Dr. Pepe’s Diploma Casebook: Case 57 – SOLVED!
Dear Friends,
This week we are presenting radiography of a 64-year-old man with dyspea. Examin the images below, leave your thoughts and diagnosis in the comments section, and come back on Friday for the answer.
Diagnosis:
1. Mediastinal mass
2. Pulmonary nodule
3. Aortic aneurysm
4. None of the above


Findings: chest radiographs show a small bulge in the aortic contour in the PA film (Fig. 1A, arrow) and a nodular lesion in the lateral film (Fig. 1B, arrow). These features are suggestive of an extrapulmonary lesion.
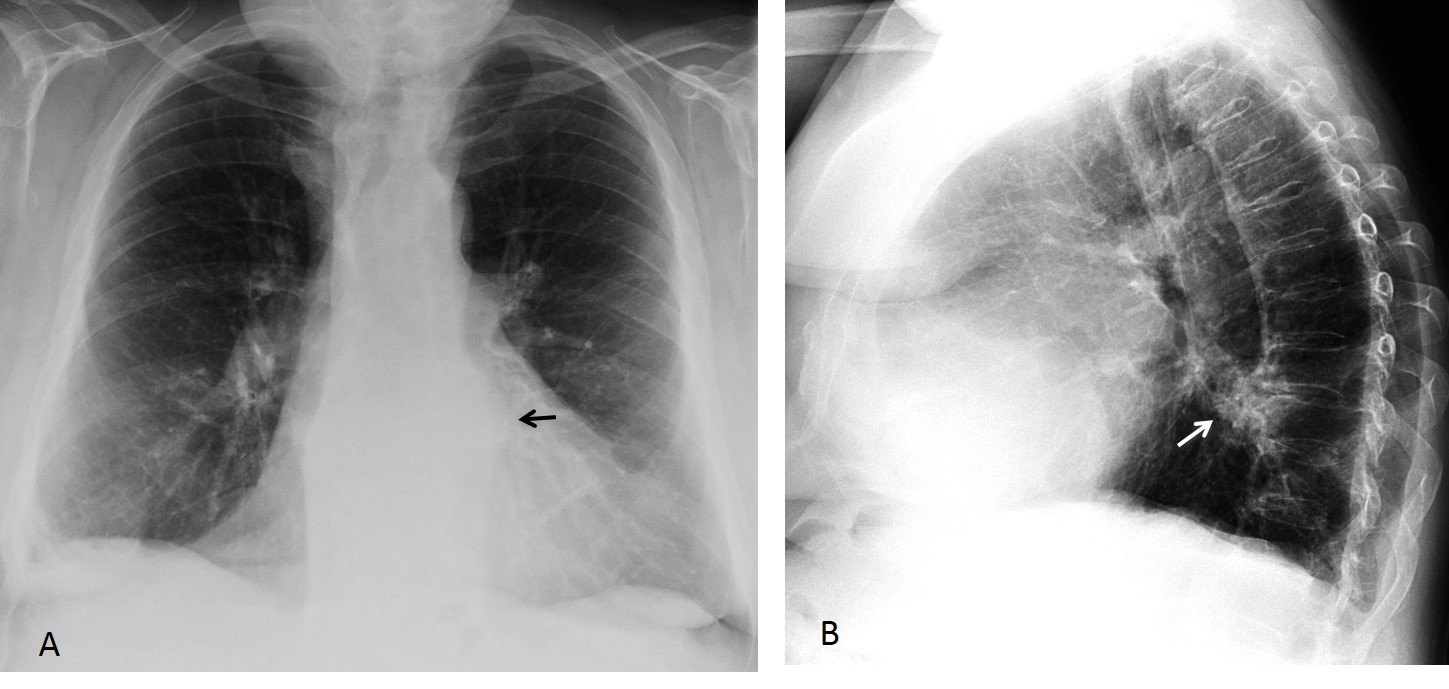
Fig. 1
Sagittal and coronal CT images show that the lesion corresponds to a large osteophyte. There is a vacuum phenomenon at the intervertebral space, which is not narrowed. Note how the osteophyte displaces the paraspinal line (Fig. 2A, arrow) and displaces the aorta forward in the sagittal view (Fig. 2B, arrow).
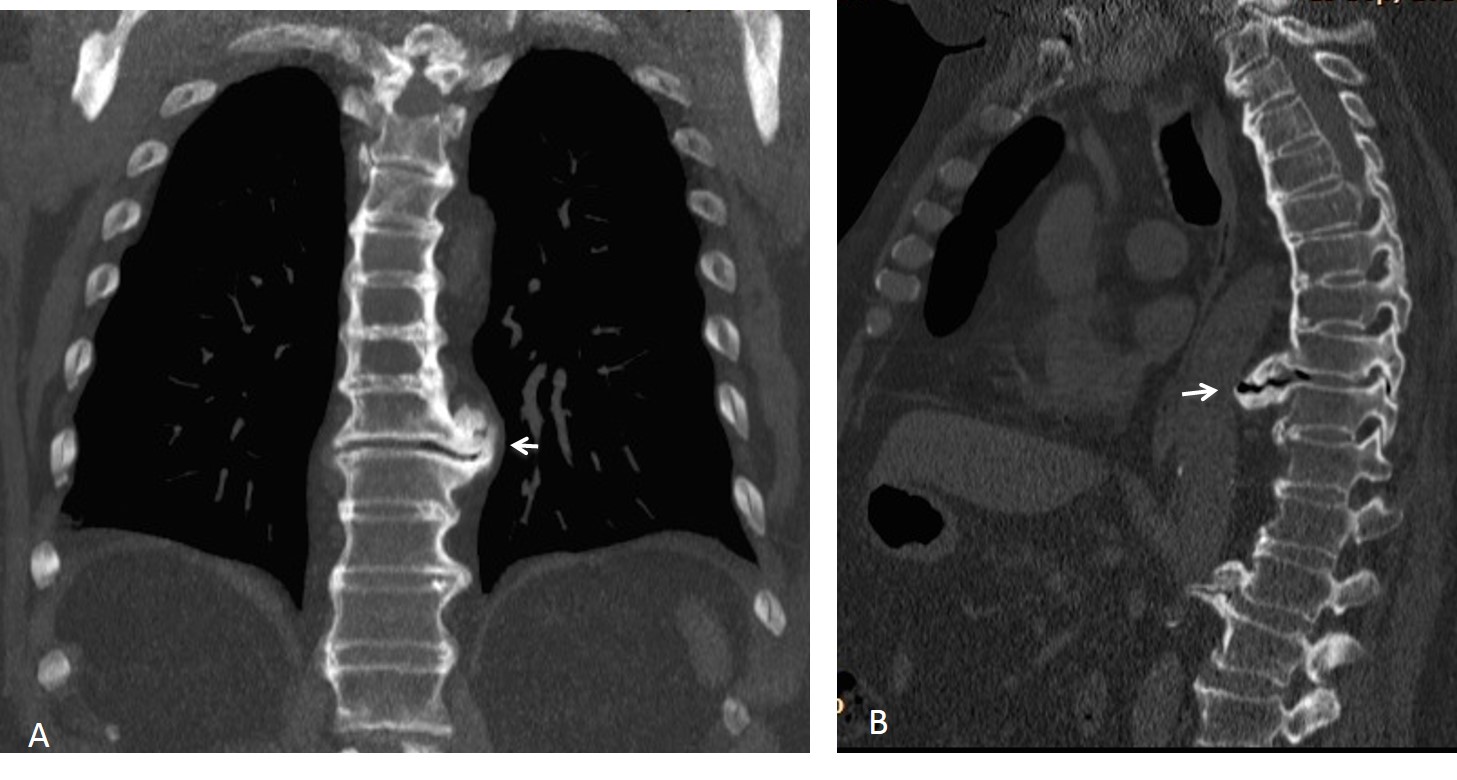
Fig. 2
Final diagnosis: large osteophyte simulating mediastinal/lung disease.
