Dr. Pepe’s Diploma Casebook: Case 64 – SOLVED!
Dear Friends,
Showing today pre-op radiographs for knee surgery of a 17-year-old girl. Check the images below, leave your diagnosis in the comments section and come back on Friday for answer.
Diagnosis:
1. Branchial cyst
2. Neurogenic tumour
3. Lymphocele
4. None of the above
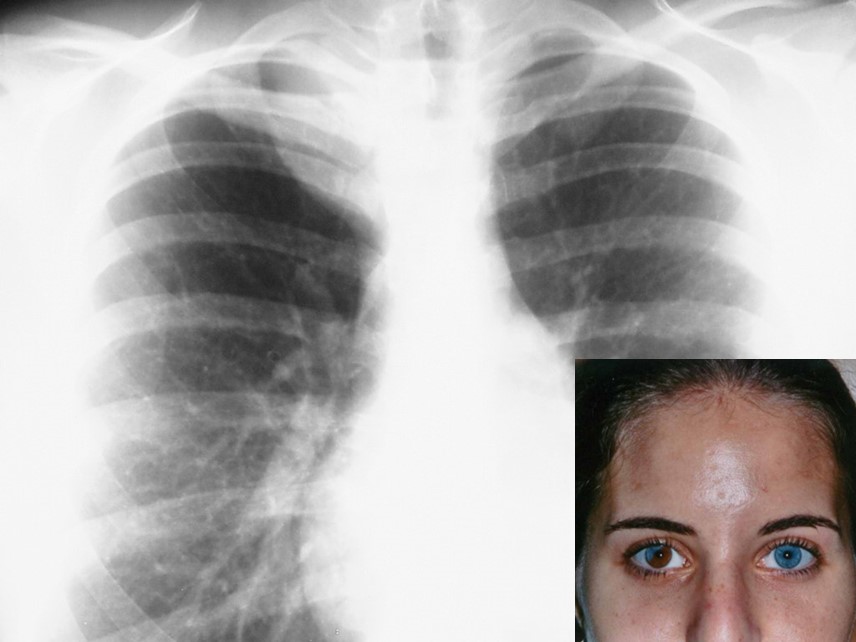
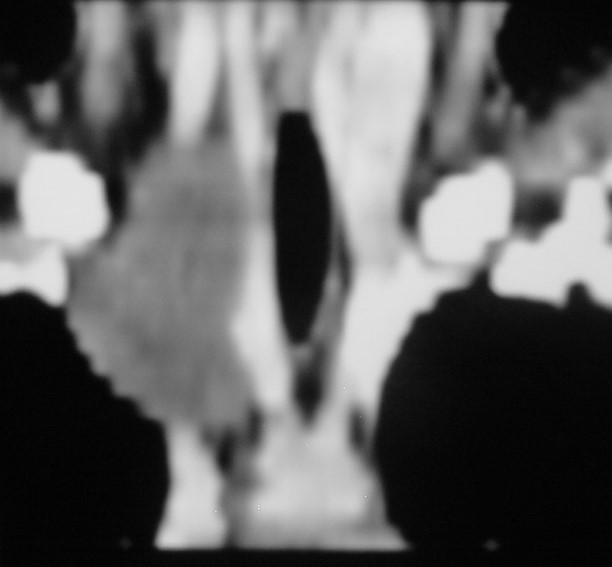
Findings: chest radiograph shows a right superior mediastinal mass (A, arrow). Coronal CT depicts a low-attenuation non-enhancing mass extending into the neck (B, arrow). The patient’s heterochromia iridis of the right eye (C) is a clue to the diagnosis. This finding is associated with tumours of the vagus nerve. Therefore, the most likely diagnosis is neurogenic tumour.
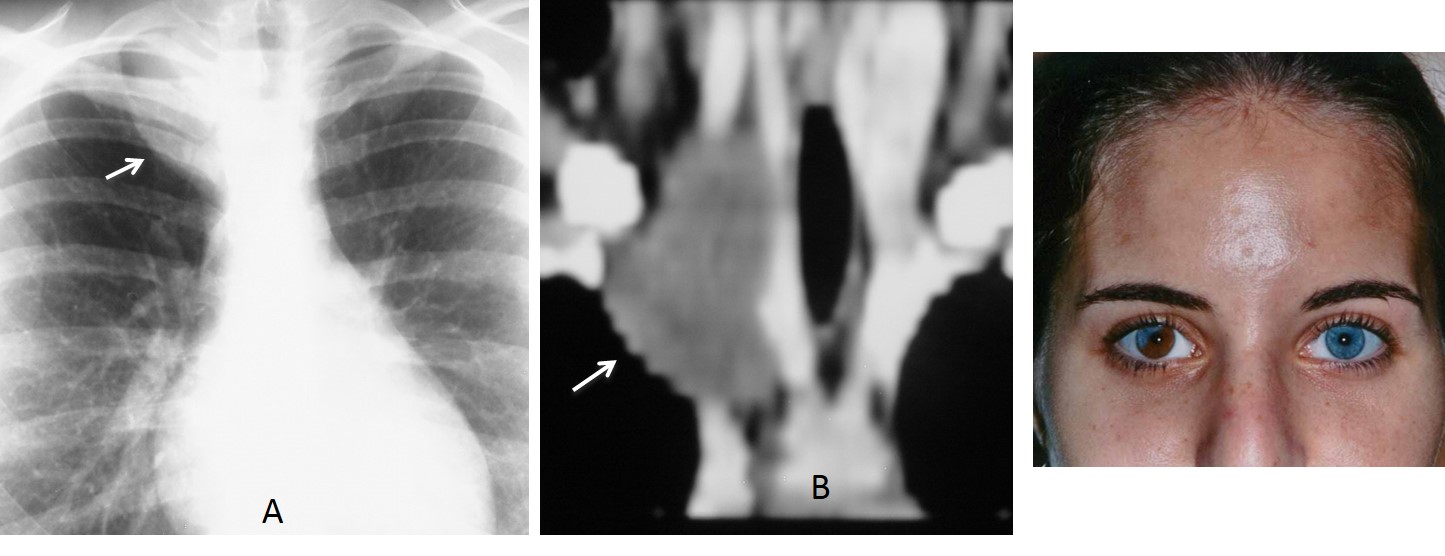
Final diagnosis: ganglioneuroma of the vagus nerve.
This case is presented to discuss posterior mediastinal masses. As was mentioned in Diploma case #41, the mediastinum is divided into four compartments (anterior, middle, posterior, and thoracic inlet). The posterior mediastinum is delimited by a line drawn 1 cm behind the anterior border of the thoracic spine (Fig. 1).
