Dr. Pepe’s Diploma Casebook: Case 62 – SOLVED!
Dear Friends,
Today I am showing PA chest and sagittal CT of a 66-year-old woman with a persistent RLL infiltrate and negative bronchoscopy. Check the images below, leave me your thoughts in the comments section, and come back on Friday for the answer.
Diagnosis:
1. Tuberculosis
2. Chronic aspiration pneumonia
3. Carcinoma
4. None of the above
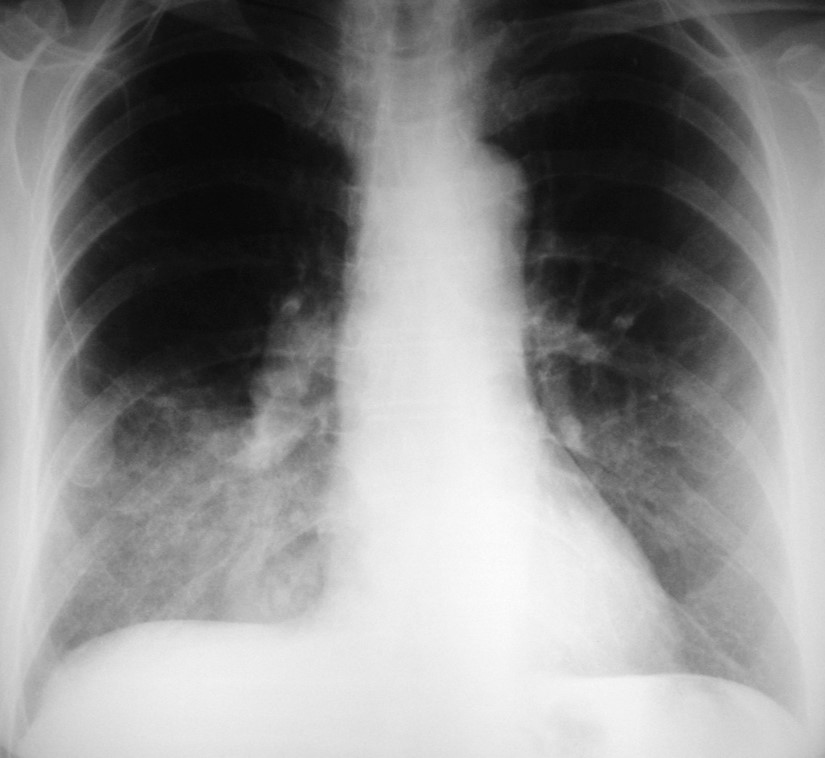
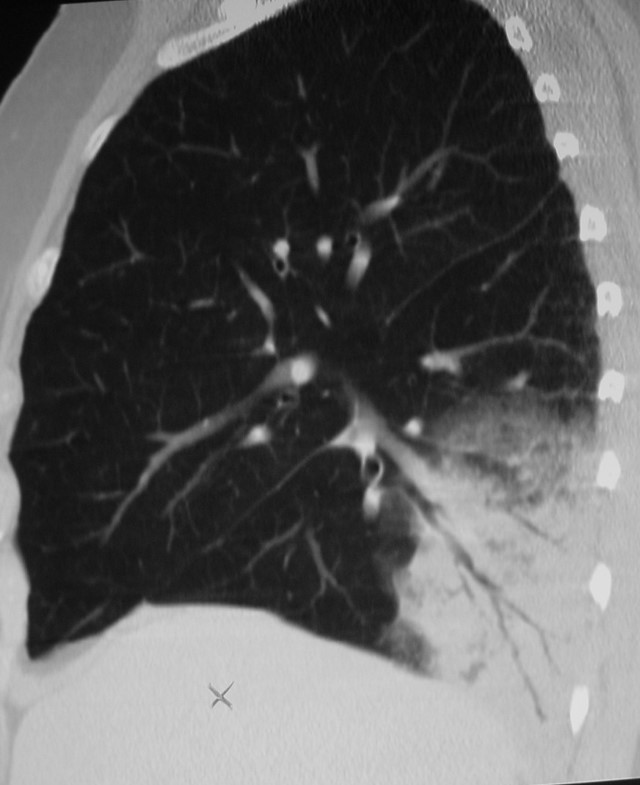
Findings: chest radiography shows an RLL infiltrate (A, arrow). Unenhanced sagittal CT depicts thin, stretched bronchi (B, arrows) within an airspace infiltrate. The clue to the diagnosis is the appearance of the bronchi. In TB and chronic aspiration, the bronchi are usually dilated, whereas thin, stretched bronchi are more common in malignant processes. Therefore, the most likely diagnosis is malignancy.