In this presentation I would like to discuss common conditions of the thoracic skeleton that can simulate chest diseases. Since the chest radiograph is a 2D representation of a 3D structure and the thoracic cage encircles the inner viscera, bone changes may be superimposed on the viscera and simulate a lung or mediastinal process, as in the case shown.
Osteophytes are one of the most common pathologies of the dorsal spine. Single osteophytes can simulate a lung nodule in the lateral view. Awareness of this fact may suggest the correct diagnosis, which is easily confirmed by comparison with previous films (Fig. 3). When in doubt, CT can be performed, although it should be unnecessary in most cases.
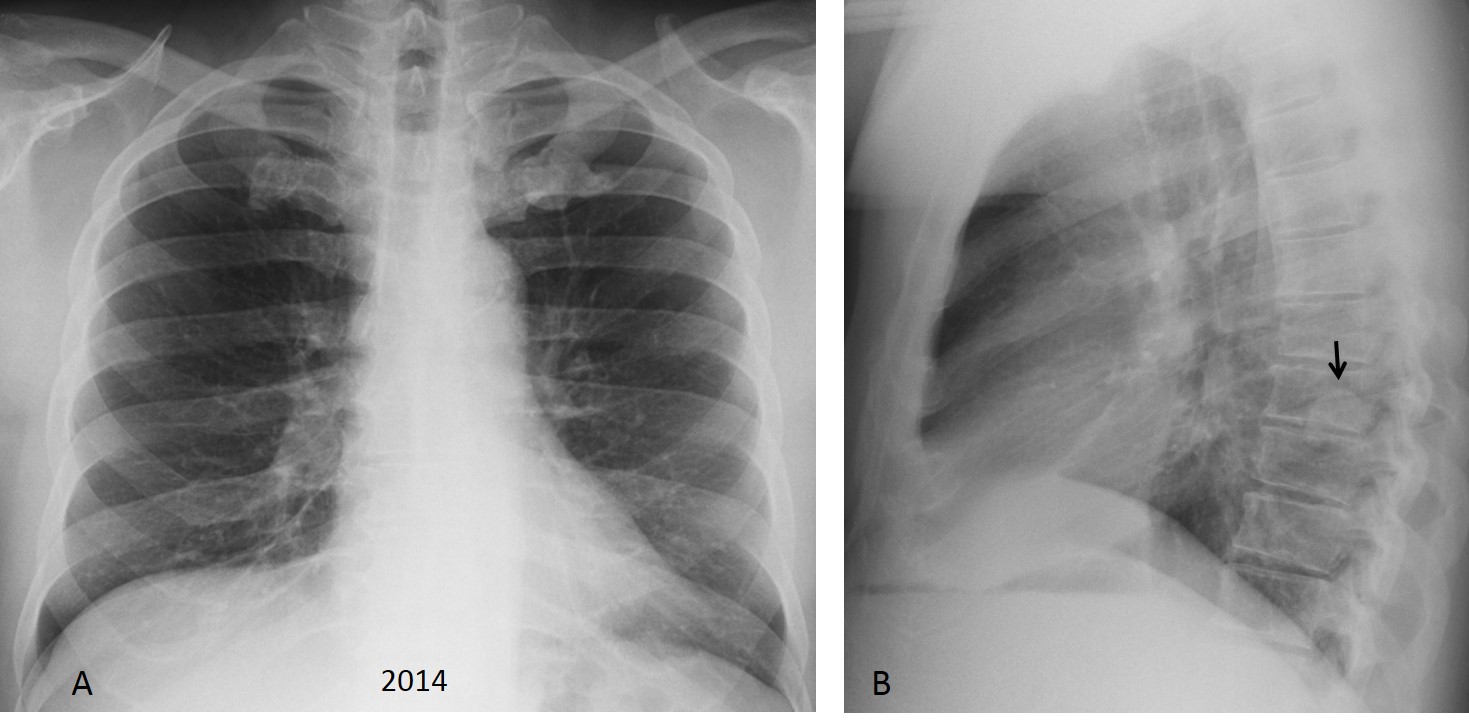
Fig. 3
Fig. 3 (above): 65-year-old man with a single large osteophyte that simulates a pulmonary nodule in the lateral view (B, arrow).
Comparison with a previous film taken four years earlier shows that the appearance of the nodule has not changed (Fig. 4A, arrow). Sagittal and coronal CT at that time confirmed the large osteophyte (B,C, arrows).
