Dr. Pepe’s Diploma Casebook: Case 46 – SOLVED!
Dear Friends,
Today I am presenting the case of a 52-year-old man who underwent a bilateral lung transplant two years ago. He developed chest pain following bronchoscopy and endobronchial biopsy.
Examine the images below and leave your thoughts in the comments section.
What do you see?
It is significant?

52-year-old man, PA chest
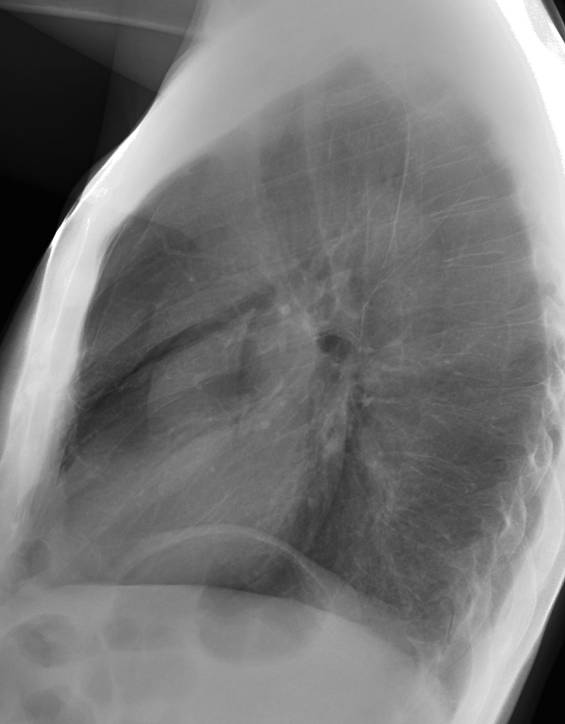
52-year-old man, lateral chest
Findings: PA radiograph shows fine bilateral paramediastinal lines outlined medially by air (A, white arrows). In the lateral view, the aortic root (B, white arrows) is well defined by air. There is bilateral pneumothorax (A,B, red arrows). The appearance is very typical of pneumomediastinum with concomitant pneumothorax.
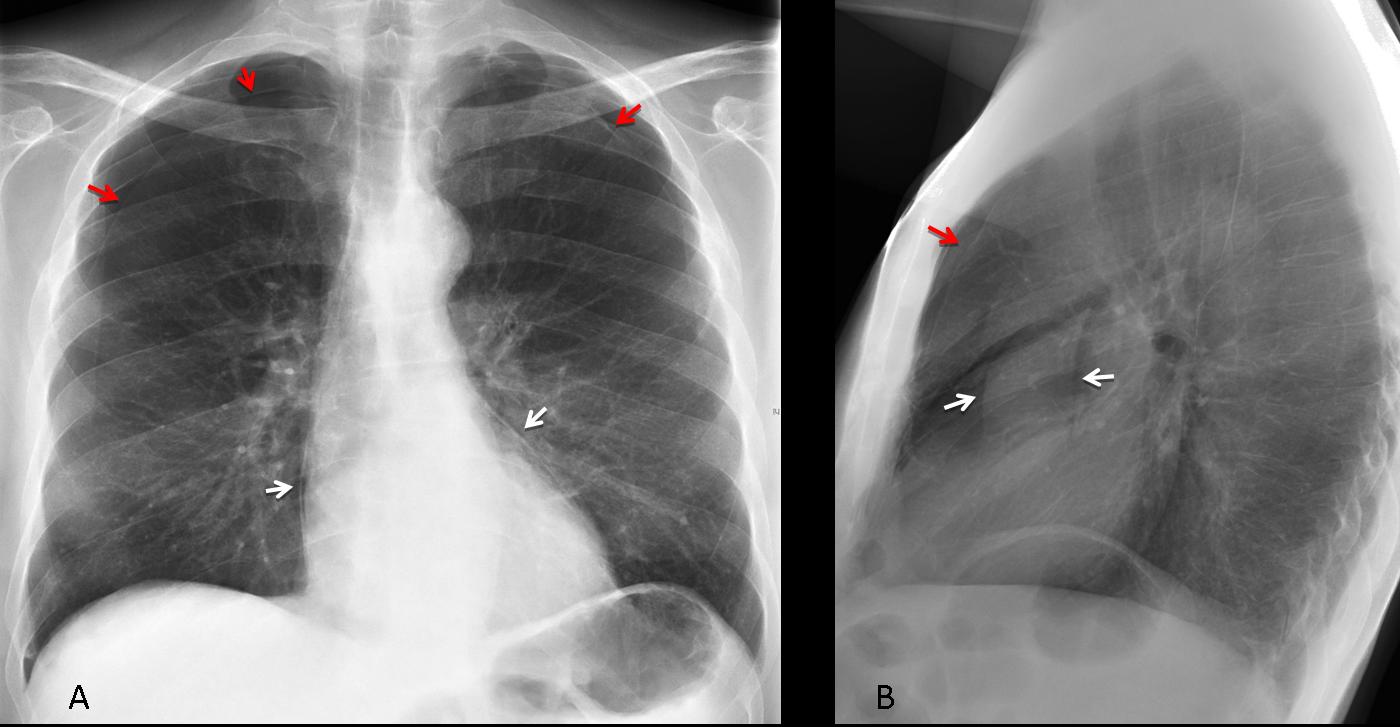
Fig. 1
Final diagnosis: pneumomediastinum and pneumothorax, secondary to endobronchial biopsy.
This case is presented to discuss mediastinal air. Pneumomediastinum has a very typical radiographic appearance, presenting as linear air streaks around the mediastinal structures, better seen in the lateral view over the anterior clear space. Air may be seen outlining the walls of the mediastinal viscera, as in the case presented. It can be accompanied by pneumothorax or subcutaneous emphysema. The imaging features of pneumomediastinum are always the same, regardless of the etiology. The amount of air can vary from scarce to massive (Fig. 2).