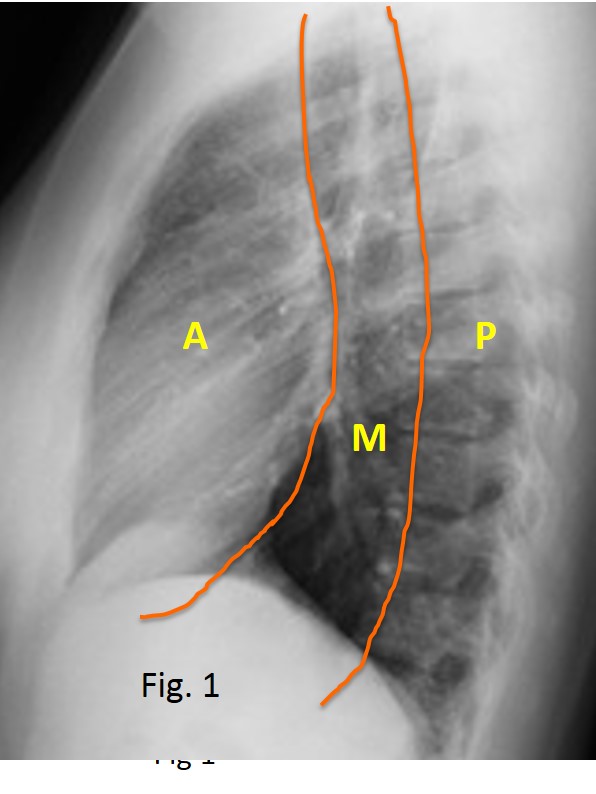
Fig. 1
About 80% of posterior mediastinal masses correspond to neurogenic tumours. They may be related to peripheral nerves (neurinomas and schwannomas, which are more common in adults) or to sympathetic ganglia (ganglioneuromas and neuroblastomas, which are seen mainly in children). Most patients are asymptomatic.
Single neurogenic tumours appear in the PA chest radiograph as posterior mediastinal masses that do not obscure the mediastinal or aortic contour. In the lateral view they are projected over the spine (Fig. 2)
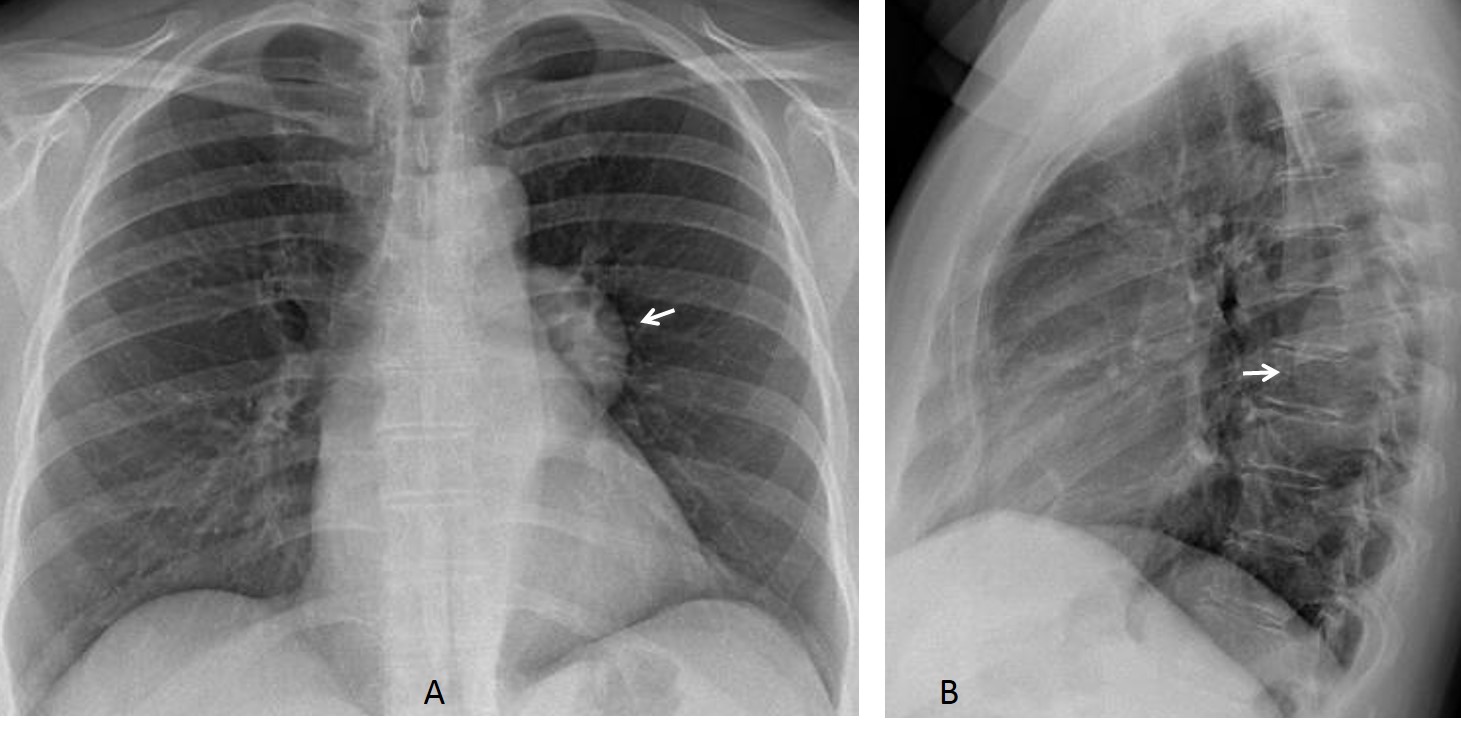
Fig. 2
On CT, up to 70% of neurogenic tumours have low attenuation values, attributed to a large amount of lipids and fluid (Fig. 3). Occasionally, this low density may simulate a cystic lesion. In these cases, MRI is helpful to confirm that it is a solid lesion.
