Dr. Pepe’s Diploma Casebook: Case 58 – SOLVED!
Dear Friends,
I am back from vacation and ready for new challenges. Present images belong to a 70-year-old man with cough and fever. Leave your thoughts and dignosis in the comments section and come back on Friday for the answer.
Diagnosis:
1. Carcinoma of the lung
2. Tuberculosis
3. Pneumonia
4. None of the above


Findings: PA chest radiograph shows a typical appearance of RUL collapse, with uniform opacity of the RUL and elevation and convexity of the minor fissure (A, white arrow). The medial aspect of the fissure is convex (A, red arrow), indicating a hilar mass (Golden sign). The lateral view shows convexity of the upper major fissure (B, arrow). There is a right pleural effusion.

Fig. 1
Fig. 2 (below): Enhanced axial CT confirms a large hilar mass (A, arrows). Coronal CT shows the collapsed RUL lobe (B, white arrow) and convexity of the lower minor fissure, secondary to the hilar mass (B, red arrow).
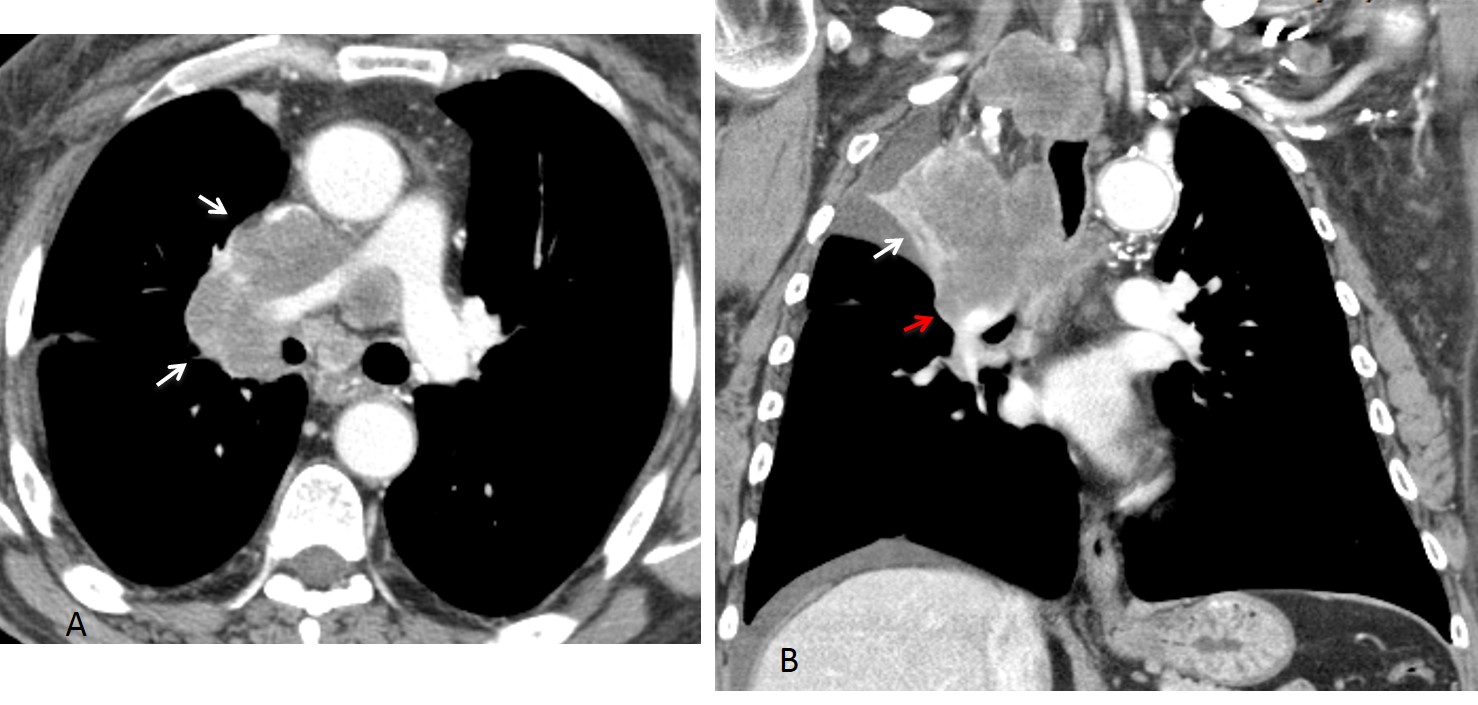
Fig. 2
Final diagnosis: central carcinoma with RUL collapse and Golden sign.
Of all the lung lobes, collapse affecting the right upper lobe is most easily recognised. Considering that RUL collapse is often due to a central carcinoma, it is important to be familiar with the related imaging manifestations to avoid diagnostic and treatment delays. In this presentation, I would like to discuss typical and atypical presentations of RUL collapse.
In the PA view, RUL collapse is typically seen as a triangular shadow in the right upper lung, delimited by an elevated, sharply-defined convex or straight minor fissure (Fig. 3A). Secondary signs, not always present, are right hilum elevation and tracheal deviation.
In the lateral view, the collapsed lobe is delimited by the minor fissure and upper portion of the major fissure (Fig. 3B). In cases of marked collapse, the lateral view is not helpful because the opaque lobe is hidden by the superior mediastinal structures (Fig. 4).
