Dr. Pepe’s Diploma Casebook: Case 55 – SOLVED!
Dear friends,
Today I am presenting today chest radiographs of a 48-year-old man with previous resection of a carcinoid tumour of the ileum. Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
Diagnosis:
1. Granulomas
2. Amyloidosis
3. Calcified metastases
4. None of the above


Findings: the PA chest radiograph shows calcified nodules (A, arrows), apparently in an intrapulmonary location. However, the lateral view reveals that they are anterior and probably attached to the anterior chest wall (B, arrows). There is also a faint calcification in the right hemidiaphragm (A, red arrow).

Fig. 1
CT demonstrates that the nodules correspond to calcified pleural plaques, located in the anterior aspect of the chest (A,B, arrows), simulating intrapulmonary nodules in the chest radiograph. There are also some calcified diaphragmatic plaques (C, arrows).

Fig. 2
Final diagnosis: calcified pleural plaques in asbestos-related disease.
This case is presented to discuss pleural calcifications. These are easily recognised in the chest radiograph and are important because they may be related to serious pleural disease or complications. In addition, they may simulate pulmonary disease and lead to diagnostic errors, as in the case shown. From the imaging viewpoint, pleural calcifications can be classified as unilateral and bilateral.
Bilateral pleural calcifications are almost always due to asbestos exposure, and less commonly, to other inhalational diseases. The most frequent manifestation of asbestos exposure is pleural plaques of varying size and number. Calcification occurs in about 10% to 15% of cases. Plaques in the diaphragmatic pleura are a reliable sign of asbestos-related disease (Fig. 3).