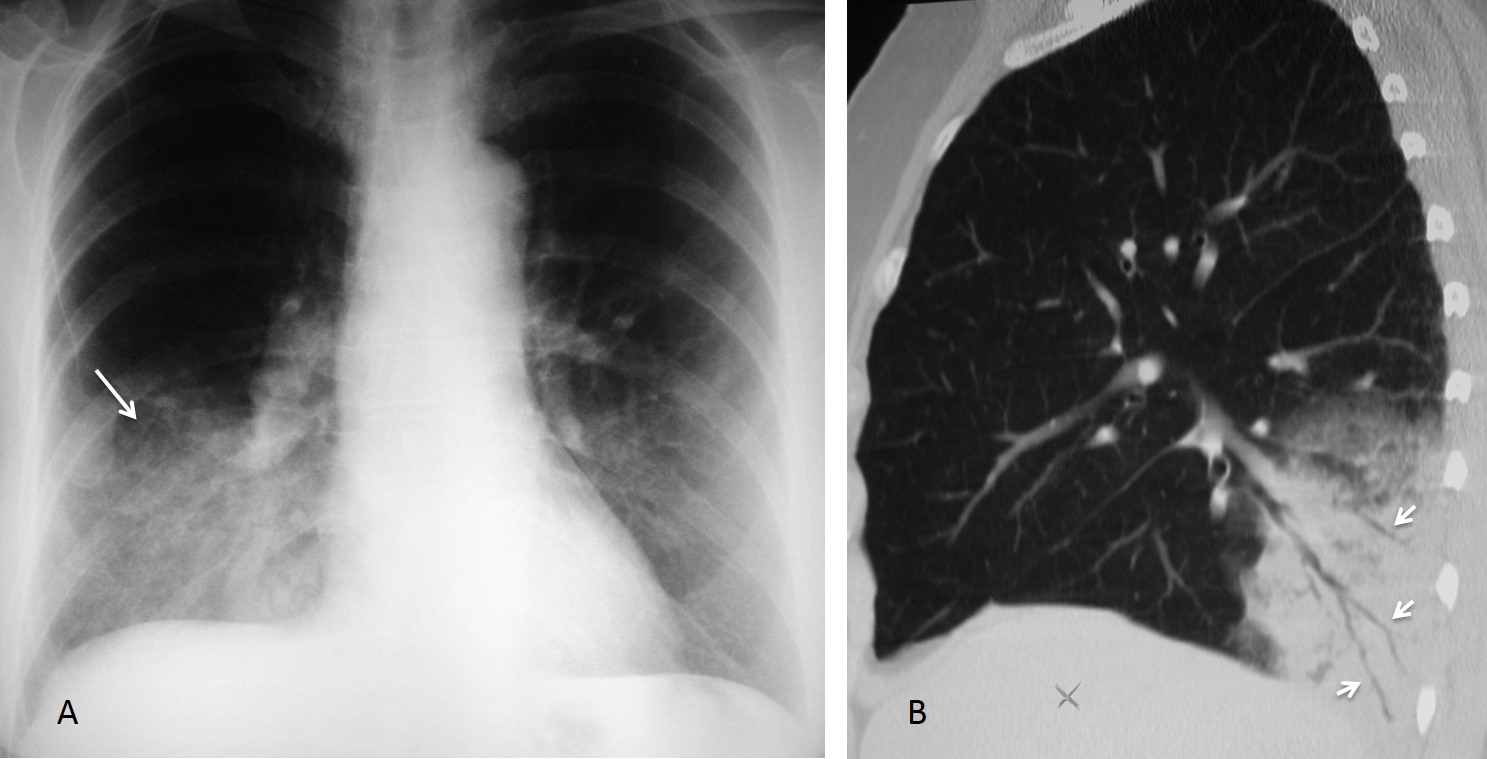
Fig. 1
Final diagnosis: adenocarcinoma
The term air bronchogram was coined by the late Dr. Benjamin Felson to describe visible bronchi outlined by air over a background of pulmonary consolidation in the chest radiograph. CT provides better visualisation of the bronchi, which can be seen when filled with air (CT air bronchogram), with normal low-density mucus (mucus bronchogram), or with dense mucus (high-attenuation bronchogram).
The purpose of this presentation is to discuss the different CT appearances of the bronchi within a pulmonary consolidation and their differential diagnosis.
Air-filled bronchi are the hallmark of the CT air bronchogram. According to their morphology, the bronchi can appear dilated or narrowed and stretched, or they may be seen as bubble-like lucencies.
Dilated bronchi are usually seen in inflammatory opacities, where the volume loss makes the bronchi shorter and wider (Fig. 2).
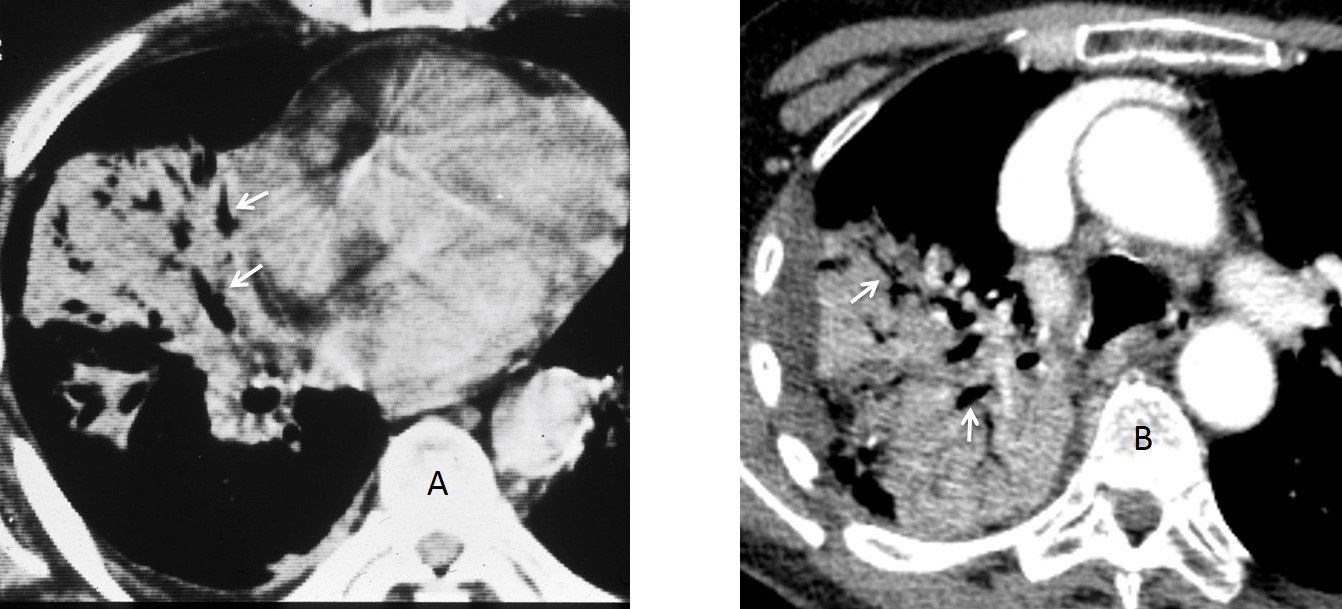
Fig. 2
Fig. 2: axial CT of two different patients. The first (A) has chronic RLL disease, secondary to a foreign body. The other (B) has RUL pneumonia. Note the dilated bronchi in both cases (A and B, arrows).