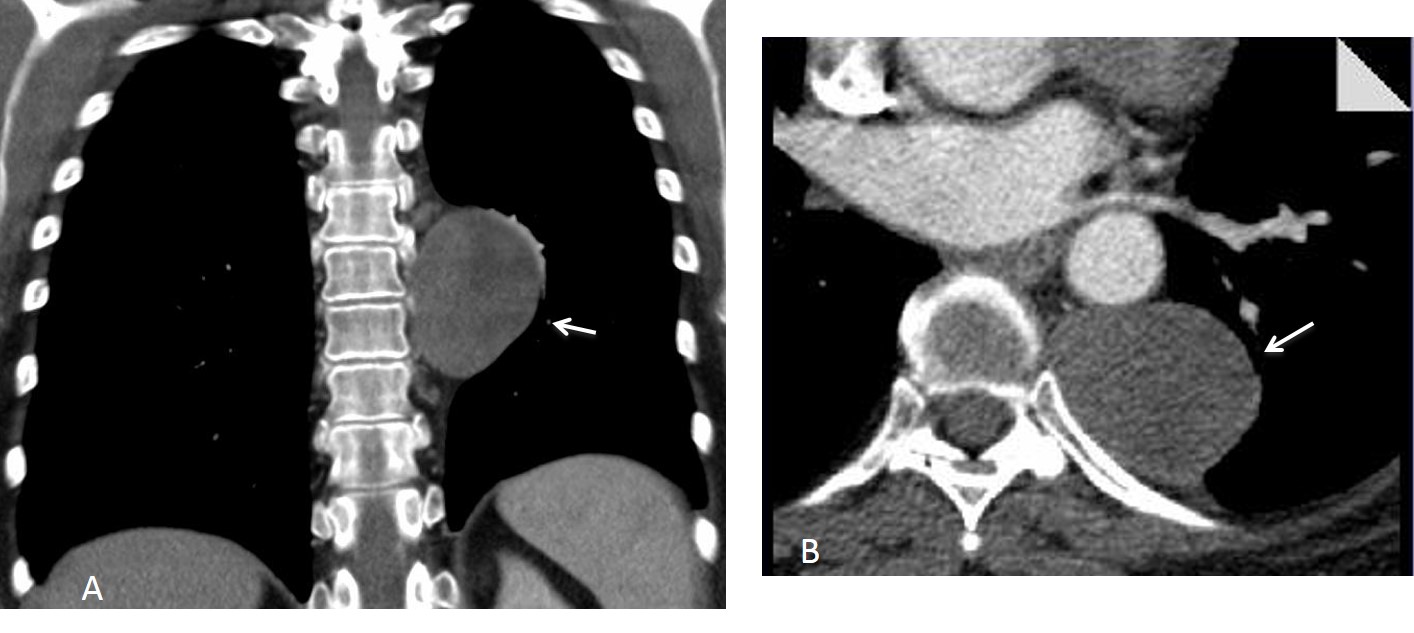
Fig. 3
Fig. 3. Same patient as Fig. 2. Enhanced coronal and axial CT images show a low-attenuation mass in the posterior mediastinum (A and B, arrows). There is no bone erosion. Diagnosis: neurinoma.
On MRI, schwannomas and neurinomas have low-to-intermediate signal intensity on T1W and intermediate-to-high signal intensity on T2W images (Fig. 4). The main indication of MRI in neurogenic tumours is to differentiate solid from cystic lesions and exclude intraspinal tumour extension.
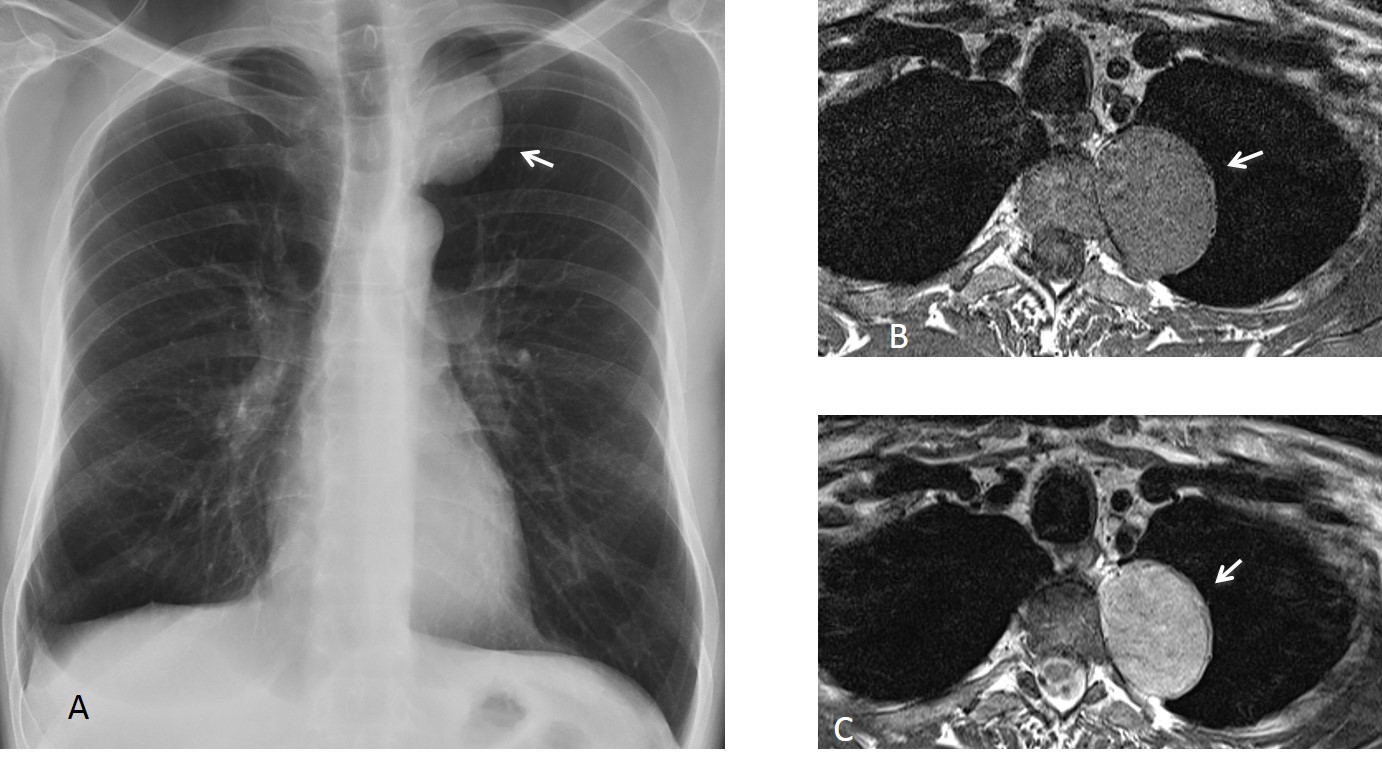
Fig. 4
Fig. 4. 45-year-old man with a neurinoma. PA chest film shows a left superior mediastinal mass (A, arrow). MRI shows a low-signal mass (B, arrow), with higher signal on the T2W study (C, arrow).
A fair number of nerve tumours cause erosion of the vertebral bodies or widening of the neural foramina, which are easily seen on CT (Fig. 5). Ten percent of these tumours grow through the intervertebral foramen and extend into the vertebral canal. MRI should always be performed preoperatively to exclude this possibility.
