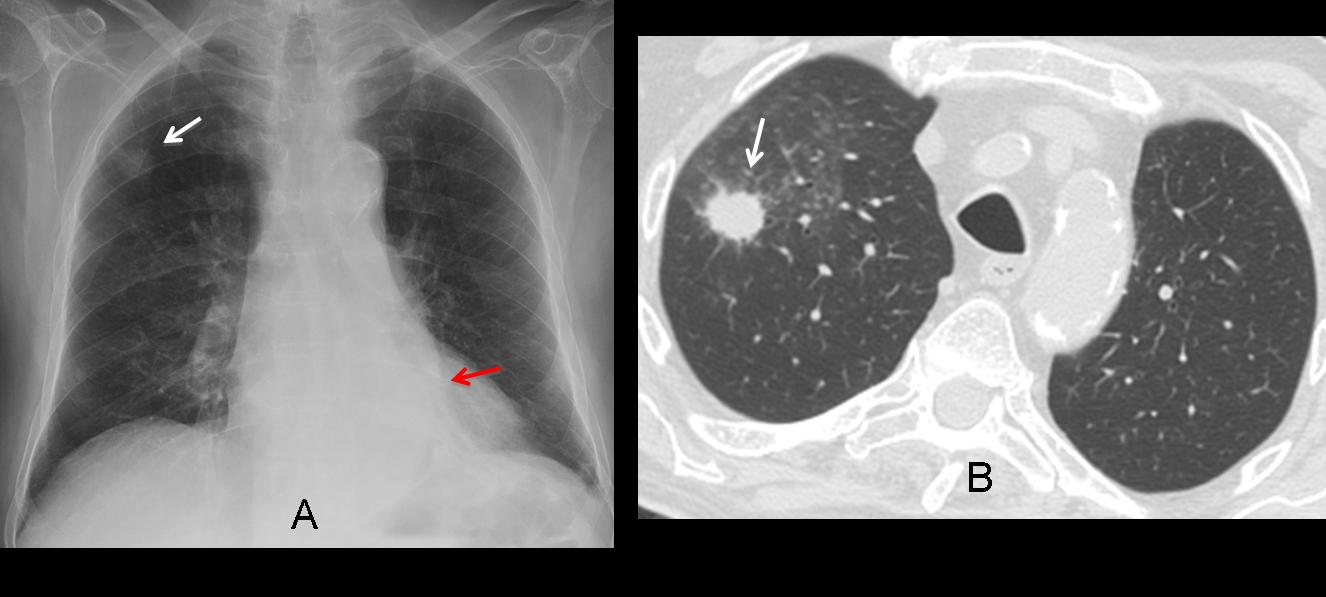
Findings: Chest PA shows a nodule in the RUL (A, arrow) and air-space disease in the LLL (A, red arrows). On CT, the nodule is surrounded by ground-glass opacity and has a spiculated border (B, arrows). The initial impression is that of a malignant nodule (option 1), but we should not omit a basic tenet in all pulmonary nodules: always compare with previous films (Fig. 1, below).
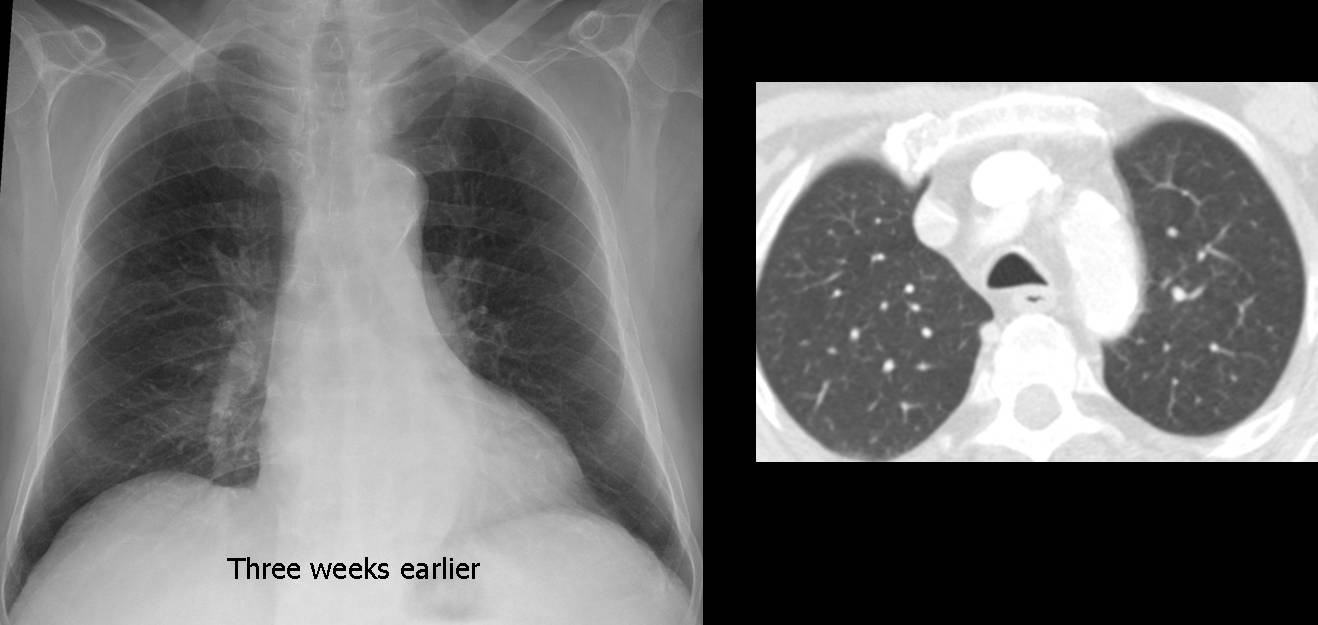
Fig. 1
Fig. 1: chest radiograph and CT performed three weeks earlier show no nodule and no LLL disease. The rapid change suggests an inflammatory process, rather than a neoplasm. The correct answer should be #4: Need previous films.