Fig. 3
Fig. 3 (above): Two patients with calcified pleural plaques (A,B, black and white arrows) secondary to asbestos exposure. Plaques in patient A are less obvious than in patient B. Diaphragmatic calcification (B, red arrow) is practically pathognomonic of asbestos-related disease.
Malignant mesothelioma is the most common primary neoplasm of the pleura and is strongly associated with asbestos exposure. Pleural masses or thickening associated with bilateral pleural calcifications are reliable indicators of asbestos-related malignant mesothelioma (Fig. 4).
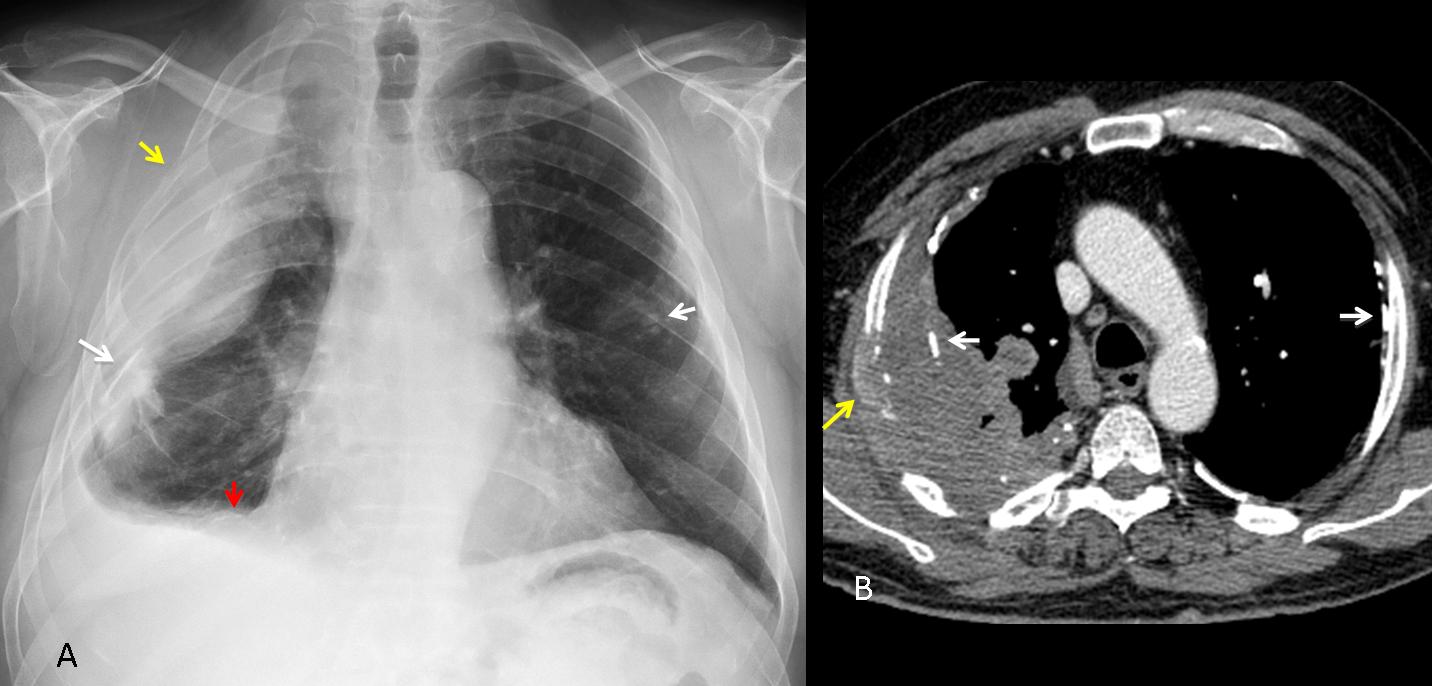
Fig. 4
Fig. 4 (above): 49-year-old man with asbestos-related malignant mesothelioma. The PA chest film shows pleural masses and calcification in both hemithoraces (A, white arrows). Note calcifications in the diaphragm (A, red arrow) and invasion of the third right rib (A, yellow arrow). The same findings are seen on CT (B, arrows).
Unilateral pleural calcifications may appear as isolated pleural plaques or chronic pleural thickening with linear calcification.
Isolated pleural plaques are innocuous and usually due to previous infection or haemorrhage, although a definite clinical history is often not elicited. They are typically flat and calcified, with well-defined borders (Fig. 5).
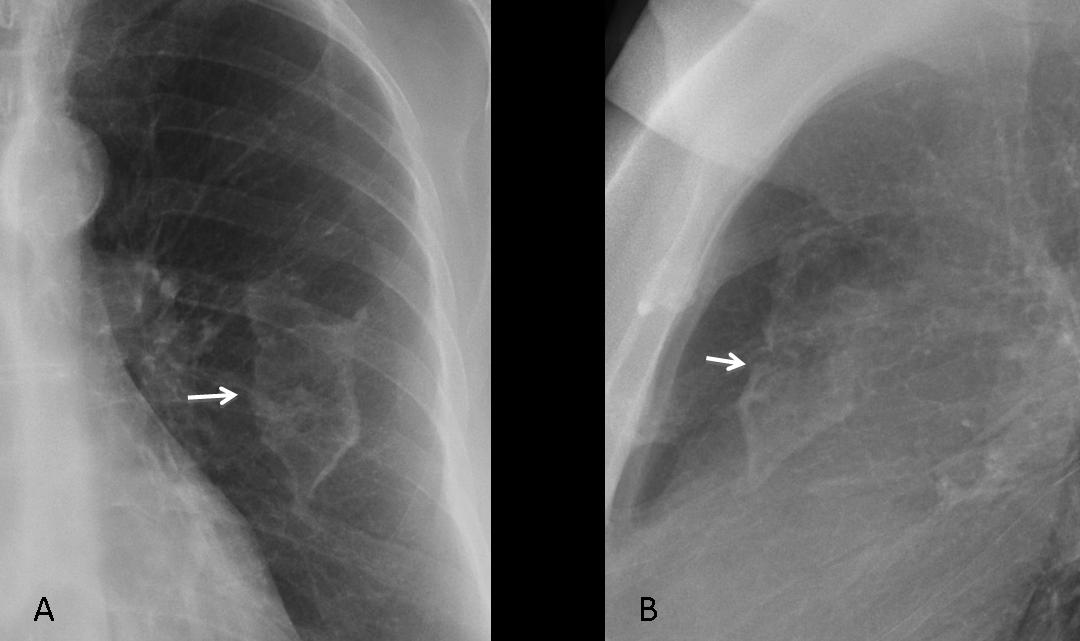
Fig. 5
Fig. 5 (above): typical appearance of an isolated pleural plaque in the PA and lateral views (A, B, arrows).
