Dr. Pepe’s Diploma Casebook: Case 54 – SOLVED!
Dear Friends,
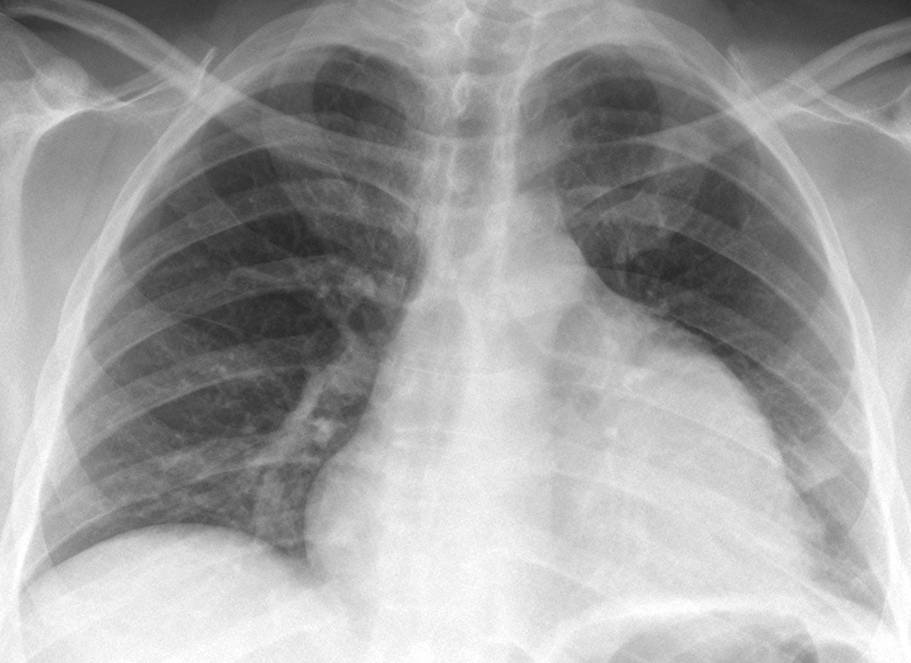
Welcome to this week’s case. Radiographs belong to a 43-year-old male with chest pain. Leave me your thoughts and diagnosis in the comments and come back on Friday for the answer.
Diagnosis:
1. Hypertrophic cardiomyopathy
2. Mitral disease
3. Non-cyanotic congenital heart disease.
4. None of the above

Findings: radiographs show an enlarged cardiac silhouette with abnormal contour of the left heart border (A, arrows). Mitral disease can be ruled out (no left atrial enlargement or vascular redistribution). There are no signs of right-to-left shunt, which is the hallmark of non-cyanotic heart disease. Hypertrophic cardiomyopathy does not change the heart contour until the late stages. A clue to the diagnosis is the faint rounded opacity in the lateral view (B, arrows), which prompted a CT study.
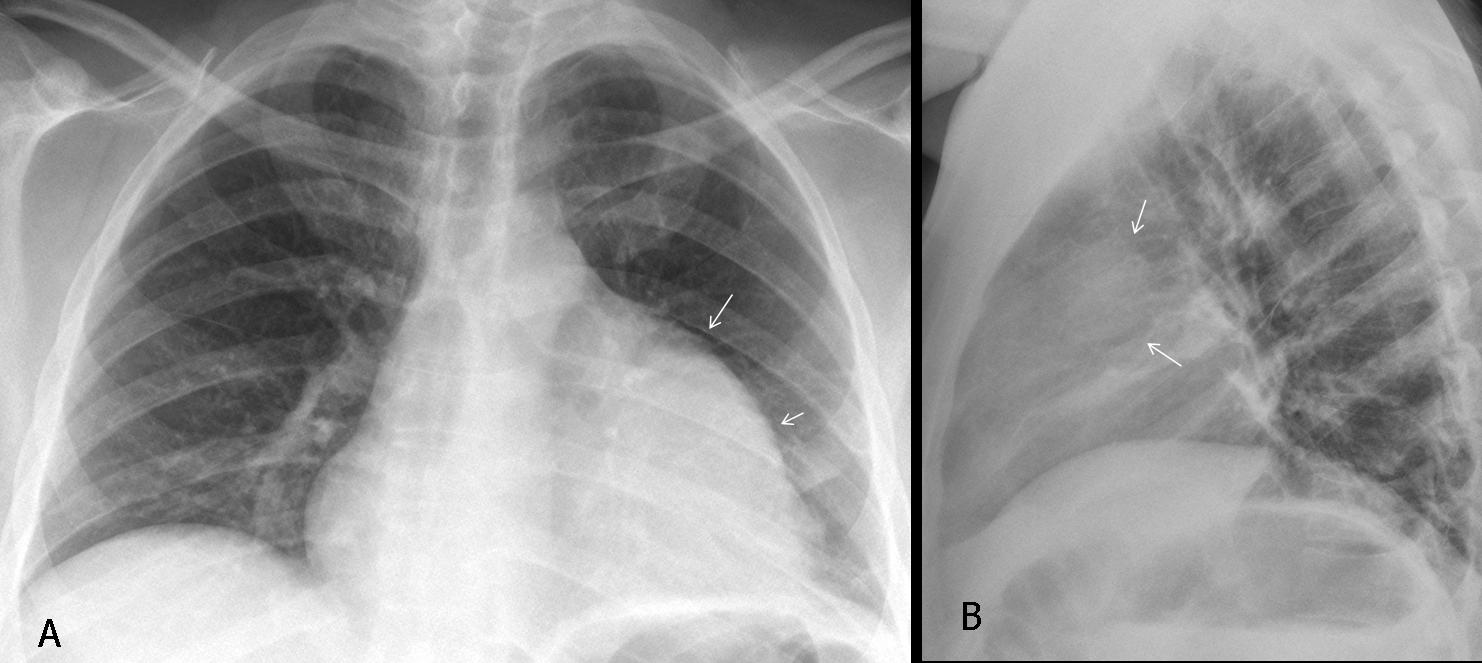
Fig. 1
Enhanced CT demonstrates that the prominent left heart border is due to a large, poorly enhancing mass apposed to the left aspect of the heart (A,B, arrows). Biopsy of the mass diagnosed a mediastinal sarcoma.