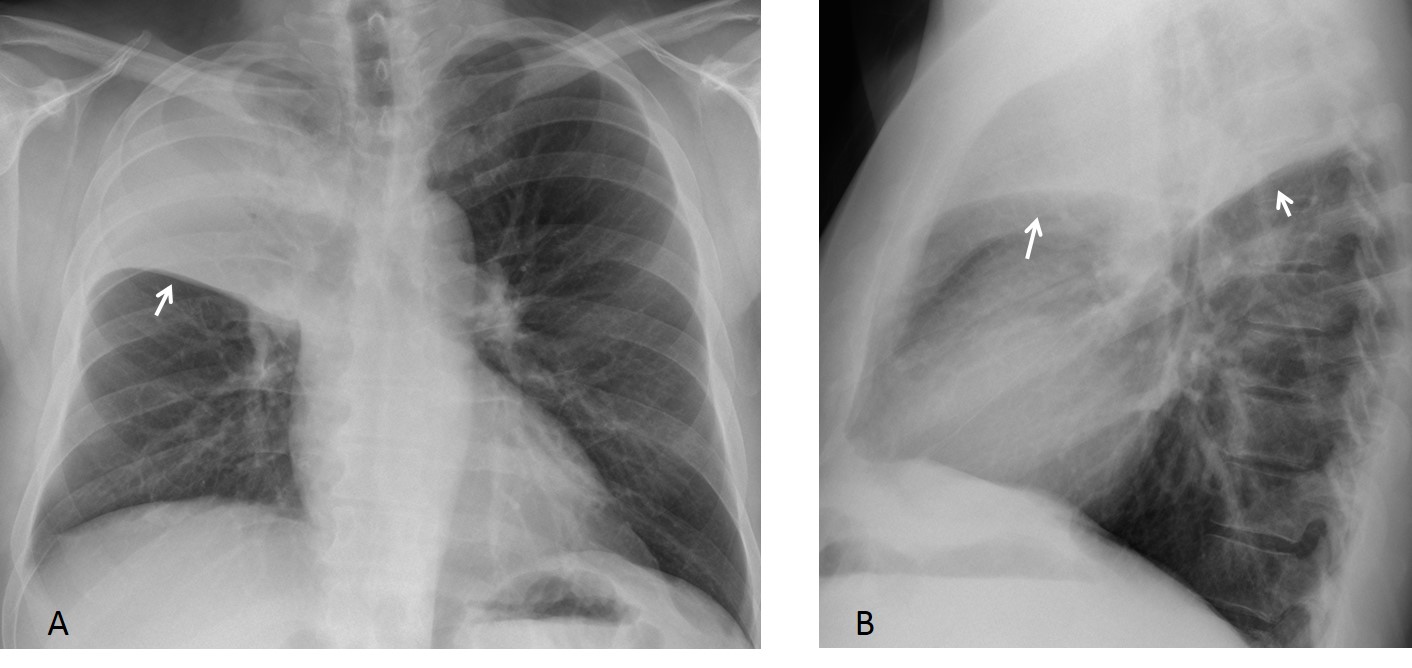
Fig. 3
Fig. 3 (above): typical features of RUL collapse. Note opacity and moderate RUL volume loss, evidenced by elevation of the minor fissure (A,B, arrows). There is no tracheal displacement and the right hilum is slightly elevated. Lateral view shows the triangular shape of the collapsed lobe, delimited by the minor and major fissures (B, arrows).
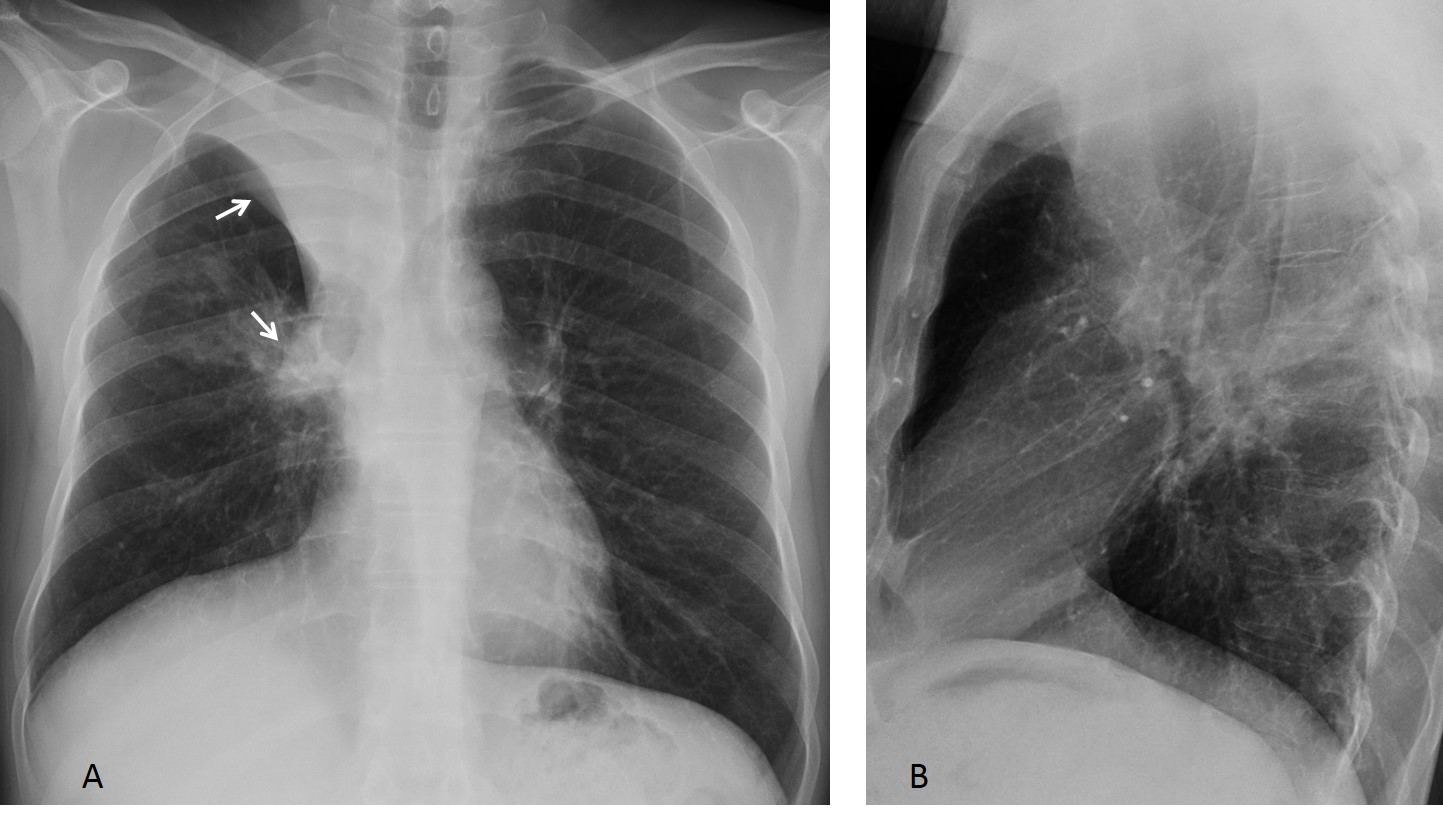
Fig. 4
Fig. 4 (above): moderate RUL collapse with evident volume loss, upward displacement of right hilum (A, arrows), and elevation of right hemidiaphragm to compensate for the volume loss. The lateral view (B) is unremarkable because the opacity of the collapsed lobe is hidden by the mediastinal structures.
