Dr. Pepe’s Diploma Casebook: Case 65 – SOLVED!
Dear Friends,
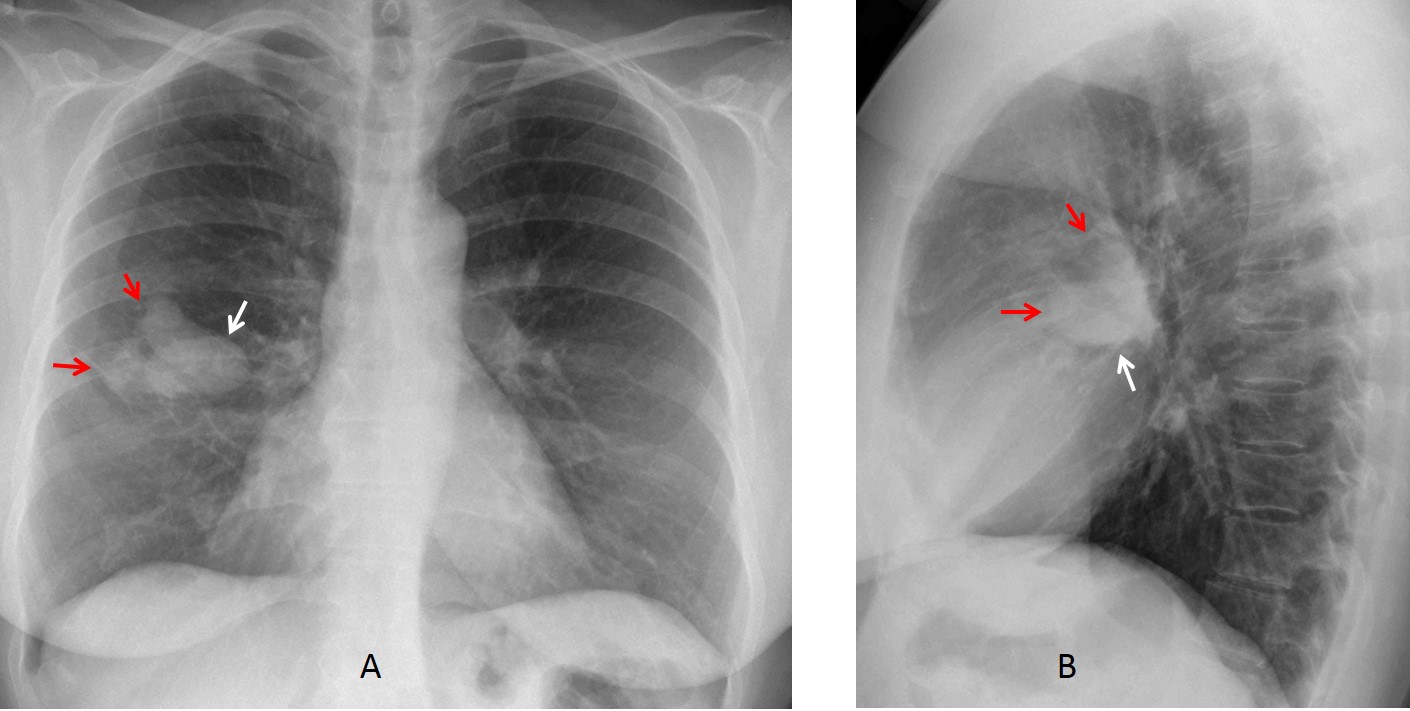
Radiographs of this week’s case belong to a 55-year-old woman, referred to our hospital for percutaneous biopsy of a lung lesion. Leave your thoughts and diagnosis in the comments section below and come back for the answer on Friday.
Diagnosis:
1. Carcinoma
2. Tuberculosis
3. Congenital lesion
4. Any of the above


Findings: Radiographs show an ovoid nodule (A and B, white arrows) with two finger-like projections (A and B, red arrows). The appearance is suggestive of mucus impaction. This finding can occur in carcinoma, as well as TB and congenital lesions. Hence, the correct answer is: 4. Any of the above.
Coronal and axial CT confirm the mucus impaction (C, arrow), which is surrounded by an area of emphysematous lung with air trapping on expiration (D and E, circle). The CT appearance is suggestive of a congenital lesion. Bronchoscopy demonstrated absence of a segmental bronchus.