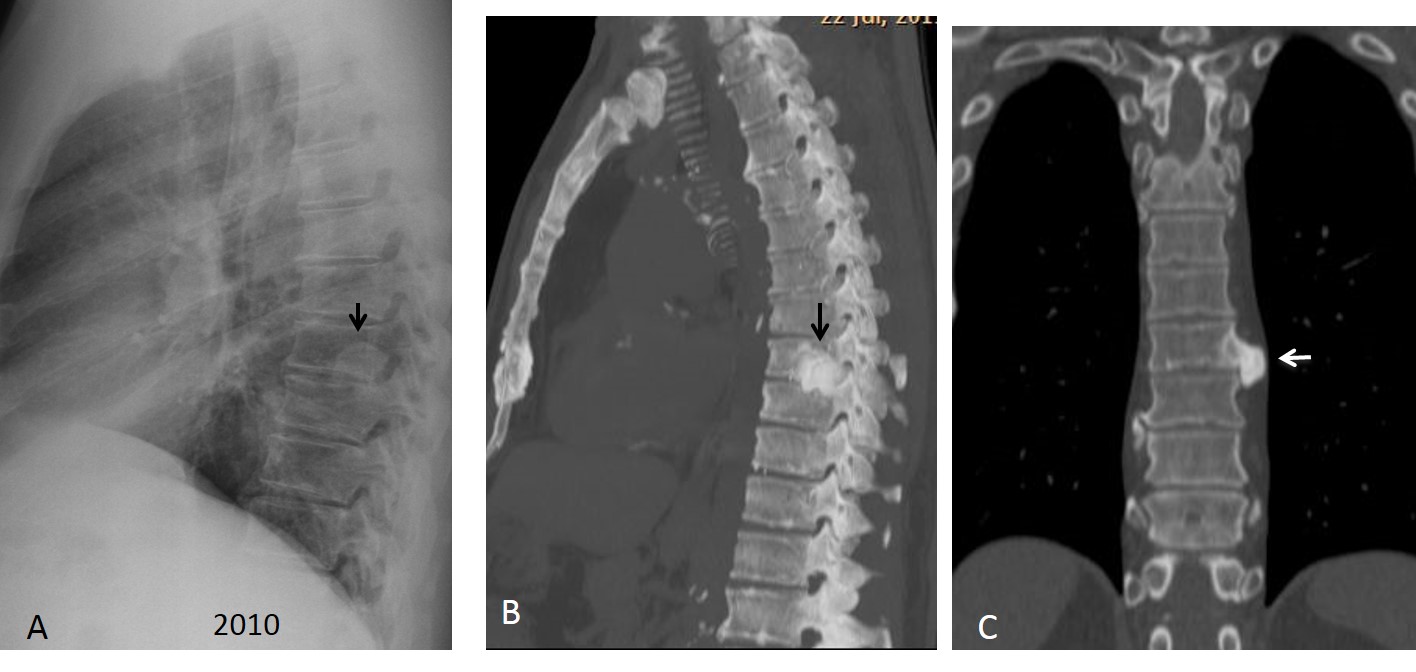
Fig. 4
Asymmetrical exuberant calcification of the first costal cartilage can also simulate a lung nodule in the PA chest film. These calcifications are fairly common in elderly people and can be recognised by their increased opacity and proximity to the costochondral area. Comparison with previous films will confirm the diagnosis (Fig. 5) . If they are not available, CT will clarify the findings (Fig. 6).
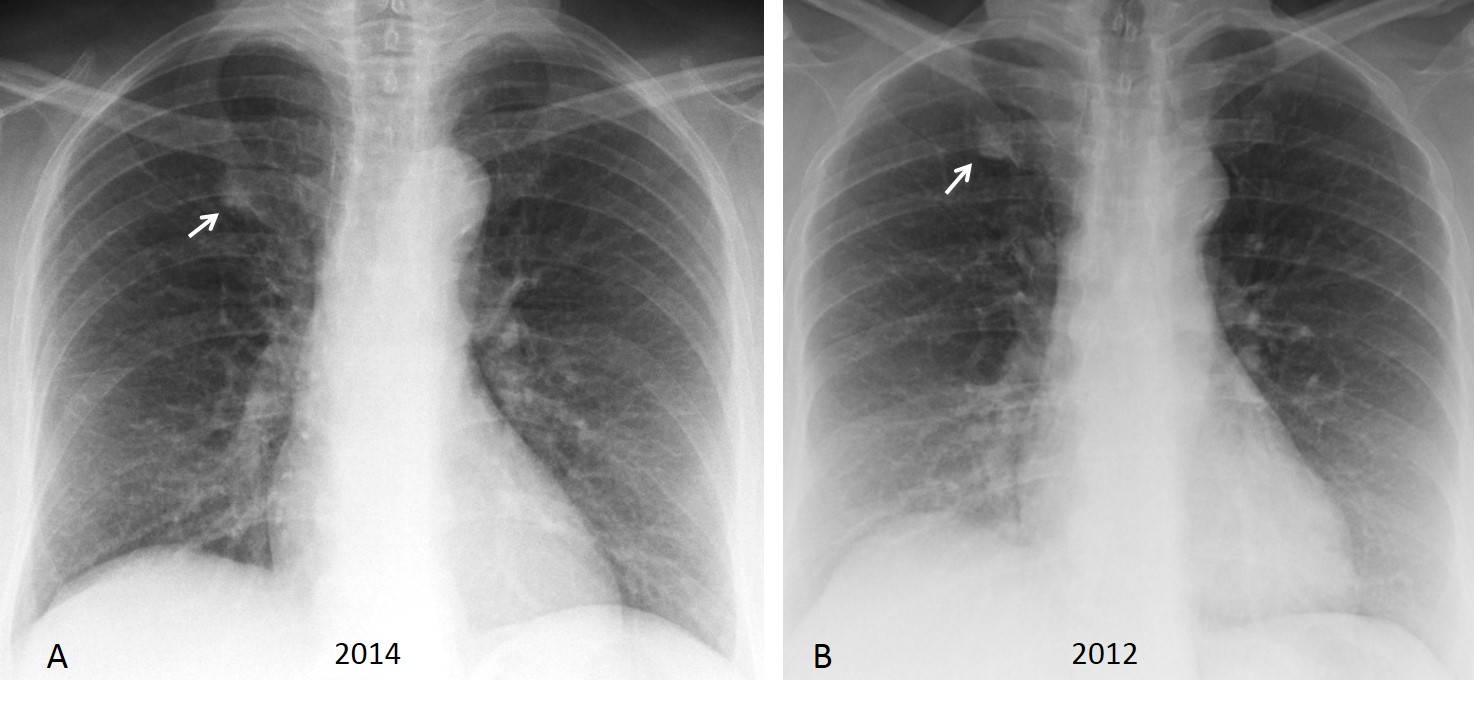
Fig. 5
Fig. 5 (above): 55-year-old man with an asymmetrical calcified first cartilage simulating a pulmonary nodule (A, arrow). Comparison with a film taken two years earlier shows no changes (B, arrow).
