Dr. Pepe’s Diploma Casebook: Case 51 – SOLVED!

Dear Friends,
I am back with radiographs of a 63-year-old woman with malaise and low-grade fever. Check the images below and leave me your thoughts and diagnosis in the comments section. Come back on Friday for the answer.
Diagnosis:
1. Carcinoma of the lung
2. Pneumonia
3. Thymoma
4. None of the above


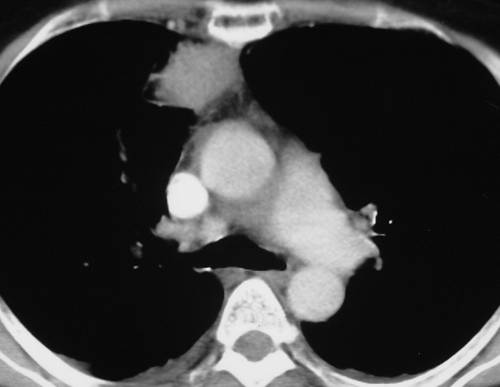
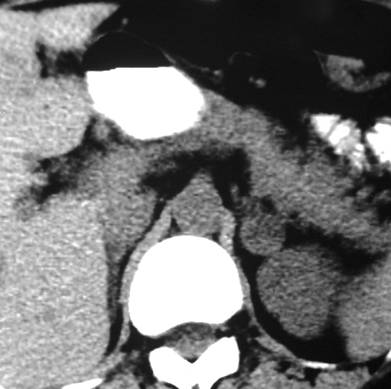
Findings: the PA view of chest is unremarkable. The lateral view shows a nodular shadow in the anterior clear space (A, arrow). Its borders are ill-defined, both in the radiograph and the CT image (B, arrow), indicating an intrapulmonary lesion and excluding thymoma. There is a non-enhancing 2cm nodule in the left adrenal gland (C, arrow).
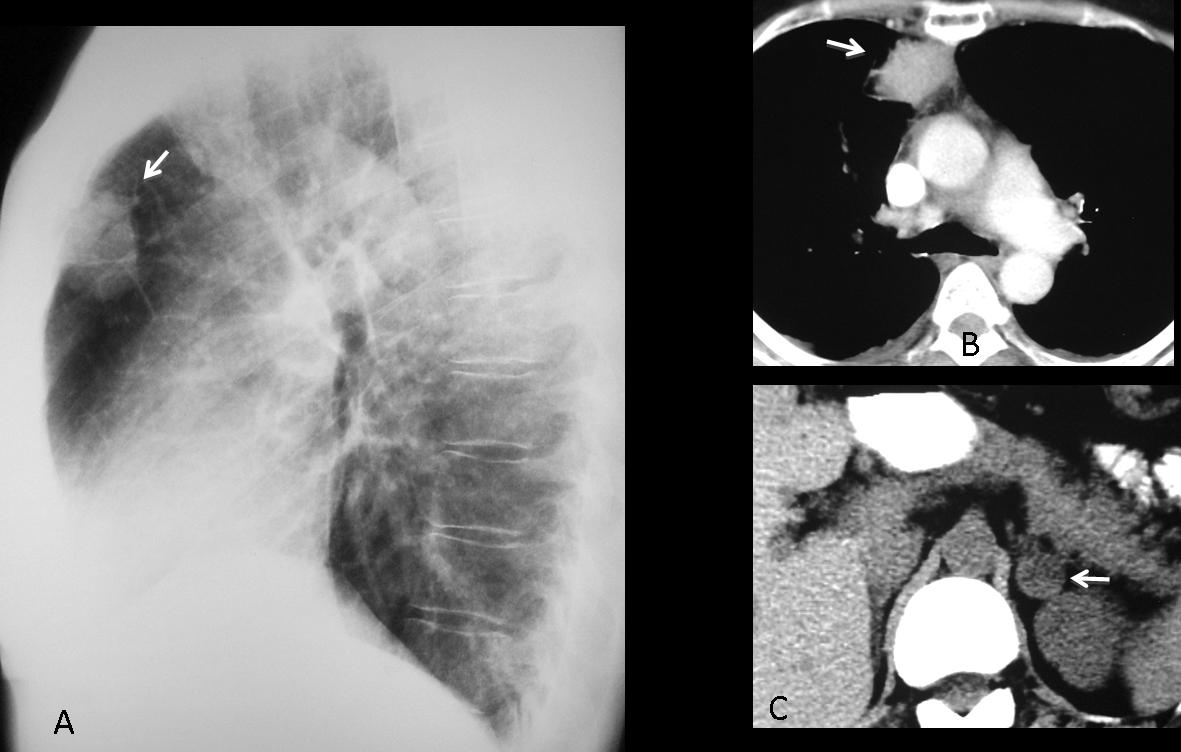
Fig. 1
Because the clinical findings were consistent with acute infection, it was decided to treat the patient with antibiotics. Radiographs and CT taken two weeks later show that the mass had markedly decreased in size.
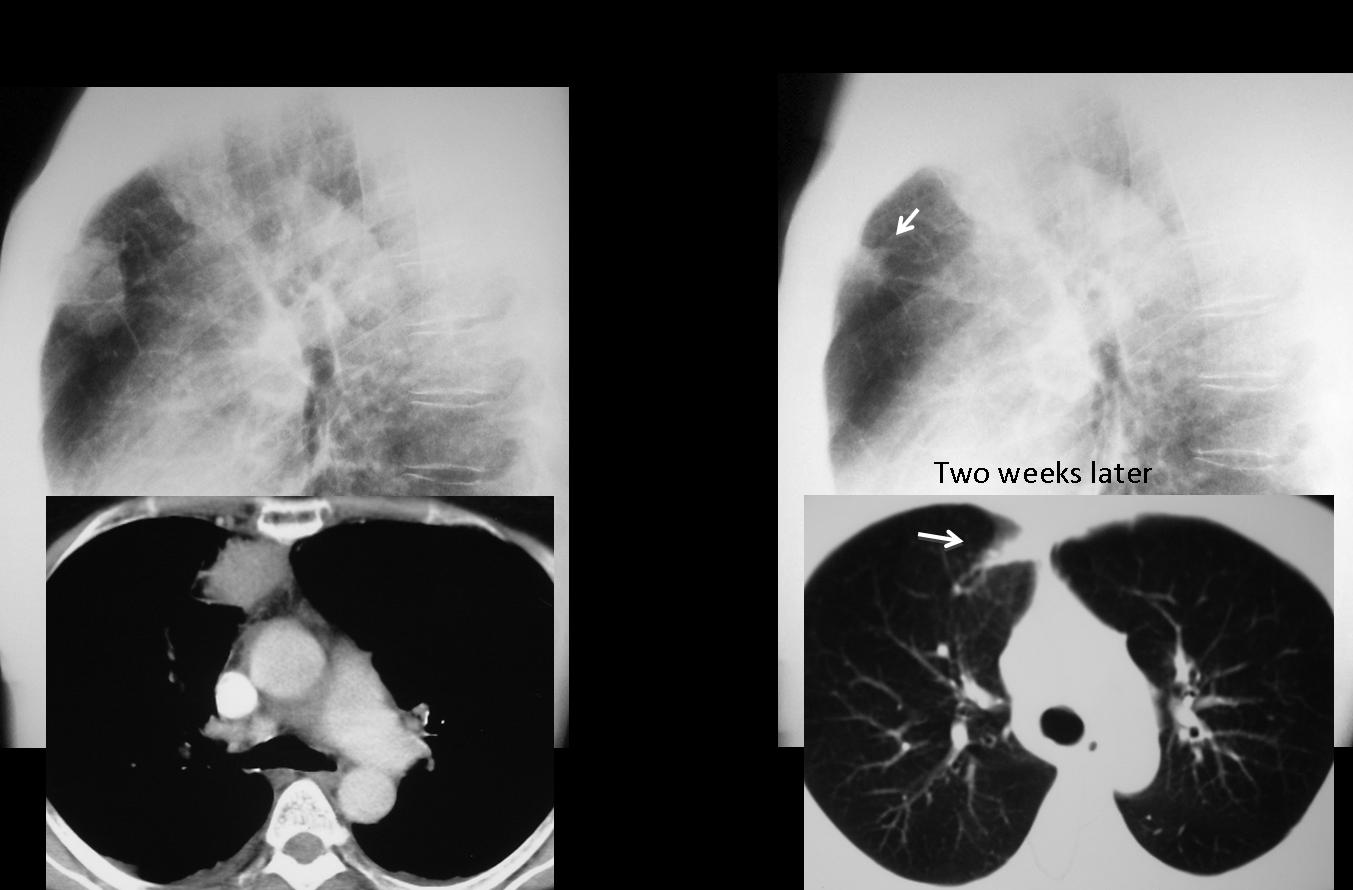
Fig. 2
Final diagnosis: Round pneumonia. Incidental adrenal adenoma
In adults, most lung nodules represent carcinomas or granulomas. In this presentation I want to discuss innocuous nodular lung lesions in which symptoms or radiography findings suggest the correct diagnosis, confirmed with CT. Some of them are transient (round pneumonia, pulmonary haematoma) and others are stable, remaining unchanged in serial studies.