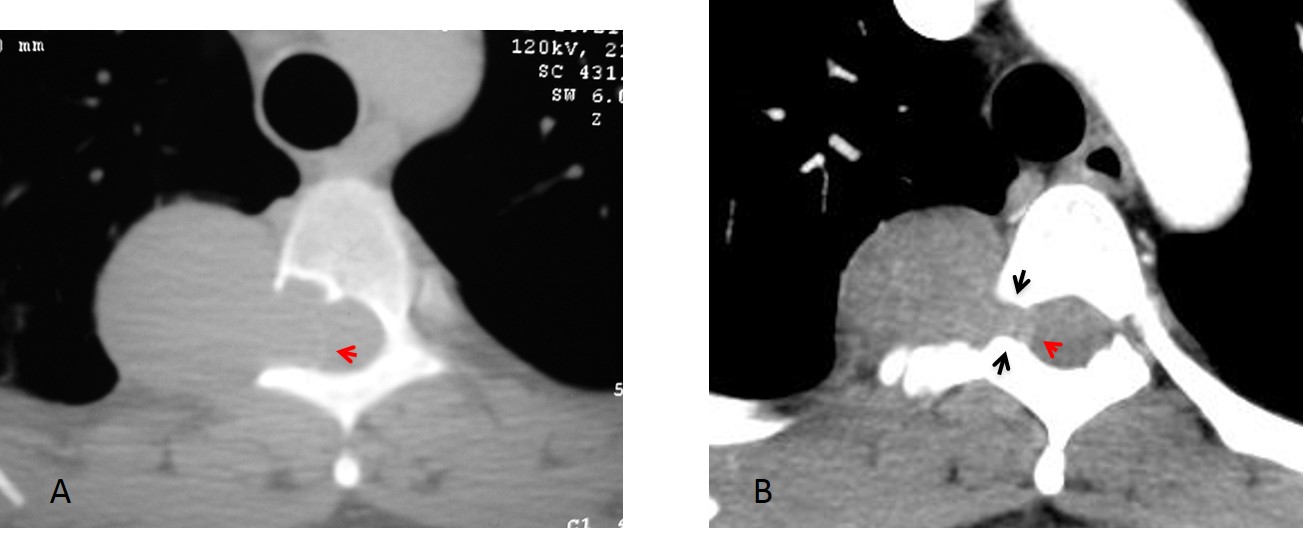
Fig. 5
Fig. 5. Two different patients with neurogenic tumours that have eroded the neural foramina. The erosion is obvious in the first case (A) and less apparent in the second (B, black arrows). Spinal canal invasion, which has occurred in both cases (A and B, red arrow), is more evident in the second patient. MRI is better able to provide this information.
Plexiform neurofibromas are nonencapsulated tumours that infiltrate along the nerves and present as multiple masses (Fig. 6). They are pathognomonic of neurofibromatosis.
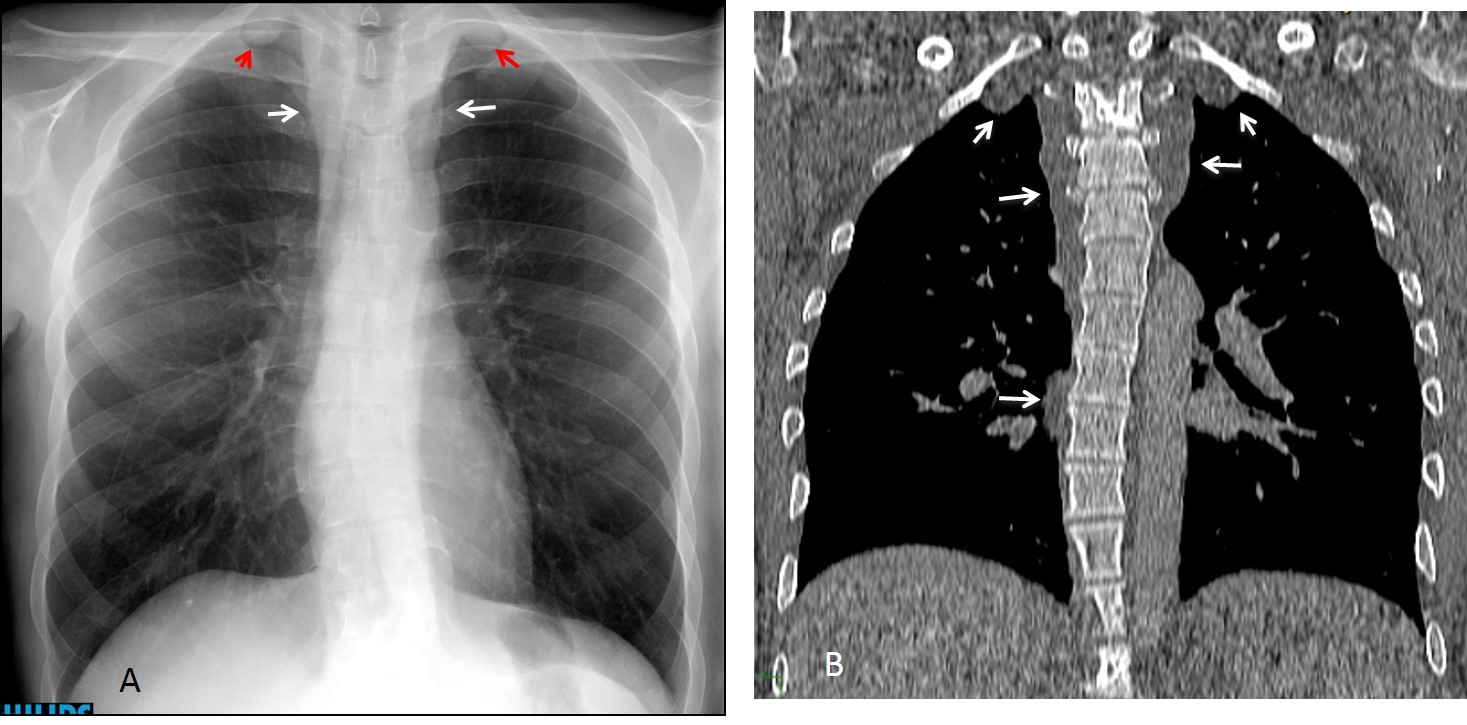
Fig. 6
Fig. 6: 45-year-old patient with neurofibromatosis. PA chest film shows mediastinal widening (A, white arrows) and nodules in the apices (A, red arrows). Coronal CT demonstrates plexiform neurofibromas extending along the posterior mediastinum and apices (B, arrows).
Cystic lesions of the posterior mediastinum are unusual. One example is neurenteric cyst (Fig. 7), which is often accompanied by vertebral abnormalities. Occasional cystic tumours and lateral meningoceles are other possibilities.