The Golden sign is a reliable indication of a hilar mass causing RUL collapse. As was mentioned earlier, this sign is caused by the minor fissure bulging outwards, being pushed medially by the hilar mass. Because of its shape, the Golden sign is also called “reverse S sign” or “Golden S sign” (Figs. 5 and 6).
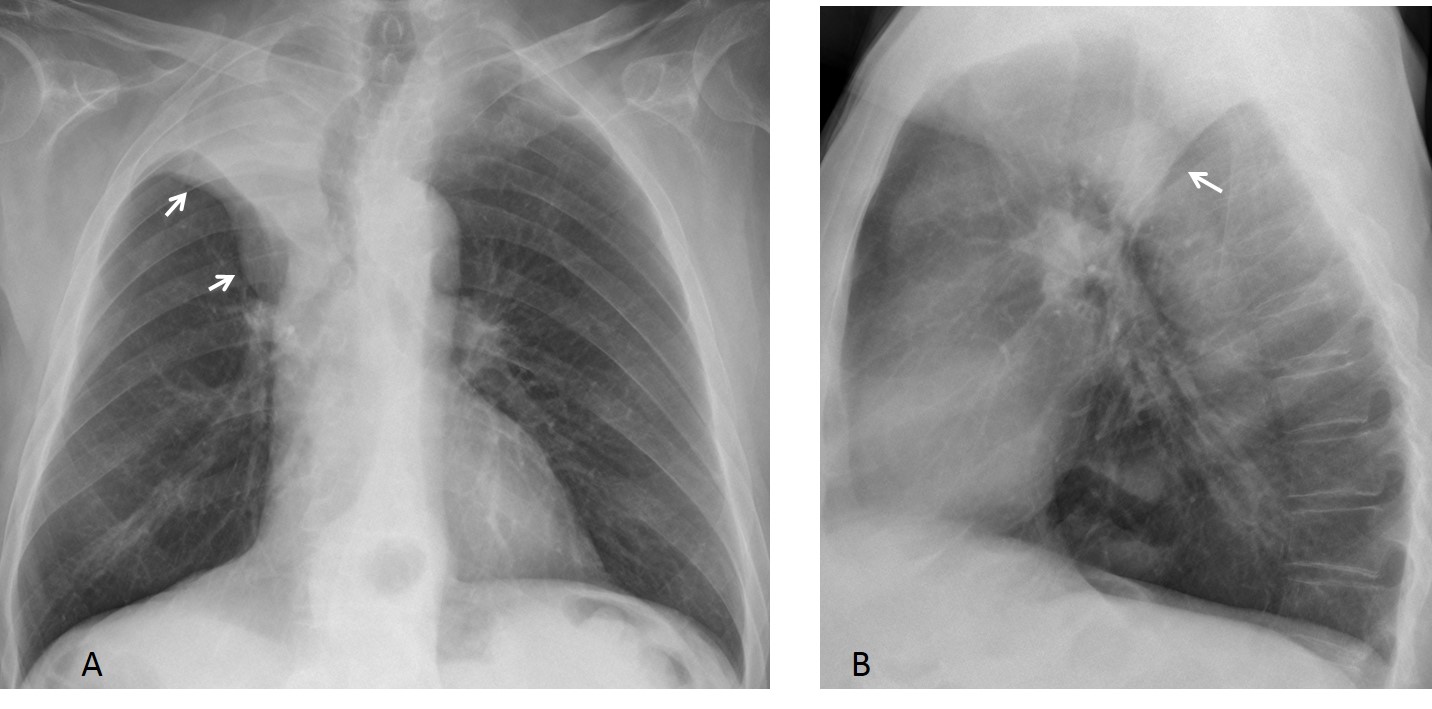
Fig. 5
Fig. 5 (above): carcinoma causing RUL collapse and Golden sign. Note the double curve of the minor fissure, simulating an inverted “S” (A, arrows). The hilum is elevated and the trachea markedly displaced. Convex major fissure in the lateral view (B, arrow).