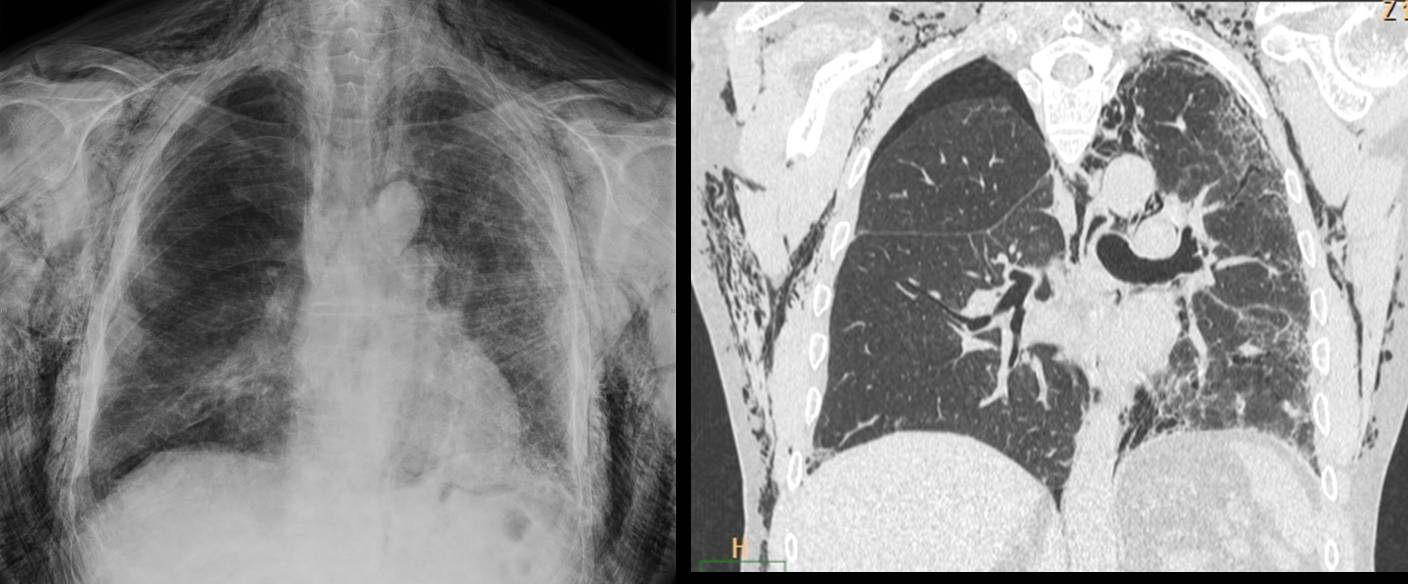
Fig. 2
Fig. 2. Massive pneumomediastinum and subcutaneous emphysema after lung transplantation. Patient recovered uneventfully.
Pneumomediastinum per se is innocuous, and the air usually disappears spontaneously in a short time. An unusual presentation form is tension pneumomediastinum, in which the extravasated air compresses the heart and sometimes causes cardiorespiratory compromise. I have never seen a case of this type.
A simple approach classifies pneumomediastinum as spontaneous or secondary to trauma or instrumentation.
Spontaneous pneumomediastinum occurs when alveoli rupture due to increased intrathoracic pressure (cough, vomiting, mechanical ventilation) and the extravasated air migrates across the interstitial space towards the mediastinum (Fig. 3). It is a benign process, with short-term resolution. In rare cases, forceful vomiting causes esophageal tear (Boerhaave syndrome) with pneumomediastinum. This is a serious condition in which other manifestations (mediastinitis, pleural effusion) overshadow the air in the mediastinal space.