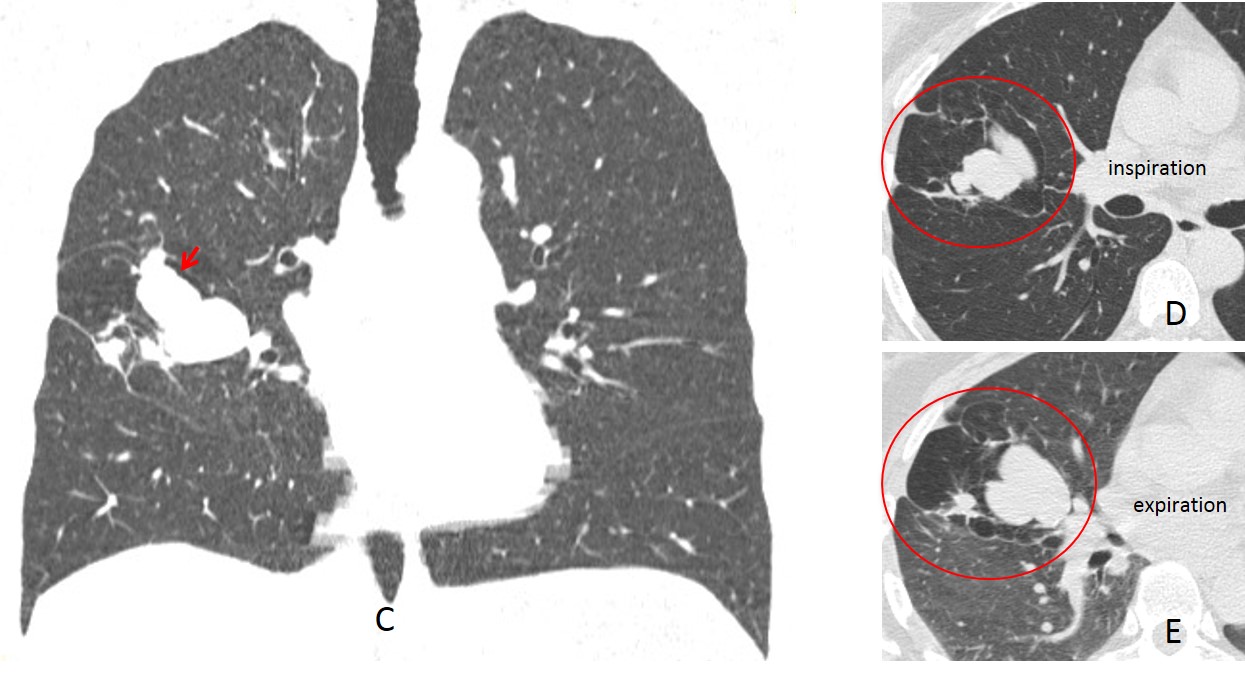
Final diagnosis: congenital bronchial atresia with mucus impaction.
This case is presented to discuss mucus impaction. It occurs when dilated bronchi fill with mucus, giving the typical appearance of tubular or branching opacities that resemble fingers (gloved finger sign). This sign may be visible in plain films, but it is better recognised on CT, where it may present different densities. The most common is low-density mucus, which may be mixed with air (Fig. 1, A and B). The mucus may also have areas of increased opacity (Fig. 1 C), a characteristic of allergic aspergillosis, or show calcification (Fig. 1, D), which suggests previous tuberculosis.