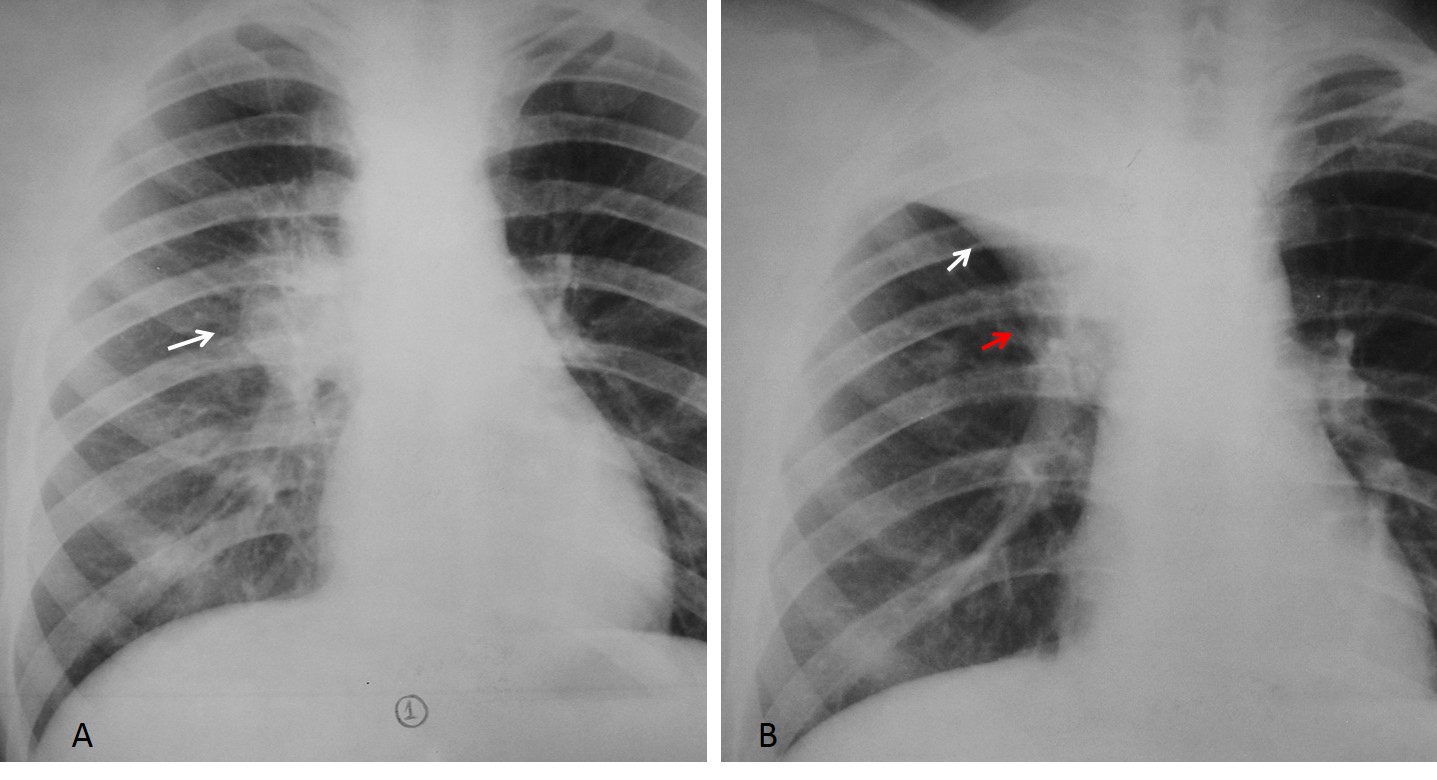
Fig. 6
Fig. 6 (above): primary TB in a 20-year-old male with large hilar lymph nodes (A, arrow). Three weeks later compression on the bronchus has caused RUL collapse (B, white arrow). Lymph nodes are hidden by the opaque lobe and there is bulging of the medial part of the fissure (B, red arrow). This case nicely explains the reverse S sign (Golden sign).
A slowly growing neoplasm permits secretions to accumulate within the lobe, preventing volume loss. This variant has been called drowned lung and it is recognised by the bulging fissures (Fig. 7). This finding has been described in some types of pneumonia, but the most common cause is a bronchus obstructed by malignancy. Bulky tumor masses may give a similar appearance.
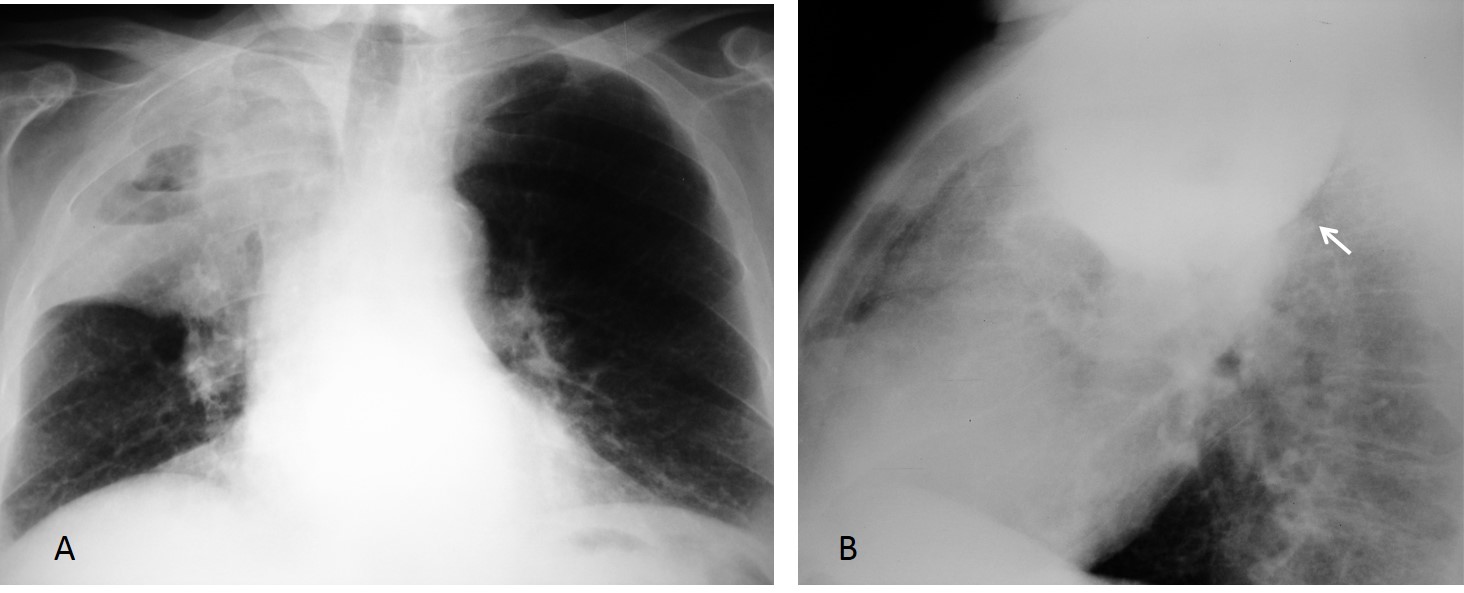
Fig. 7
Fig. 7 (above): 62-year-old man with bronchogenic carcinoma of RUL bronchus. The lobe is full of secretions and shows no volume loss in the PA view (A). In the lateral view, there is bulging of the major fissure (B, arrow). There is cavitation inside the lobe.