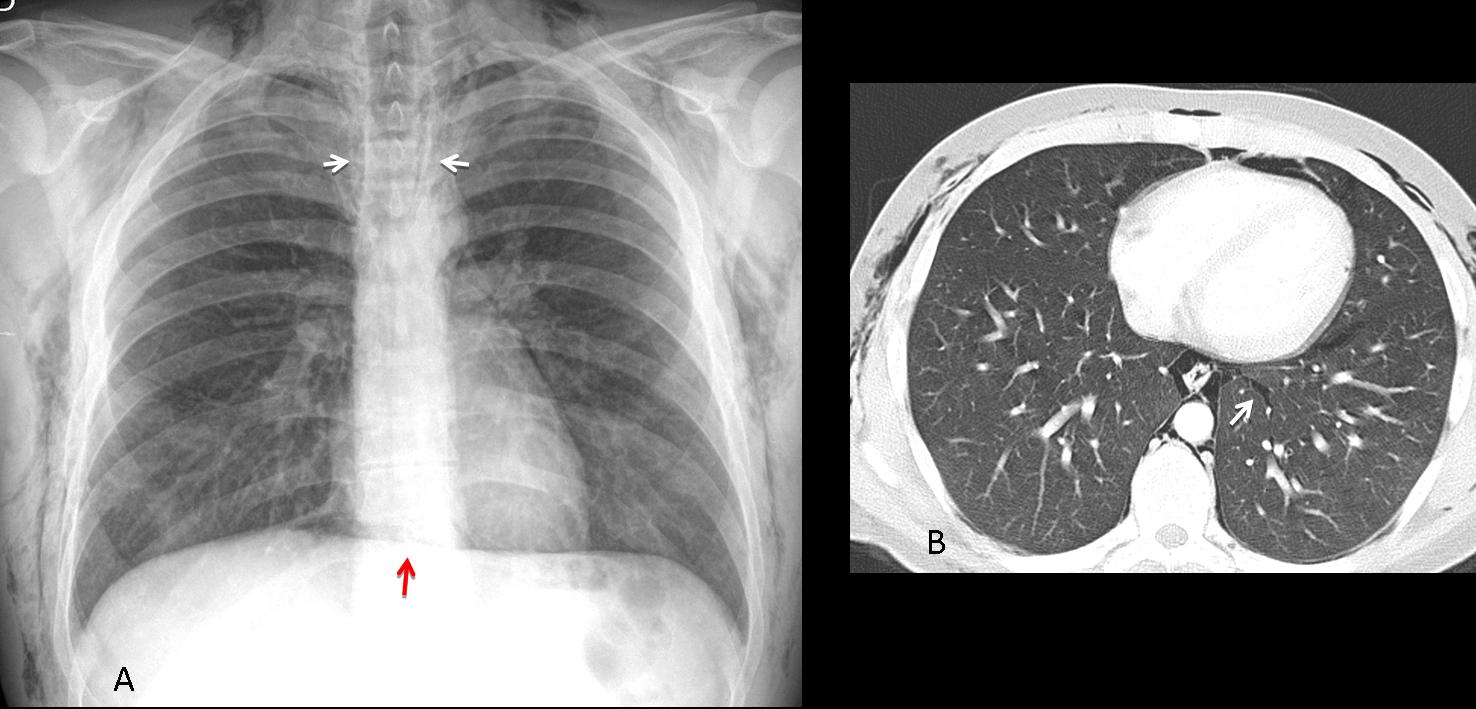
Fig. 3
Fig. 3 (above): 40-year-old cocaine-addicted man with chest pain. Cocaine snorting is a well recognised cause of pneumomediastinum. PA chest film shows air in the mediastinum and soft tissues of the chest (A, white arrows). Note the continuous diaphragm sign (A, red arrow). Axial CT depicts the extravasated air as well as air in the interstitium , migrating towards the mediastinum (B, arrow).
(Case courtesy of Eva Castañer, MD)
One of the most common causes of pneumomediastinum in young people is acute asthma leading to increased alveolar pressure against a closed glottis, with subsequent air extravasation (Fig. 4).
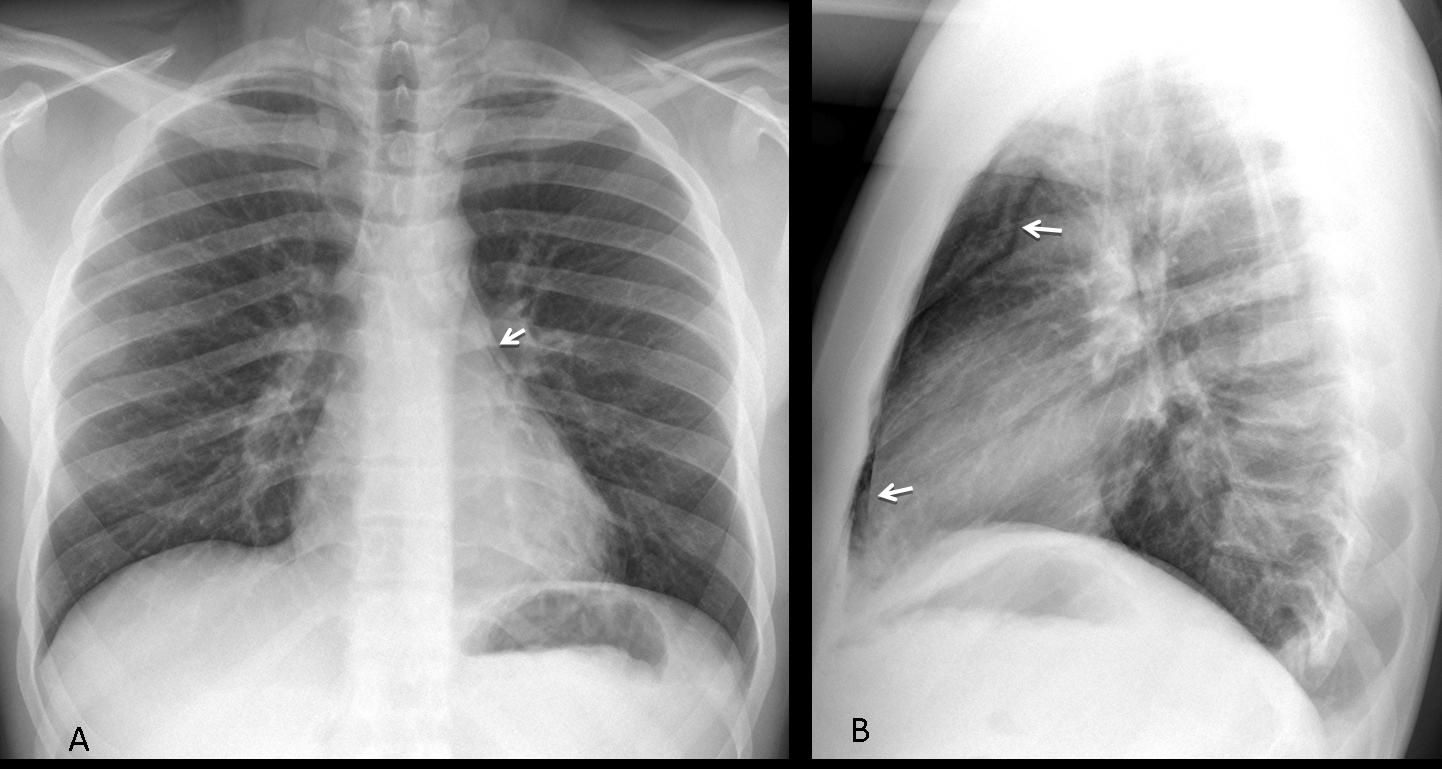
Fig. 4
Fig. 4 (above): 20-year-old patient with asthma. In the PA view, air is barely visible (A, arrow), whereas it is more evident in the retrosternal space in the lateral view (B, arrow).