In isolated pleural plaques, high KV techniques tend to “burn” the calcium. When seen on-face, they may simulate a pulmonary infiltrate. Seen in profile they appear as a calcified line (Fig. 6) and the diagnosis is then apparent.
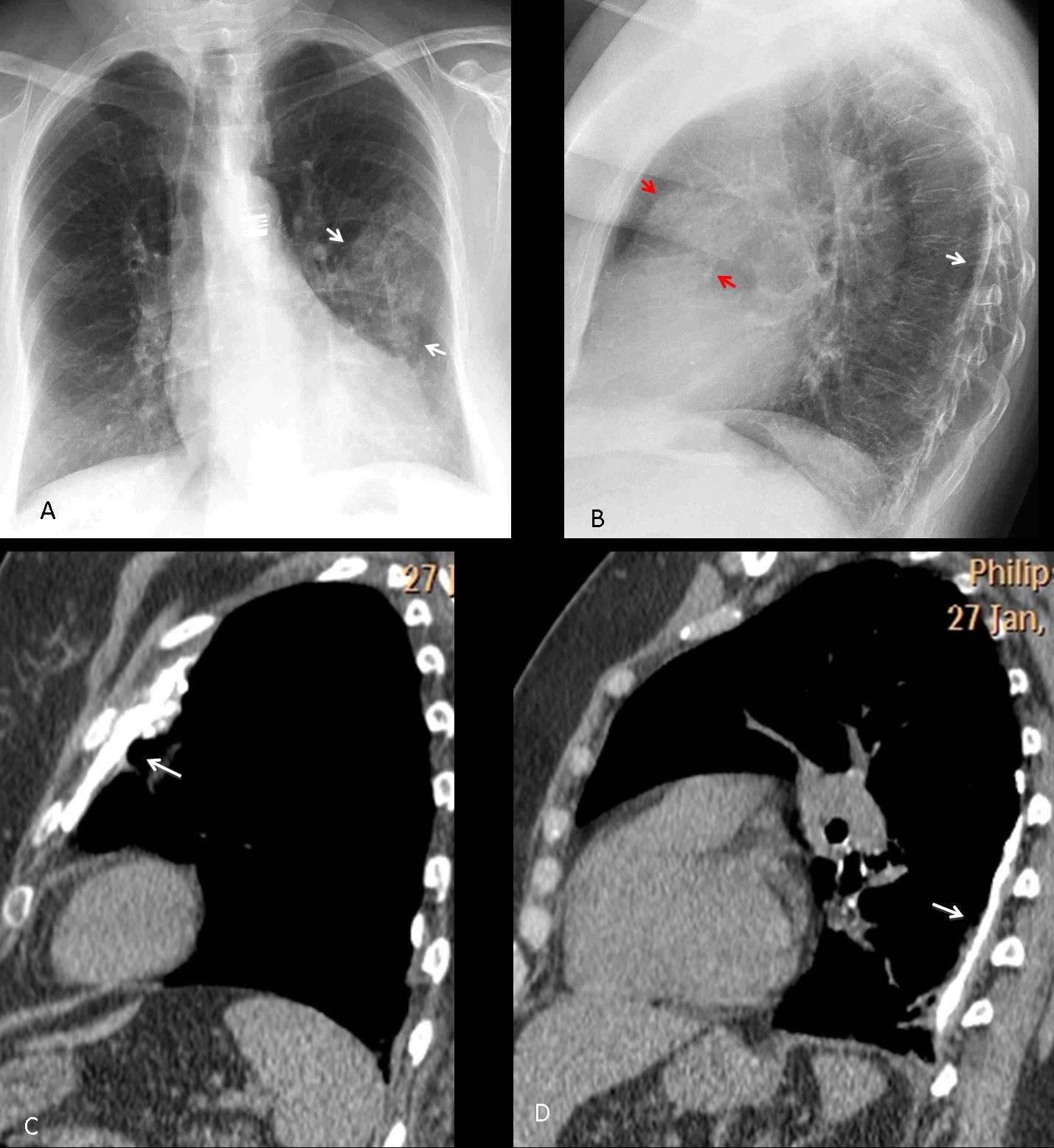
Fig. 6
Fig. 6 (above): 52-year-old woman with two pleural plaques. The PA radiograph shows the plaques on-face simulating a pulmonary infiltrate (A, arrows). In the lateral view, the posterior plaque is depicted as a calcified line (B, white arrow), whereas the anterior one is more oblique and simulates a rounded opacity (B, red arrows). Sagittal CT clearly shows the anterior (C, arrow) and posterior plaques (D, arrow).