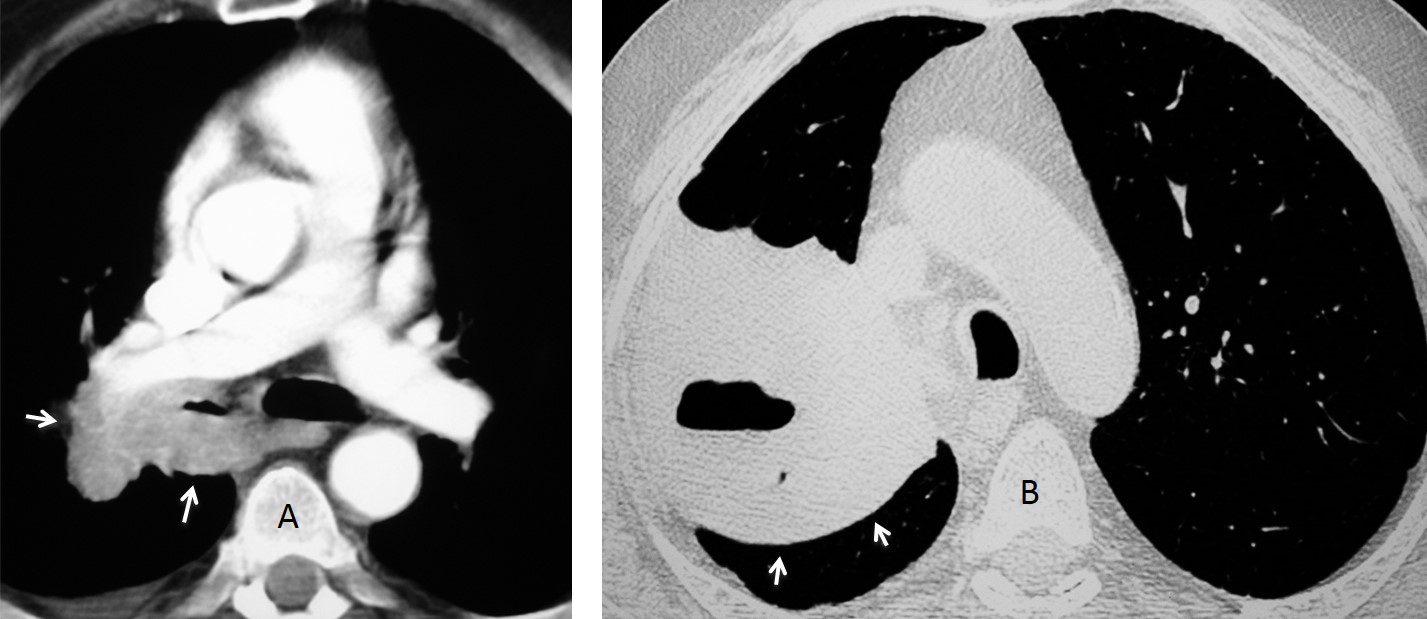
Fig. 8
Fig. 8 (above): enhanced CT of the same patient shows a tumoral mass in the right hilum, narrowing the RUL bronchus (A, arrows). A cephalad view shows opacification and cavitation of the RUL. Note the obvious bulging of the major fissure (B, arrows).
In severe RUL collapse, the markedly diminished lobe becomes apposed to the mediastinum medially and simulates mediastinal widening (Fig. 9). The sharp interface of the minor fissure contributes to this appearance. Clues to the diagnosis are a small and slightly elevated hilum and compensatory increased lucency of the right lung.