In lobar collapse, dilated bronchi suggest inflammatory rather than neoplastic changes. Demonstration of an open bronchus helps to exclude a central carcinoma (Fig. 3).
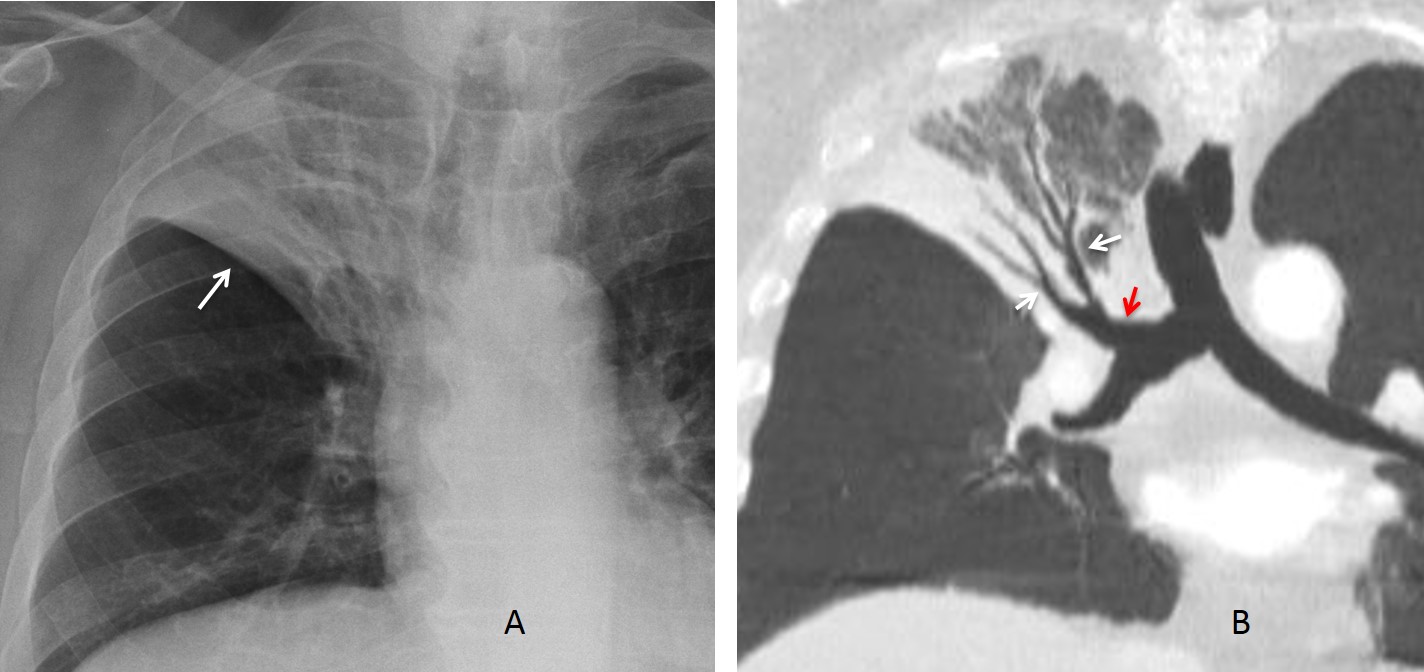
Fig. 3
Fig. 3: RUL lobar pneumonia with loss of volume (A, arrow), which makes it necessary to rule out carcinoma. Coronal CT shows dilated bronchi within the infiltrate (B, white arrows), suggesting an inflammatory process. The RUL bronchus is open (B, red arrow), excluding a central lesion.
Narrowed bronchi, the so-called leafless tree appearance, are seen as thin, stretched, scarcely branching bronchi within a pulmonary consolidation. This appearance is due to infiltration of the alveolar space surrounding the bronchi (Fig. 4).
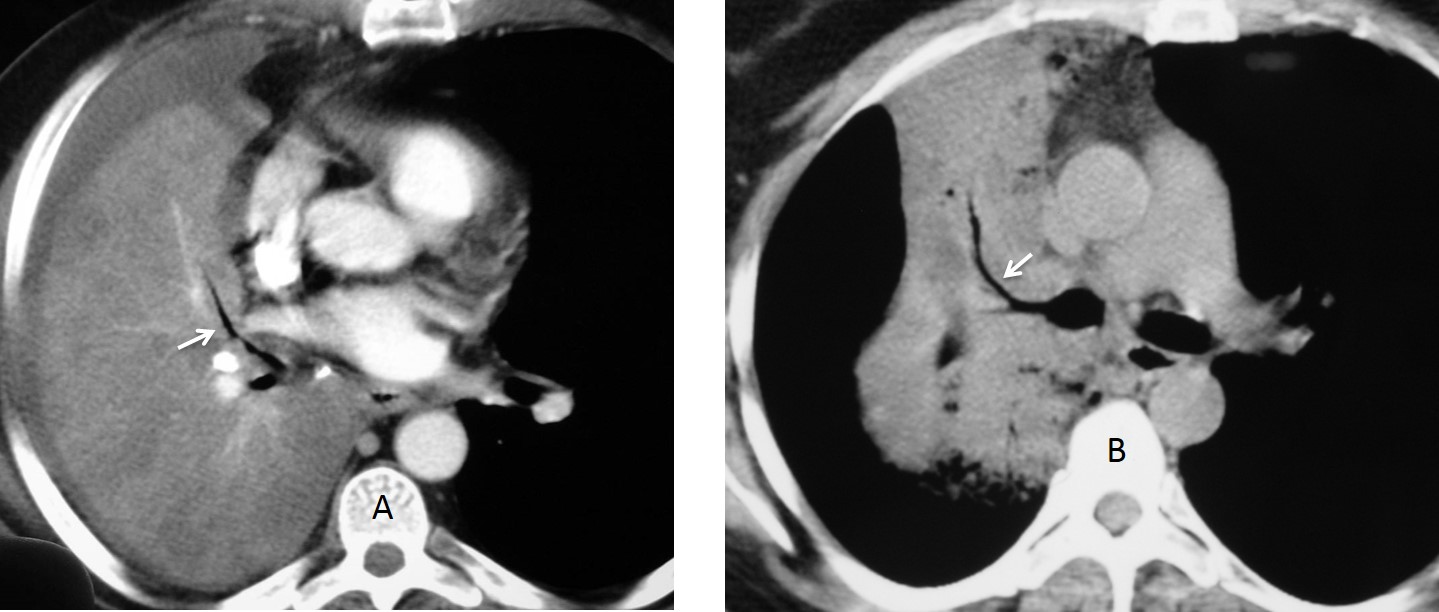
Fig. 4
Fig. 4: two different patients with adenocarcinoma. Note the leafless tree appearance of the visible bronchi in both cases (A and B, arrows).