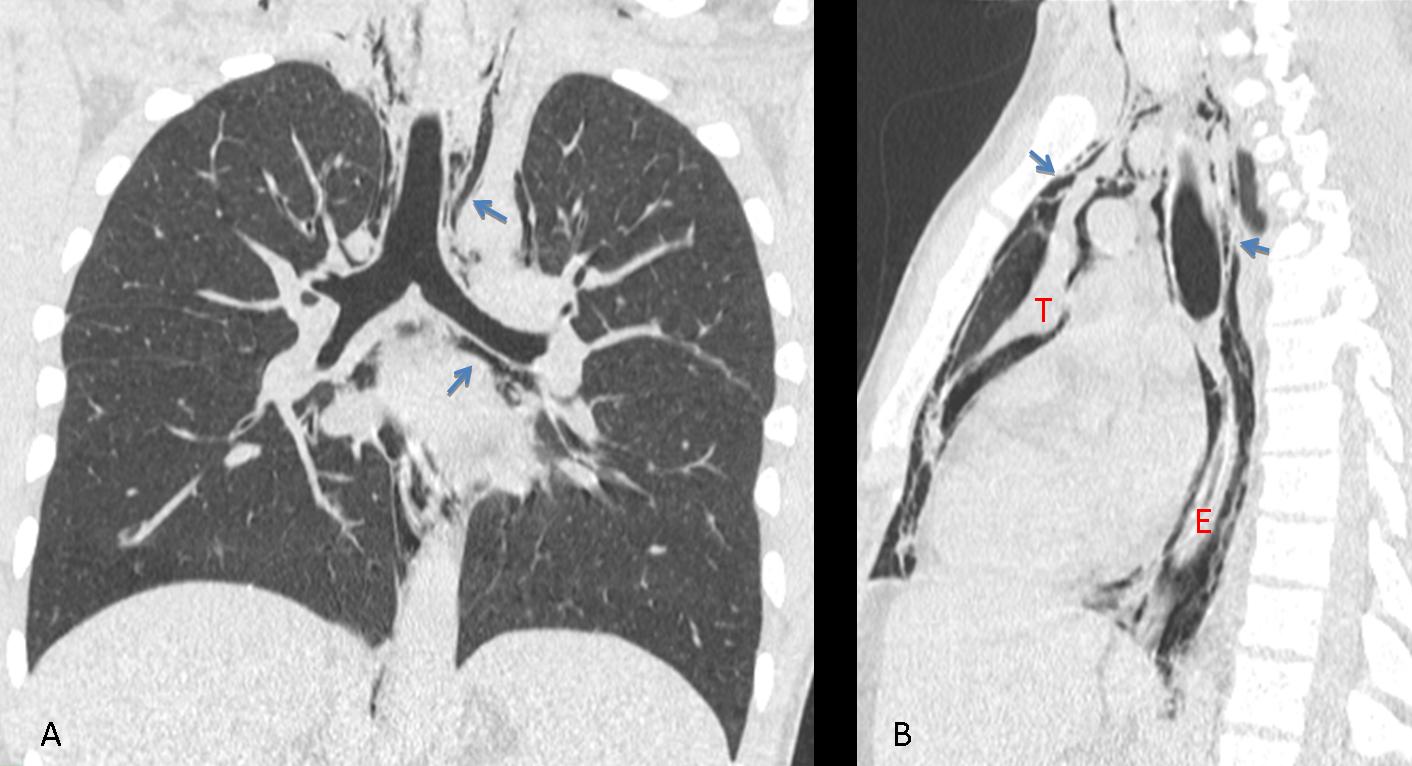
Fig. 5
Fig. 5 (above): same patient. CT confirms the mediastinal air (A,B, arrows). Note the air outlining the thymus (T) and the esophagus (E) in the sagittal reconstruction (B).
Secondary pneumomediastinum results from laceration of air-containing viscera (tracheobronchial tree, esophagus) due to trauma or instrumentation (Fig. 6). In blunt or open trauma, pneumomediastinum may underlie a serious process (e.g. fractured bronchus) and should be properly investigated.
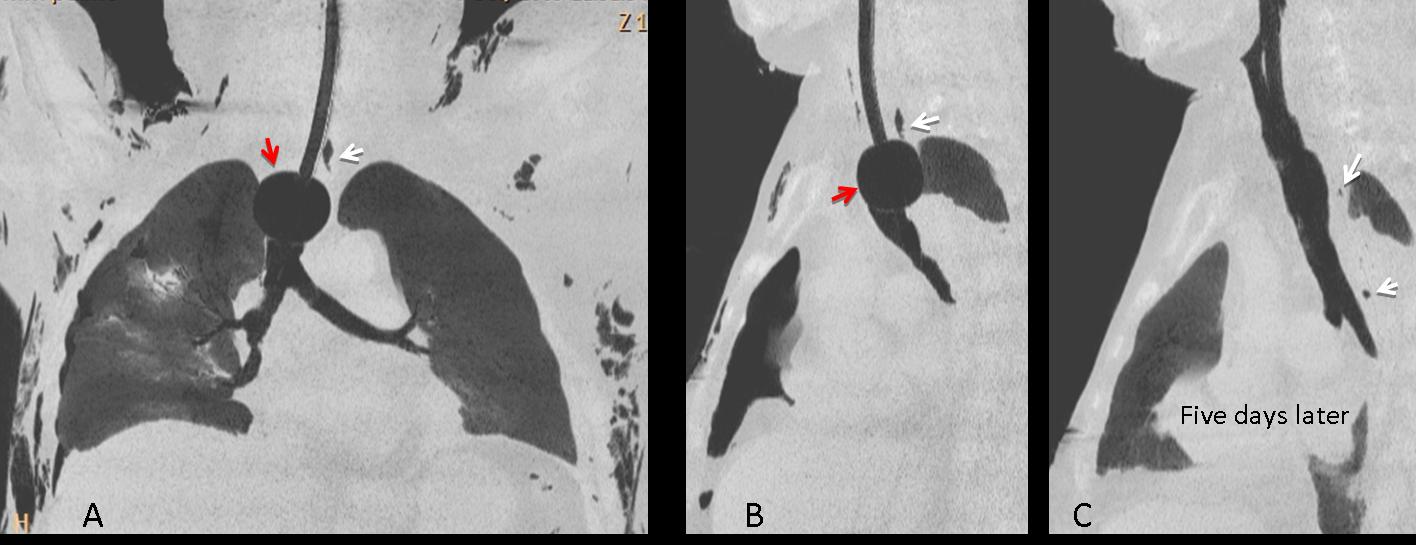
Fig. 6
Fig 6. Secondary pnumomediastinum caused by tracheal tear after overinflation of the balloon (A,B, red arrows). Initial films show linear air in mediastinum (A,B, white arrows), as well as subcutaneous emphysema. Five days after removal of the balloon, air has practically disappeared (C, arrows).