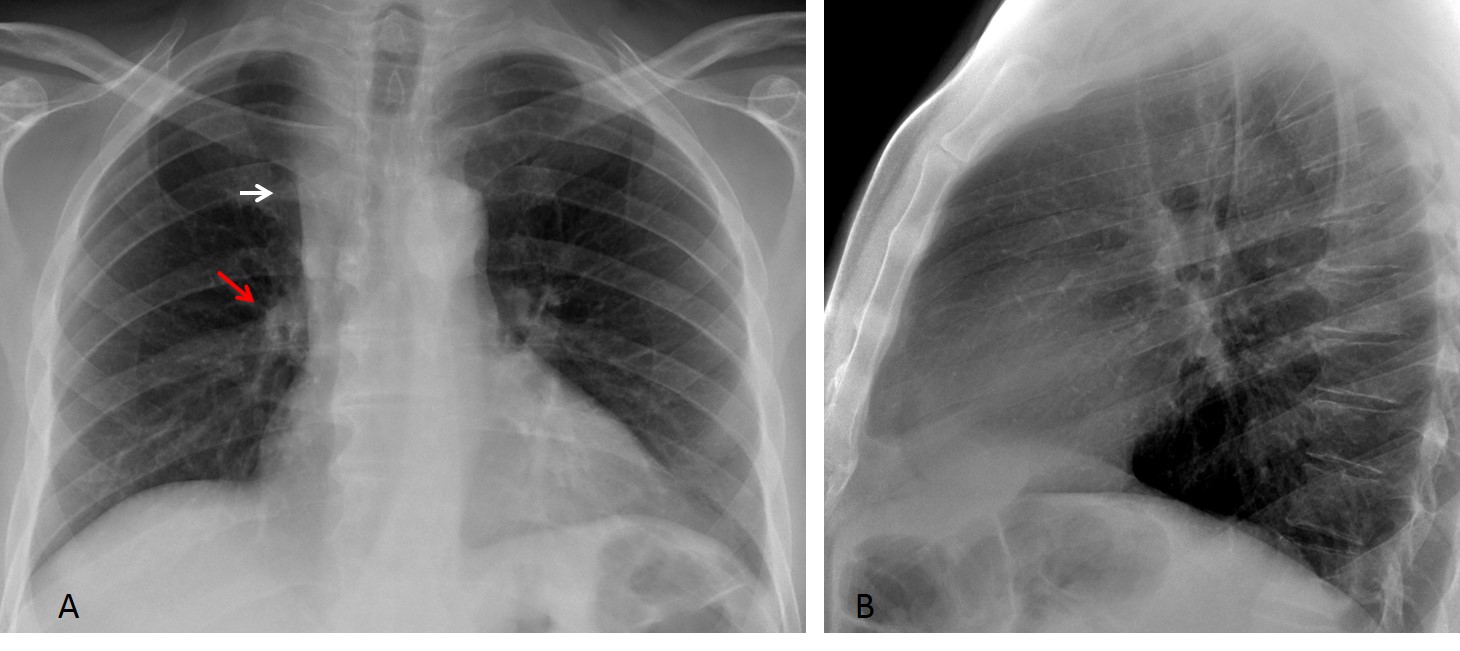
Fig. 9
Fig. 9 (above): 57-year-old man with carcinoma of RUL bronchus causing severe RUL collapse. Note the apparent mediastinal widening (A, white arrow), secondary to medial displacement of the collapsed lobe. The right hilum is small and slightly elevated (A, red arrow). There is compensatory right lung hyperlucency. The lateral view is unremarkable.
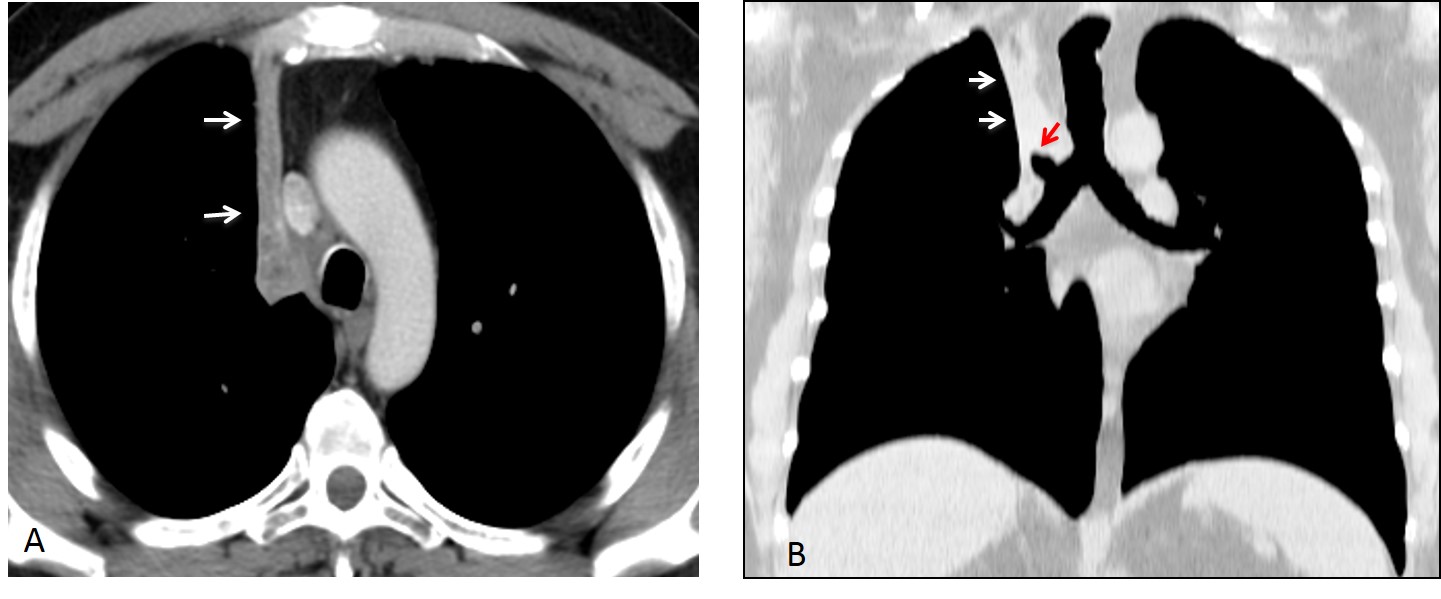
Fig. 10
Fig. 10 (above): enhanced axial CT image depicts a horizontal sliver of tissue, corresponding to the markedly collapsed RUL (A, arrows). Coronal CT shows the sharp outline of the minor fissure (B, white arrows). Note the obstructed RUL bronchus (B, red arrow).
RUL volume loss and bronchiectasis are common sequelae of healed tuberculosis, found in up to 15% of treated patients (Figs. 11 and 12). The diagnosis is easily made with the clinical history and comparison with previous films.