The most common cause of leafless tree is neoplastic disease, mainly adenocarcinoma and lymphoma (Figs. 5 & 6). In my experience, leafless tree is a good sign to suspect malignancy, although it can also occur in non-malignant processes.
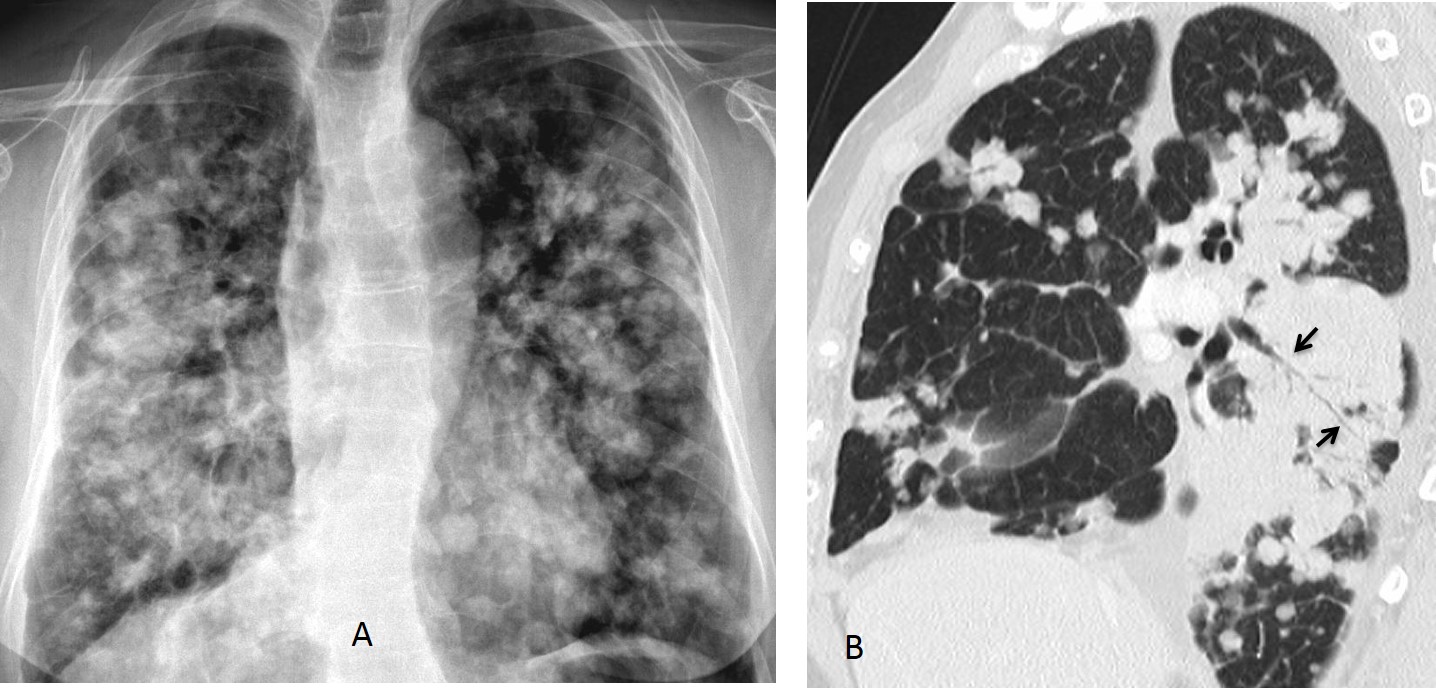
Fig. 5
Fig. 5 (above): 74-year-old woman with widespread adenocarcinoma. Note the leafless tree sign in the sagittal CT reconstruction (B, arrows).