Final diagnosis: fungal infection in immunocompromised patient.
This case is shown to illustrate the basic criteria in the management of solitary pulmonary nodules (SPNs), such as looking at previous studies before suggesting a diagnosis.
SPN is defined as a well- or poorly-defined rounded opacity, measuring up to 3cm in diameter. Larger than that is considered a mass, which is very likely malignant.
SPNs are not uncommon and are usually an incidental finding in chest radiographs. The main goal is to differentiate benign from malignant nodules as accurately as possible. The fundamental question when facing an SPN is: what should I do?
I’ll give you my basic approach to SPNs, in both plain films and CT studies, to help you make the correct decisions.
The most reliable criterion in plain films is nodule growth (or lack of it). For that reason, it is essential to compare with previous films, when available. A nodule that has grown in the interval is probably malignant and should be acted upon (Fig. 2). SPN with a doubling time of 7 days or less is likely inflammatory. If no growth is evident in a period of 24 months, the nodule is likely benign and can be controlled by CT follow-up.
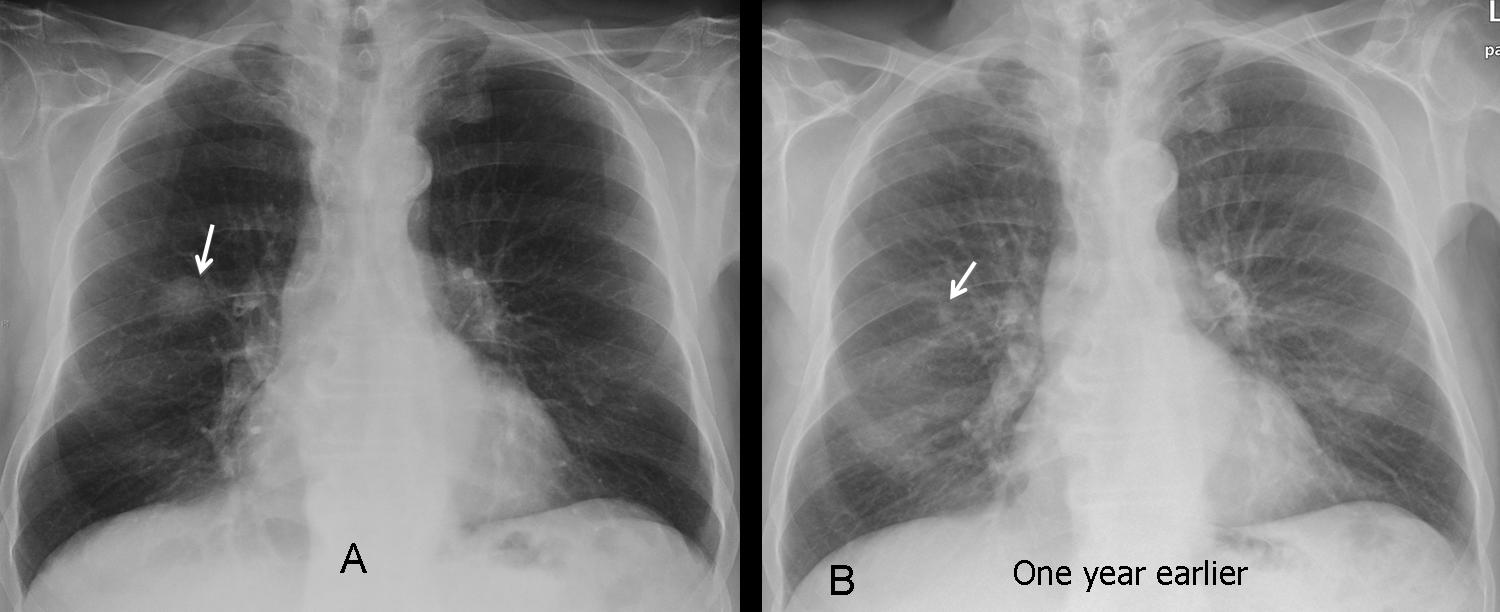
Fig. 2
Fig. 2: indeterminate nodule in the right lung (A, arrow). Plain film one year earlier shows the nodule, considerably smaller (B, arrow), which was missed at that time. Diagnosis: adenocarcinoma.
Nodule calcification in plain film is also mentioned as a reliable criterion of benignancy. In my experience, calcification is difficult to evaluate in most cases because the high KV technique used nowadays “burns” calcium (Fig. 3, below). If you do see calcification, it is a reliable sign of benignancy, but most of the time it is not visible (Fig. 4).