The first such lesion is the so-called round pneumonia, which appears as a rounded lesion in the chest radiograph. Round pneumonias usually occur in childhood, but they are also seen in adults. They are due to incomplete development of collateral airways, limiting spread of an infection and resulting in a rounded infiltrate.
In the appropriate clinical setting (acute fever, cough), round pneumonia should be suspected when a rounded lung lesion is seen in an adult. Before CT is performed, a follow-up film should be taken to confirm or exclude this possibility (Fig. 3).
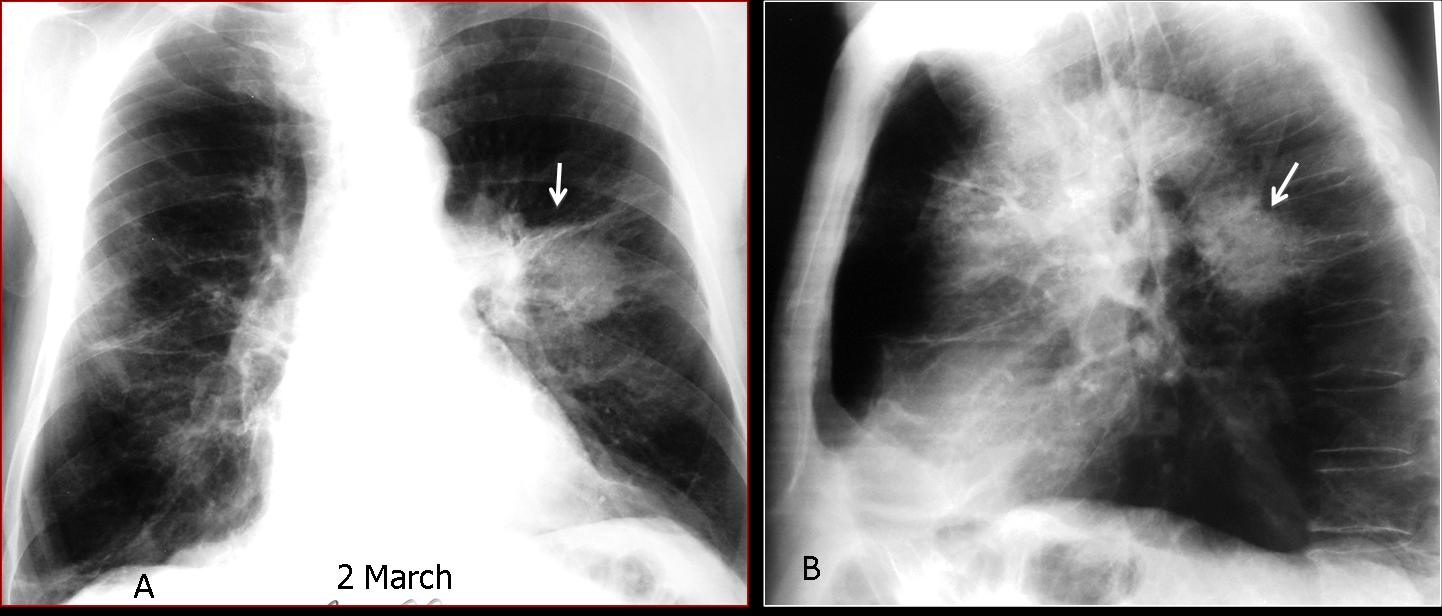
Fig. 3
Fig. 3 (above): 68-year-old smoker with cough and high fever. Chest radiographs show a round lesion in the left lung suspected to be carcinoma (A, B, arrows). Because of the fever, antibiotic treatment was started. Seven days later, the round lesion has disappeared and a linear scar remains (C, arrow). Diagnosis: round pneumonia.
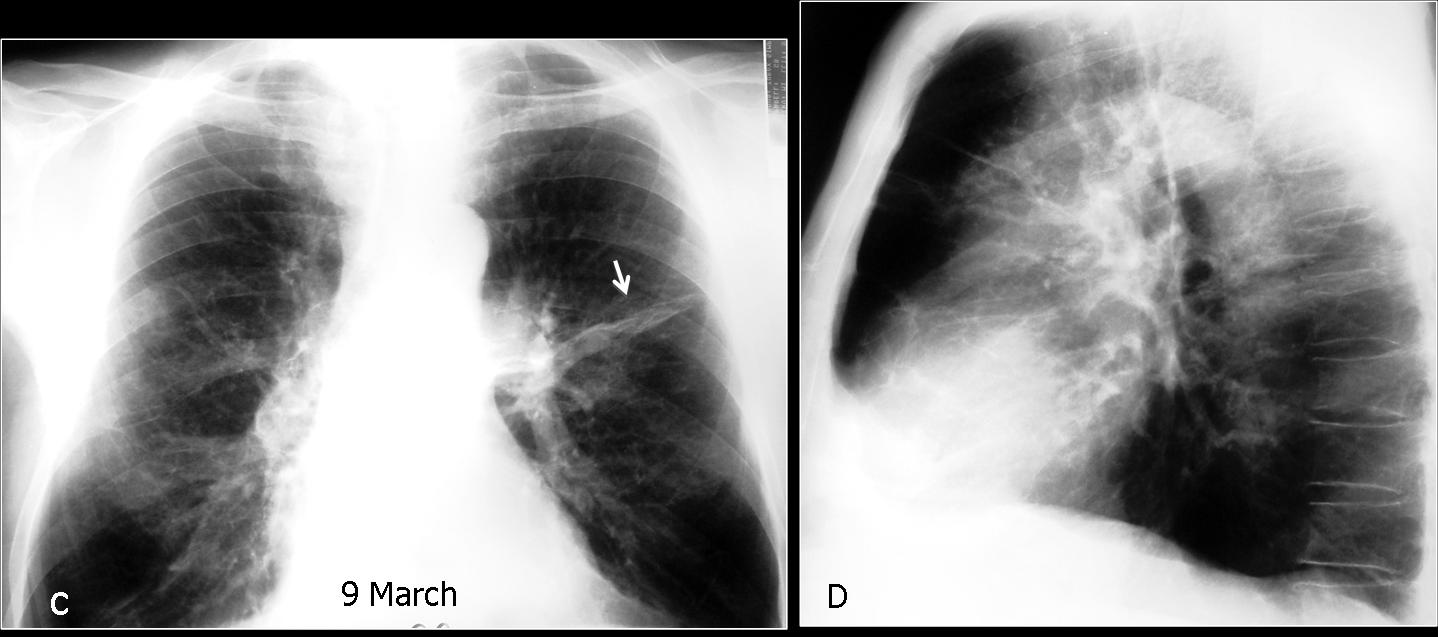
Fig. 4
Pulmonary haematoma is a transient nodular lesion secondary to localised parenchymal haemorrhage due to a traumatic injury or coagulation disorder. In the first scenario, blunt trauma causes a laceration in the lung parenchyma that fills with blood. Spontaneous haematomas are usually related to anticoagulation therapy. In both cases they present as a relatively high attenuation nodule on CT that decreases in size over time. The clue to suspecting the diagnosis is the background of trauma or the blood dyscrasia. When haematoma is suspected, follow-up films confirm progressive shrinkage of the nodule and its eventual disappearance (Figs. 5, 6 and 7).