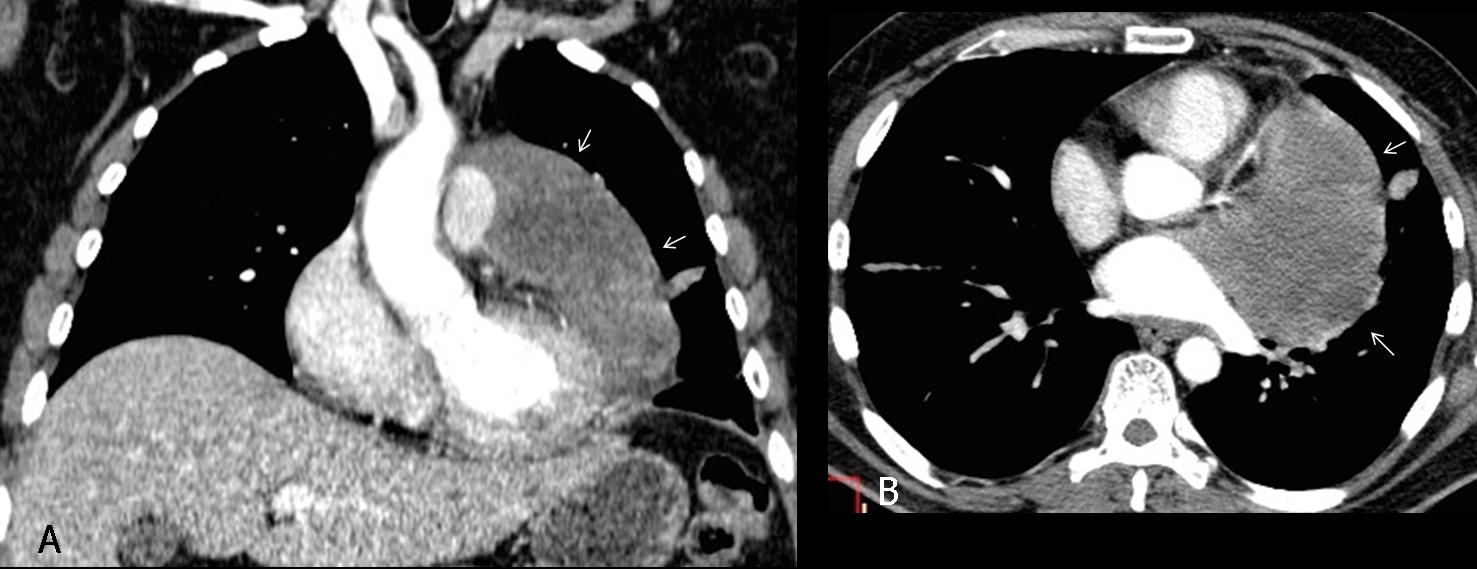
Fig. 2
Final diagnosis: Mediastinal sarcoma simulating cardiomegaly.
The presentation today focuses on causes of false cardiomegaly. When the cardiac silhouette is seen to be greater than or equal to 50% the diameter of the chest, our immediate response is a diagnosis of cardiomegaly, and most of the time we are right. But, occasionally, the apparent cardiomegaly is not real and is caused by a process that simulates it.
One uncommon cause of false cardiomegaly is the presence of a lower anterior mediastinal mass apposed to the heart and having a similar density, thus creating the illusion of an enlarged cardiac silhouette. The diagnosis is suspected based on a lack of clinical and EKG signs of heart disease and an abnormal appearance of the cardiac contour. Confirmation of the suspected diagnosis is easily made with CT.
Any anterior mediastinal tumour can lead to this misdiagnosis. The most common ones are of thymic origin because they have a tendency to descend and locate around the heart (Fig. 3). Thymolipoma is an unusual fatty tumour that surrounds the heart and simulates overall cardiomegaly (Fig. 4).