Fig. 3
Fig. 3: hamartoma with popcorn calcification (arrows), poorly visible in the chest radiograph.
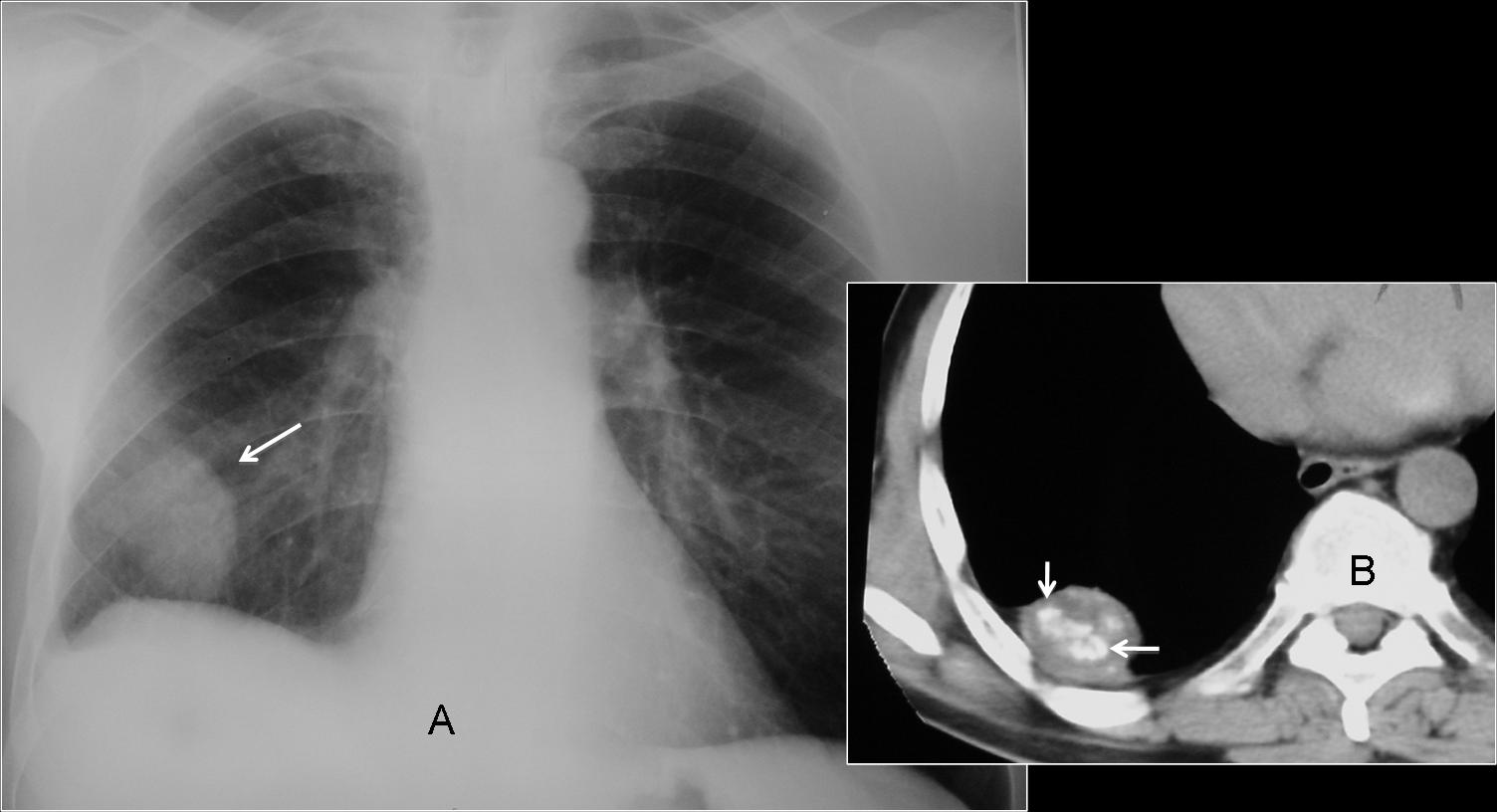
Fig. 4
Fig. 4. Large nodule in the lower lung (A, arrow) apparently not calcified. CT shows obvious calcification within the nodule (B, arrows).