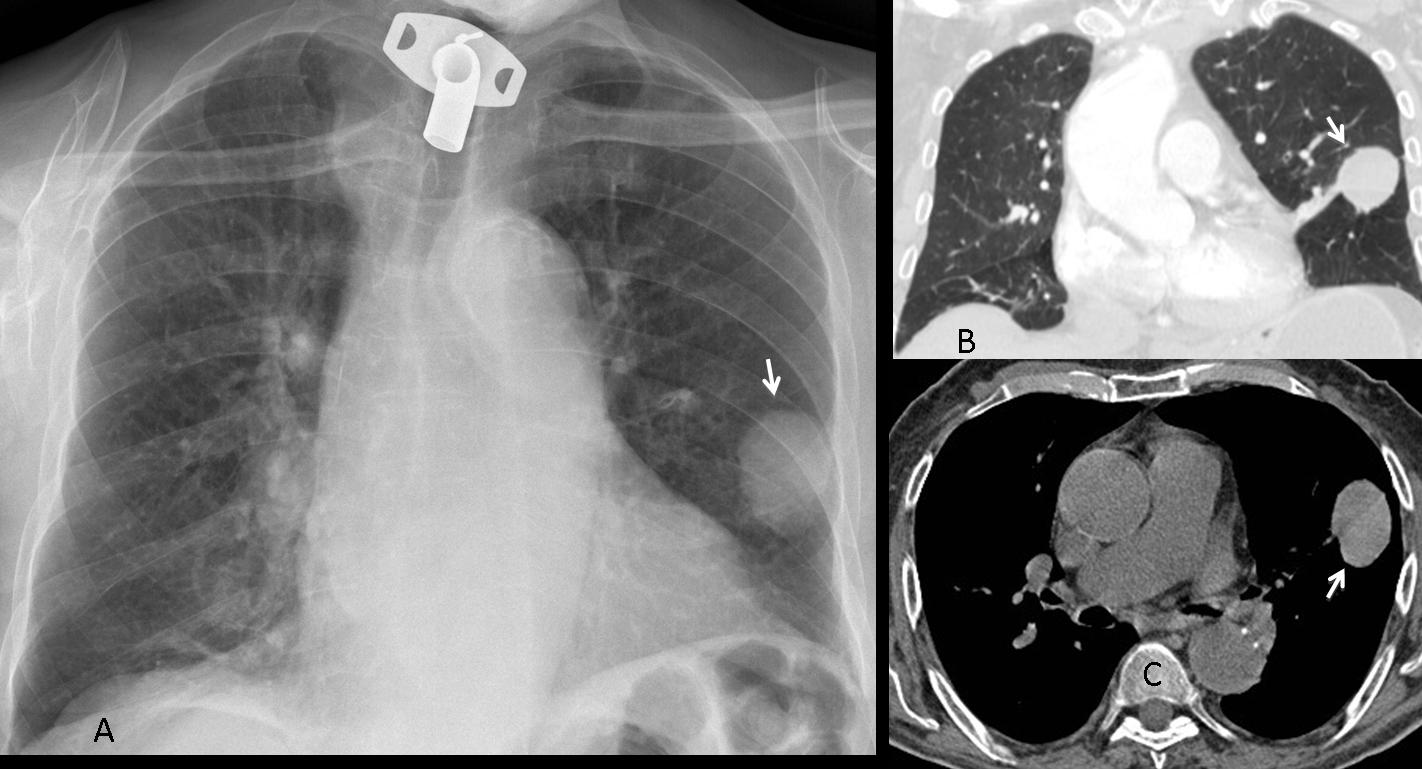
Fig. 5
Fig. 5a (above): 75-year-old man with acute pulmonary embolism treated with anticoagulants. During his stay at the hospital, a round nodule appeared in the left lung (A,B arrows), showing high density in the CT study (C, arrow). It was interpreted as a spontaneous haematoma related to the treatment. The nodule progressively decreased in size and disappeared three months later, leaving a linear scar (Fig. 6 A,B, arrows).
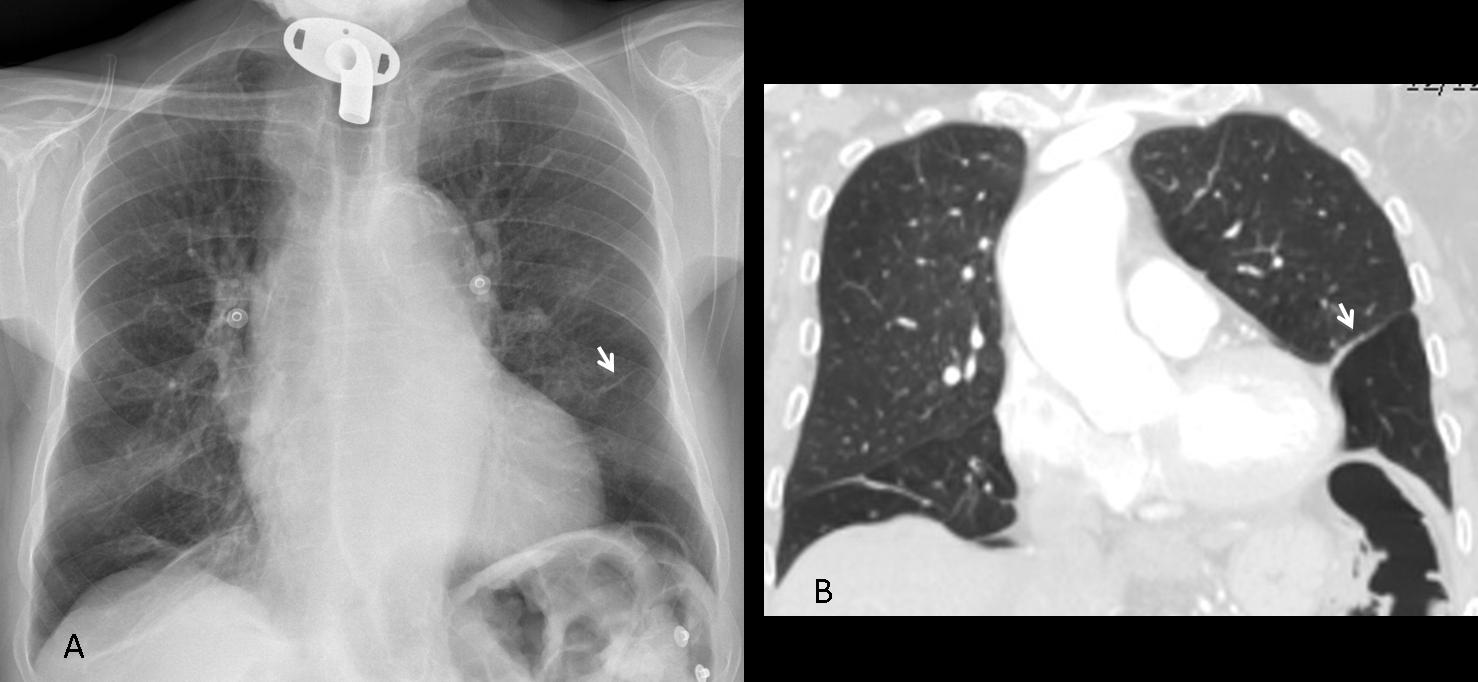
Fig. 6
Fig. 7 (below): 27-year-old man following a motorcycle accident. CT shows several pulmonary haematomas (A,B, white arrows), surrounded by areas of pulmonary contusion (B, red arrows). One month later, the RLL hematoma has disappeared, and the others have decreased markedly in size (C,D, arrows).