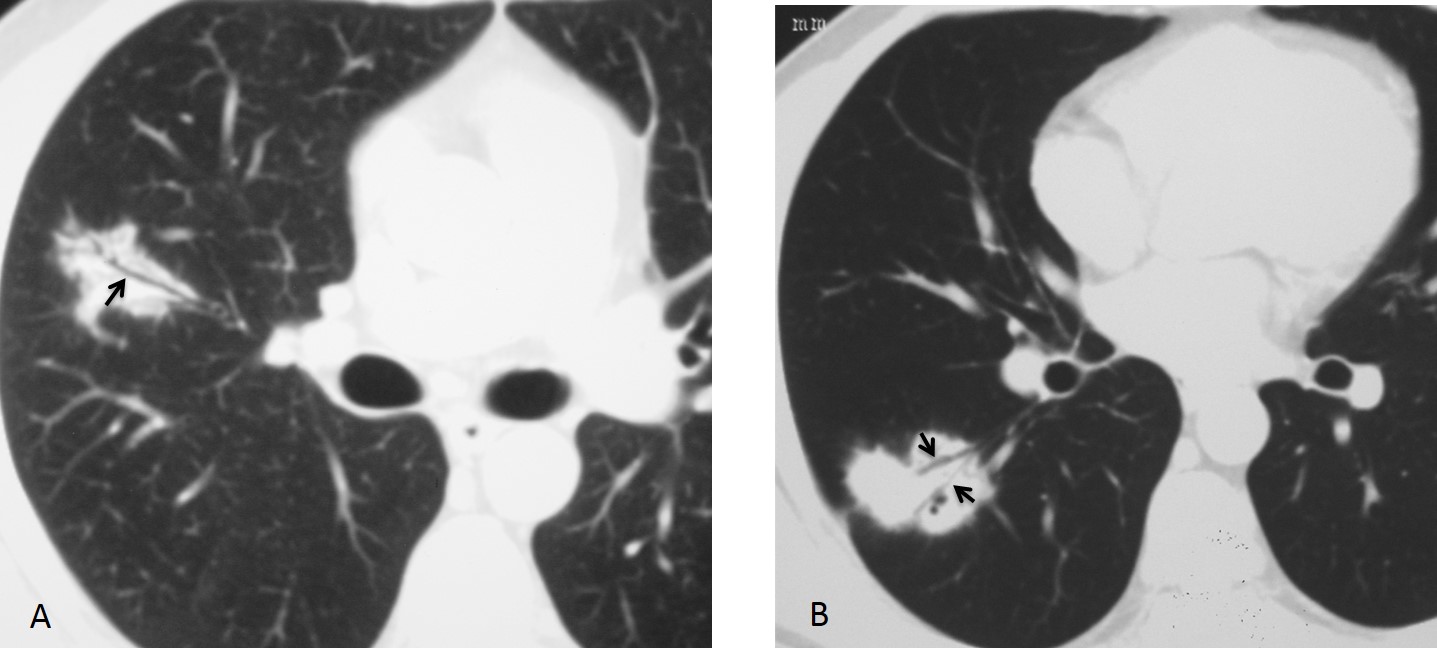
Fig. 6
Fig. 6 (above): 31-year-old man with scattered pulmonary infiltrates. The leafless tree sign is evident in two of them (A and B, arrows). Diagnosis: Hodgkin disease.
Bubble-like lucencies represent air in small bronchi and occur in peripheral infiltrates. They are highly suggestive of peripheral adenocarcinomas (Fig. 7).
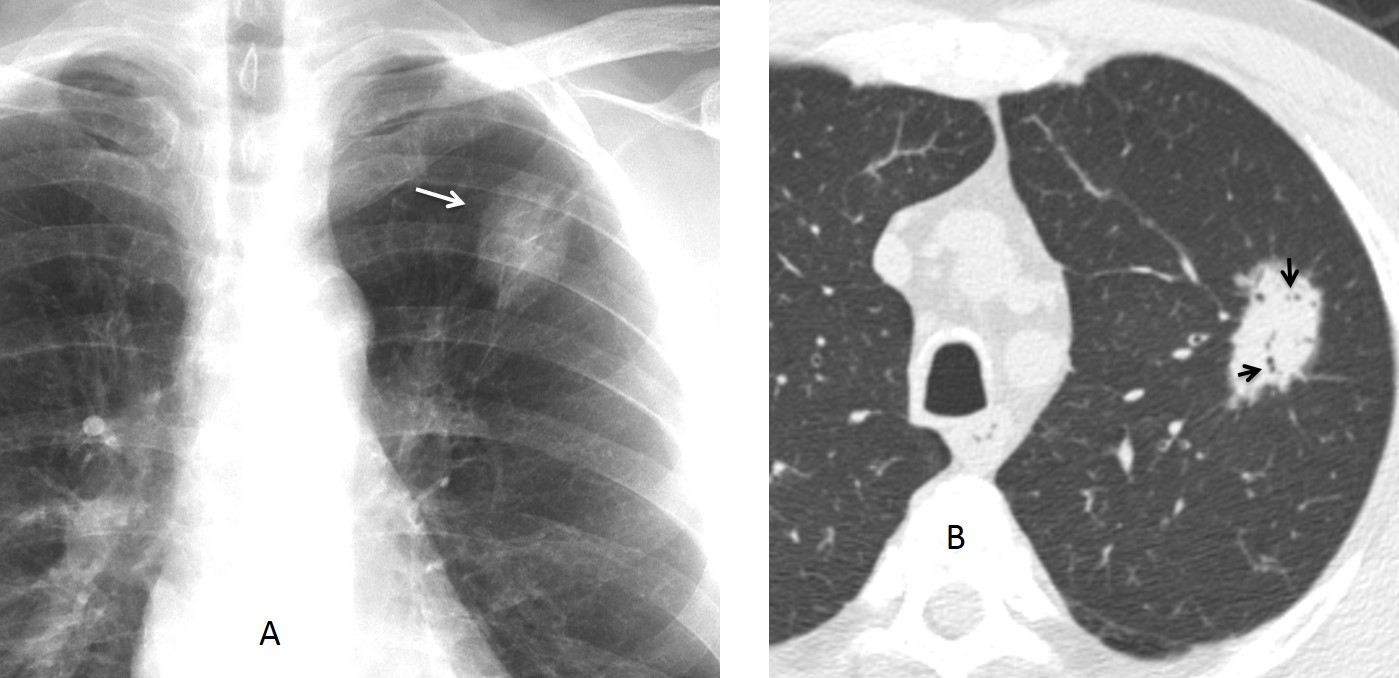
Fig. 7
Fig. 7 (above): 69-year-old. man with a slow-growing nodule in the LUL (A, arrow). Axial CT shows numerous bubbly lucencies within the nodule (B, arrows). Diagnosis: adenocarcinoma.
Mucus bronchogram occurs when the bronchi are filled with low-density mucus. The bronchi are seen as branching, linear low-density structures within the pulmonary consolidation (Fig. 8).