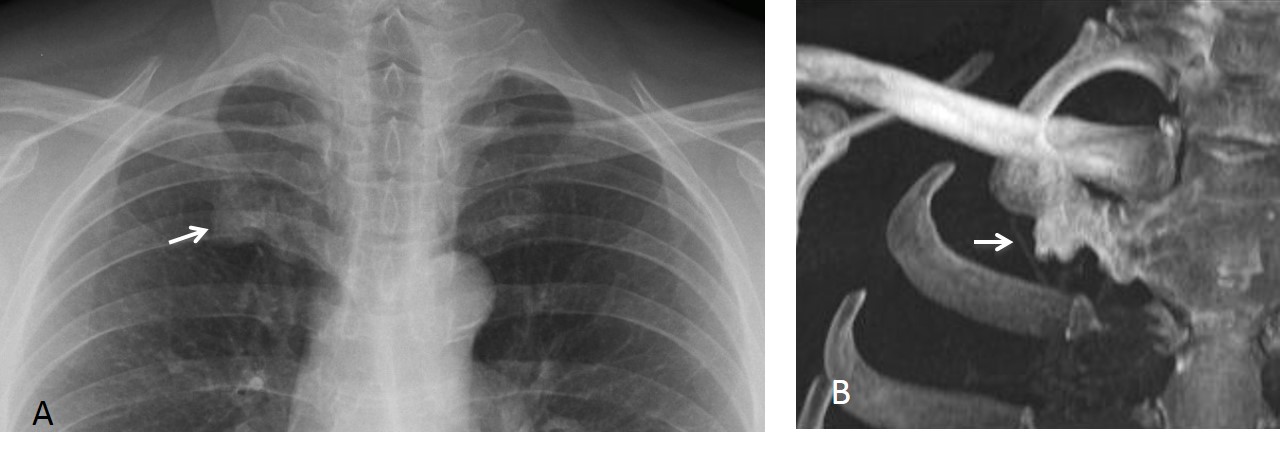
Fig. 6
Fig. 6 (above): 45-year-old man with calcified first costal cartilage simulating a lung nodule (A, arrow). No previous films available. CT confirms the findings (B, arrow).
Rib fractures are a common cause of false pulmonary nodules. They are often multiple and easily identifiable in the PA view (Fig. 7). They may pose problems when the callus is single and hypertrophic (Fig. 8). The diagnosis is easily made by eliciting a history of previous trauma.
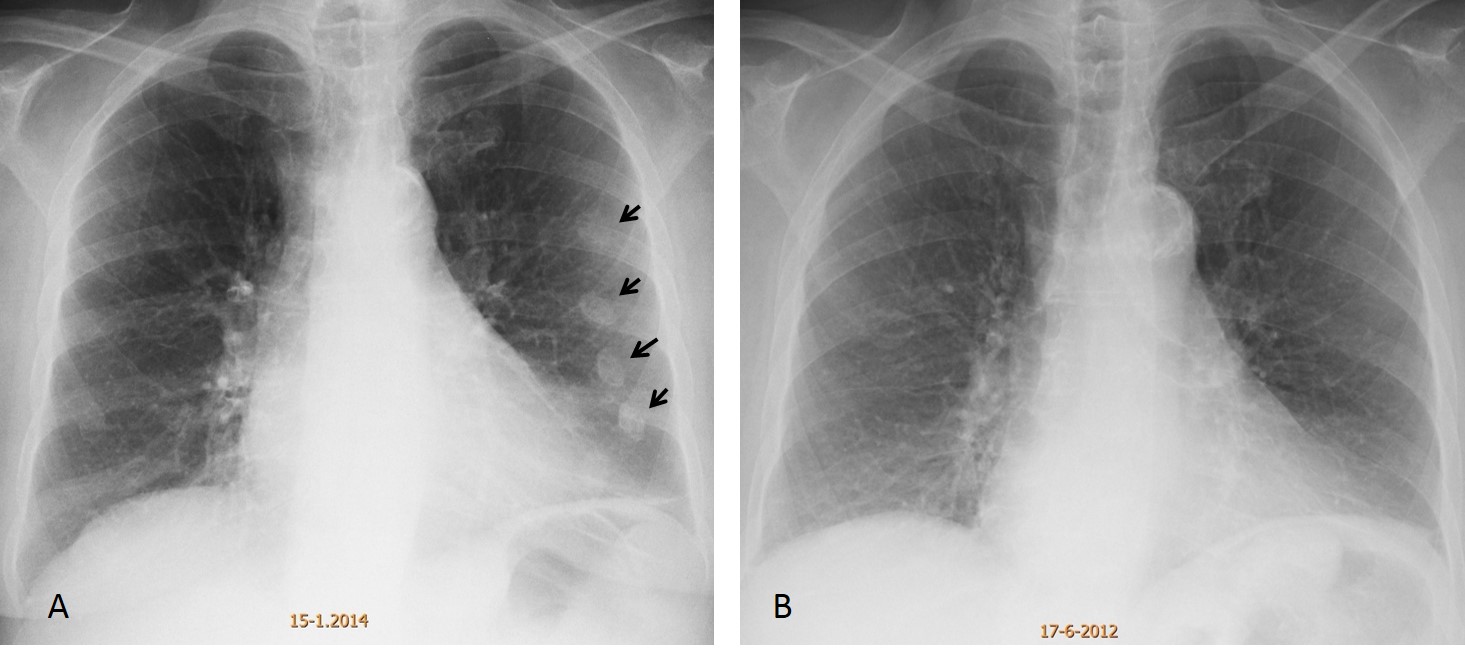
Fig. 7
Fig. 7 (above): 62-year-old woman with several rib fractures, which, at first glance, simulate pulmonary nodules (A, arrows). PA chest film two years earlier (B) did not show the fractures. She was in a car accident during the intervening years.