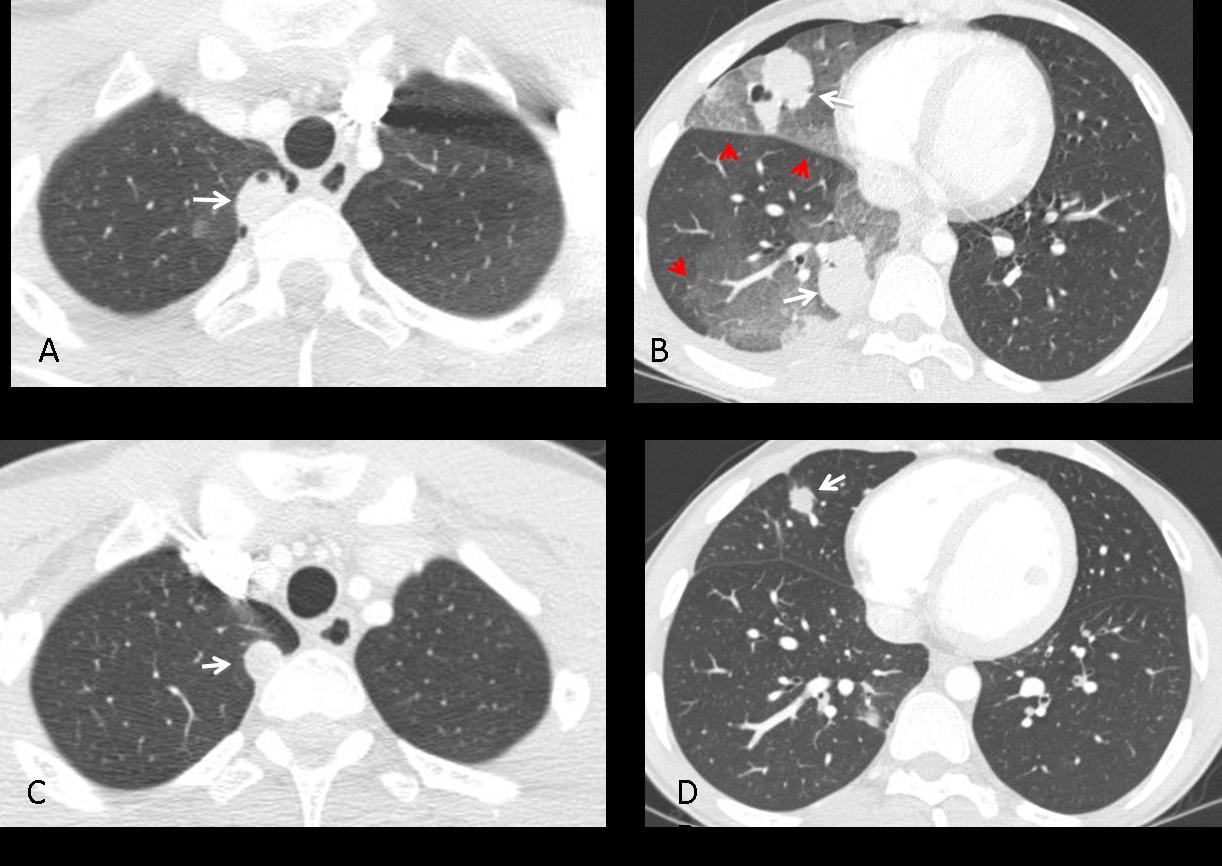
Fig. 7
Rounded atelectasis is not an uncommon cause of a stable nodular lesion. It occurs secondary to spiral folding of the lung parenchyma when fixed by thickened pleura. The consequence is a peripheral rounded opacity which should not be confused with a true nodule. It is usually asymptomatic and associated with asbestos-related disease. The imaging appearance of rounded atelectasis is very characteristic. The typical features include:
1. Peripheral lung nodule
2. Pleural thickening
3. Loss of volume of the affected lobe
4. Curving of vessels and bronchi on CT
These features are well demonstrated in Fig. 8.
TIP: Since rounded atelectasis occurs as a consequence of pleural disease, a lack of pleural thickening should lead us away from this diagnosis and suggest other possibilities.
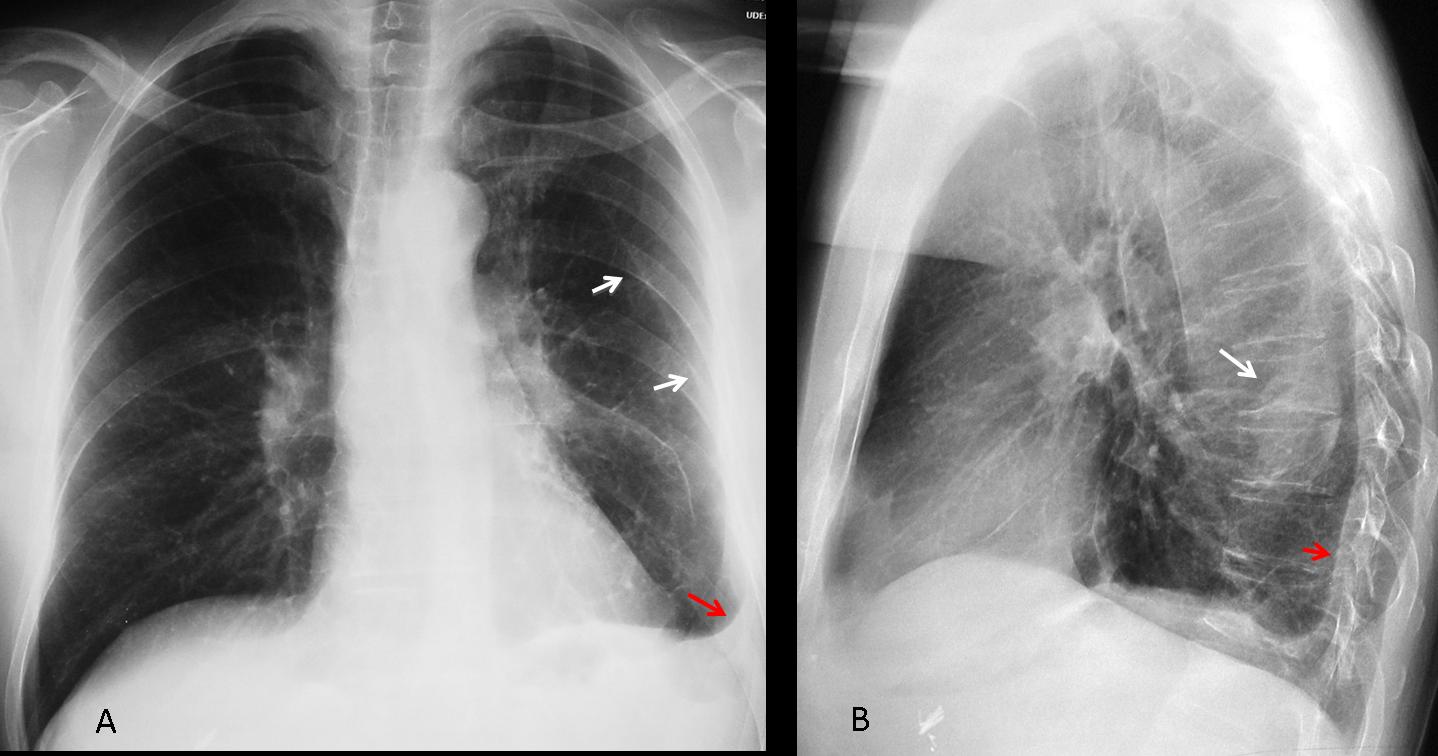
Fig. 8
Fig. 8 (above): asymptomatic 49-year-old man with rounded atelectasis. Notice the peripheral nodular component (B, white arrow), inner displacement of left major fissure indicating loss of LLL volume (A, white arrows), and the pleural disease (A, B, red arrows).