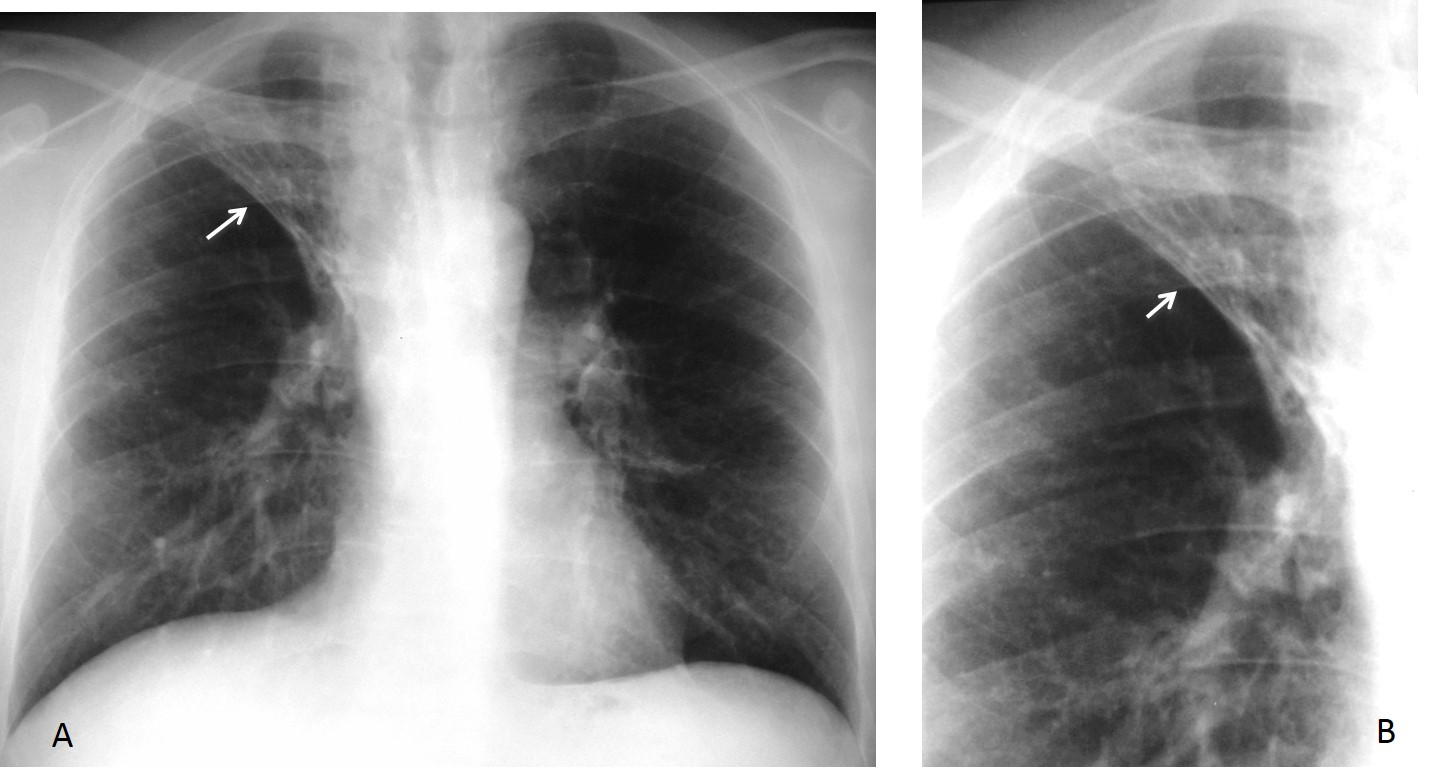
Fig. 11
Fig. 11 (above): 62-year-old man with previous TB infection. There is marked displacement of the minor fissure (A,B, arrows). The collapsed lobe is aerated, a common finding in inflammatory collapse.
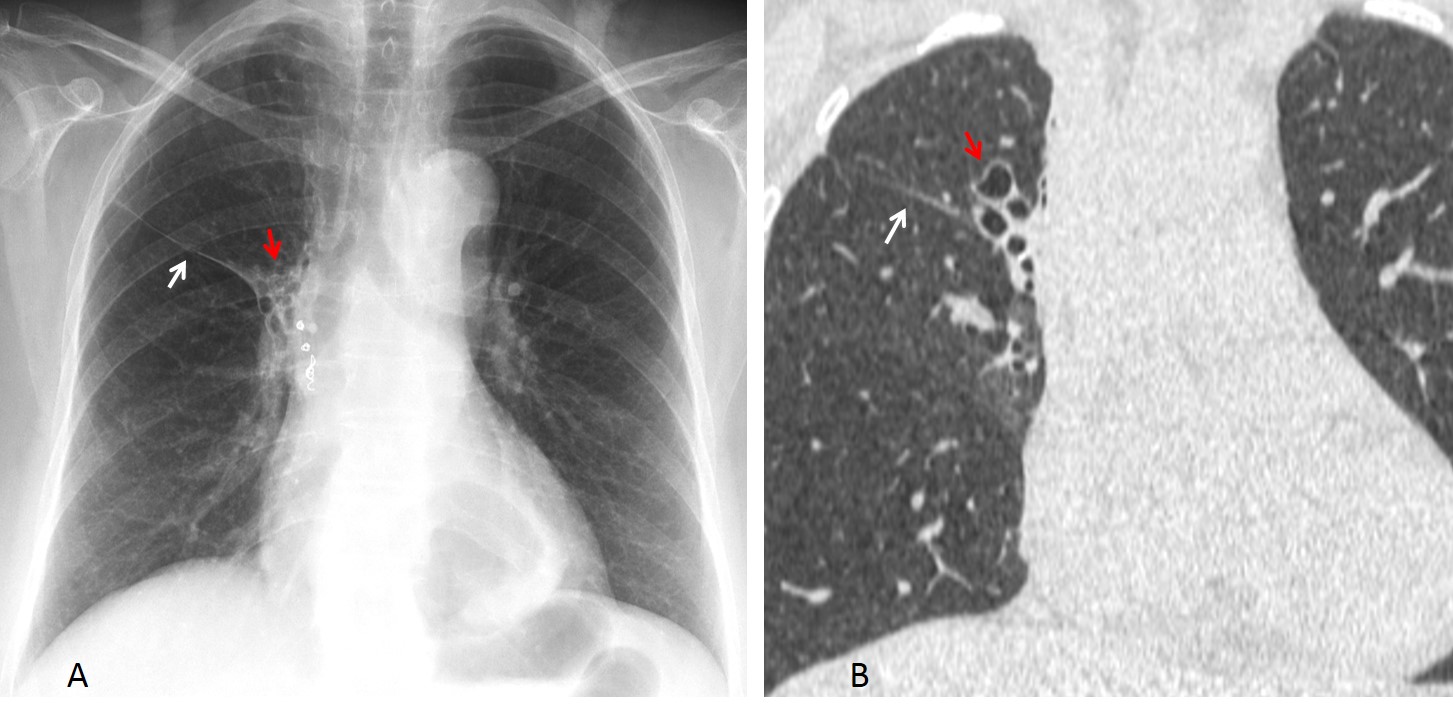
Fig. 12
Fig. 12 (above): old TB with moderate RUL collapse (A,B white arrows) and bronchiectasis (A,B, red arrows). Visible metal coils are secondary to embolisation for hemoptysis.