Calcified unilateral pleural thickening is usually secondary to previous TB or pyogenic infection. The appearance is typical, with thickened pleura rind and linear calcification at the inner border. Sometimes the apparent pleural thickening is not real, but instead, due to expanded extrapleural fat (Fig. 7).

Fig. 7
Fig. 7 (above): chronic pleural thickening with calcification (A, arrow). The apparent pleural thickening in the left apex is due to expanded pleural fat (B, arrow).
In about 15% of patients with chronic pleural thickening, CT discovers persistent effusion between the two pleural layers. In these cases, lowering of defences may convert a quiescent infection into an active one. The fluid may bore its way into the lung, resulting in a bronchopleural fistula (Fig. 8), or drain towards the chest wall, causing a wall abscess, the so-called empyema necessitatis (Fig. 9).

Fig. 8
Fig. 8 (above): chronic calcified pleural thickening (A, arrows), which develops an air-fluid level (B, arrow) two years later. CT confirms the calcified pleural layers and the air-fluid level (C, arrow). This is a characteristic appearance of bronchopleural fistula.
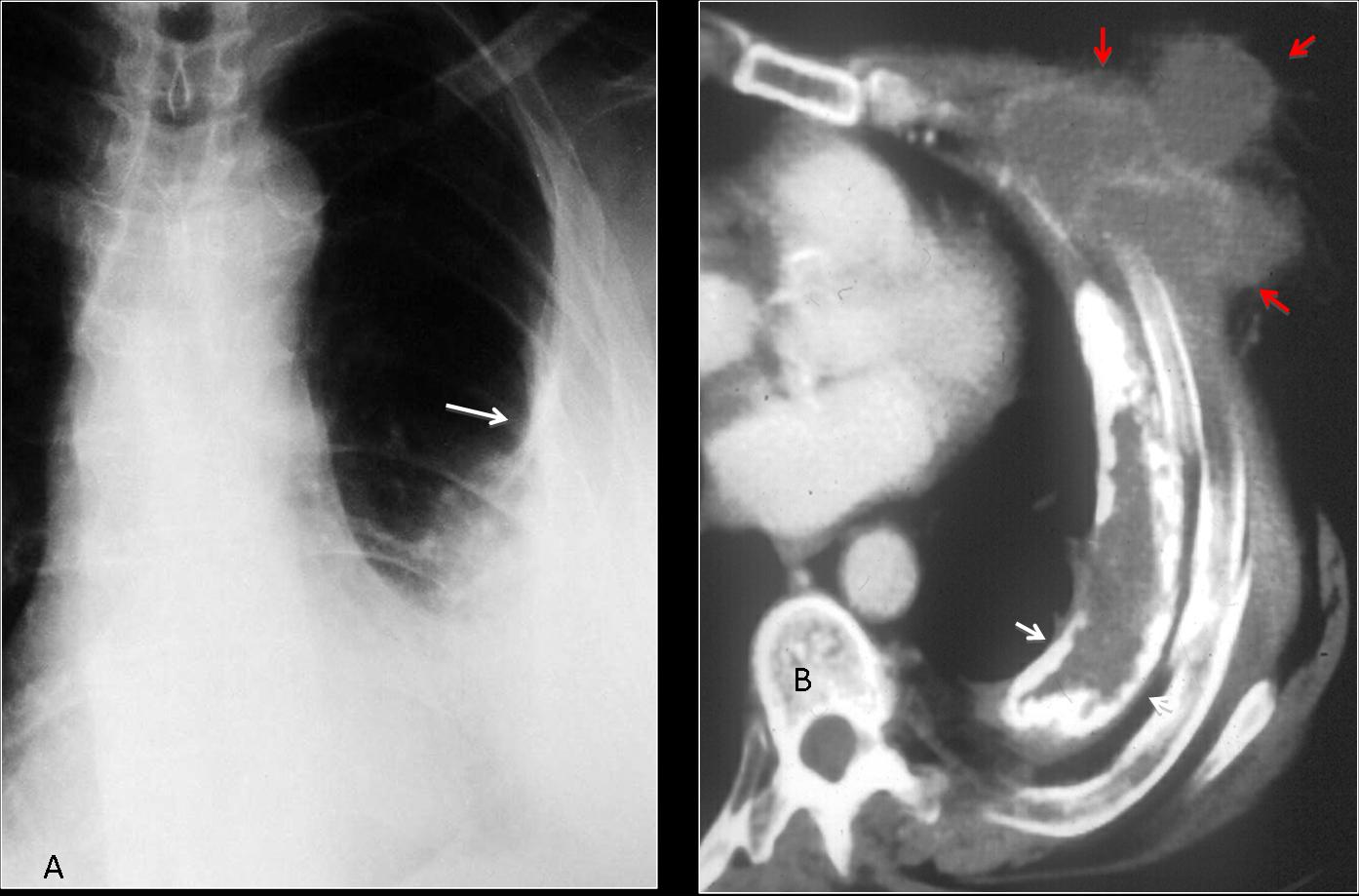
Fig. 9