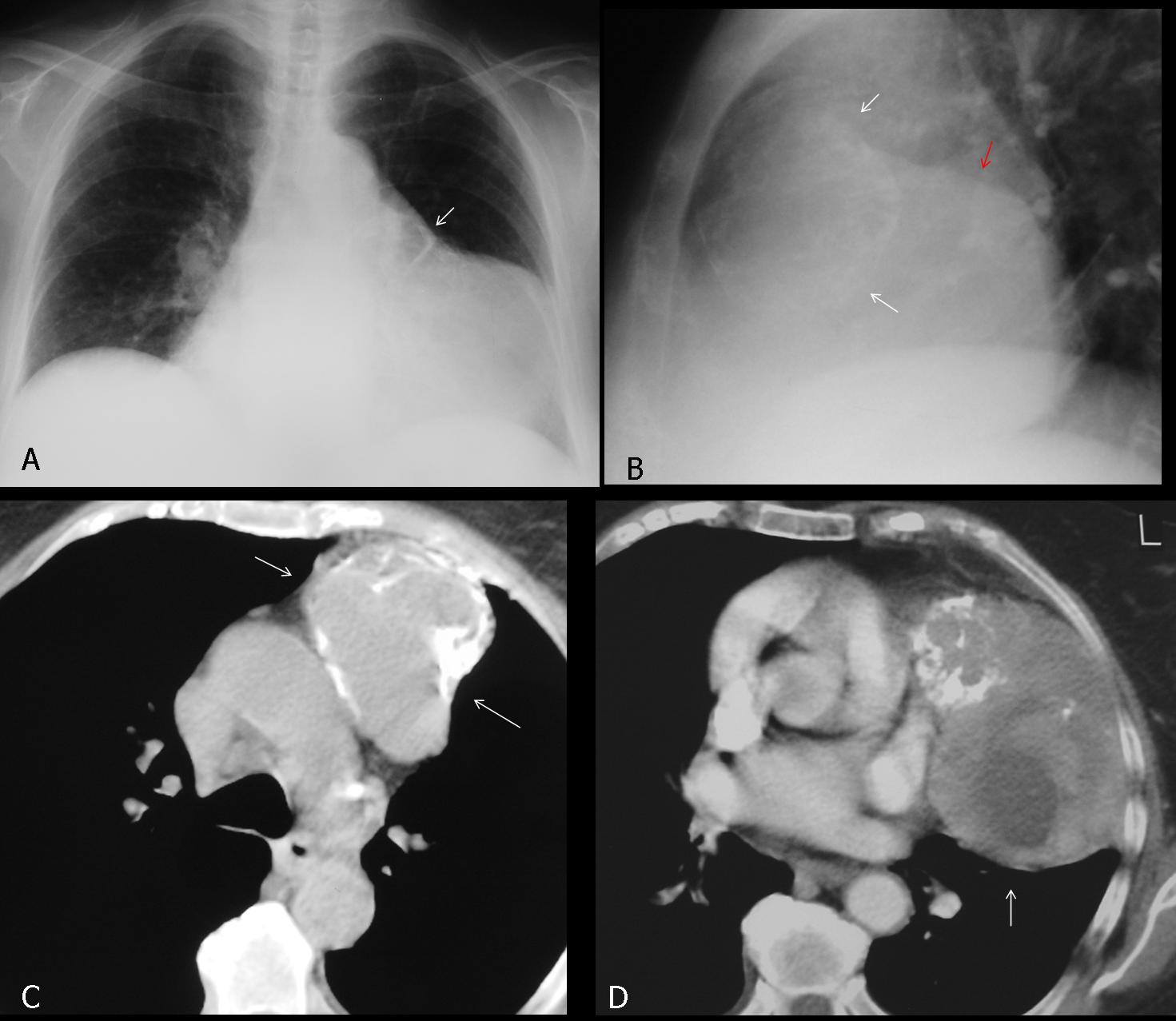
Fig. 3
Fig. 3 (above): 58-year-old man with apparent cardiomegaly. Nonetheless, a diagnosis of mediastinal mass is suggested by the extra-cardiac calcification (A,B white arrow) and a double contour in the lateral film (B, red arrow). Axial CT confirms the partially calcified mediastinal mass (C,D, arrows), apposed to the left heart border. Diagnosis: Malignant thymoma.
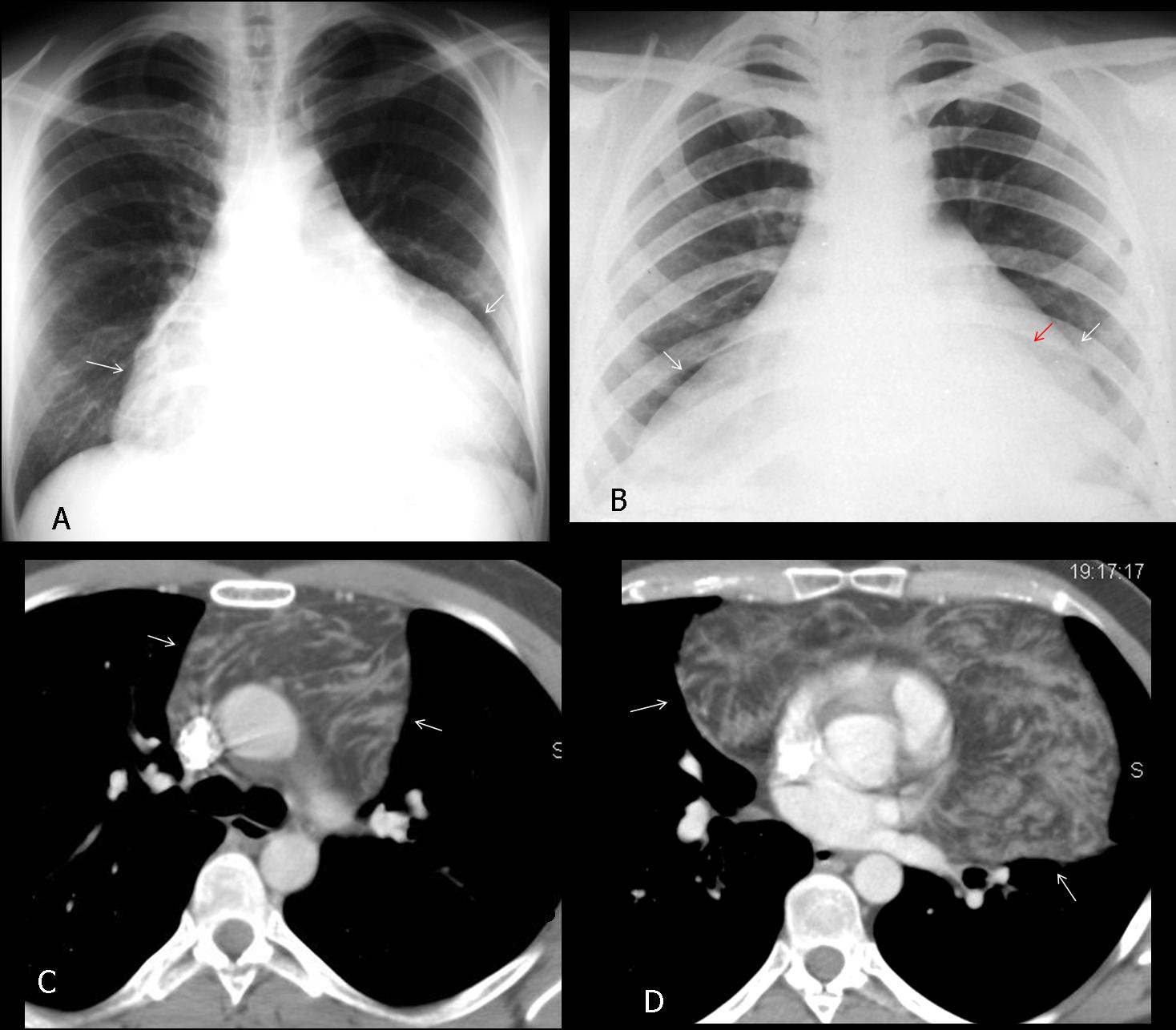
Fig. 4
Fig. 4 (above): two patients with thymolipoma. In both cases, the tumour surrounds the heart, simulating overall cardiac enlargement (A, B, white arrows). In B, the outline of the heart is faintly seen (B, red arrow), enclosed by tumoural fat. Axial CT in the first patient confirms the fatty nature of the thymolipoma surrounding the heart (C,D, arrows)