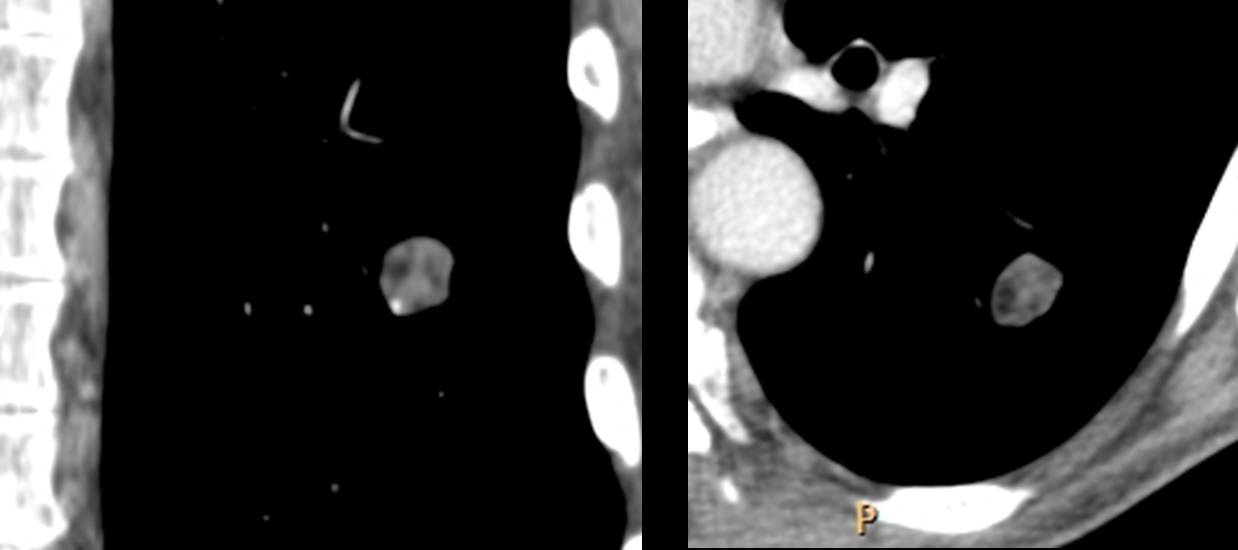
SPN assessment should be completed with CT, which provides additional criteria to differentiate benign from malignant. Before going into these factors, I would like to test your knowledge with the following coronal and axial CT of an SPN discovered in the pre-op study of a 52-year-old man with carcinoma of the colon. What would your diagnosis be?
1. Probably benign
2. Probably malignant
3. Malignant
4. Benign
The most common CT criteria to evaluate SPNs are:
1. Intranodular fat
2. Intranodular coarse calcifications
3. Nodule contour (spiculated, irregular, well-defined)
4. Intranodular air bronchogram and bronchiologram
5. Cavitation
Intranodular fat (-40 to -120 HU) is a reliable sign of benignancy. In this case, CT shows a round SPN with areas of fat attenuation. (Fig. 5 A and B, arrows). The correct answer should be # 4: Benign. The great majority of cases correspond to hamartomas, although granuloma with caseum may show similar findings in rare cases. In my experience, intranodular fat is practically pathognomonic for hamartoma.
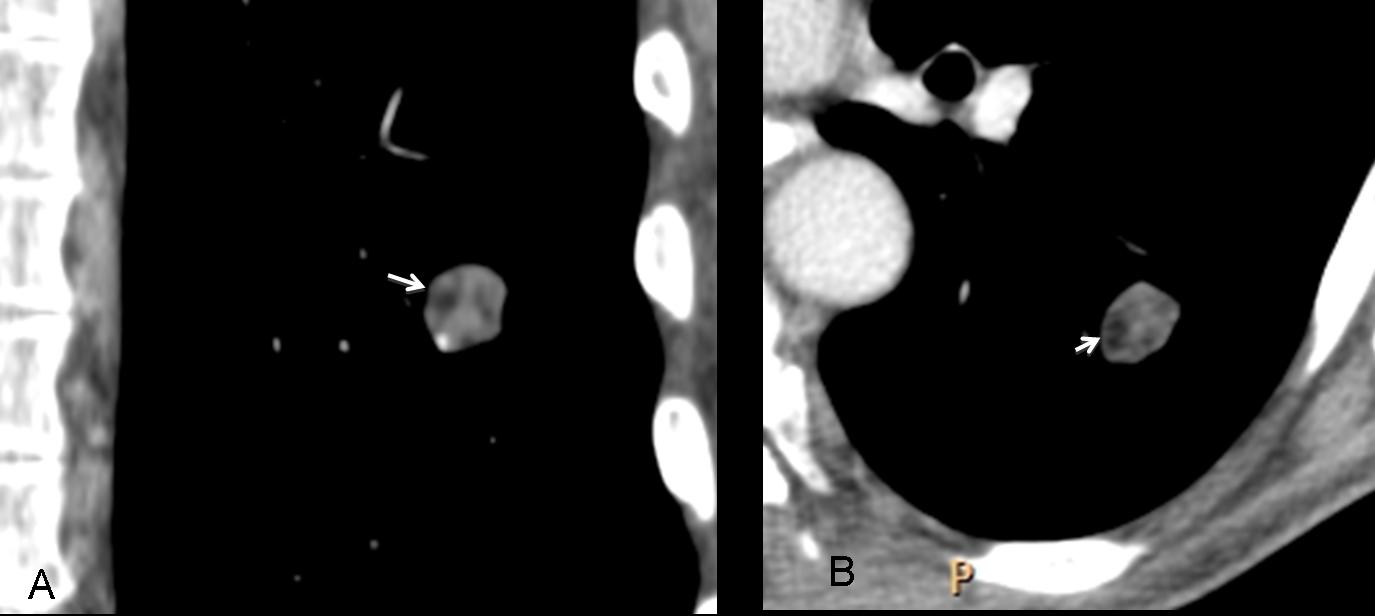
Fig. 5
Fig. 5. Small SPN with areas of intranodular fat (arrows). This finding is virtually pathognomonic of hamartoma.
Coarse intranodular calcifications are a strong sign in favor of benignancy, usually seen in hamartomas and granulomas. Uncommonly, some malignant lesions may have coarse calcifications, such as carcinoids, sarcomas (primary or metastatic), and treated metastases. Although 15% of carcinomas may show stippled calcifications, they are quite different from coarse calcium and occur very rarely in nodules less than 3cm.