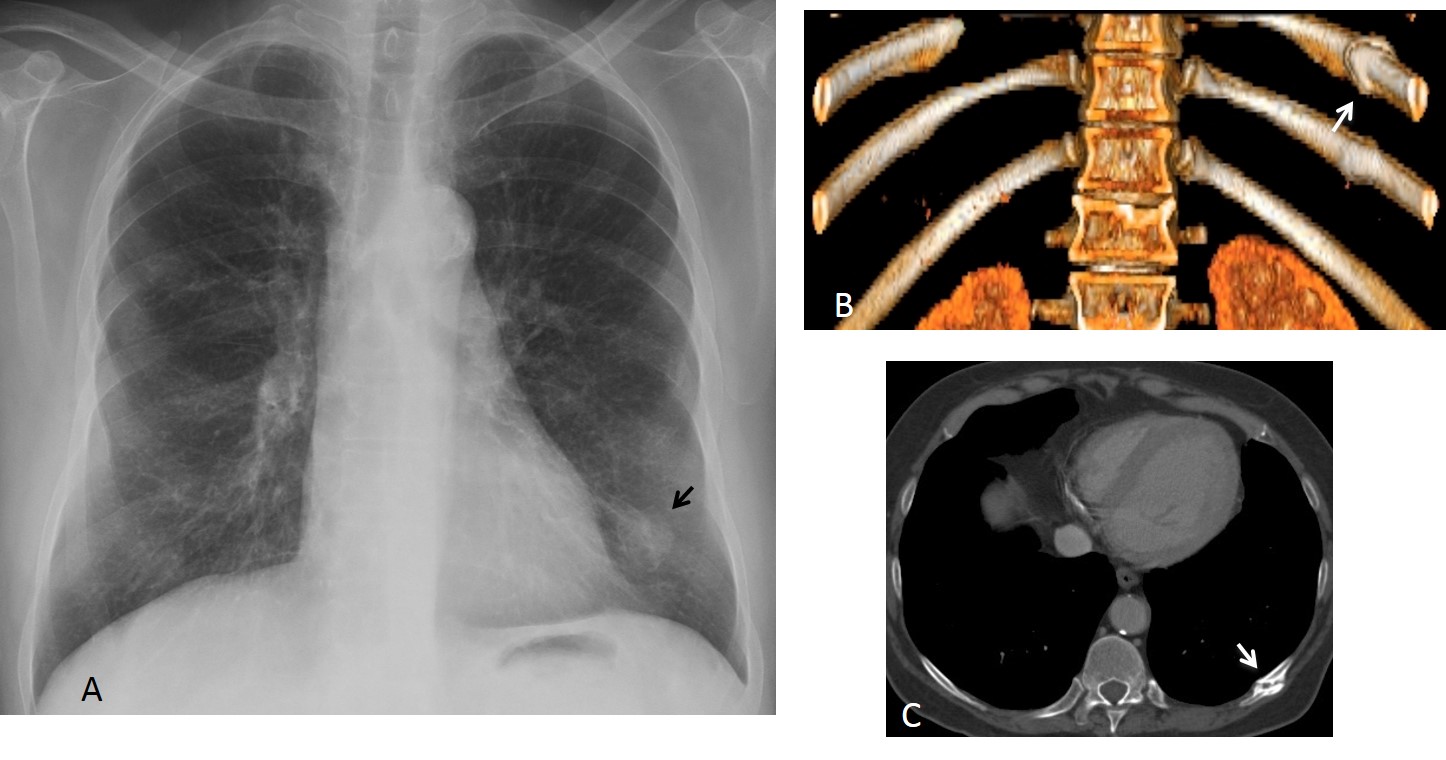
Fig. 8
Fig. 8 (above): 62-year-old male smoker with renal carcinoma. Pre-op radiograph discovered a LLL nodule (A, arrow) that was not visible 3 years before. CT shows a non-consolidated fracture of the 10th left rib (B,C, arrows). There is also an old fracture of the 11th rib.
Iatrogenic fractures of the ribs occur in 3% to 16% of patients undergoing median sternotomy. These patients lack a history of trauma and the resulting callus may create diagnostic problems, unless we are aware of this fact.
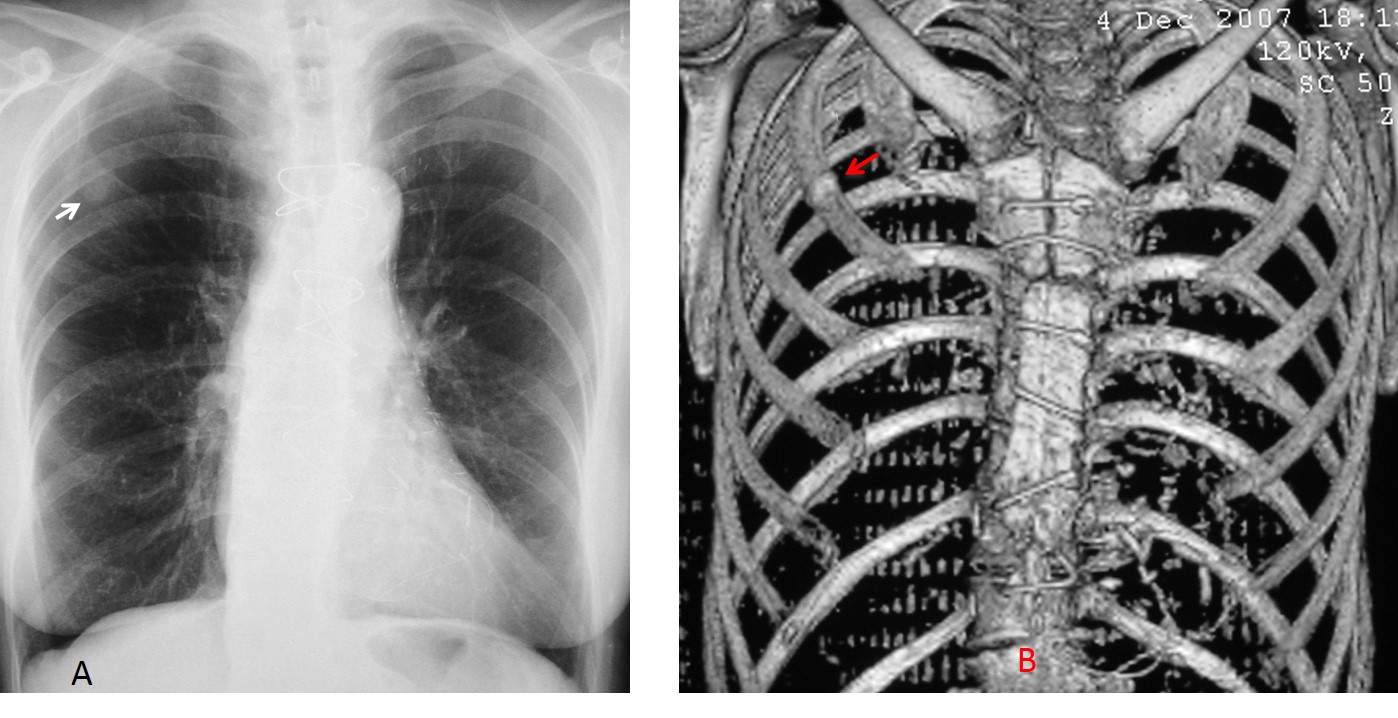
Fig. 9
Fig. 9 (above): 65-year-old female smoker one year after coronary surgery. Follow-up radiograph shows a nodule in the RUL (A, arrow) that was not visible in the pre-op film. CT confirms that the nodule represents a iatrogenic fracture of the second right rib (B, arrow).