By far the most common cause of false cardiomegaly is pericardial effusion of any cause. In the PA chest film, it is typically seen as a globular cardiac silhouette with decreased pulmonary circulation. However, this appearance may be deceiving because cardiomyopathy can show similar features (Fig. 5). In my experience, the best sign of pericardial effusion is posterior displacement of the epicardial fat in the lateral view (fat pad sign) (Fig. 6). On visualisation of the anterior mediastinal fat, pericardial thickness can be measured (Fig. 7), and this should not exceed 2-3mm in normal conditions. The fat pad sign is not always seen, but when present, it is a highly reliable finding. Nonetheless, it is not pathognomonic and should always be followed by echocardiography to confirm the suspected effusion.
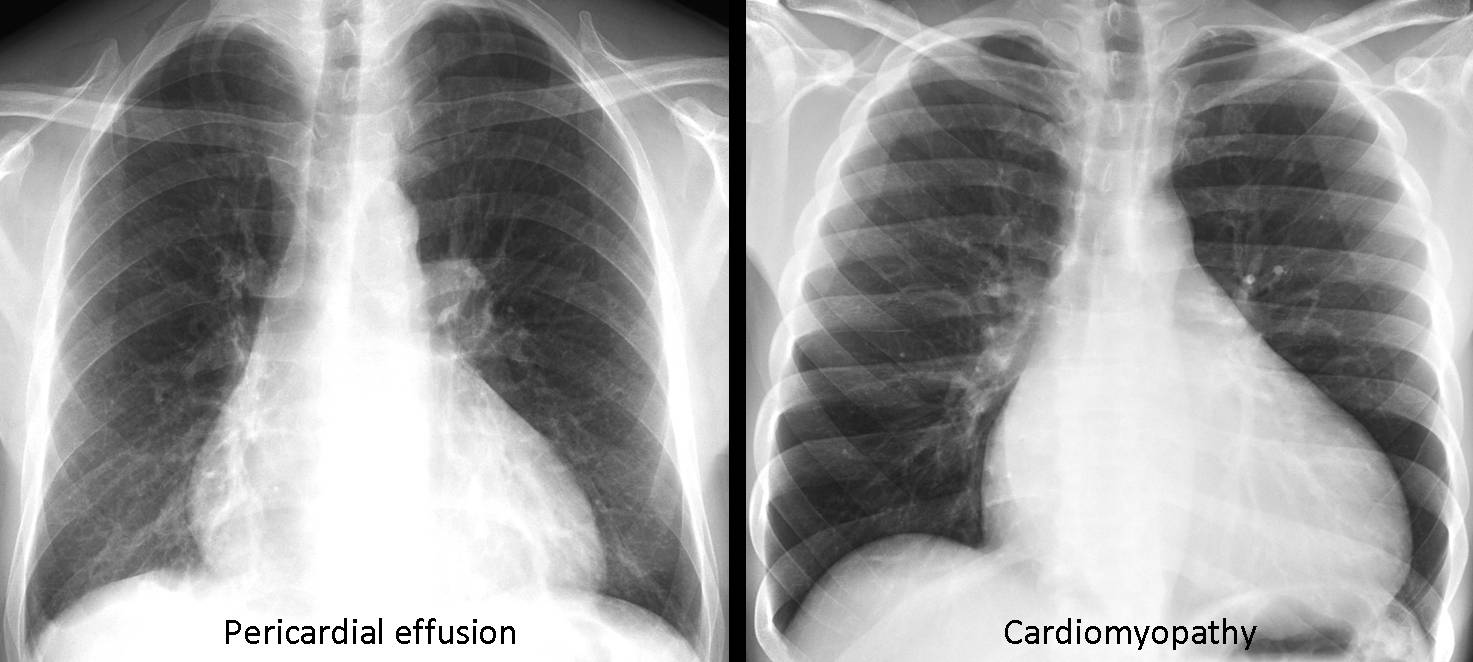
Fig. 5
Fig. 5 (above): two patients; one with pericardial effusion (A) and the other with cardiomyopathy (B). Note the similar appearance of these conditions.