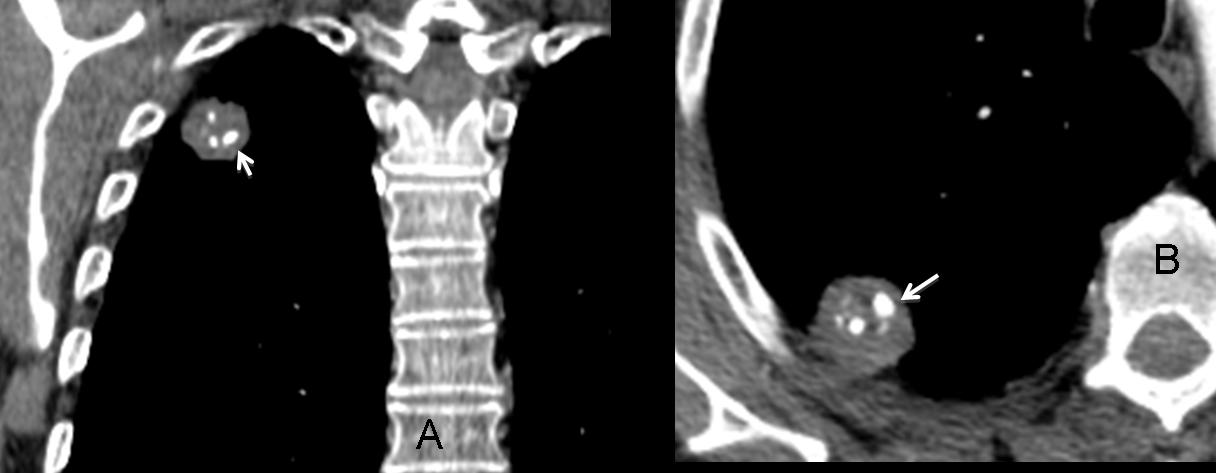
Fig. 6
Fig 6. CT shows a round well-defined SPN with several coarse calcifications (A,B, arrows). Diagnosis: hamartoma.
The contour of the nodule is another helpful criterion. An irregular contour is highly suspicious of malignancy (Fig. 7A, arrow). A well-defined contour (Fig. 7B, arrow) points to benignancy. However, it is important to remember that about 20% of carcinomas are well-defined (B, arrow).
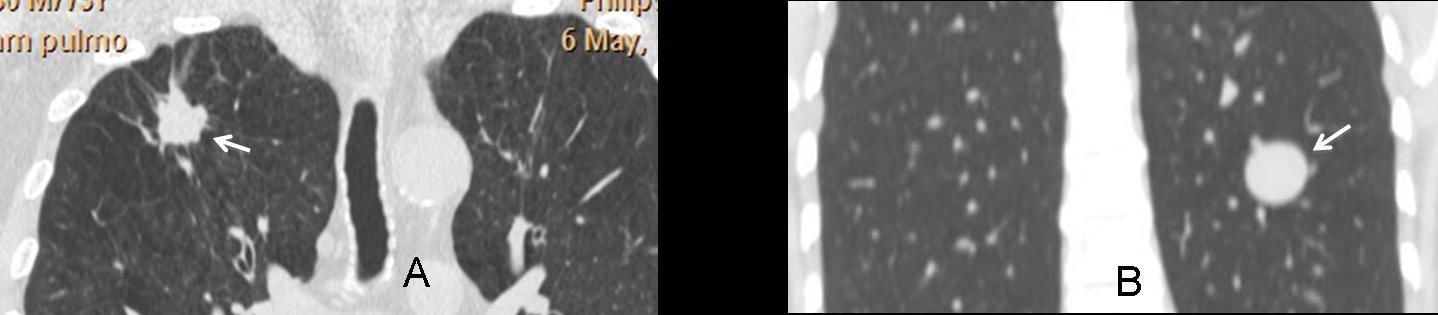
Fig. 7
Fig 7A: SPN with highly spiculated borders (arrows). Fig. 7B: Another patient with an SPN with well-defined borders (arrows). Both were carcinomas.
The presence of an air-bronchogram and bronchiologram within the nodule suggests malignancy and is more frequent in bronchioalveolar carcinomas. Incidentally, this type of carcinoma may be negative on PET, as in the case below (C).