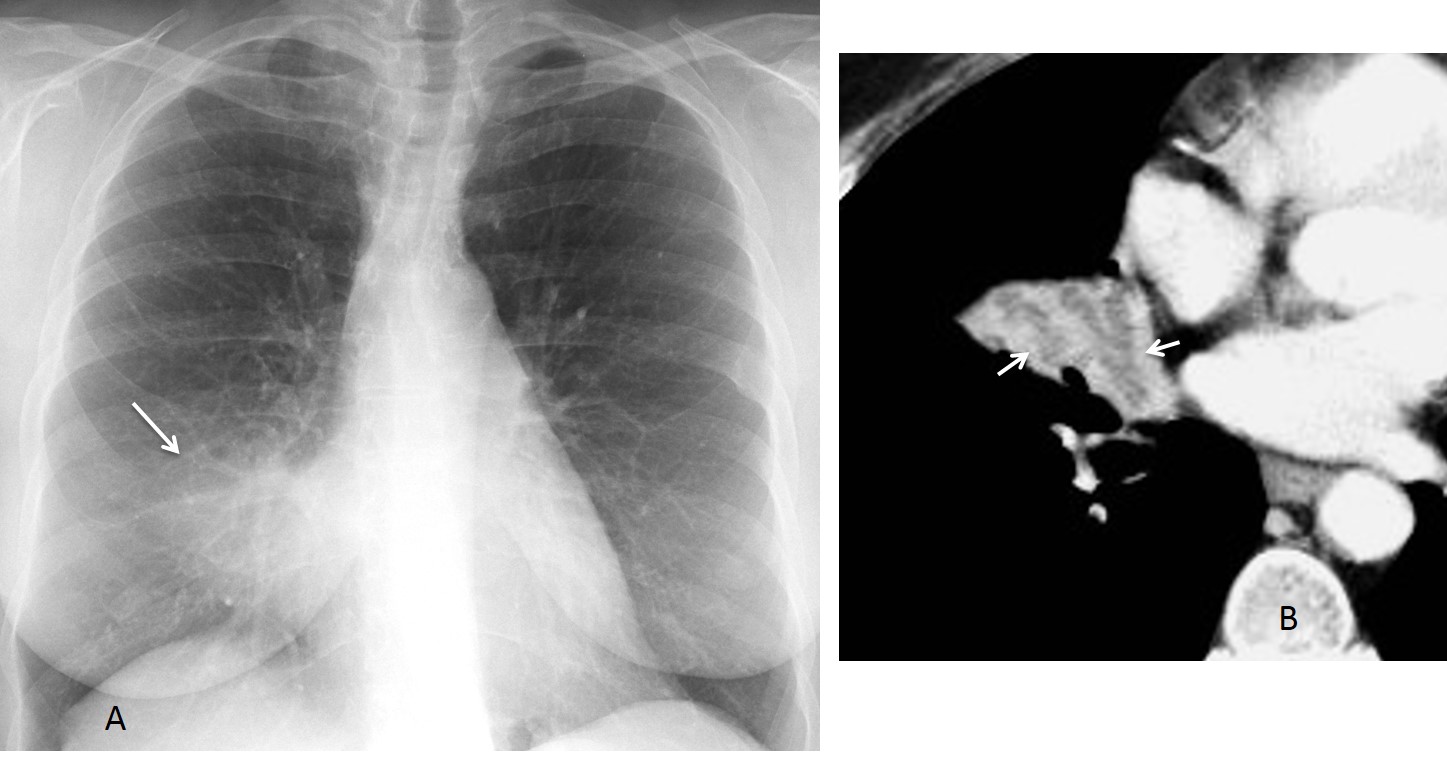
Fig. 8
Fig. 8 (above): 59-year-old woman with chronic RML disease (A, arrow). Enhanced axial CT shows RML collapse with a typical mucus bronchogram (B, arrows). At bronchoscopy a green pea was found obstructing the RML bronchus.
Mucus bronchogram usually occurs in lobar collapse secondary to central obstruction of any cause. The prevalence of bronchogenic carcinoma makes it the most common etiology (Fig. 9).
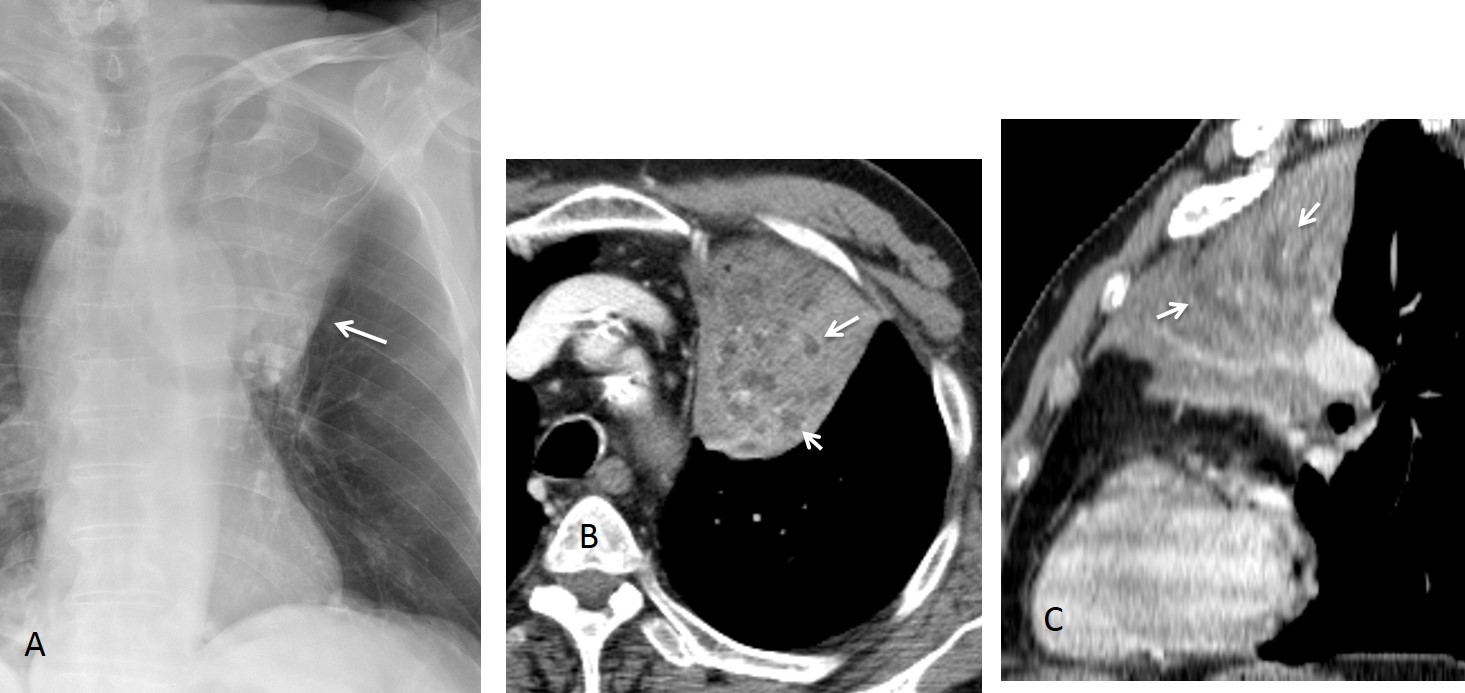
Fig. 9
Fig. 9 (above): 80-year-old man with bronchogenic carcinoma. The chest radiograph shows a collapsed LUL (A, arrow). Enhanced axial CT depicts the mucus-filled bronchi as numerous rounded lucencies (B, arrows). Sagittal CT confirms the mucus bronchogram (C, arrows).