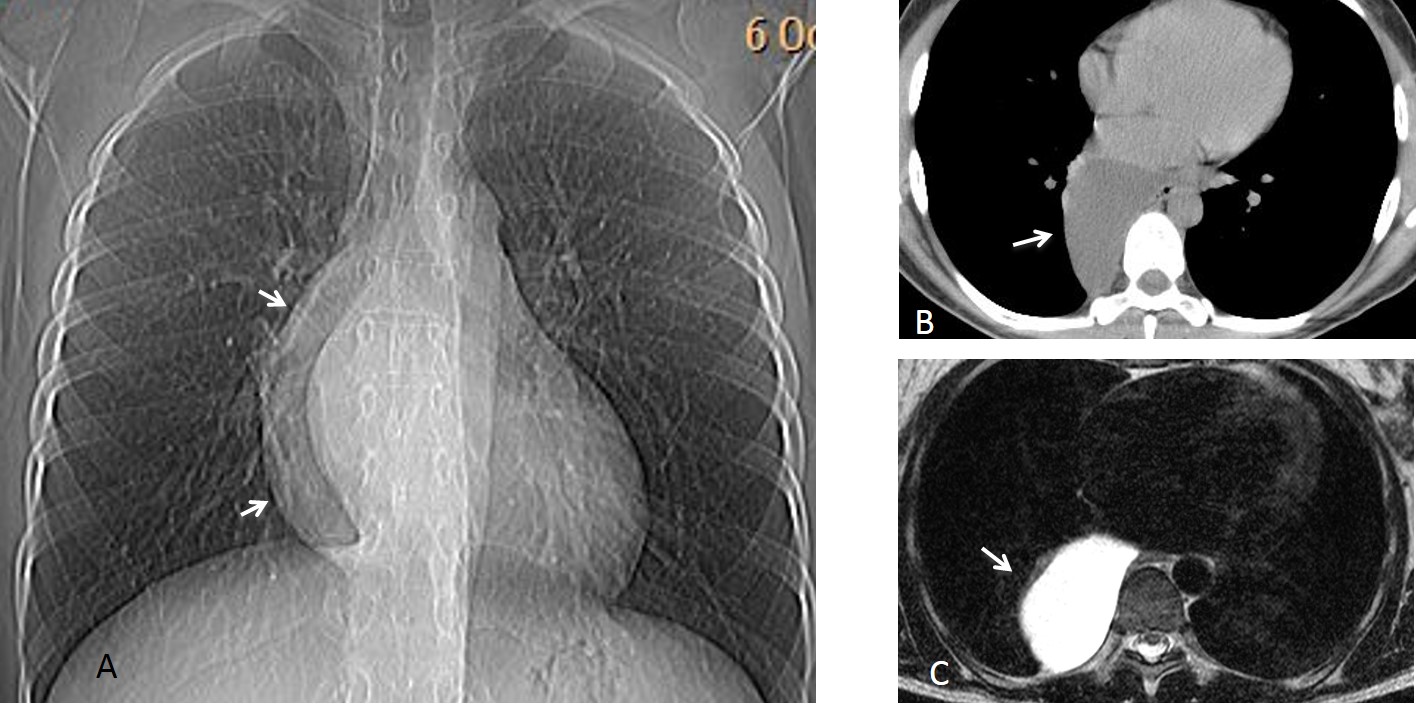
Fig. 7
Fig. 7: 37-year-old woman, asymptomatic. PA chest film shows a posterior mediastinal mass (A, arrows). Unenhanced axial CT depicts a posterior low-density lesion (B, arrow). MRI confirms a cystic lesion (C, arrow), probable neurenteric cyst. Patient refused surgery.
Lateral meningocele refers to herniation of the leptomeninges through a defect in the vertebral foramen. It is usually found in neurofibromatosis. Lateral meningocele appears as a cystic lesion associated with vertebral defects. MRI confirms the cystic nature of the lesion and the connection with the spinal canal (Fig. 8).
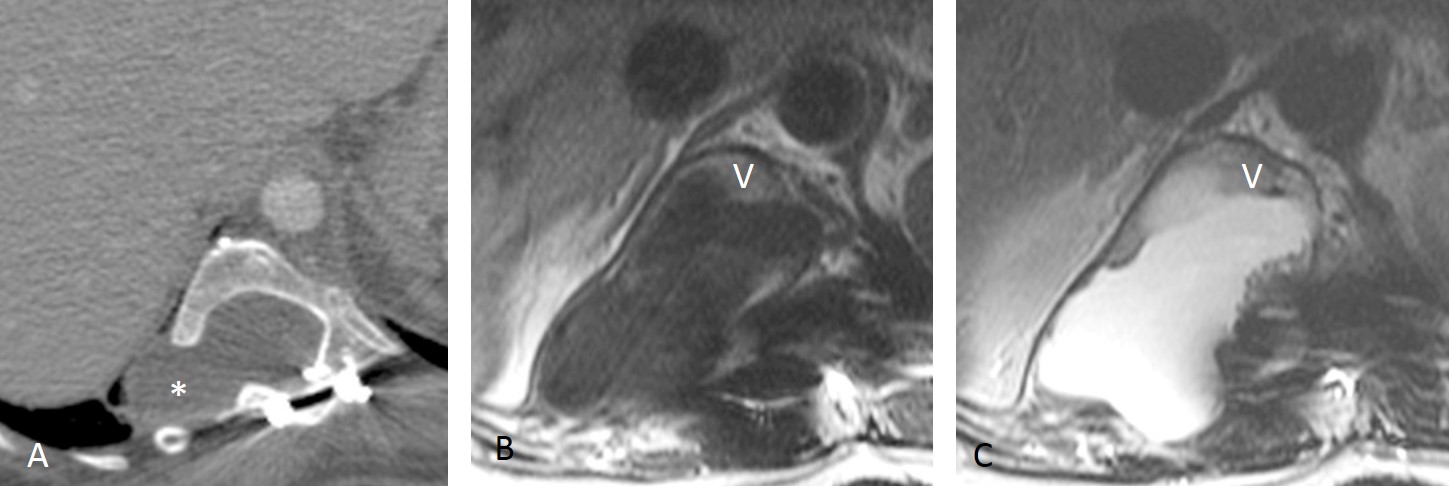
Fig. 8
Fig. 8. Lateral meningocele in a patient with neurofibromatosis. Axial CT shows a low density lesion (A, asterisk) with widening of the neural foramina. MRI (B and C) confirms the presence of liquid which communicates freely with the spinal canal (V, vertebra).
The second most common processes in the posterior mediastinum arise from the spine: tumours (primary or metastatic) or infection (spondylitis), both of which may be accompanied by a soft tissue mass. Tumours affect the vertebral body, whereas infection narrows the disk space, and shows bilateral paravertebral soft tissue enlargement (Figs. 9 and 10).