CT shows pathognomonic signs: curving of the vessels into the atelectatic nodule (Fig. 9 A,B, white arrows), which also has an air bronchogram in the proximal portion (B, blue arrows). Note the pleural thickening (A,B, red arrows).
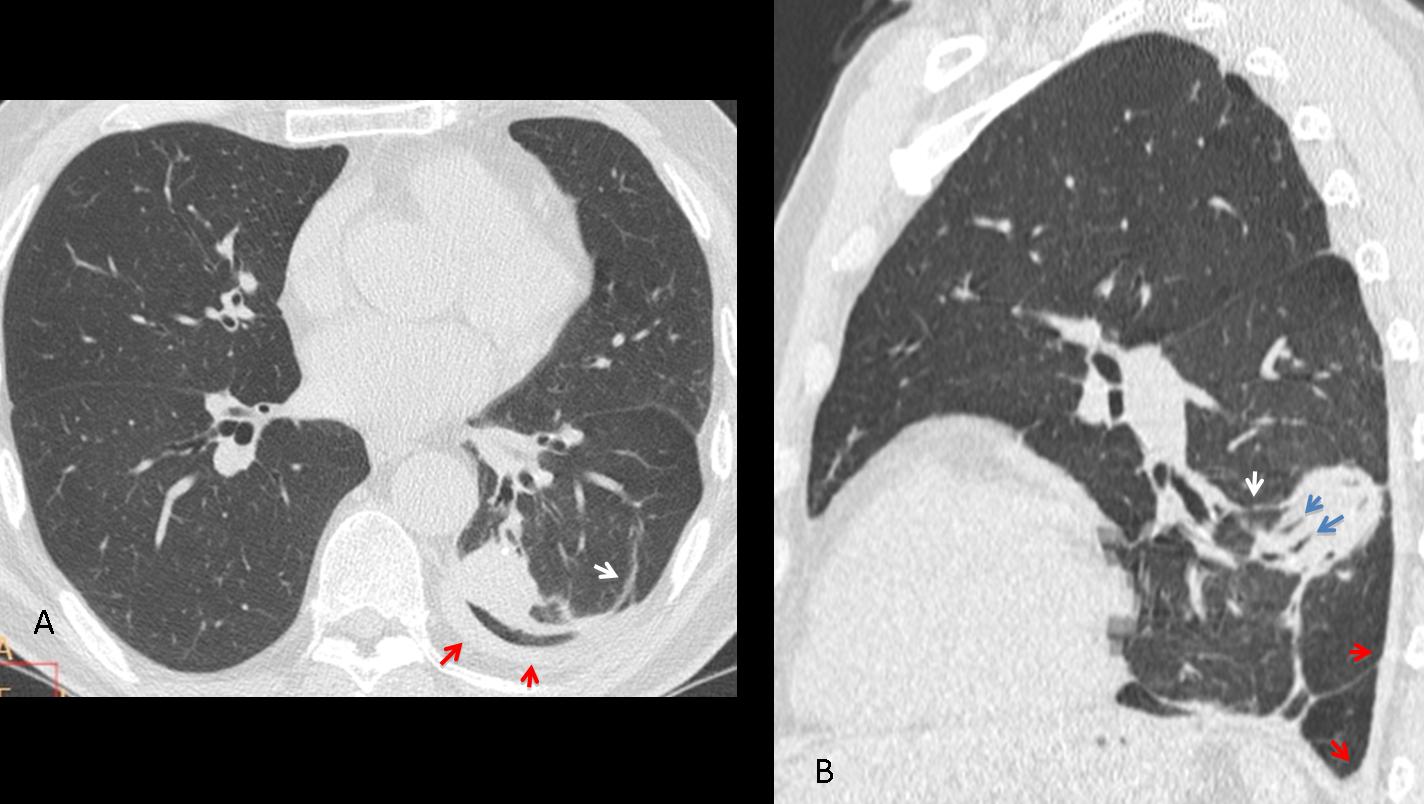
Fig. 9
At times, rounded atelectasis may be difficult to diagnose in the plain film; the typical features are discovered when performing CT to study an indeterminant nodule (Fig. 10)
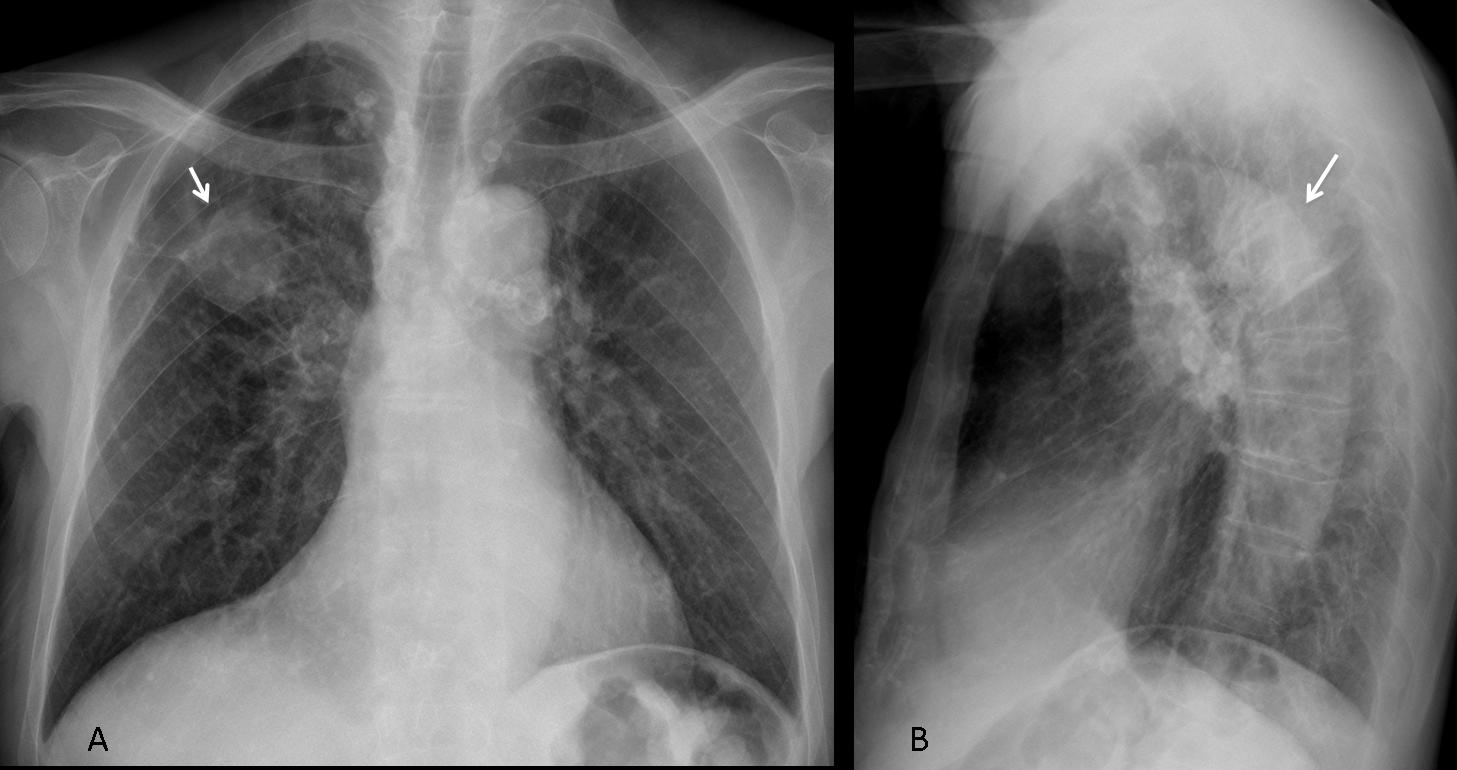
Fig. 10
Fig. 10 (above): rounded atelectasis in a 63-year-old man with an indeterminate nodule in the chest film (A, B arrows). The minor fissure is elevated, indicating RUL volume loss.