Secondary pneumomediastinum may also originate outside the chest when air migrates from neighboring areas, such as the soft tissues of the neck (Fig. 7) or the retroperitoneal space.

Fig. 7
Fig. 7 (above): 27-year-old male stabbed in the neck, injuring the upper trachea. Extravasated air has collected mainly in the soft tissues of the neck, and some has travelled downward into the mediastinum. Chest radiograph one week later shows that air has reabsorbed.
Time for a test. Radiographs of a 52-year-old man, asymptomatic.
Do you see any abnormality?
It is significant?

Fig. 8
Findings: PA view shows an air-fluid level in the upper mediastinum (A, arrow), located behind the trachea in the lateral view (B, arrow). The location is consistent with dilated oesophagus or diverticulum. Considering that the patient is asymptomatic, the second possibility is more likely.
Final diagnosis: Zenker’s diverticulum.
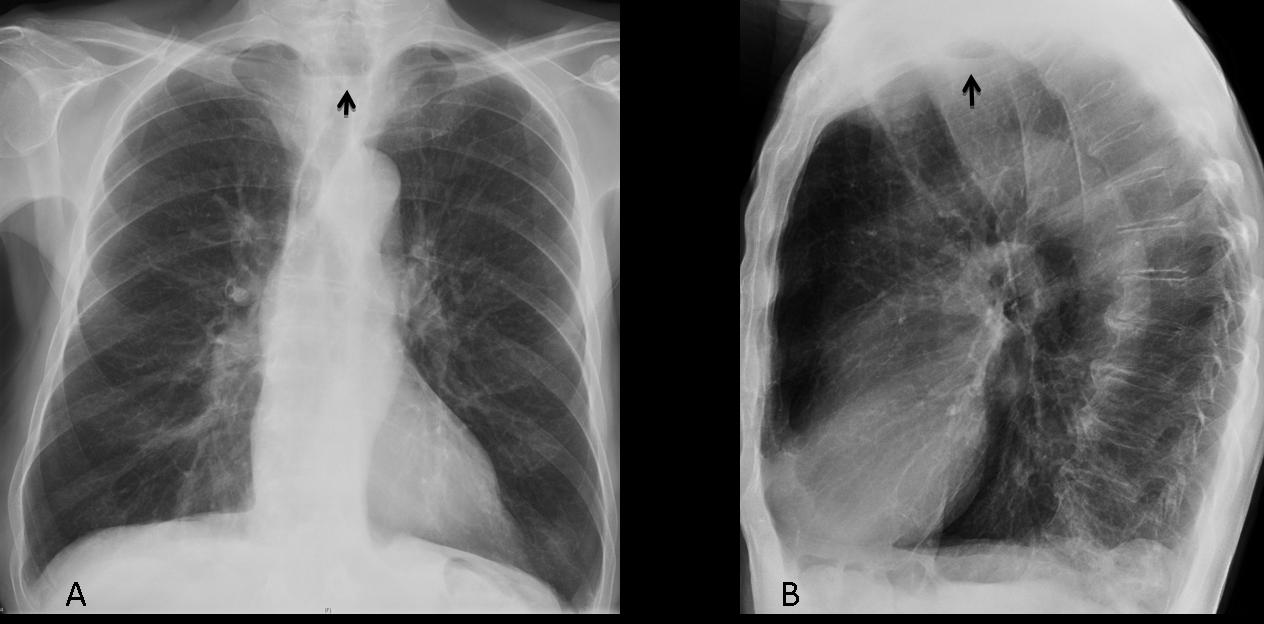
Fig. 9
This case is shown to point out that air-fluid level is another presentation form of mediastinal air. It requires a closed space where fluid and air can collect. This requisite is met by diverticula, as in the present case, obstructed oesophagus (Figs. 8, 9), and hiatus hernia (Fig. 12). Air-fluid level is unusual in mediastinal abscess because the air is mixed with inflammatory exudate, giving the abscess a bubbly appearance.