Fig. 9 (above): patient with old TB calcified empyema (A, arrow) who developed a chest mass. CT shows fluid between the calcified pleural layers (B, white arrows) and a fluid-filled collection in the chest wall (B, red arrows). The appearance is characteristic of empyema necessitatis.
An uncommon complication of chronic pleural disease is the development of malignant neoplasm associated with the long-standing inflammatory process. Patients complain of chest pain and develop a chest wall mass, not unlike empyema necessitatis. CT demonstrates a solid mass affecting the pleura and invading the soft tissues of the chest wall (Fig. 10).
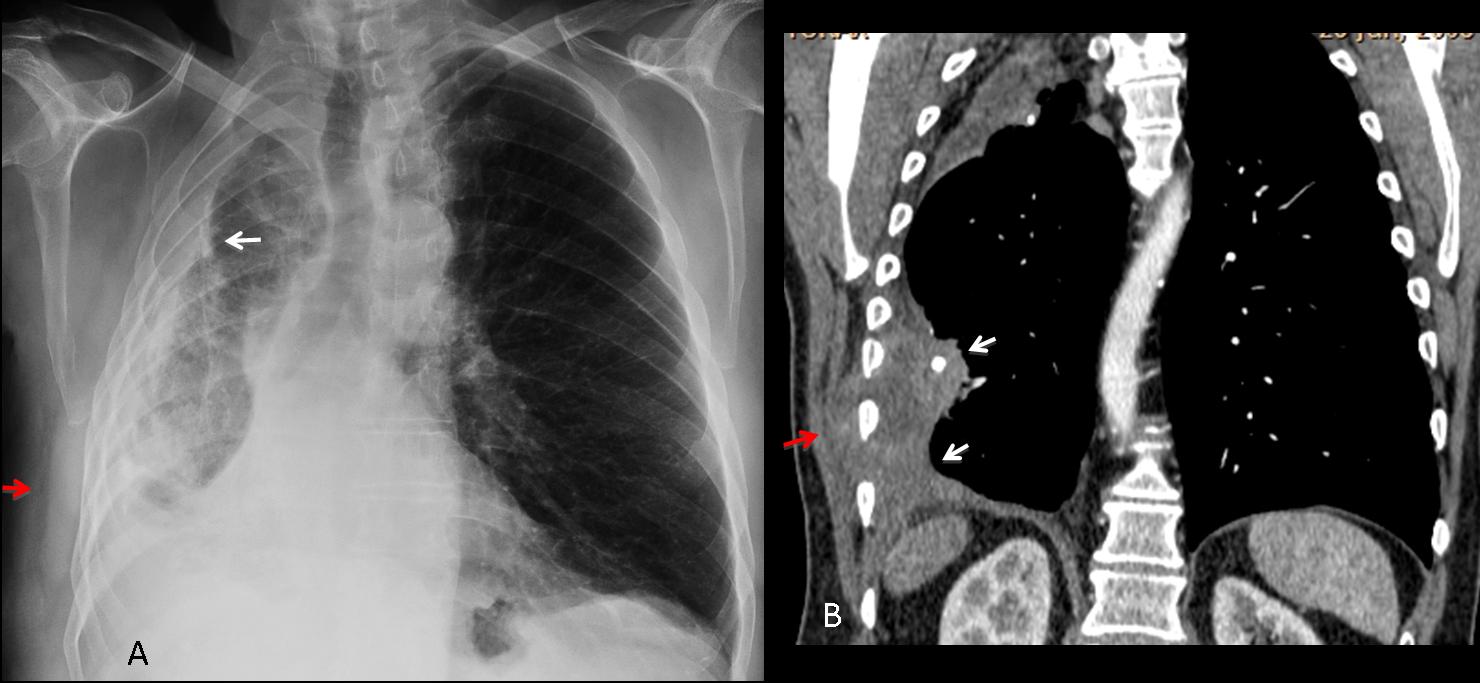
Fig. 10
Fig. 10 (above): 72-year-old old man with old TB and chronic pleural thickening who developed chest pain and a mass in the right chest wall. The chest film shows the calcified pleural thickening (A, white arrow) and a possible chest wall mass (A, red arrow). CT confirms the mass (B, red arrow) and the solid tumour component (B, arrows). Diagnosis: lymphoma.
A possible pitfall of calcified pleura is previous talc pleurodesis in which high-attenuation areas may simulate pleural calcification on CT. The plain radiograph does not show calcium-like opacities (Fig. 11).
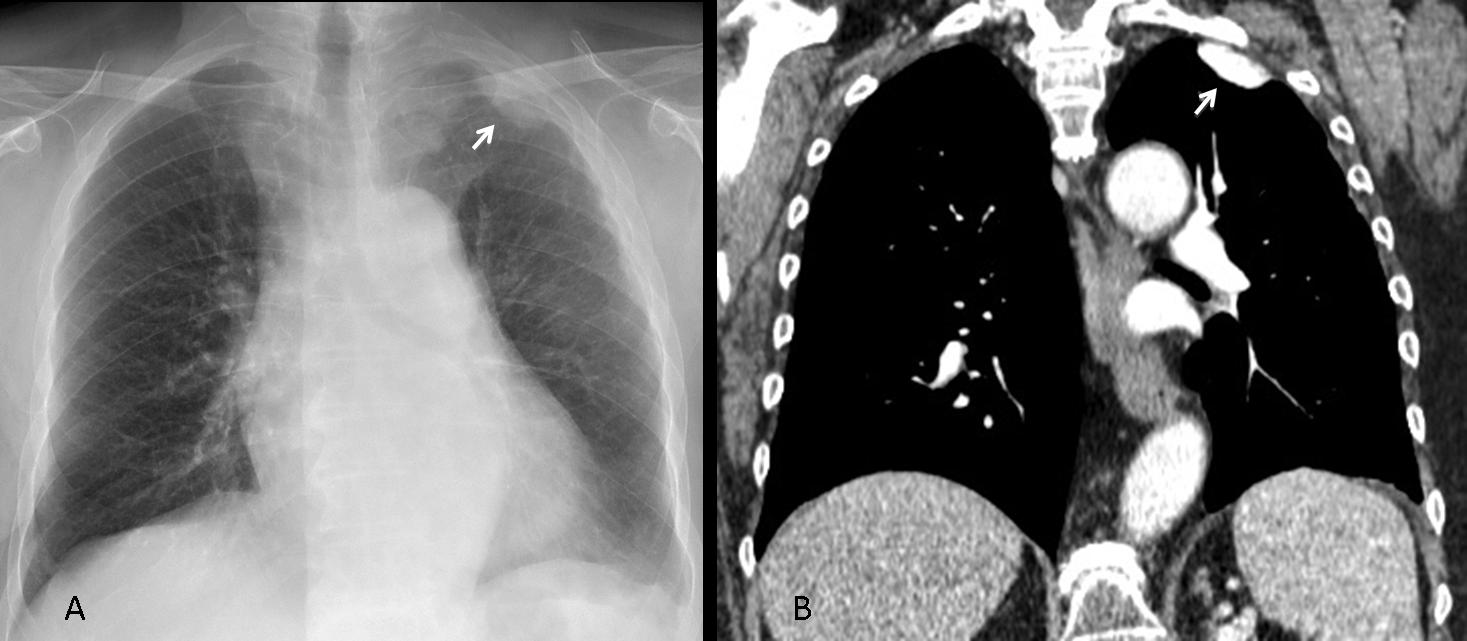