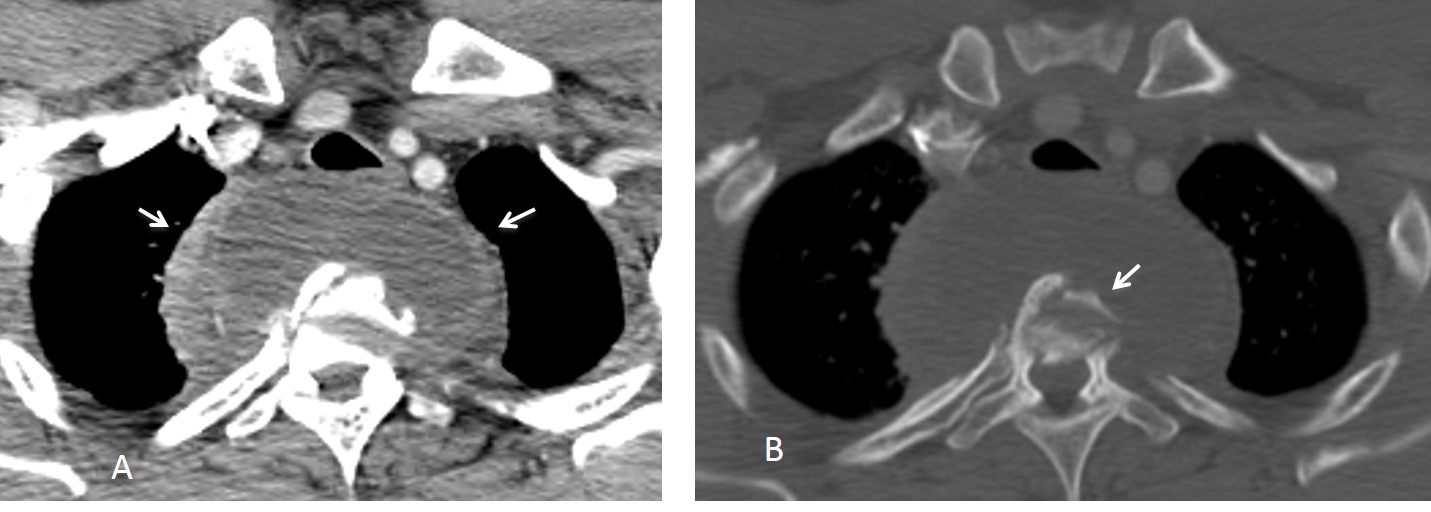
Fig. 9
Fig. 9. Tuberculous spondylitis with a large fluid-containing abscess (A, arrows) that pushes the trachea forward. There is marked vertebral body destruction (B, arrow).
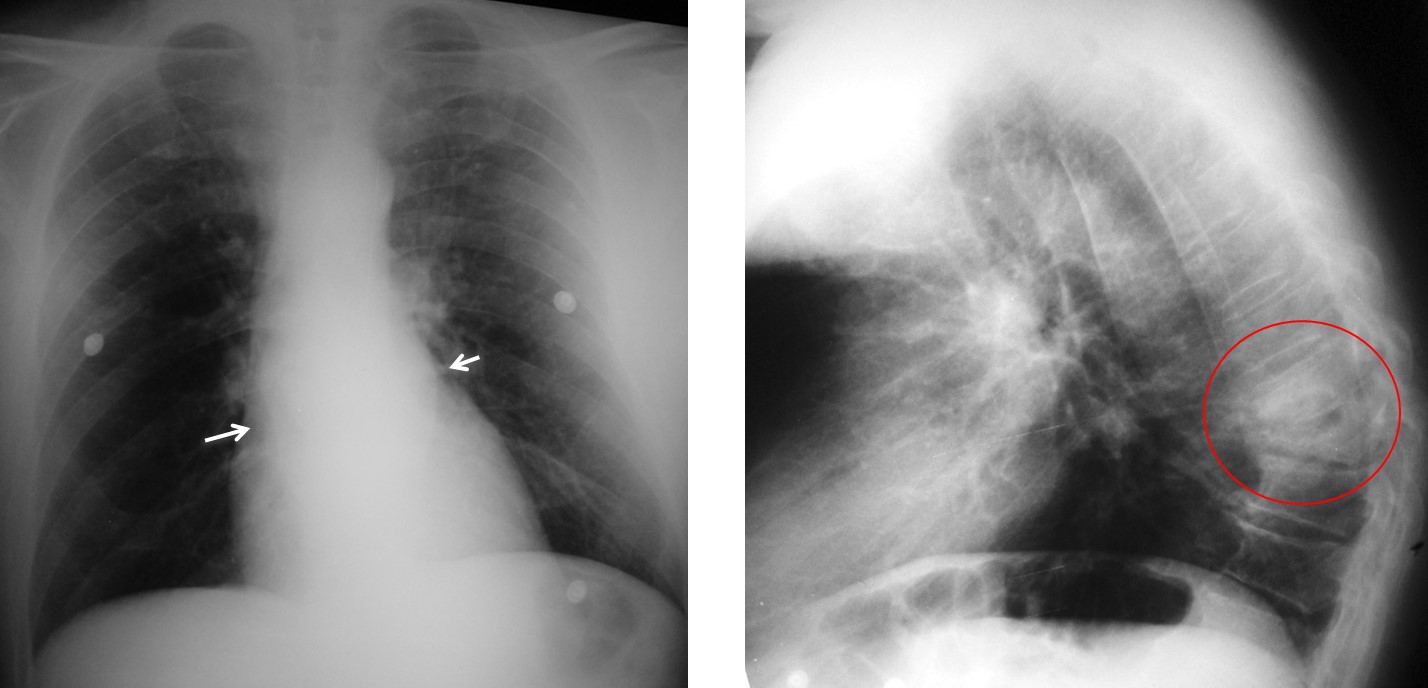
Fig. 10
Fig. 10: 54-year-old patient admitted with severe back pain lasting several weeks. Initial portable film shows widening of the paraspinal lines (A, arrows). A lateral film taken days later shows D9 collapse and destruction of the superior disk space (B, circle).
Coronal and sagittal CT views (C and D) show marked destruction and sclerosis of D8 and D9 with a paravertebral soft tissue mass (C, arrows). The D8-D9 space is destroyed. Pyogenic spondylitis.