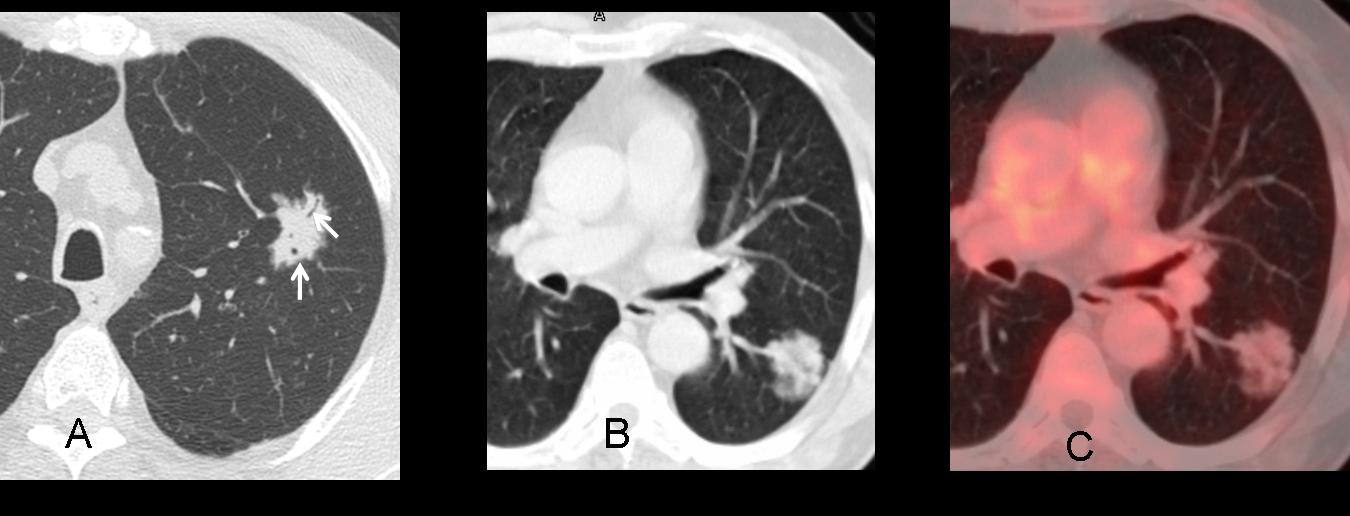
Fig. 8
Fig. 8: SPN with spiculated contour and intranodular air-bronchogram and bronchiologram (A, arrows). B,C: Another
case with similar appearance and negative PET. Both cases are bronchioalveolar carcinomas
Cavitation of an SPN is a nonspecific finding, seen in both malignant and benign nodules. It is, however, very helpful because it indicates an active process and therefore, one that requires further investigation.
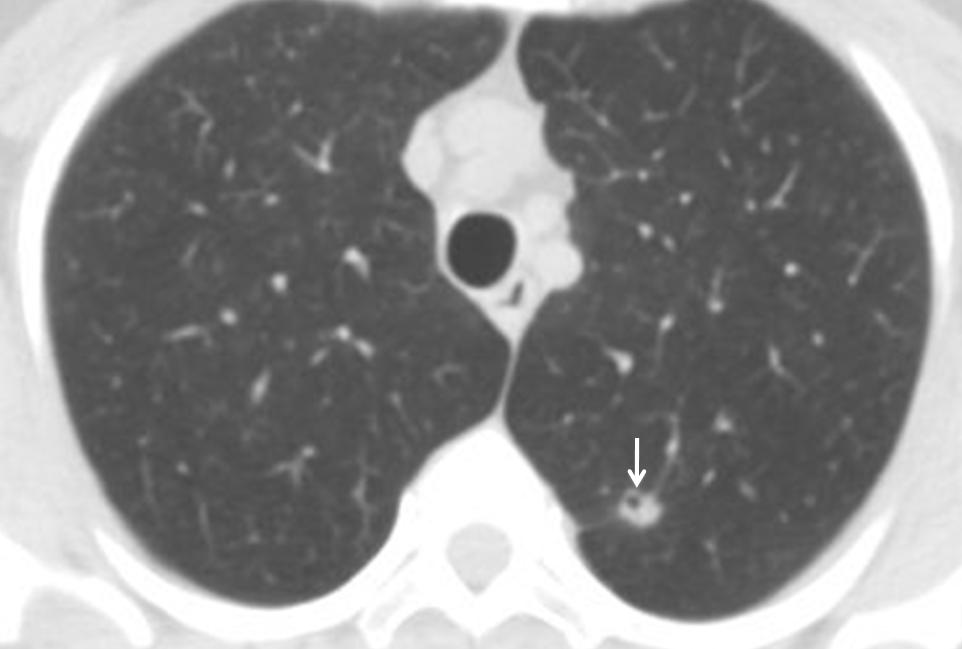
Fig. 9
Fig. 9: 45-year-old woman, smoker, with a cavitated nodule in LUL (arrow). Diagnosis: bronchioloalveolar carcinoma.
The last case is that of a 68-year-old woman surgically treated with a coronary bypass. The right upper lung nodule (arrow) was not present in the pre-op film taken one year earlier. What would your diagnosis be?