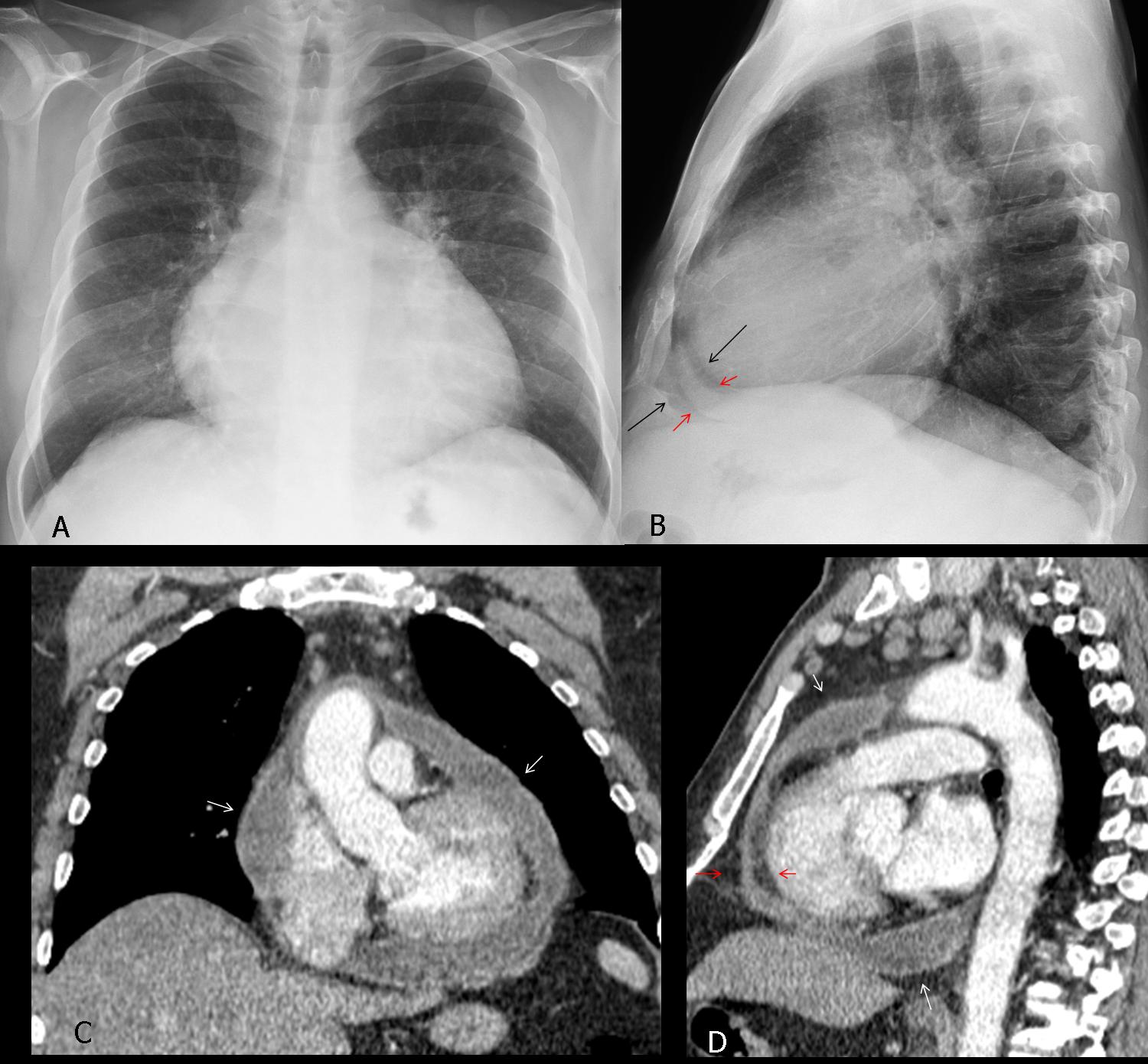
Fig. 6
Fig. 6 (above): 46-year-old man with liver cirrhosis and pericardial effusion. Note the typical globular appearance of the cardiac silhouette in the PA view (A). The diagnosis is evident in the lateral view, which shows the thickened pericardium (B, red arrows) between the epicardial and mediastinal fat (black arrows). Coronal and sagittal CT confirm the presence of a moderate amount of pericardial fluid (C,D, white arrows). Note the fluid between the epicardial and mediastinal fat in the lateral view (D, red arrows).