Follow Dr. Pepe’s advice
Follow Dr.Pepe’s Advice:
1. Uniform opacity of the lobe and elevation of the minor fissure are typical signs of RUL collapse
2. RUL collapse with the Golden sign is highly suggestive of malignancy
3. In drowned RUL, there is bulging of fissures without volume loss
4. Severe RUL collapse should not be confused with mediastinal widening. Elevated hilum and lung hyperlucency point to the right diagnosis


RUL atelectasis with Golden S sign, suggesting central carcinoma of the lung. Or any other central lesion, for that matter.
….gentile collega…a prima vista sembrerebbe una atelettasia del lobo polmonare superiore dx, con versamento pleurico….tuttavia la immagine tracheale non è attratta omolateralmente ed anzi sembra medializzata, …inoltre è apprezzabile la linea paracavale e paratracheale….per cui farei un confronto con eventuali precedenti e, prima della TC ,risolutiva, farei ciclo di terapia antibiotica(febbre) e rifarei un rx- di controllo ….
Superior displacement of horizontal fissure with RUL triangular opacity. On lateral view widening of retrosternal stripe. Compensatory hyperexpansion of right middle and lower lobe (intercostal space widening in the middle and lower zones on the right) and elevation of right diaphragm. These signs indicate right upper lobe atelectasis. Right pleural effusion. Medial part of horizontal fissure looks convex so I will agree this could be reverse S sign – possible carcinoma of the lung causing postopstructive atelectasis. In differential I would add enlarged lymph nodes,metastases or mediastinal tumour for causing the obstruction.
i think the opacity is in pleural space.
how about the left clavicle? there is relationship?
Clavicles may present weird apperances, depending of their position. This one is OK.
Why do you think that the opacity is pleural?
there is not evidence of atelectasia on the right side. it looks like but is not.
in leteral view the opacity is continued from the base to the apex with smooth borders and with out fluid levels.
DD pleural mass?
Interesting case, two of us are against atelectasis,and two of us are for it. 50/50 🙂
And I know the right diagnosis!
i can see too a pretracheal lymph node and the extention of the mass in the left apex.
mesothelioma?
its a carcinoma of the lung, what we see if the golden s sign, its a lobar collapse with possible complicating pneumonia with underlying carcinoma.
The RUL opacity I believe is not due to atelectasis of central origin. The right hilum on the profile x-ray images no apparent central mass.The trachea seems to have an indented contour on the right and left. Air delineates the upper right mediastinal line. Mild hyperinflation of the right middle and lower lung zone.The right hemodiaphragm is elevated and abnormal thoracic and epidiaphragmatic pleura is evident (fluid? pleura thickening?). The left hemithorax also presents findings: there is an opacity above the aortic knob (LUL atelectasis?) in the PA x-ray and an apical cap in the left apex. Dr Pepe,is there a history of plombage/ collapse therapy???? Previous Tb?
No history of plombage , nor anything else. When I posted the case I thought it very straightforward; but I guess I was wrong.
pneumonia
and pleural effusion l.dex.
The mediatine isn’t displacement. For correlation and simtomas Pneumònia Of Superior Right Lobul
My first impression is RUL atelectasis with Golden S sign, regardless, it could be plural effusion as the costophrenic angle is also obliterated.
We should be aware of the symptoms, don’t just focus on the X ray signs. Atelectasis and fever, among the suggested diagnosis, could be found in tuberculosis.
I disagre with you. Sometimes, the signs can be a strong indicator of the disease (as in this case).
En la radiografía de ve una opacidad homogénea de límite definido compatible con una atelectasia del lobulo superior, signo de golden. Al haber una compresión intrínseca o extrínseca sobre el bronquio se produce la atelectasia. Puede corresponder a tuberculosis o un tumor (adenopatia o compromiso por masa)
Postobstructive atelectasis due to a mucus plug in the right superior lobar bronchus in a patient has COPD.
PNEUMONIA OF RUL AND EFFUSION OF CAVI PLAEURE LAT.DEX.
PNEUMONIA OF RUL AND EFFUSION OF CAVI PLEURAE LAT.DEX
I believe I can say that the case corresponds to a RUL collapse with a Golden sign.
More images tomorrow.
Congratulations to all winners!
Sorry professor i think i see phantoms on the films. 🙂
It was too easy to be true. but a good lesson for next time!
Remember that Dr. Pepe’s mission is to teach in order to prepare people for the Diploma. Cacere’s corner shows difficult cases, for fun.