CT images show that the nodule represents rounded atelectasis. Note the peripheral localisation with associated pleural thickening (Fig. 11 A,B, red arrows), the curving vessels (A,B white arrows) and the air bronchogram in the proximal portion (B, blue arrows).
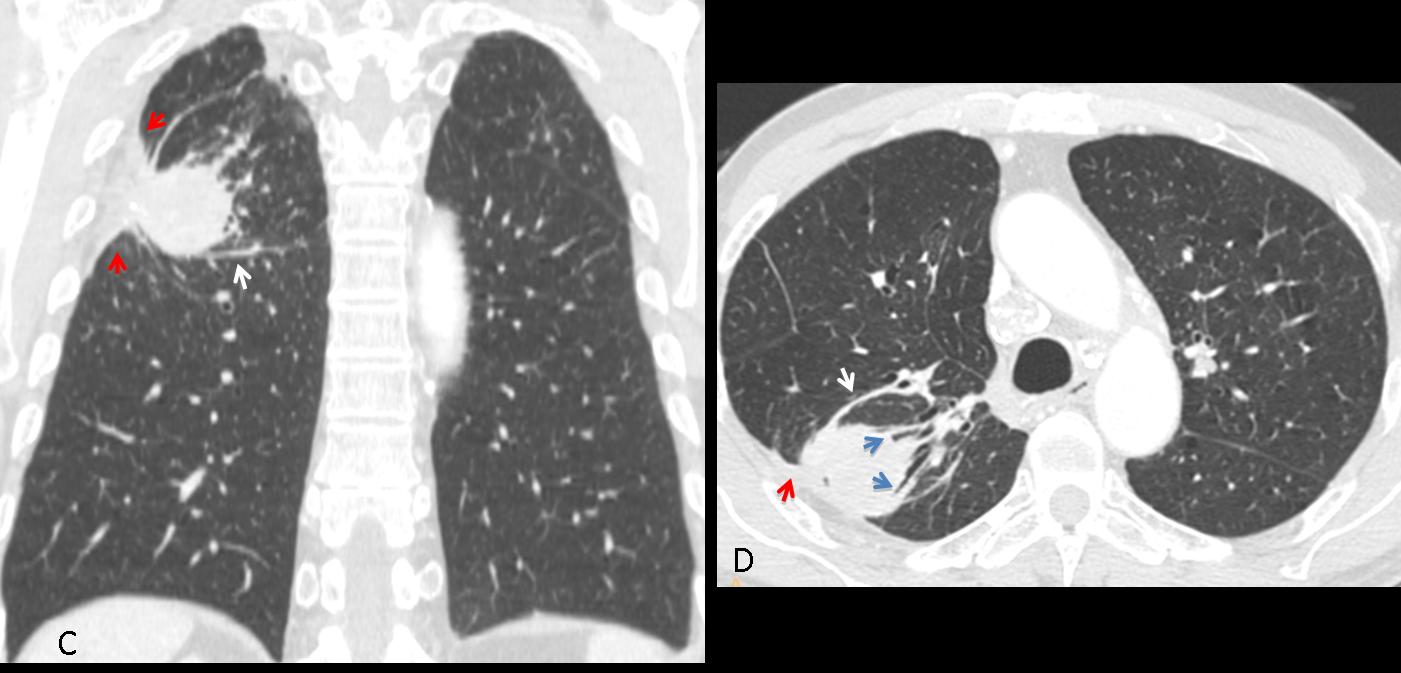
Fig. 11
Time for a test. Below is the PA radiograph of a 47-year-old asymptomatic man, in whom an RUL nodule was found. What would your diagnosis be?
1. Granuloma
2. Hamartoma
3. Mucus plug
4. None of the above
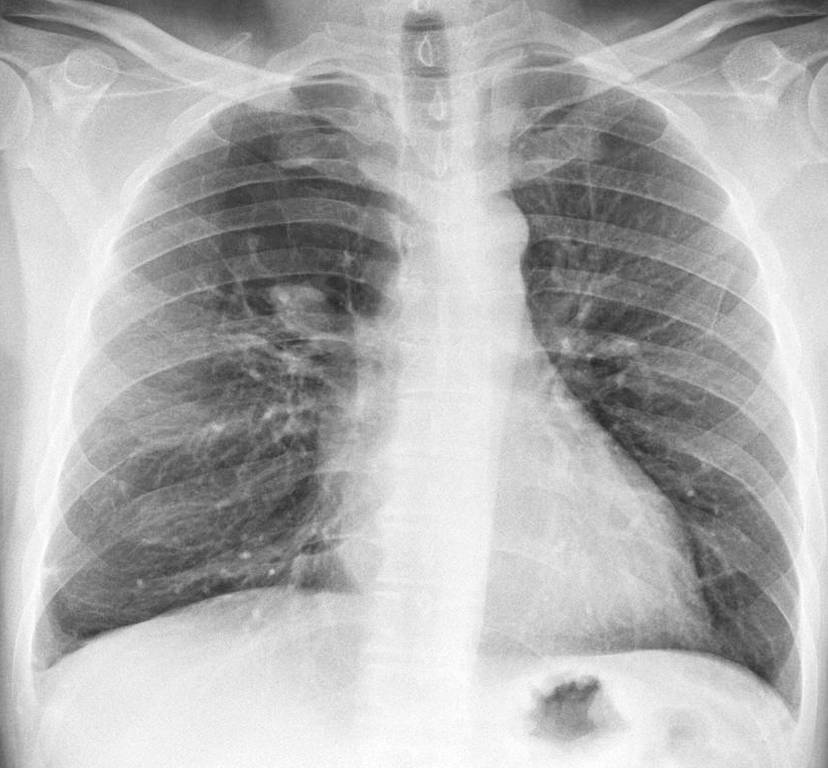
Fig. 12
Findings: PA radiograph shows a right parahilar nodule (A, arrow). Most of the right upper lung is hyperlucent compared to the left side. The combination of a central nodule and peripheral hyperlucency is suspect of mucus plugging with distal overinflation. Coronal CT shows the mucus plug (B, arrow) and the lack of bronchi in the right upper lung. Diagnosis: mucus plug in congenital bronchial atresia.