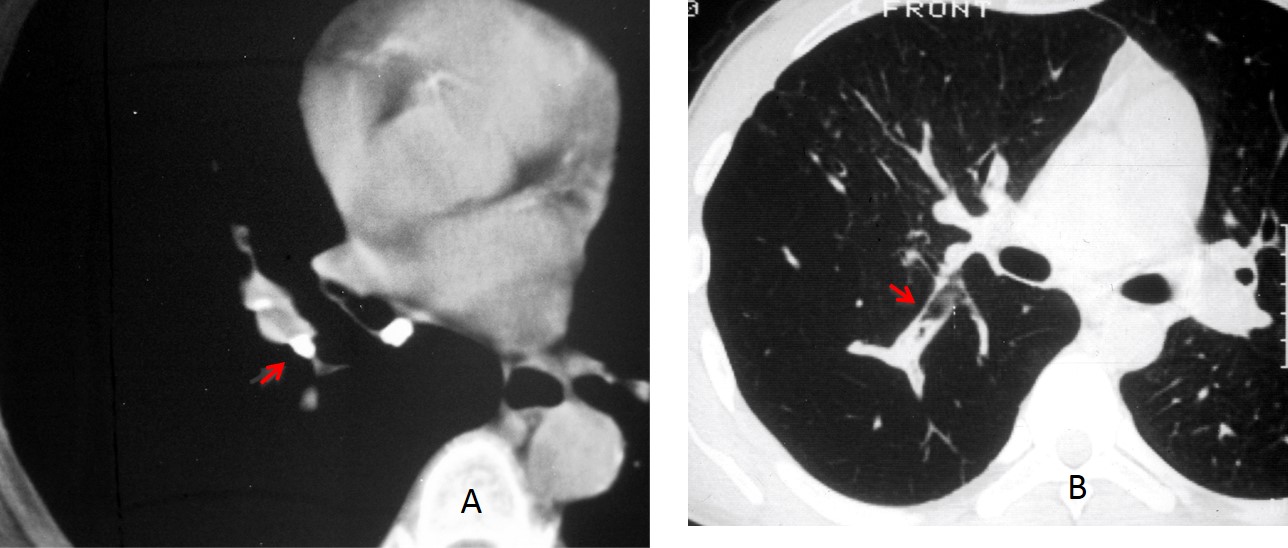
Fig 1
Fig. 1. Image A shows a broncolith (A, arrow) obstructing a mucus-filled bronchus. Image B shows a bronchus partially filled with mucus and air (B, arrow) in a patient with bronchial atresia.
Unenhanced coronal CT in a patient with allergic aspergillosis shows a large mucus impaction (C, white arrow), with an area of increased density (C, red arrow). Image D depicts a branching calcified impaction (arrows) in a patient with previous TB.
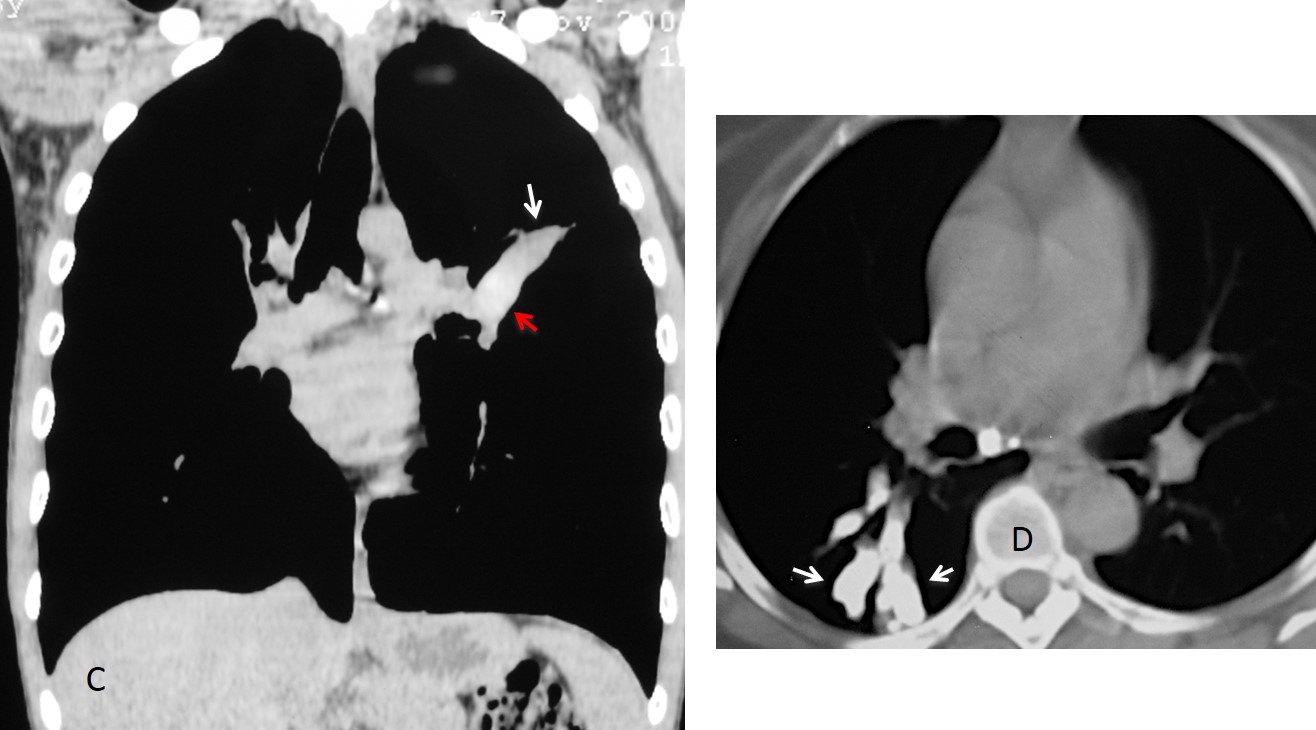
Fig. 1
An initial approach to mucus impactions divides them into localized and widespread. The first are secondary to segmental bronchial obstruction. Widespread impactions are non-obstructive and related to respiratory diseases that cause bronchiectasis and thick mucus.