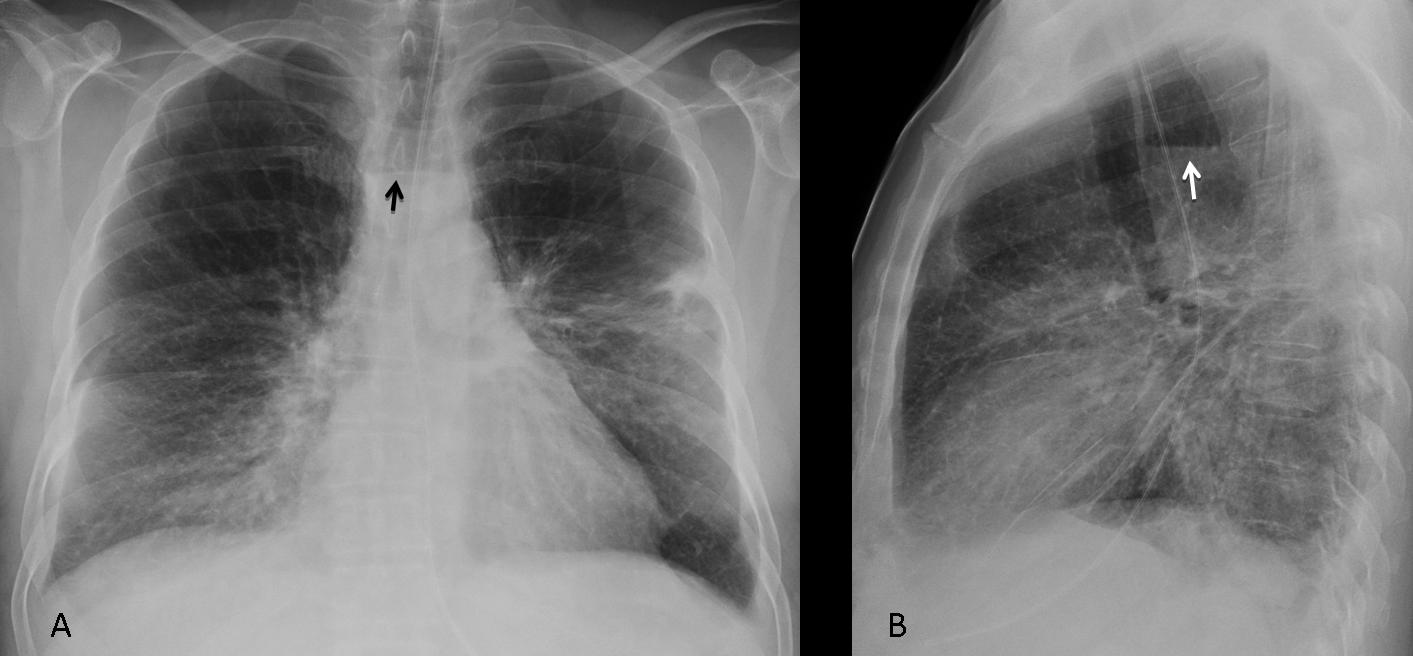
Fig. 10
Fig. 10 (above): 52-year-old man with upper oesophageal dilatation and air-fluid level (A,B, arrows), secondary to carcinoma of middle third of oesophagus.
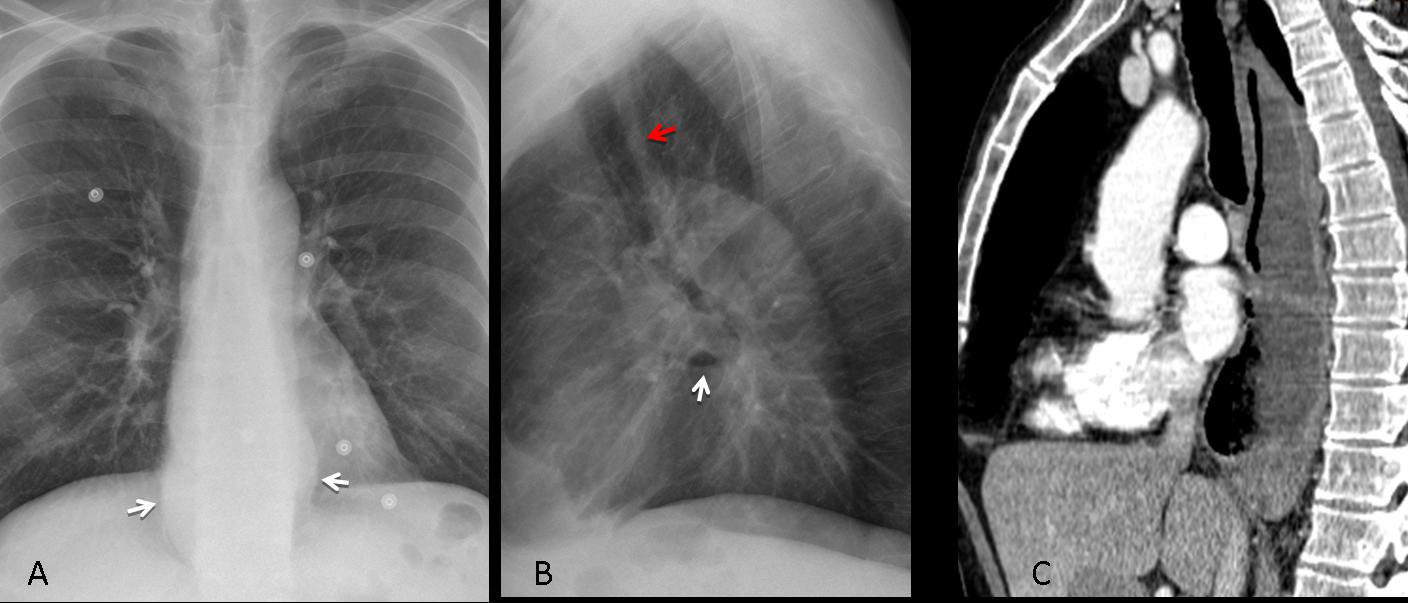
Fig. 11
Fig. 11 (above): 47-year-old man with dysphagia. PA radiograph shows a dilated lower oesophagus (A, arrows). In the lateral view, an air-fluid level is seen in mid-oesophagus and there is thickening of the retrosternal stripe (B; red arrow). CT confirms the dilated oesophagus, containing air and fluid (C). Diagnosis: oesophageal achalasia.