1. Probably benign
2. Probably malignant
3. Surgical complication
4. None of the above
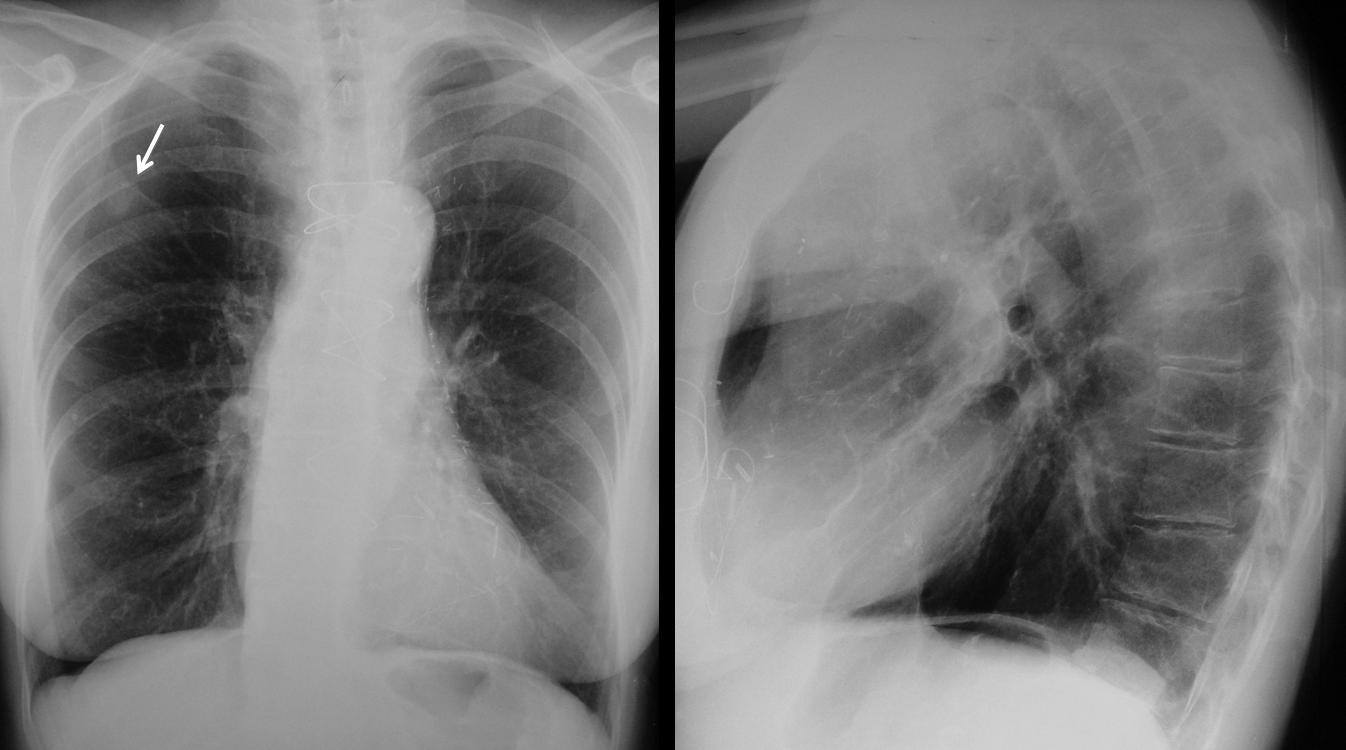
Fig. 10
3D CT reconstruction shows that the nodule corresponds to a fracture of the second right rib (Fig. 11B, arrow). It is important to remember that sternotomy can cause upper rib fractures that may later simulate lung nodules.
I’m showing this case to remind you that up to 20% of suspected SPNs are false nodules created by extrapulmonary structures, such as nipples, rib fractures or bone islands, skin lesions, etc.
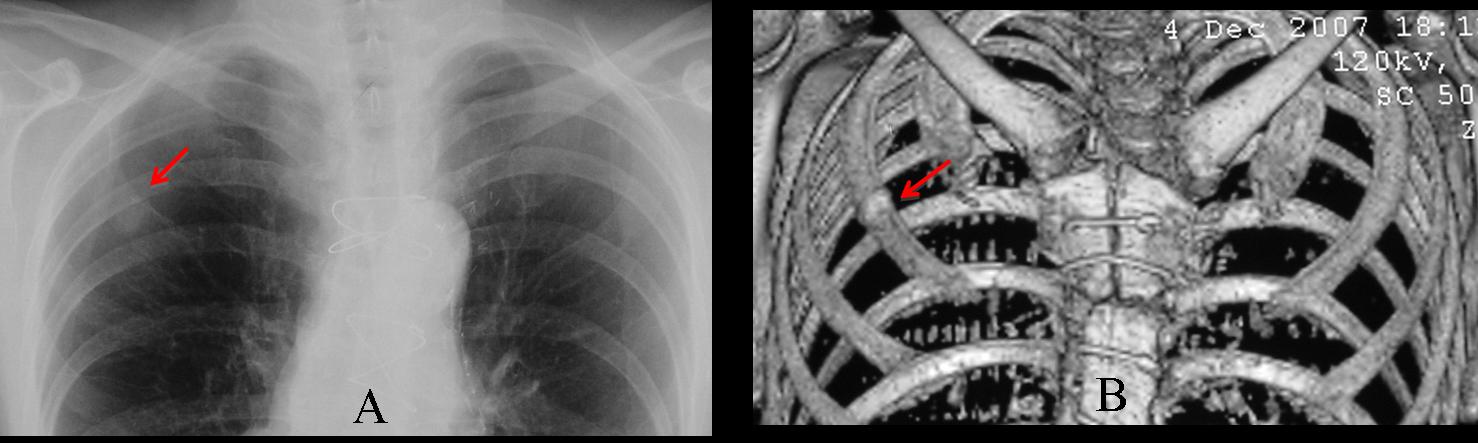
Fig. 11
Fig. 11. Post-sternotomy fracture simulating a lung nodule (A, arrow). 3D reconstruction confirms the fracture (B, arrow).

Follow Dr. Pepe’s advice:
- Growth (or lack of it) is the best criterion to evaluate SPNs in plain films
- Spiculated borders on CT are suggestive of malignancy. About 20% of malignant SPNs are well-defined
- Coarse calcifications on CT are highly suggestive of benignancy
- CT demonstration of intranodular fat is practically pathognomonic of benignancy
- Always be aware of pseudonodules!