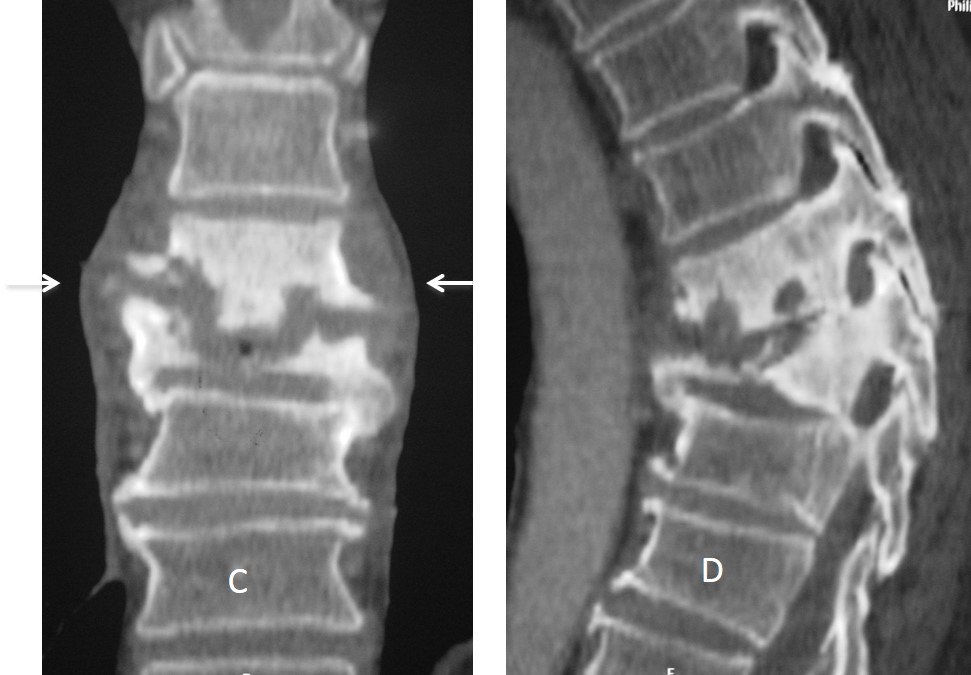
Fig. 10 C&D
Another cause of posterior mediastinal mass is Bochladeck hernia (Fig. 11), which appears on CT as a fatty mass of the posterior mediastinum. CT confirms the discontinuity of the diaphragm. A much rarer cause of posterior fatty mass is extramedullary hematopoiesis.
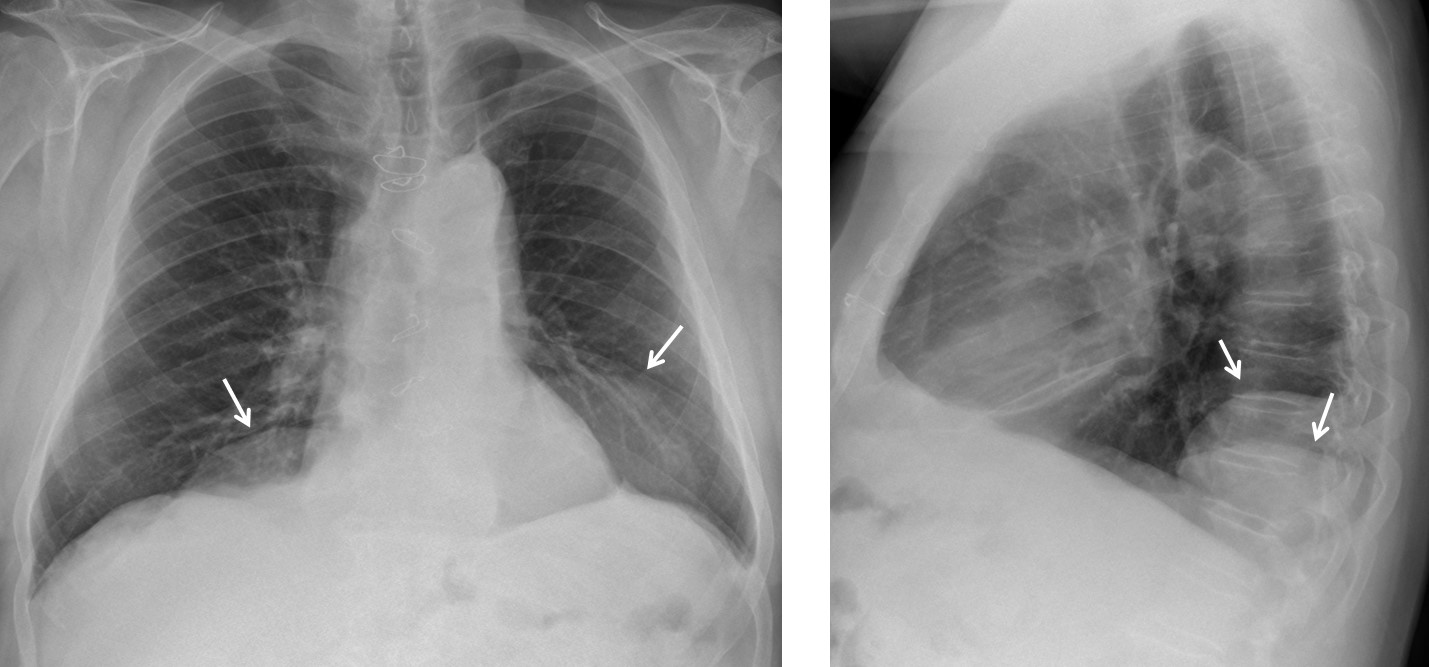
Fig. 11
Fig. 11. In this 72-year-old man, chest radiographs show bilateral masses in both posterior costophrenic angles (A and B, arrows).
Coronal and sagittal CT confirm the presence of bilateral herniated abdominal fat (C and D, white arrows) through posterior discontinuities of the diaphragm (C and D, red arrows).
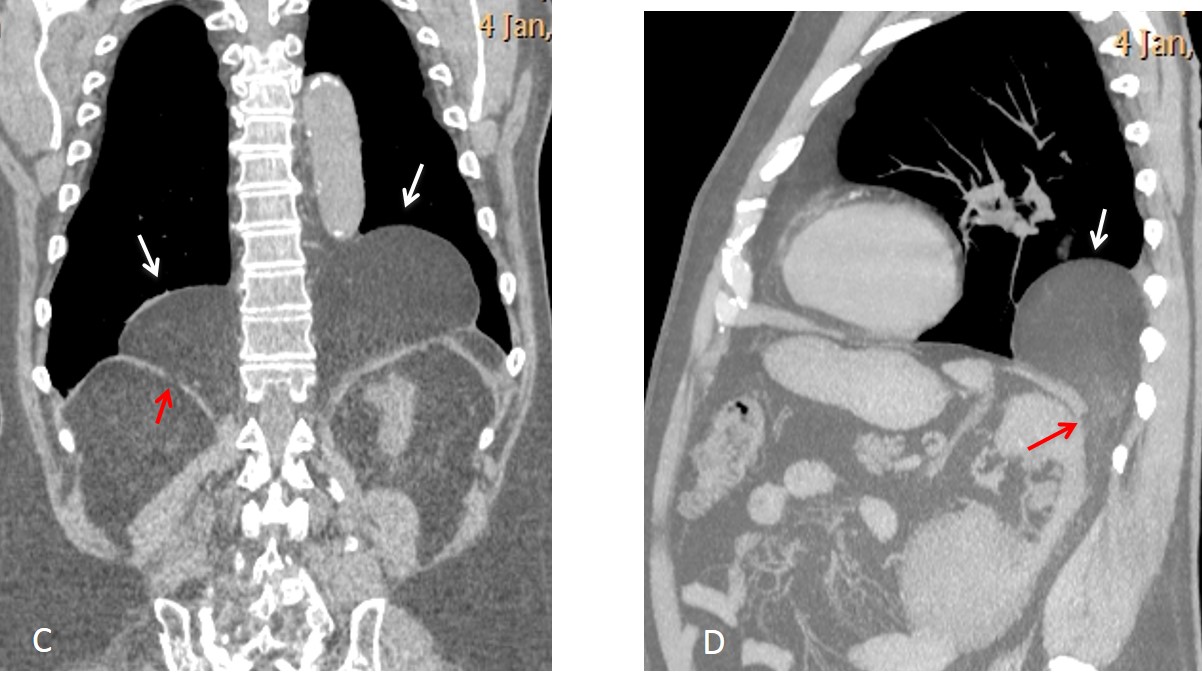
Fig. 11 C&D
Posterior lymph nodes or dilated azygos/hemiazygos veins are another cause of posterior mediastinal lesions, seen as widening of posterior inferior mediastinal lines (Fig. 12).