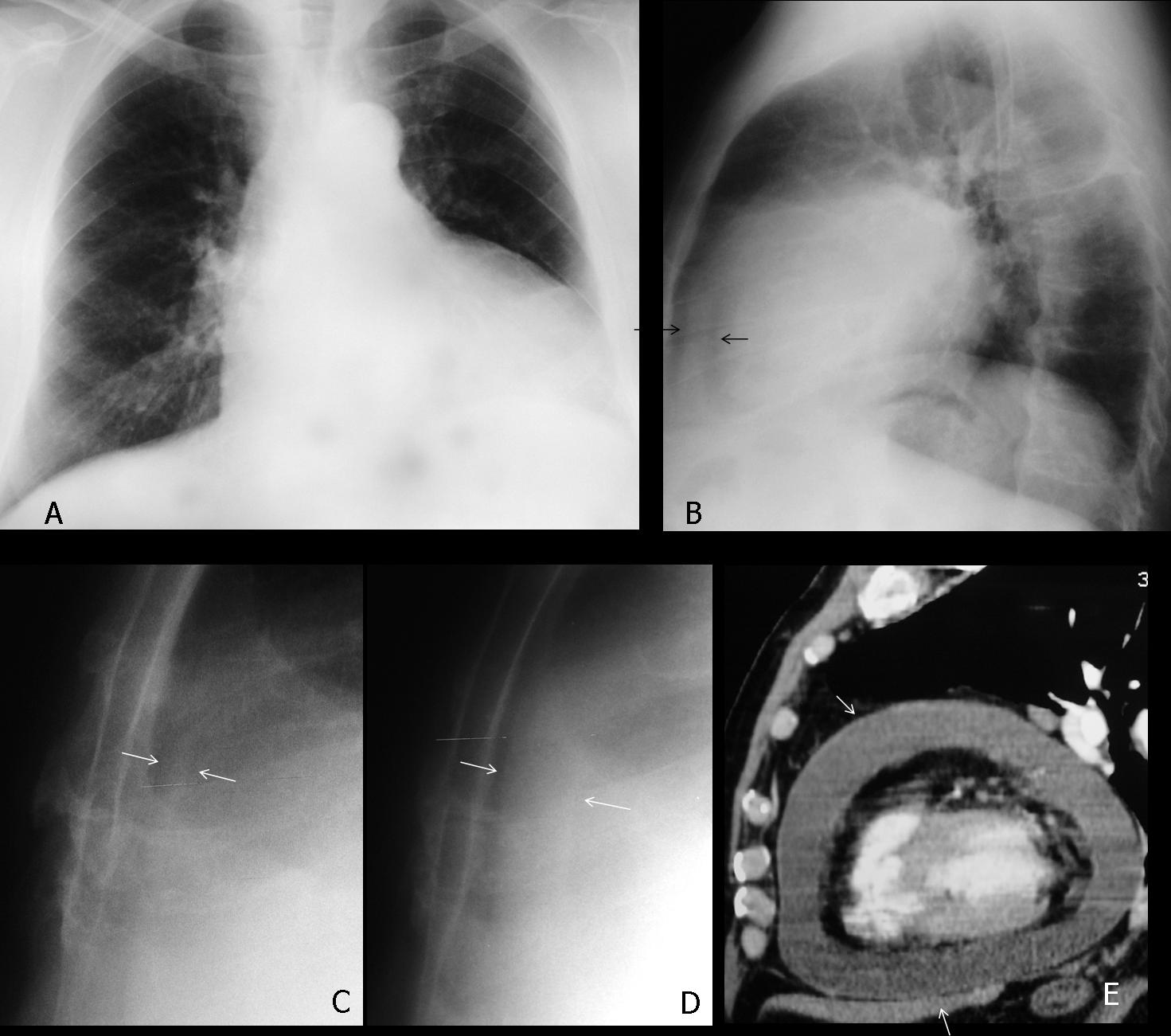
Fig. 7
Fig. 7 (above): 53-year-old man with pericardial effusion simulating cardiomegaly in the PA view (A). The diagnosis is suggested in the lateral view by the thickened pericardium between the epicardial and mediastinal fat (B, arrows). Cone down lateral view taken three months earlier shows normal pericardium (C, arrows). Compare with the present film (D, arrows). Sagittal CT confirms the presence of a large pericardial effusion (E, arrows).
Pericardial metastasis is not rare in patients with disseminated malignant disease. The most common primaries are lung and breast. They can be suspected by the irregular contour of the cardiac silhouette and confirmed with CT (Fig. 8).
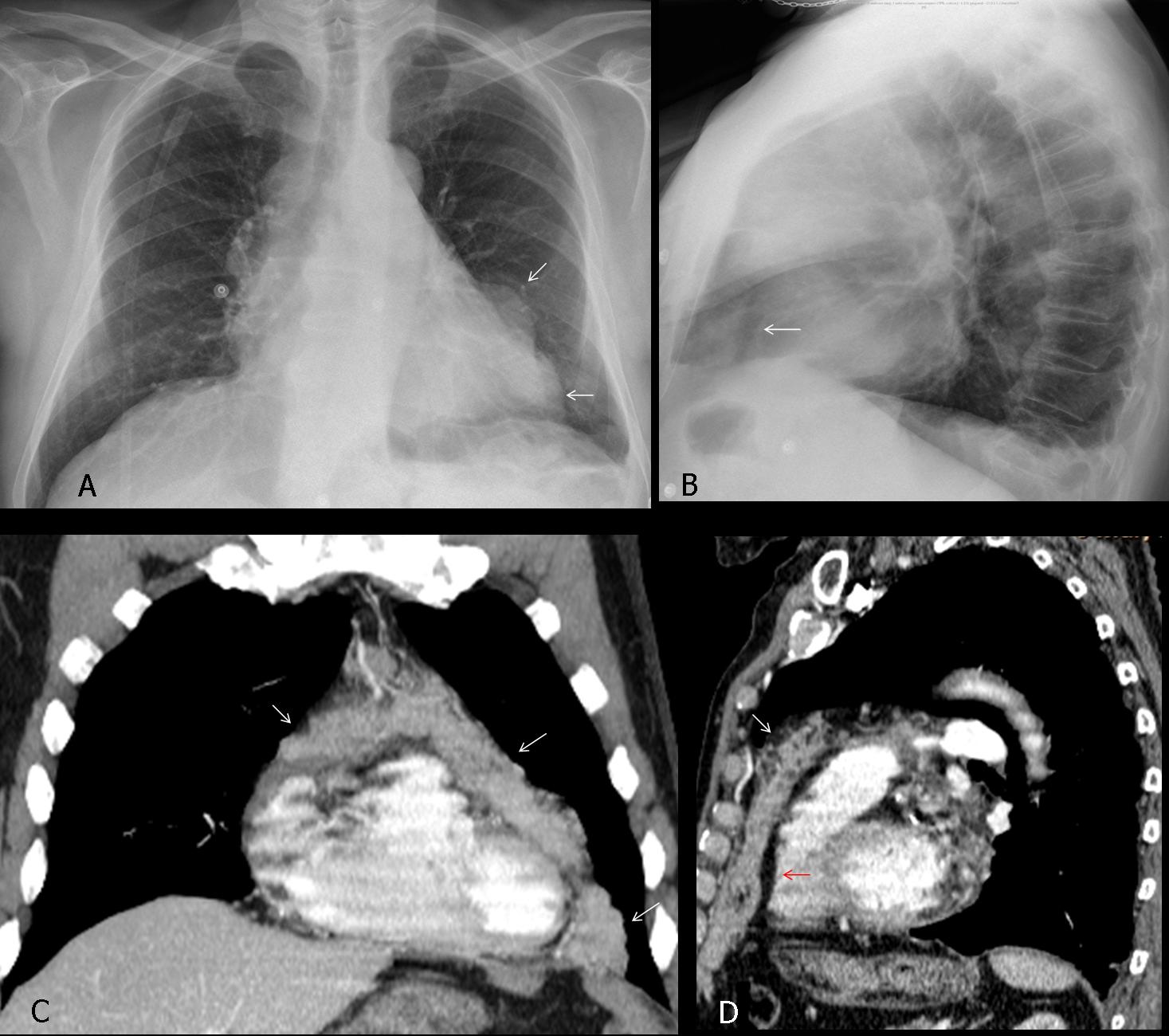
Fig. 8
Fig. 8 (above): patient with widespread malignancy. Pericardial metastasis is suggested by the abnormal heart contour (A, arrows) and epicardial fat displacement in the lateral view (B, arrow). Axial and coronal CT images confirm metastasic invasion of pericardium by solid masses (C,D, white arrows). Note the displaced epicardial fat in the lateral view (D, red arrow).