Localised (obstructive) mucus impaction affects segmental bronchi. Collateral ventilation maintains lung aeration and renders the impaction visible over a background of aerated lung. It is important to note that when the obstruction occurs in a lobar bronchus, lobar collapse ensues. In these cases, the bronchi are seen as an air/mucus bronchogram (see Diploma Casebook case #62).
Primary or metastatic malignant endobronchial tumours are the first cause of mucus impaction. The prevalence of bronchogenic carcinoma makes it the most common cause of mucus impaction in clinical practice (Fig. 2).
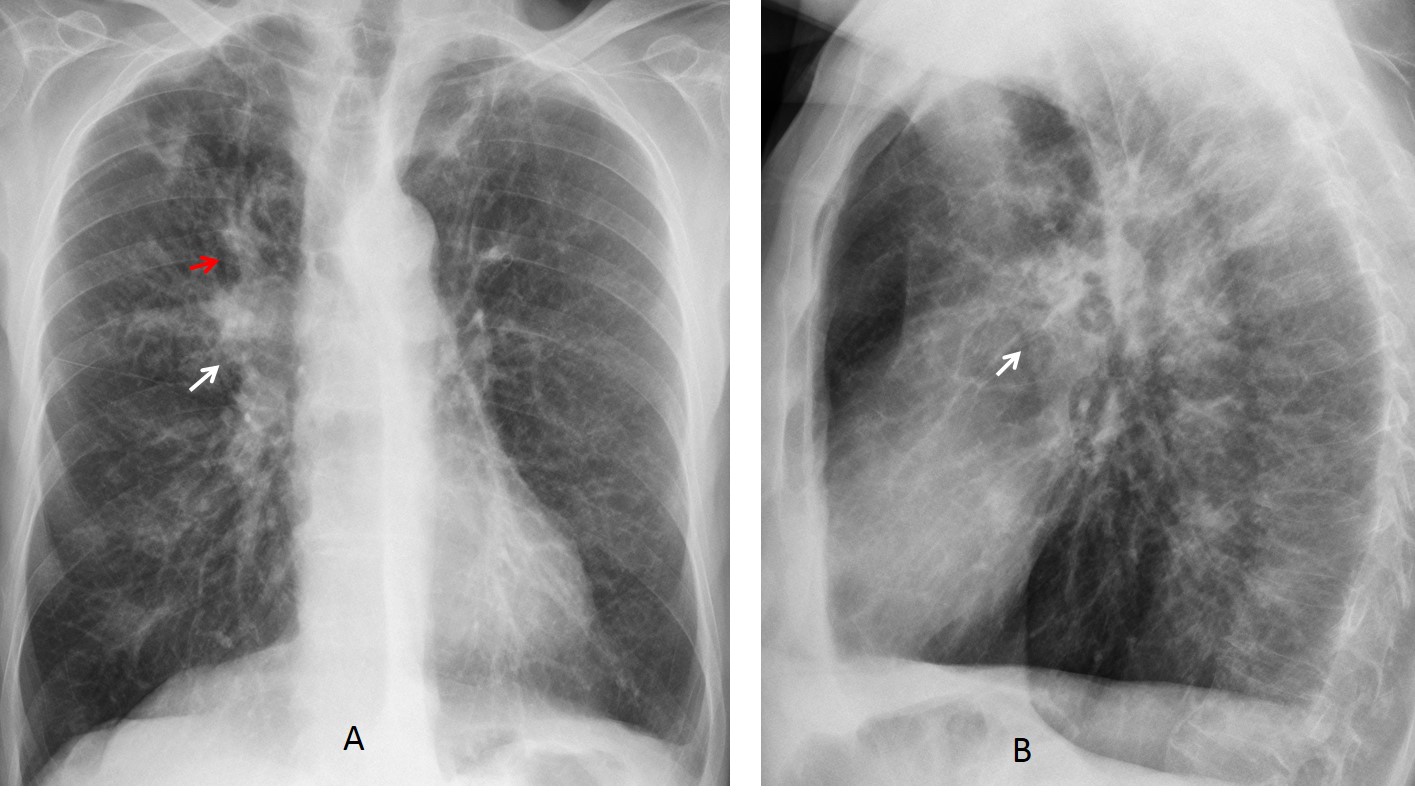
Fig. 2
Fig. 2: 56-year-old patient with carcinoma, visible as a mass in the right hilum (A and B, white arrows). Mucus impaction is present (A, red arrow).