Bone islands are benign sclerotic bone lesions with a predilection for the pelvis, long bones, spine, and ribs. In this last location, they can simulate a pulmonary nodule (Fig. 10). Comparison with previous films and careful observation will demonstrate the location of a bone island within the rib. CT study resolves inconclusive cases.
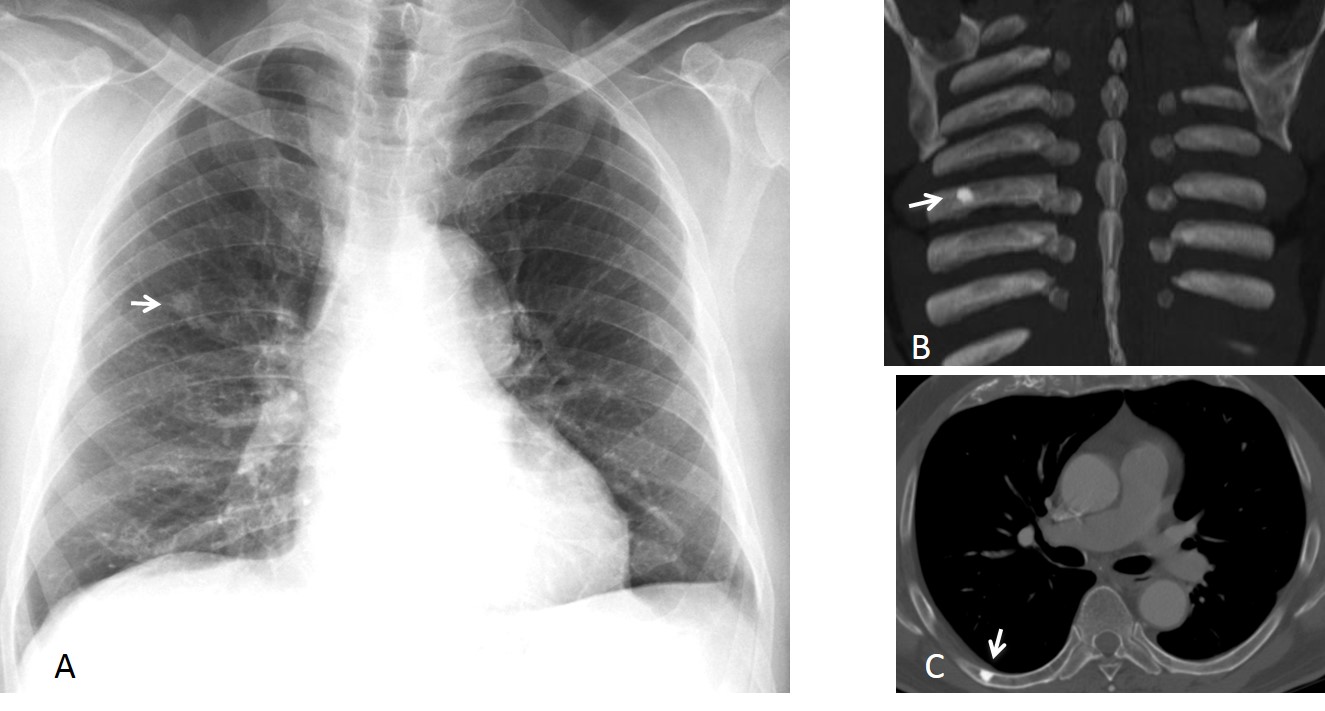
Fig. 10
Fig. 10 (above): 65-year-old man, asymptomatic. A small nodule (A, arrow) was discovered in a routine examination. CT demonstrates that the nodule corresponds to a bone island of the right 7th rib (B,C arrows).
Normal bone variants may impinge on the underlying viscera and cause an abnormal appearance, simulating disease. The most common one is pectus excavatum, which occurs in less than 1% of the population. It narrows the AP diameter of the chest, displacing the heart towards the left side and causing blurring of the right heart border, simulating RML disease. (Fig. 11). Extreme cases of pectus excavatum markedly displace the heart towards the left, simulating cardiomegaly (Fig. 12). A lateral film confirms the displaced sternum and excludes other pathology.