High-attenuation bronchogram occurs when the bronchi are more opaque than the surrounding pulmonary condensation. The increased density of the mucus is due to the presence of calcium salts and metals. This sign is highly suggestive of allergic bronchopulmonary aspergillosis and is seen in up to 25% of cases.
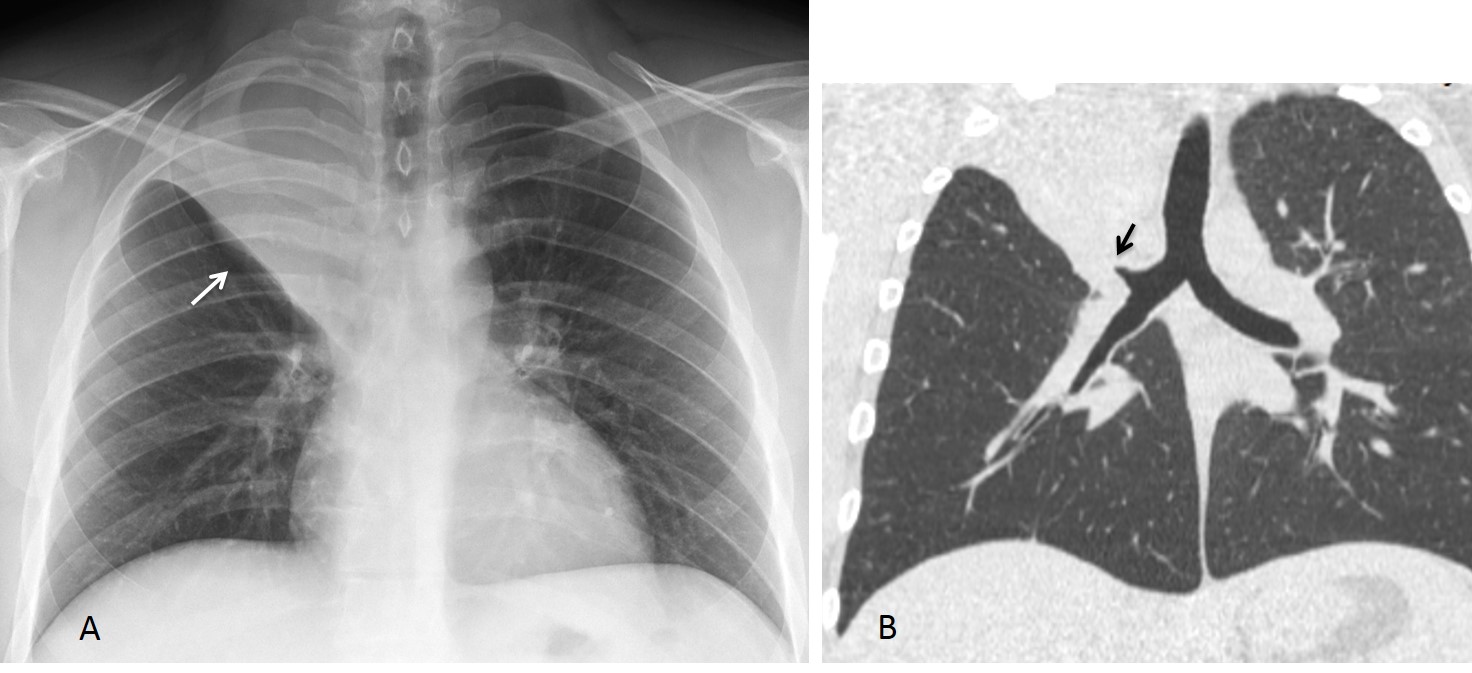
Fig. 10
Fig. 10 (above): 32-year-old man with RUL collapse (A, arrow). Coronal CT shows obstruction at the origin of the RUL bronchus (B, arrow).

Fig. 11
Fig. 11 (above): unenhanced axial and coronal CT show rounded opacities within the collapsed RUL lobe (A, arrows), which correspond to high-attenuation mucus plugs within the bronchi, better seen in the coronal reconstruction (B, arrows). Aspergillus was found and removed at bronchoscopy, with marked improvement of the findings.