In young people, another cause of apparent cardiomegaly is severe pectus excavatum. The sternum compresses and displaces the heart towards the left, simulating cardiac enlargement (Fig. 9). The diagnosis is readily apparent by looking at the lateral film.

Fig. 9
Fig. 9 (above): 17-year-old male with marked pectus excavatum simulating cardiomegaly in the PA chest film (A). Lateral film confirms the pectus (B, arrow). Sagittal and axial CT images (C,D) confirm marked narrowing of AP diameter of the chest and displacement of the heart towards the left.
Last, but not least, remember that heart size cannot be evaluated properly in expiratory and supine films (Fig. 10).
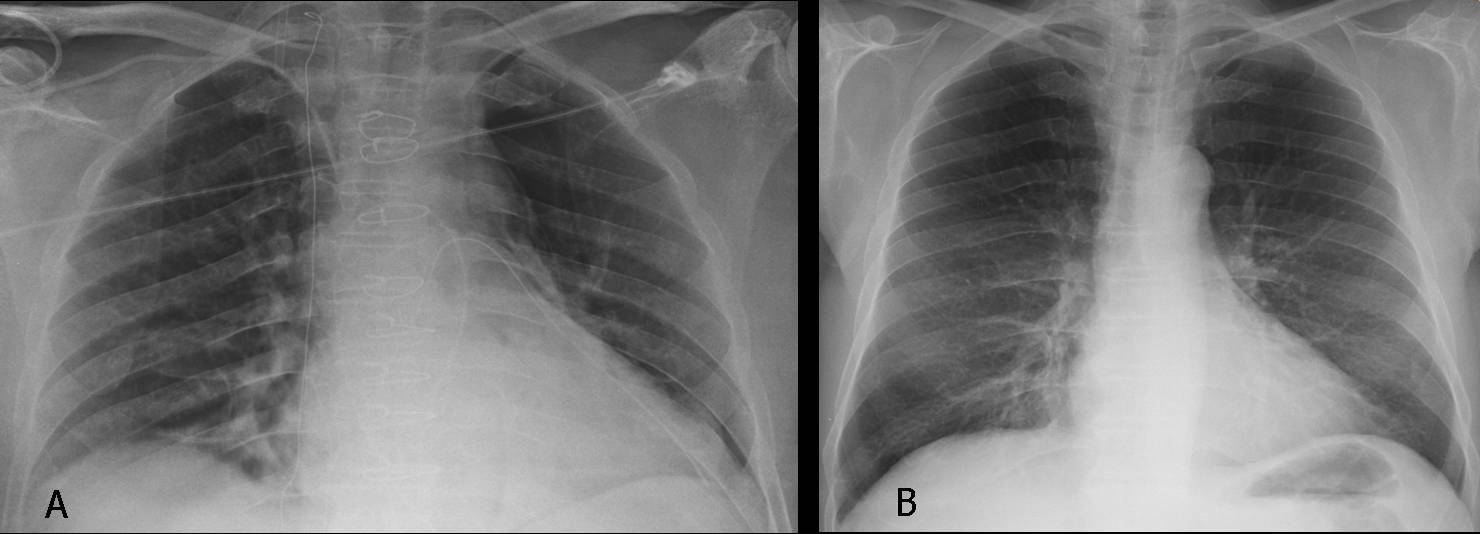
Fig. 10
Fig. 10 (above): supine film (A) in which the cardiac silhouette appears enlarged (A). Previous upright film in the same patient shows a normal-sized heart (B).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
1. The most common cause of false cardiomegaly is pericardial effusion.
2. The most reliable sign of pericardial effusion is posterior epicardial fat displacement in the lateral view.
3. An uncommon cause of false cardiomegaly is an anterior/inferior mediastinal mass.
4. In an asymptomatic young person with enlarged heart, think of pectus excavatum.


Hello,
I’ll tryo to be the first one this week.
So first of all I think correct answer is 4. none of the aobve because in my opinion the heart itsefl is quite intact.
The morfology of changes makes me think of pericardial mass.
In this case with history given I think I would consider a malignancy although it is not so common.
Perhaps it could be neoplastic pericarditis.
On the lateral mage I can’t see the descending aorta- is it there? If not I would consider pathology among aorta.
Maybe a little hint- although it is quite soon.