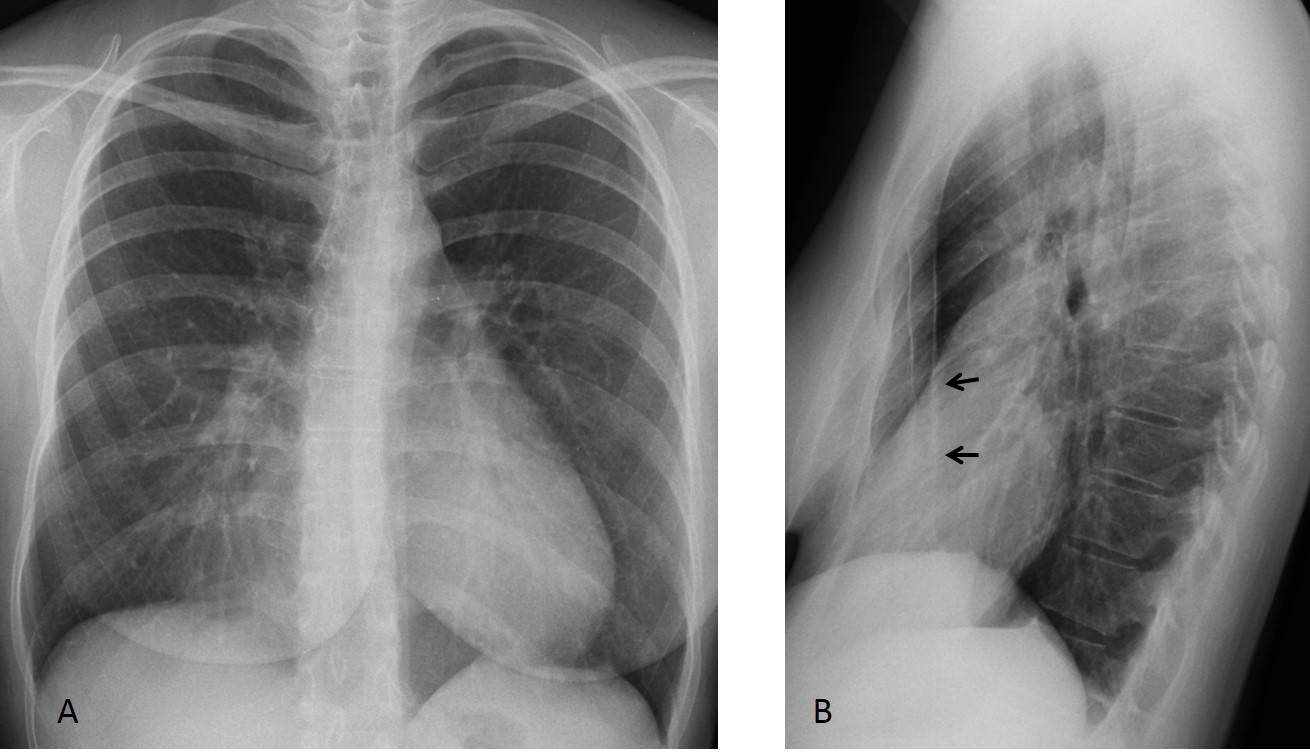
Fig. 11
Fig. 11 (above): 22-year-old woman, asymptomatic. PA chest film shows blurring of the right heart border, which raises the possibility of RML disease. The lateral film shows an obvious pectus excavatum (B, arrows). No RML disease is seen.
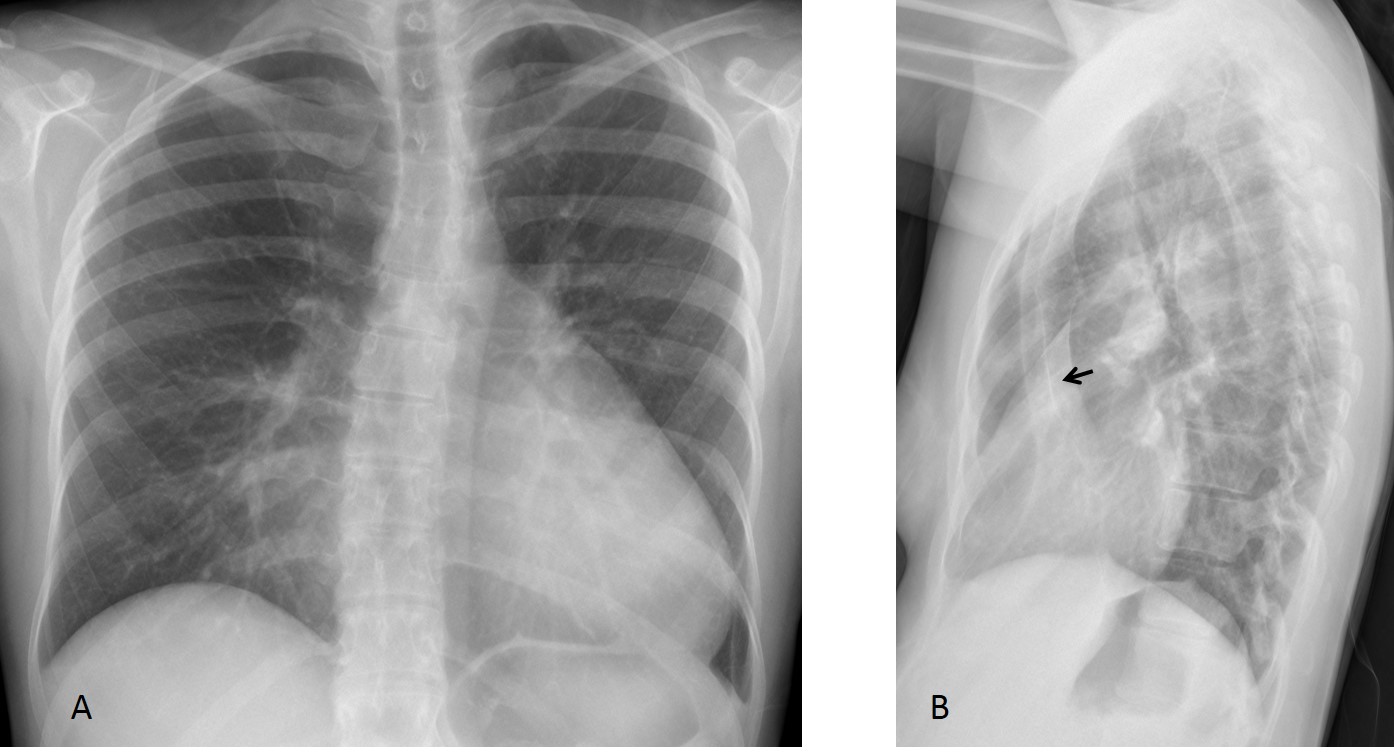
Fig. 12
Fig. 12 (above): 18-year-old male with dyspnea. PA radiograph shows an apparently enlarged heart. The lateral view demonstrates pectus excavatum (B, arrows). Axial and sagittal CT show marked narrowing of the AP chest diameter and displacement of the heart towards the left (Fig. 13 A,B, arrows).