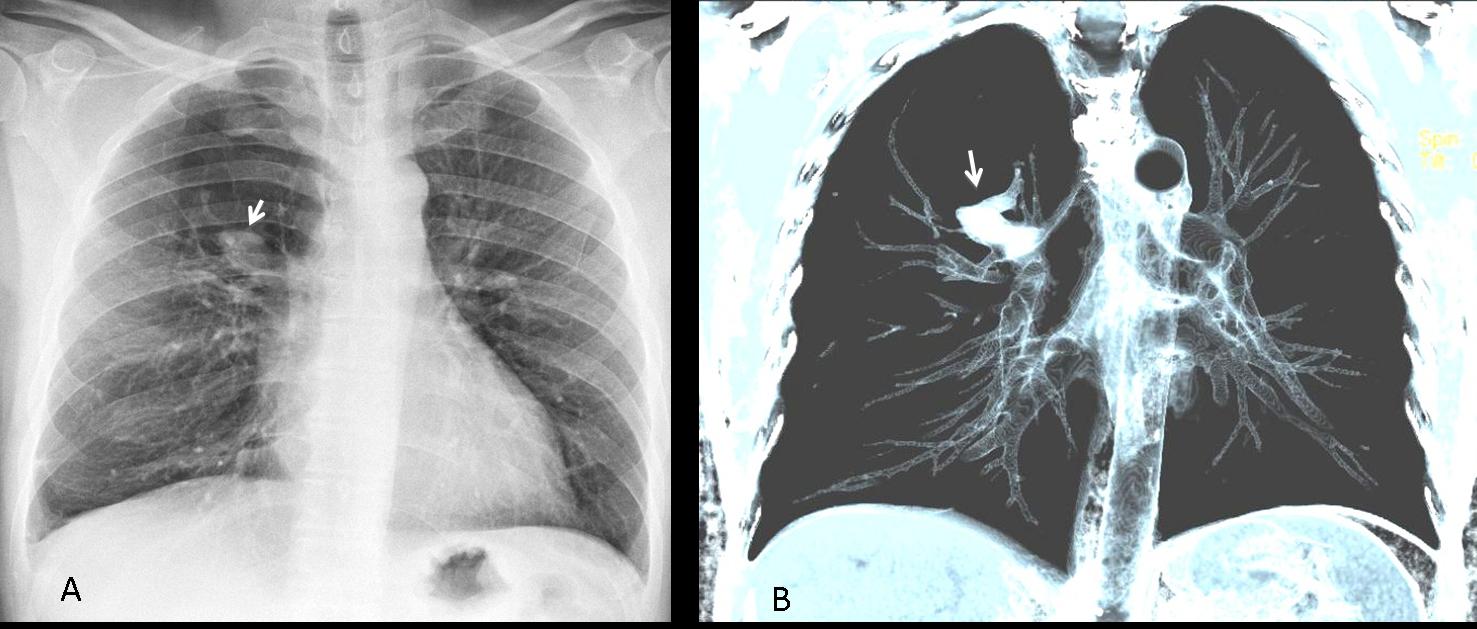
Fig. 13
Mucus plugs occur when obstruction of a segmental bronchus allows the mucus to accumulate distally. They usually manifest as tubular opacities which, when seen end-on, may simulate a nodule. Mucus plugs can be seen in congenital and acquired conditions. In my experience, the hyperlucency associated with congenital bronchial atresia facilitates identification of the plug in the chest radiograph. CT easily confirms the diagnosis (Fig. 14).
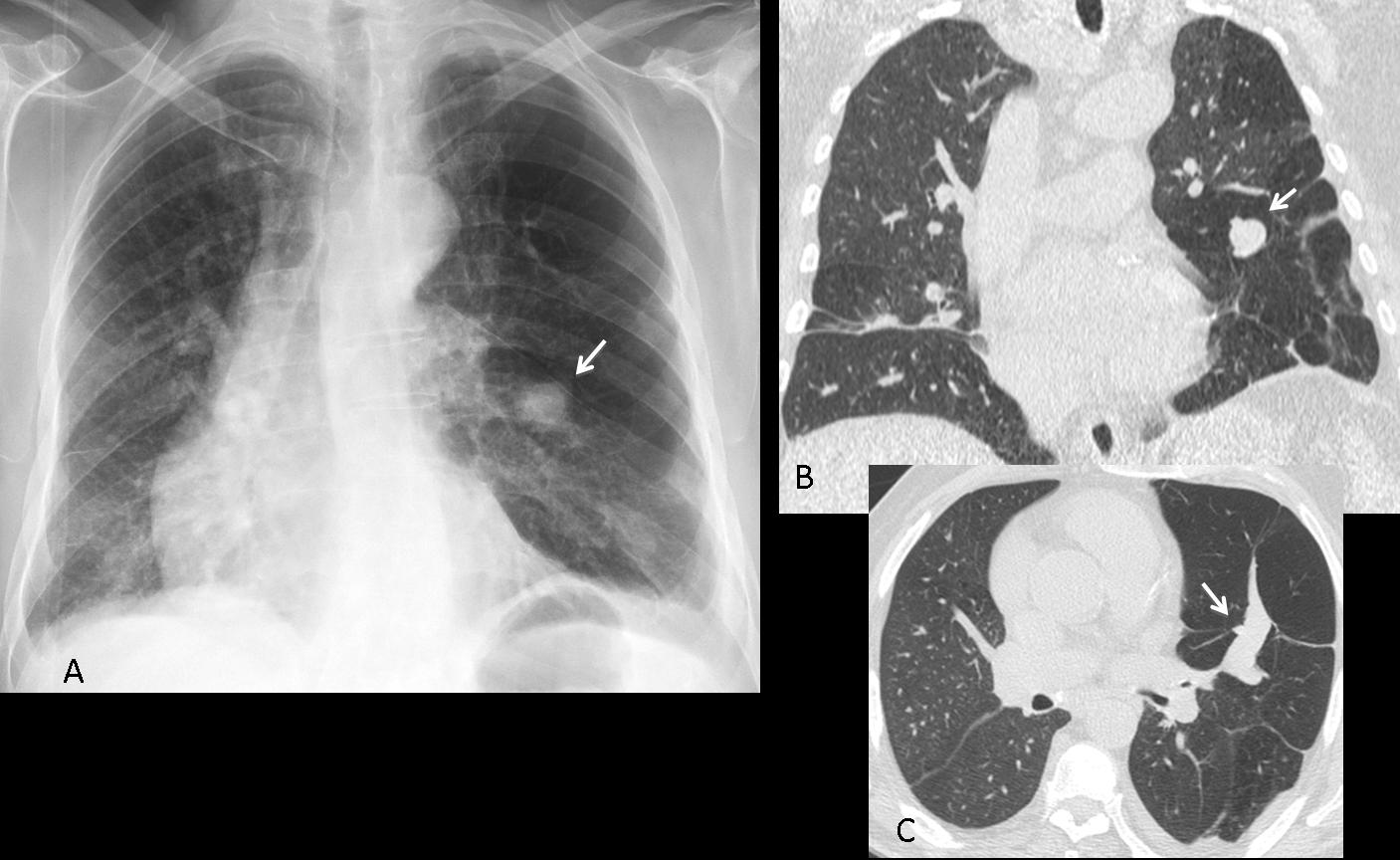
Fig. 14
Fig. 14 (above): 64-year-old man with cough and moderate dyspnea. PA chest film shows left lung hyperlucency with a nodule in the middle field (A, arrow). Coronal CT confirms the nodule (B, arrow) and hyperlucency of lower lung. Axial CT depicts the typical appearance of a mucus plug (C, arrow). Diagnosis: congenital bronchial atresia.

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- Not all nodular lung lesions represent carcinomas or granulomas.
- Round pneumonias and hematomas present as transient nodular lesions, which are easily suspected based on the presenting symptoms and confirmed with follow-up films.