PS Are You coming to Warsaw for the next EDIR ?
You must feel like Gary Cooper in “High noon”. You are totally alone!
Not invited to Warsaw for EDIR. Next time.
I hope I won’t be needing NEXT time :]
there is enlargement of the right heart which we can see on the lateral view,it is filling more then 1/3 of retrosternal space.In mitral stenosis we can see left atrial enlargement( double density in a heart silhouette)and pulmonary hypertension.Here this is not the case.In non-cyanotic heart disease there would be changes in pulmonary circulation (ASD,PDA,APSD,coarctatio aortae etc. ).On a film there is no vascular changes. I would go with hypertrophic cardiomyopathy (right heart). Or maybe is something else.. 🙂
dont be to hard to me too,as mr.jose said..l am still a resident.. 🙂
For a resident you didn’t perform badly. As you will see tomorrow, it is a mediastinal tumor simulating cardiomegaly.
Mitral disease
….vi è una congestione del piccolo circolo, con ipertrofia ventricolare sx; dilatato il tratto ascendente dell’aorta mentre è scarsamente visibile( perchè ipoplasico) il tratto discendente….ci sono incisure sul bordo inferiore di alcune coste, bilateralmente(ipertrofia art. intercostali)…..Diagnosi finale: coartazione aortica post-duttale. NB. Il Bari è in netta ripresa in campionato…..aspettiamo acquirenti anche dalla Turchia!
….quello che mi ha fuorviato la diagnosi è che hai proposto tra le possibili diagnosi, solo patologie cardiache…tralaltro sono stato forse fuorviat0 da presunte irregolarità sul margine costale inferiore…però, però però….la morfovolumetria cardiaca è “insolita” per qualunque cardiopatia…inoltre lo spazio retrosternale è “occupato” da una massa( pensavo all’ectasia pre.stenotica di una cortazione)….rivedendo la diagnosi finale direi che è una delle 4 cause di masse di tale comparto e siccome”scende” a rivestire il cuore, io penso ad un Timoma.
In my humble opinion, there is an enlargament of the left ventricle, with the right heart with a normal size and morpphology. Aorta and pulmonary arteries seem normal. I would bet on a mitral disease.
P.S. It is my first time here, so don’t be too hard with me…
As a welcome present, I will give you a tip: in the plain film it is difficult to determine which ventricle is enlarged, unless it is obvious. Perhaps is not a ventricle…
2. Mitral disease, because the left atrium is enlarged.
Mitral disease
is the pulmonary vasculature increased? If so, then together with the left ventricular enlargement a ventricular septal defect might be an option.
At the same time there is insufficient inspiration, which can simulate increased vascularity.
Do you really think that the pulmonary vasculature is increased?
Hello!
Heart shadow is enlarged, but asymmetrically, it’s not suppose to be neither mitral configuration nor HCM. Congenital heart disease in unlikely because of normal pulmonary vascularity.
I’m agree with Murzin, abnormality is not in the heart itself. It could be mediastinal mass, possibly pericardial cyst or teratoma.
I think that we should include an intracardial mass such as a mixoma or a sarcoma in our ddx. Moreover i believe there is a small gap at the continuation of the posterior segment of the left diaphragram on profile image.
Believe the diaphragmatic changes are secondary to plate-like atelectasis at the lung base.
Any comment about the mass?
Not yet. Others are watching.
I think the answer is D. Could be a Tetralogy of Fallot?
i think the mass is extra cardiac. there is not realy enlargment of the heart.
the hulum is not enlagment,the pulmonary vasculature is not increased , there is not widening of the angle of tracheal bifurcation. the mass is located in anterior mediastinum.
There is obliteration of retrocardial space on profile view.
On PA view tracheal bifurcation seems normal to me.
Additionally, on profile view through cardial sillhouette, it seems there is a lobulated contour of a mass, borders most discernible at the height of the tracheal bifurcation so I would say a mass is positioned in middle anterior mediastinum.Left ”heart” contour could be contour of a large mass, i see that the left contour reaches above aortic arch which on PA looks just fine. Differential diagnosis: I would go for thymic origin or germ cell tumor (e.g. teratoma).Regards 🙂
I think the right answer is 4. No left atrium enlargement is against 1. and 2. And again for option 3. no cardiac chambers enlargement + the pulmonary arteries and veins look normal.
Probably the key for the diagnosis is the hilum overlay sign on the left (pulmonary artery <1 cm medial to the cardiomediastinal contour), this sign usually tells us that a mediastinal (anterior, middle-posterior) or paravertebral mass is present. The retrosternal space is occupied, so in my opinion there is a thymic neoplasm, lymphoma or germ cell tumor present. A vascular lesion such an aneurym can cause this sign but I don't think there is any.
This is the first time I wrote a comment in this blog, so don't be very tough with me,… just in case 🙂
As the answer will be posted tomorrow, I can give you a diagnosis;
correct answer is: mediastinal mass simulating cardiomegaly.
Congratulations to Murzin, who was the very first to suggest the diagnosis
and that’s so crazy these days, really?
could be myopathy equally fine;
here’s what happened in Romania; after all CT craziness with people like me refusing to go back to Xray and perform only head CT and no head Xray a famous sports player got hit by a car in some accident , CT wasn’t working and Xray was done was interpreted as normal cause some good old docs know how to do that and refused to send patient to some CT, it was hemorrhage and patient died and legal issues sprang over the case and good old radiologists and good old radiological science and good old Xray was not only useless and stupid but also detrimental like mortal….so why can’t we replace the good old crap with new bright good science and the useless means that proof wrong?
Wow! You have to stop drinking so much coffee!
Seriously, I don´t think anybody would be happy with a chest X-ray in a patient with significant trauma.
Blame the not-working CT unit, rather than the radiologist.