Fig. 12
Fig. 12 (above): 76-year-old man with a large and obvious hiatus hernia. It is important to mention that hiatus hernia is by far the most common cause of air-fluid level in the lower mediastinum in elderly people, as in this case.
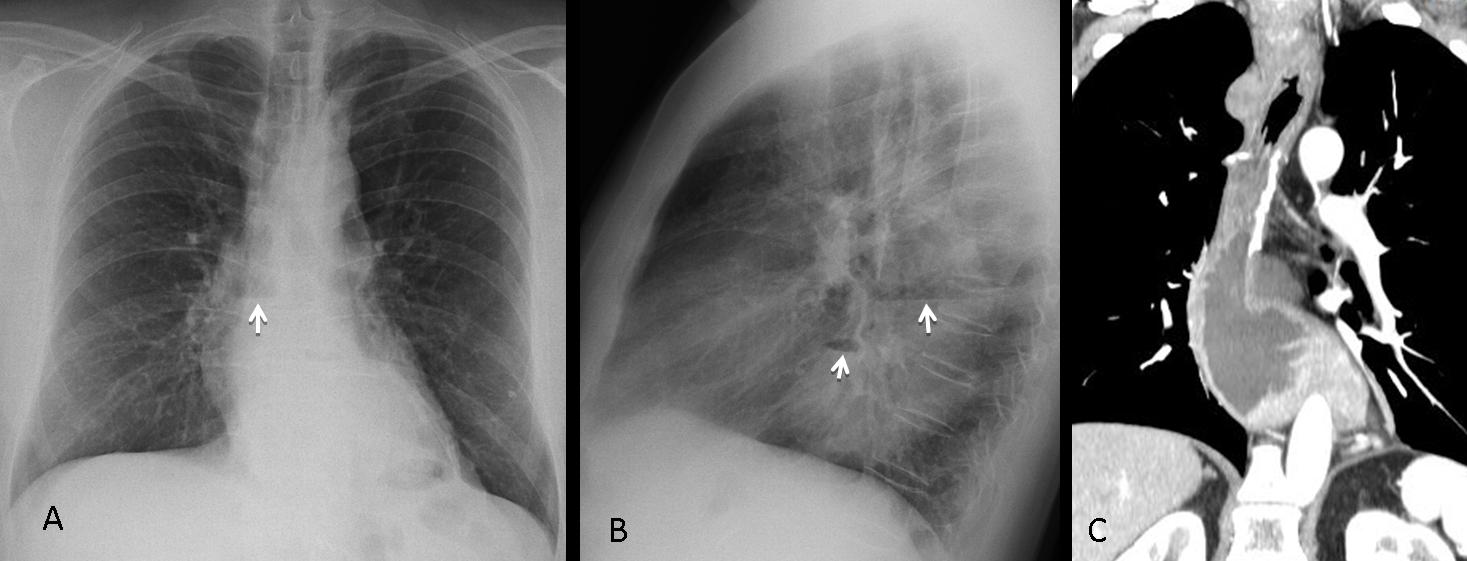
Fig. 13
Last, but not least, do not forget to investigate previous oesophageal surgery as a cause of mediastinal air-fluid levels (Fig. 13 A,B arrows). Patient had resection of lower oesophagus and stomach pulled up (C), giving the air fluid levels apparent on chest radiography.
For the sake of completeness, I am including a case of pneumopericardium presenting with an air-fluid level. These are very uncommon and usually post-surgical.
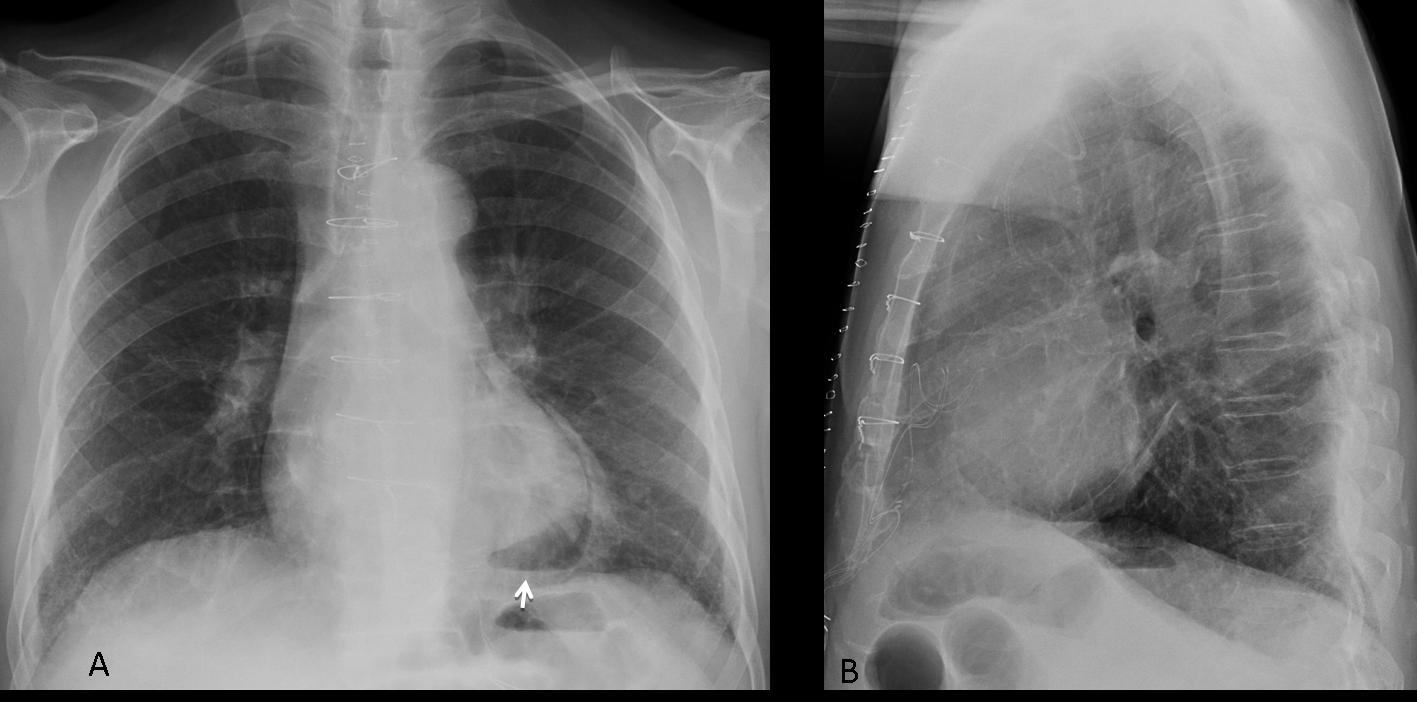
Fig. 14
Fig. 14 (above): 47-year-old male with pneumopericardium and air-fluid level after cardiac surgery (A, arrow).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- Pneumomediastinum appears as streaks of air, accompanied or not by pneumothorax and/or subcutaneous emphysema
- Spontaneous pneumomediastinum is secondary to rupture of distal alveolar sacs, with the air migrating across the lung interstitium
- Secondary pneumomediastinum is mainly caused by medical procedures or external trauma
- Mediastinal air-fluid levels point to an obstructed esophagus, hiatus hernia, or diverticula


Bilateral pneumothorax, suspecious also for a small pneumopericardium. Not yet significant.