Fig. 11
Fig. 11 (above): 62-year-old man who underwent talc pleurodesis for recurrent pleural effusion. The PA radiograph shows a non-calcified pleural talc collection (A, arrow), with high attenuation on CT (B, arrow).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
1. Bilateral pleural calcifications indicate previous asbestos exposure.
2. Malignant mesothelioma has a strong connection with asbestos exposure.
3. Isolated calcified plaques are innocuous and should not be confused with pulmonary infiltrates.
4. Complications of chronic pleural thickening include broncho-pleural fistula, empyema necessitatis, and malignant tumours.


4.
Calcified chondrocostal cartilagues
Calcificazione di alcune coste anteriori con iperostosi. Metastasi scheletriche?
I think is Calcified metastases
costal cartilage calcifications ?
At least one of them is offside the rib. This goes against your diagnosis
At least one of them is offside the rib. This goes against your diagnosis
there is correlation with carcinoid tumor?
If I say no, you would eliminate option #3. And if I say yes, you will choose it.
My option: not saying a word.
What about chondroid tumors? (multiple enchondromas(maffucci)? chondroblastomas?) I believe there is matrix calcifications.
Interesting diagnosis, but not the right one
Besides lesions mentioned before it seems to me there is widening of upper mediastinum seen on PA view (eg. above aortic arch in left paratracheal region convex contour).
If metastases are excluded , could it be neurofibromatosis?
I believe calcification excludes neurofibromatosis
Carcinoid skin metastasis ?
Try the KISS method. What is calcified and close to the wall?
Pleural calcifications?
Yes
Pleural metastases (carcinoid or other malignancy) or pleural plaques.
…in LL sembrano osservarsi delle alterazioni destruenti a carico dello sterno con reazione periostiosica….potrebbe essere un tumore dello sterno con metastasi pleuriche….
….noduli silicotici…..
….e noduli “silicotici” non poteva essere la risposta giusta?Solo l’anamnesi, in questo caso, poteva determinarne la esatta etiologia….
Sorry, my friend. Silicotic nodules are widespread, smaller and do not cling to the periphery. Do not feel bad. The problem cases are just an excuse to discuss (and, hopefully, teach an specific pattern).
It is not at all neurofibromatosis it’s just a simple pleural calcification. easy dr.pepe send some tough diagnosis.
For tough ones you have to go Cacere’s corner. I haven’t seen you there.