- Rounded atelectases are peripheral nodules associated with pleural disease and loss of volume of the affected lobe. CT appearance is pathognomonic.
- When seen end-on, mucous plugs occasionally simulate nodular lesions. The association with hyperlucency suggests bronchial atresia. CT is diagnostic.


chest, CT, diagnosis, EDiR, European Diploma in Radiology, radiography
dear Dr Pepe,
thank you for interesting case.
PA chest x ray :
– bilateral lungs parenchyma is visible specially i LF like in parenchymal fibrosis changes and scars.
– there are no visible nodular leasions in PA projection
– there is no pleura effusion, no pneumotorax.
– the left diaphragm is a bit to high but it can be subjective
– the middle part of mediastinum i slightly enlarge withe a smooth relief of the right margine.
in lateral projection in retrosternal projection is well see, with a sharp margines rounded mass.
in lateral projection are also seen DJD changes of T spine.
The CT scan prove a well define mass in retrosternal compartment.
On the CT scan of upper abdomen anterioly to the upper pole of left kidney is well rounded with sharp margines mass suggest a adrenal TU.
The right adrenal gland is fainty see, but it has also round not well define margine – Tu susp.
An anterior mediastinal mass is shown in the lateral projection. This finding is confirmed in the CT and it has soft tissue density. Also, a probable adrenal metastases is seen on the lower images.
Given the age and symptoms of the patient, thymic carcinoma is my first option. Lymphoma is my second one, but I miss the nodal involvement.
Thanks for the case Doc. Greetings from Chile!!!
Welcome to the blog! Why do you place the lesion in the mediastinum?
the joint images from an xray and Ct scan suggest a primary Tu with metastasis to adrenal glands, bilateraly wich is not very rare. the pulmonary primary tumor i on the first place metstaic changes to andrenal glands, and it usually bilateral.
the secound ddx is an rounde pneumonia, which featers in pediatric group of patient, with independed adrenal leasions.
that doesnt fix with this patient. the bone age show this is an adult patient.
against thymoma talk the localisation which is usually the anterior mediastinum.4 T rule.
Round pneumonias occur in adults. I assume your excluding thymoma because the lesion is not in the anterior mediastinum is a typographical error.
thank you for answer. I was suggesting that round pneumonia ist mostly typical
for pediatric group of patient. it is also possible in a adult grup of patient.
thymoma ddx is rather improbable. there are maybe couple of cases describe an ectopic pleural thymoma….and in this case the mass isnt really well rounded. it has small spikules whats suggest that the leasion comes from the lung. when its comes from the lung and we have belateral adrenal leasions, that strongly suggest the lung cancer with metastasis to the lungs….it also has a slightly CE(its hard to say it on one image ).
but of course in medicine everything is possible and it could be also a round atelektasis with comet tail sign with independent adrenal leasions. such lungs leasions are very often in subpleural localisation.
dear dr Pepe I hope I become clear with my invastigetion…hopefully:-)
How would you differentiate a lung tumor from a round pneumonia?
dear dr Pepe, to ddx lung leasion in the beginning i ll have an interview with the patient. after that i ll compare present images with past imagies of course in realation to time periods.
I ll also check inflamation morfological markers.
After that, when the ddx ll be still uknown I ll choose pet ct scan becouse of high sensivity for metabolic leasions. that ll help me to diferentiate.
Ill also consider biopsy under ct.
besides i ve one more thought about an ddx lung lesion, namely it is an hampton hump with no related bilateral adrenal leasions?…..:-)
Apart from the lesion at the anterior mediastinum and the adrenal lesion , there is also a lesion a little bit superior to the first lesion , just anterior to the trachea. So there are multiple mediastinal lesions and the adrenal lesion. Thymic tumors with metastases is an option. Thymic carcinoid tumor does not correlate well with the clinical evidence.
The lesion you describe is the upper portion of right pulmonary artery. Of course, you need the whole CT study to be sure.
squam cell carcinoma with adrenal glands metastases….
Carcinoma of lung with adrenal met.
Timoma!
This case iż a typical coincidence of mediastinal thymoma with adrenal adenoma (Cushing’s perhaps). This requires further blood evaluation for hormones and tests for myasthenia.
Let me know id tej answer is any food- I have a low self esteem level 😉
Ok, my lesson is not to review images via cell phone 🙂
The mass in fact is located in the lung… so probably cancer with metastasis to adrenal adenoma (adrenal collision tumor?)- there are two densities visible fat like and soft tissue in the left adrenal. The right one seems to be enlarged by a tumor- meta?
Looking at films in your cell phone will lead to misreadings and will lower your self-esteem.
Naturally I ment the quiz pictures- it would be quite irresponsible for diagnostics…
Can’t wait for the answer- this one is really good, brings up many doubts…
OK one more update concerning the lateral projection film where the lung infiltration is seen (correlating with the ct) plus a anterior mediastinal mass is seen that needs further evaluation perhaps a mateastatic lymph node or thymoma.
Common things being common, this is statistically most likely a thymoma with adrenal adenoma. Ddx would include thymic carcinoma with metastatic disease to the adrenal gland. A fascinating possibility would be a MEN I syndrome, which would make the ant mediastinal mass most likely a thymic carcinoid tumor.
What about the statistical probability of the clinical findings?
I think dominik is right.
thymus is normal for the age of patient (fat replacement).
on CT the mass is intrapulmonary, lateral of thymus with irregular borders.
On chest x ray also we can see enlargemet hilum lymph nodes on the lateral view.
lung carcinoma with metastatic disease to the adrenal gland?
…cosmico Professore….la prima cosa da interpretare è la sede della opacità, vista all’Rx e TC: non penso che sia mediastinica, ma di pertinenza polmonare( escludiamo il Timoma)…una polmonite “rotonda” può anche essere esclusa, per sede non tipica nel polmone e mancante dei segni dell”angiogramma” alla tc con m.d.c….un cr polmonare primitivo mi sembra strano per la omogeneità della massa e per il fatto che non prende contrasto alla Tac…nel frattempo hai mostrato un espanso surrenalico a sx, che non produce sindrome endocrina…anche su tutti dicono cr polmonare e metastasi surrenalica , io penso ad una ipotesi inversa, molto rara in verità, di Cr surrenalico e metastasi solitaria nel polmone.
Pancoast tu at the right side
metastatic lymph node in the retrosternal space and in the adrenal gland
Pancoast tu at the right side
metastatic lymph node in the retrosternal space and meta in left adrenal gland
I believe there is some degree of left hilum downwards displacement. Or not?
Location of left hilum seems OK to me.
Crazy idea! I don’t like aorta’s contour. Is arteritis excluded?
Aorta is OK. See comment by Genchi Bari today
…gentile collega….una analisi più attenta delle immagini, mi porta alle seguenti conclusioni: la formazione polmonare, che appare omogenea e non assume m.d.c. ( anche senza il segno dell”angiogramma”, come nelle polmonite classiche) depone per polmonite “rotonda”….mentre l’immagine surrenalica sx, piccola ed a margini regolari, depone per adenoma”non funzionante”…scusa per la “revisione” del referto.
Now you are applying wisely the KISS method…
….grazie dr Pepe ma a me, come a tutti i radiologi, piace avere molto fantasia….ed i radiologi sono artisti a cui piace andare “controcorrente”…a volte!!!!
Yours cases are very hard!!!! Compliments!!!!!B 🙂
I believe the cases can be diagnosed if we pay attention to the details. The case presented here was suspected of pneumonia and confirmed by waiting. That was hard because the lady’s husband was a VIP!
…congratulazioni dal dottor Genchi Bari, che dopo una inceretezza iniziale, ha fatto la corretta diagnosi di plomonite “rotonda” ed adenoma surrenalico “non-funzionante”.
Yes. Well done!