Bilateral pneumothorax
Bilateral pneumothorax with pneumomediastinu
Bilateral pneumothoracies, and pneumopericardium.
1.pneumothorax, pneumopericardium.
2.i dont like the inner contour of the main bronchus, because they are irregular (stenosis?granulation tissue?).
3.thickening of the interstitium.
Bilateral pneumothorax and pneumopericardium. Significant in right hemithorax
bilateral pneumothorax more severe on the right side
bilateral pneumothorax more severe on the right side.
Needs CT to look for bronchial dehiscence
bilateral pneumothorax,pneumopericardium. and I notice few cystic
spaces in inner region of right middle field ? bullae.
Bilateral pneumothorax
Pneumomediastinum
corpus alienum ?
Bilateral yatrogenic pneumothorax and pneumopericardium (because the lucent band terminates at the hilar level), suggest a penetrating injury of trachea/barotrauma/broncial tree(?). It could be solved placing a drainaje tube.
Indirect signs of bronchial dehiscence include the presence of a new or persistent air leak, pneumothorax, and pneumomediastinum
Indirect signs of bronchial dehiscence include the presence of a new or persistent air leak, pneumothorax, and pneumomediastinum (in the early postoperative period..(
Pneumothorax may also occur after
transbronchial biopsy
Bilateral-lung and heart–lung transplantations frequently result in a single communicating pleural space. Therefore, fluid and gas collections are often bilateral.
Is necessary a prior study.
Pneumothorax bilateral and pneumomediastinum.
Pneumothorax and pneumocardium seems too easy. There must be something more. One can’t be satisfied by the first finding. We can’t forget important clinical data: can we see the cause of performing bronchoscopy and biopsy?
Sometimes, cases are easy. WYSIWYG (What you see is what you get)
Bilateral pneumothorax and pneumomediastinum
Bilateral pneumothorax, pneumomediastinum
pneumopericardium & pneumopericardium
Bilateral pneumothorax and pneumomediastinum,……But I think that there is another thing as your cases are not easy from the first impression…..:)
Cases from Dr. Pepe are reasonably easy. They aim to prepare for the Diploma examination. Cases in Caceres’ corner are harder. Muppet is pitiless!
😉
…scusa per il ritardo:ero a Congresso.Tante risposte significa che in tanti ti seguono ! Si vede chiaramente un pn.torace, bilaterale ed un pnpericardio…..ma gli esami precedenti, per confronto, cosa hanno evidenziato? Il trapianto, bilaterale, di polmone porta inevitabilmente a pn.torace, post-operatorio.Perchè non è stato fatto anche un rx in pronda espirazione?
Since the pneumothorax was obvious, expiratory films were not considered. I believe that the appearance is typical of pneumomediastinum; pneumopericardium is much more unusual and does not follow endoscopic biopsy.
I like to know what is the reason of the lung heart operation.
LAM?Sarcoidosis?
could be a recurence of a prior pathology.
If pneumopericardium is not follow endoscopic biopsy…
i think we have two options.
-bronchial dehiscence (but that is in the early postoperative period)
-Bronchomediastinal fistlas is rare complication of the lung-heart transplantation.
You are assuming that the patient have pneumomericardium.
Better think of oneumomediastinum, a common occurence after endoscopic biopsy. Follow the KISS method.
Obviously the patient has an bilateral pneumothorax, pneumomediastinum and pneumopericardium. The mainbronchus on the left side seems tho be constricted, so they did the bronchoscopie for dilatation by a ballon and caused a iatrogenic Pneu. Obstructive airway complications (OACs) effect 5-25% after LTX.
My information is that no balloon dilatation was performed. Will check the chart and get back to you. Personally, I don’t see any sign that suggests pneumopericardium, which is very rae in my experience.
Sorry, its the right bronchus constricted!
Checked the clinical history and at bronchoscopy there was a 30% stenosis of intermediate bronchus and 50% of middle lobe bronchus. No dilatation was performed. Biopsy was made because bronchiolitis obliterans was suspected.
Air dissapeared on March 30 2011, fifteen days after the biopsy was performed.
pneumomediastino