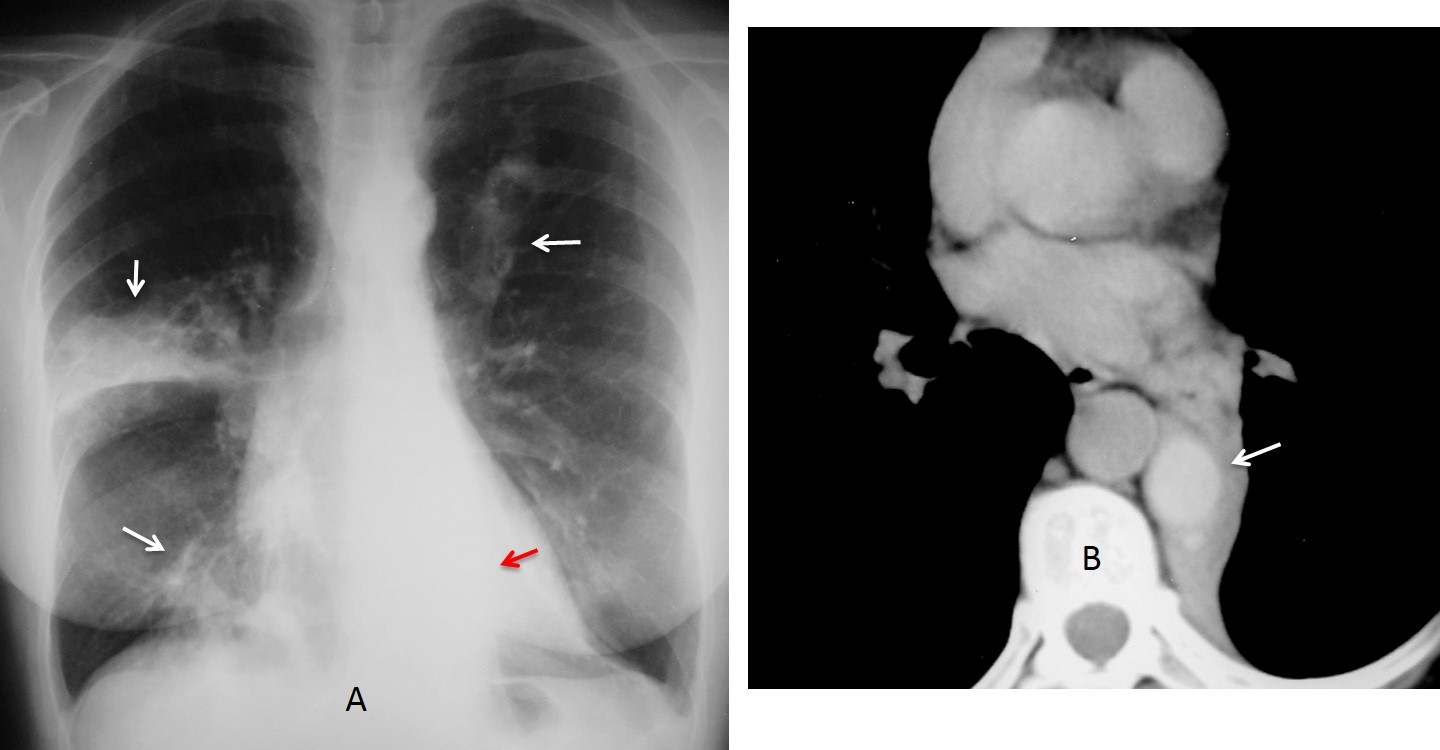
Fig. 12
Fig. 12 (above): 66-year-old woman with allergic bronchopulmonary aspergillosis. PA chest film shows widespread lung changes (A, white arrows), as well as LLL collapse (red arrow). Enhanced CT reveals a large, high-attenuation mucus plug at the origin of the LLL bronchus (B, arrow), confirmed at bronchoscopy.

Follow Dr. Pepe’s advice
Follow Dr.Pepe’s Advice:
1. The CT density of bronchi within a pulmonary condensation is helpful for orienting the diagnosis.
2. Air bronchogram with dilated bronchi suggests inflammatory disease.
3. The leafless tree appearance is highly suggestive of malignancy.
4. Mucus bronchogram suggests central bronchial obstruction. The most common cause is bronchogenic carcinoma.
5. High-attenuation bronchogram occurs in allergic aspergillosis.


Bronchoalveolar carcinoma = minimally invasive adenocarcinoma
….regola KISS….non adenopatie….broncogrammi aerei….Cronica aspirazione polmonite….alla BAL , macrofagi !Scusa se continuo a rispondere in italiano, ma non so l’inglese e , per questo motivo, non prenderò mai il Diploma….!!!!Sempre comunque affezzionato fans…..
Don’t worry. Italian is easy to understand. And we always have google translator!
As far as I know, you can take the oral Diploma examination in your native language
Bad location for TB, no lymph node enlargement.
Good location for aspirarion pneumonia, and I feel there is left side compromise on the Xray.
With air broncogram, it could be adenocarcinoma or lymphoma, but in think this case is bilateral.
I choose aspirarion.
Greetings!!!
Right lower posterior segment consolidation with air bronchogram,, suggestive of chronic aspiration pneumonia
consolidation, D/D includes broncho alveolar carcinoma
Is this your first choice?
Carcinoma
4. None of the above.
it is a intralobar sequestration (ILS)
She’s got fever?
No.
I think the infiltration is bilateral.
Chronic aspiration pneumonia?
There is no infiltrate on the left side. Think harder.
Good case for this season. The threes are loosing their sheets and the gardeners are going to prune them. So this case should be an Adenocarcinoma.
Welcome back. Good answer. Congratulations to the family gardener
My housband is gardener
if you agree with me that good history take for this patient will be useful with us as aspiration pneumonia is in my mind as the first choice as we see there is segmental distrubution of the opacity and is noted in an expected area for the aspiration pneumonia ., however follow up of the size of this lesion should be done to exclude any neoplastic lesion.
thank you
I agree with you that the clinical history is crucial in many cases. However, in this particular patient the imaging signs were the ones which pointed to the right diagnosis.
Thanks for participating.
THANK YOU SIR
At this time of the week I believe I can safely disclose the diagnosis: adenocarcinoma of lung, discovered because of the lefless tree sign. Full explanation tomorrow.
Congratulations to Dr. AMR SAADAWY, who was the first to suggest the right diagnosis.
…..Stupenda lezione di semeiotica…..Grazie Galactico Professore !!!!!!
Prego. Thanks for participating!
great case professor!!! very useful course.
Thanks. You almost got it. Told you to think harder 😉
Answer no. 2
Chronic aspiration pneumonia
No 4.
Chronic Aspiration pneumonia.My greetings from Albania.