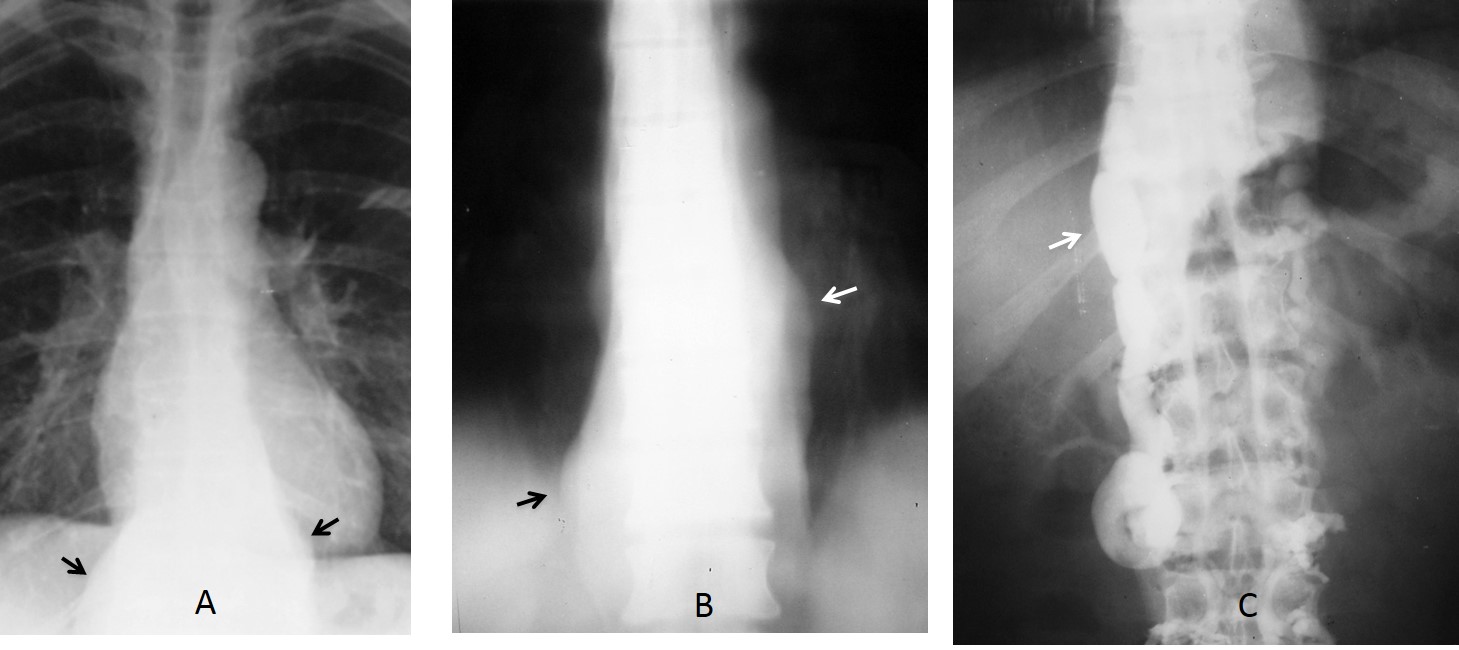
Fig. 12
Fig. 12: two patients with widening of inferior paramediastinal lines, secondary to lymphoma (A, arrows) and dilated azygos and hemiazygos vein (B and C, arrows).

Follow Dr.Pepe’s Advice:
1. Most posterior mediastinal masses are neurogenic tumours.
2. Two thirds of them show low attenuation on CT. MRI is indicated to exclude cystic lesions and investigate spinal canal invasion.
3. Cystic lesions are uncommon in the posterior mediastinum.
4. The second most common etiologies of posterior mediastinal masses are spinal tumours and infections.


The iris heterochromia suggests me neurofibromatosis therefore it may be neurogenic tumour?
Moreover it is not water density in CT so i discard the other two options.
Lisch nodules NF1
Quote from the NEJM: “Lisch nodules are melanocytic hamartomas that appear as well-defined, dome-shaped elevations projecting from the surface of the iris and are clear to yellow or brown”. Does this patient have Lisch nodules?
NO !
Branchial cyst
She didn’t come for her eyes that means is something not acquired recently.
the mass extends above the superior clavicle on the face view so it is located either in the neck or in the posterior mediastinum.
on CT the mass it looks like solid from the neck to the mediastinum
Lisch nodules NO
Waardenburg syndrome NO
Congenital Horner’s syndrome ? but we don’t have all the symptoms of Horner’s syndrome
This case was diagnosed by the resident searching the web. Of course, you have to look for the right information. This is why it is important to make a correct interpretation of the findings.
paraganglioma ?
schwannoma ?
It is probably a lesion of the posterior mediastinum. I go for lymphocele.
..eterocromia, ma anche mosaicismo somatico occhio dx, da S,di Claude-B-Horner, per neuroblastoma toracico.
Cervicotoracic sign. Means most probably the mass is in posterior medistnium. Most peobably neurogenic tumor. Schwanoma with iris color change … Will go for NF 1.
It’s Thursday evening and time for recognition. Congratulations to Cocotet, who was the very first to suugest the diagnosis and to Genchi Bari, who made the exact diagnosis.
Full information tomorrow.
Have a nice weekend.
….grazie PROFESSORE…..NB.il Bari ANCHE in serie B va male…Anche per il BARCA i tempi bui passeranno !!!!!