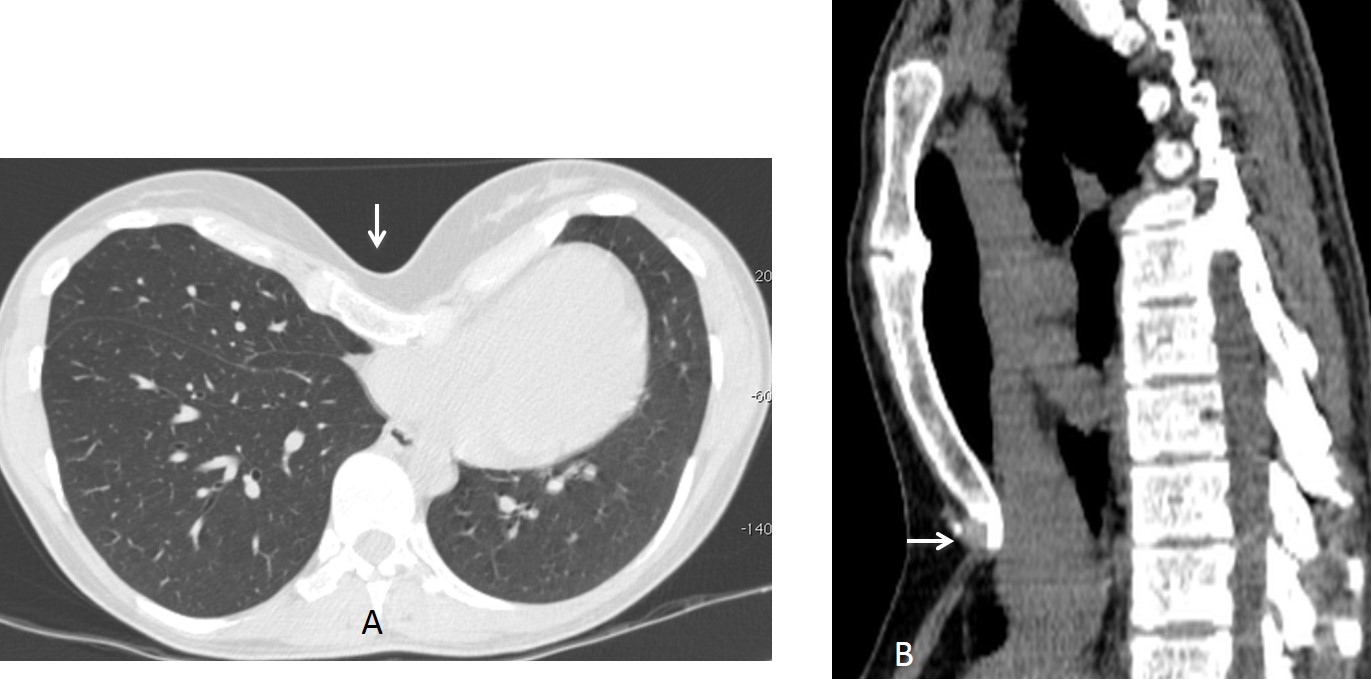
Fig. 13

Follow Dr. Pepe’s advice
Follow Dr.Pepe’s Advice:
1. Asymmetric calcifications of the first costal cartilage and solitary osteophytes may simulate pulmonary nodules in the PA and lateral chest film, respectively.
2. Rib bone islands may also simulate pulmonary nodules in the PA view.
3. Pectus excavatum may simulate RML disease and/or cardiomegaly.


I see a superior mediastinal opacity that fad out into the neck and attenuates the tracheal air column…retrosternal goiter. Also a well defined pulmonary nodule is seen in the right lower lobe so metastatic thyroid mass is considered
None of the above
Right hemitorax-in mediobasal segment seen consolidation
Rheumatoid factor (RF)is normal?
As far as I know, yes. Any ideas?
he has gynaecomastia?
sorry no gyneacomastia i mean Infertility
No. What are thinking?
I can clearly determine round opacity in LLL, I can also speculate that there are round masses behind a trachea. So, enlarged lymph nodes in the mediastinum suspected and CT indicated.
DDS: Lymphoma? Sarcoidosis? Metastasis?
Where are the usual suspects? I miss you all
….opacità omogenea dell’angolo cardio-frenico di dx, che “maschera”il margine cardiaco inferiore( segno della “silhoutte”) indicante una patologia del lobo medio, come si vede in LL….tale opacità è compatibile con atelettasia del lobo….una immagine nodulare si vede in LL a livello del bronco lobo medio…. modicamente sollevata la cupola diaframmatica omolaterale … come reperto collaterale gozzo “plongeant” in alto a dx….
Is this patient under corticosteroid therapy?
PTH levels are ok?
No corticosteroid therapy. PTH OK.
Follow the KISS method. Answer is simple.
We have a fat man with pericardial fat, with lower lung zone reticular pattern (fibrosis), pleural thickening on pulmonary base,and nodular opacities at the carinal level.
Osteoporotic bones and ossification of the anterior longitudinal ligament.
What do you think of the nodular opacity in the lateral view and the bulge of the aortic contour in the PA?
Possible aortic aneurysm of descending aorta.
Actually, there is a lateral displacement of descending aorta. So,no aneurysm. Retropetitoneal mass displacing aorta .
I mean paravertebral mass, my mistake.
Getting closer…
…cisti broncogena….opacità rotodeggiante,a margini netti che impronta e disloca la trachea…. frapponendosi tra trachea ed arco aortico…. l’adiposità del soggetto e del seno mi hanno sviato la diagnosi…scusami….
On profile view at the level of nodular opacity anterior vertebral osteophytes are prominent. Calcified anterior longitudinal ligament is displaced anteriorly. Osteophytes causing pseudolesion sign?
Good! Why it took you so long?
For the last 3 days radiology lectures all day, had to analyze case via mobile phone. 🙂 Next week I am back on my PC. 🙂
widening of the posterior mediastinal shadow at the PA view with prominent both hilar shadows, prevertebral opacity noticed on lateral view, concerning about neoplastic process in such age group for post contrast CT chest correlation
anterior vertebral scalloping; prevertebral mass a middle/posterior mediastin; Aortic Aneurysm?
lymphoma
Could this be ankylosing spondylitis ?