Ref. The solitary pulmonary nodule. Radiology 239:34-49, 2006


Opacità nodulare a contorni irregolari, dendritici con area di ground-glass( da linfangite carcinomatosa):nodulo maligno sino a dimostrazione contraria (3)
The right upper lobar nodule has definitely irregular spiculated outline and surrounded by GG opacity(Halo sign)The size looks around 10-15 mm diameter (50% possibility )of malignancy.
Advice previous films if present or follow up within 1 and 3 months if there is increase in diameter by 0,26 % (doubling time for the volume )after 1 month it is likely infection (?fungal as invasive aspergillosis )/or TB) after 3 month it is most likely malignant and should be biopsied.
NB : PET/CT can help if no metabolic activity it is benign..if there is activity it can be either infection or malignat.
I think in this case the first step should be a comparison to previous films to determine if the nodule is new or old. If the nodule is old, it’s important to determine if the nodule is getting larger. If getting larger, this could be suggestive of a malignancy depending on how much time has passed between the two radiographs. Therefore, if the question is “what is the best next step?” I would answer #4 – need previous films. Subsequently, CT shows an irregular spiculated mass in the periphery of the right lung without cavitation or internal calcifications. This could be suggestive of adenocarcinoma. However, there is no way to be 100% sure without biopsy, therefore, answer #3 – indeterminate – would be the best answer.
Right upper zone opacity with irregular margins and a possible satellite in right lower zone, likely malignant. Tissue diagnosis can be obtained under CT guidance. No adenopathy is appreciable on plain film/single CT slice. No effusions.
Left lung is clear.
Mi scuso per la errata numerazione: la risposta è il numero1.Nodulo probabilmente maligno sino a prova contraria
Se observa una opacidad nodular de bordes irregulares y patron dendritico sin calcificacione ni cavitacion en el lobulo superior derecho. Ademas se identifica otro nodulo mas pequeño de forma redonda en la base pulmonar derecha, sin calcificaciones. Tambien se observa atelectasia del lobulo inferior izquierdo con desplazamiento inferior del hilio izquierdo y opacidad triangular retrocardiaca. Por todos estos datos no se descarta que existan metastasis pulmonares.
Good. You looked at the whole film.
According to the ACCP Evidence-Based Clinical Practice Guidelines (2nd Edition) (http://journal.publications.chestnet.org/article.aspx?articleid=1211609),
1.In every patient with an SPN that is visible on CXR, we recommend that previous CXRs and other relevant imaging test be reviewed. Grade of recommendation, 1C.
2. In patients who have an SPN that shows clear evidence of growth on imaging tests, we recommend that tissue diagnosis be obtained unless specifically contraindicated. Grade of recommendation, 1C.
3. In a patient with an SPN that is stable on imaging tests for at least 2 years, we suggest that no additional diagnostic evaluation be performed, except for patients with pure ground-glass opacities on CT, for whom a longer duration of annual follow-up should be considered. Grade of recommendation, 2C
So,regardless of the probably malignant appearance of the nodule I choose
4. Need previous films
I think that the two nodules that project over the lung bases are symmetric, and therefore are more likely to be breast nipples.
Good discussion. Basal nodules are nipples.
Just looking at these two images: probably malignant. Quite large with spiculated margins.
We can see a peripheral nodulal opacity with spiculated margins and ground-glass infiltration with satelite centolobular nodules.We see apical caps too.
Could be a tb?… but we need to compare with previous films to exclude the malignacy (that is important).
i would like too see the profile view first.
The nodules of the lung bases i think is the breasts nipples.
(i think centrolobular is wrong):)
A HRCT is indicated to characterize the nodule and the infiltrations of the lung before biopsy.
My answer is 1 probably malignant.
In the chest x-ray shows 2 NP´s The big one in the Right Upper Lobe and the small one in Right Lower Lobe. Also shows caudal retraction of the right pulmonar hilum (atelectasis) and in the left lower lobe a trinagular opacity.
On the CT the NP has a “corona radiata” and ground glass sorrounding, malignant characteristics.
So in conclusion, in a man over de >50 years old, with 2 NP´s in the chest x´ray and with non bening morphology characteristics on the CT. My first choice is to think in probably malignant.
du fait des characteristiques radio et CT (contour, dimensions, densité – pas de cavité central -), mesieur, age, plutot malign. mais tout ca devrait etre evoquer aussi en fonction de la clinique (symptomes, durée, etat generale, antecedent perssonnel et en famille etc).
Findings: Spiculated nodule surrounding by patchy ground glass is seen in the anterior segment of RUL peripherally.
The best answer is No.4; need previous film …..why?
Because the Pt.Age is > 30 to see if there is increasing in size ==> biopsy or not ==> follow up.
If previous films are not available ==> HRCT Chest to see if there is benign/malignant calcification or fat and so.
Finally, I think this is a malignant bx the age,irregular border and peripheral location.
One thing more on PA-CXR there is Lt.Retrocardiac opacity but there is no Lat.View to rule out LLL collapse.
Most of you are offering sensible discussions about the approach to solitary pulmonary nodules. Congratulations and wait for the answer on Friday.