Enhanced coronal and sagittal CT confirms the hilar mass (C and D white arrows) as well as the mucus impactions (C and D, red arrows), which are easily distinguished from the enhanced vessels.
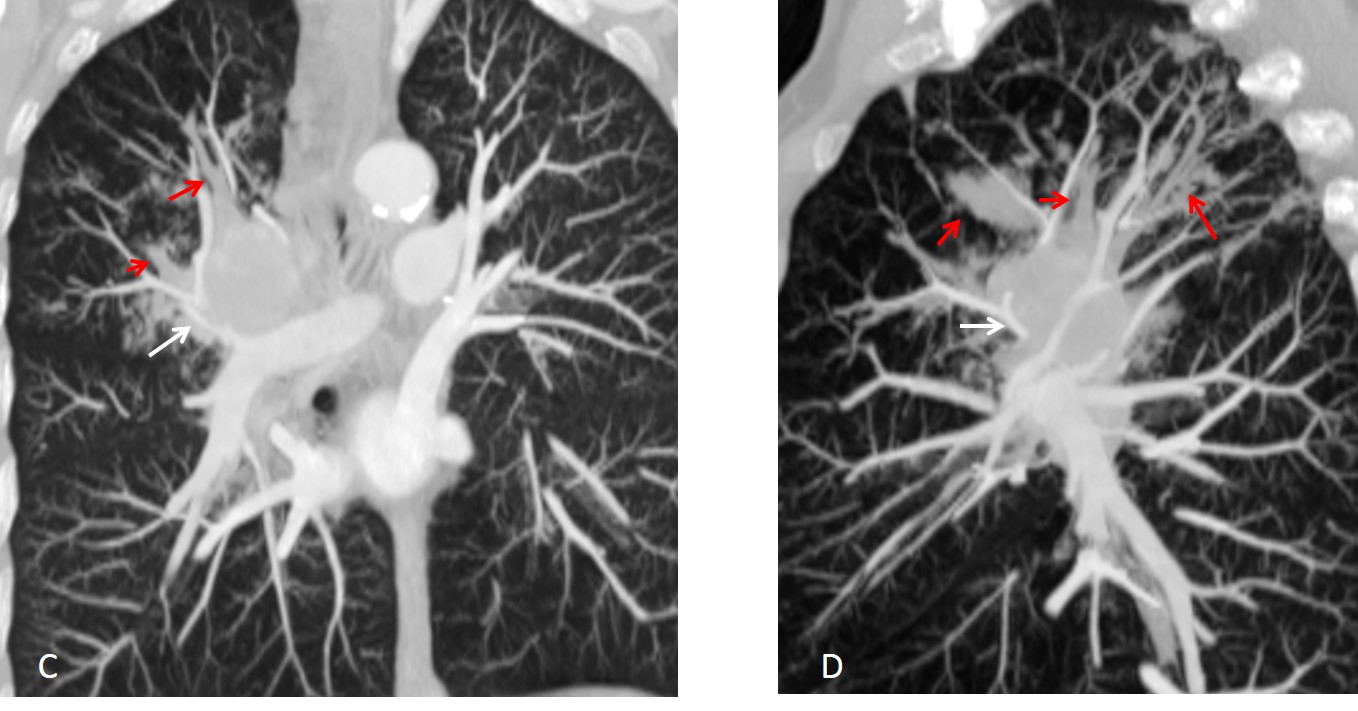
Fig. 2
Carcinoids are low-grade endobronchial neuroendocrine neoplasms. About 80-90% are located in the bronchial tree. Peripheral tumours are visible as round masses which may be accompanied by distal mucus impaction (Fig. 3).
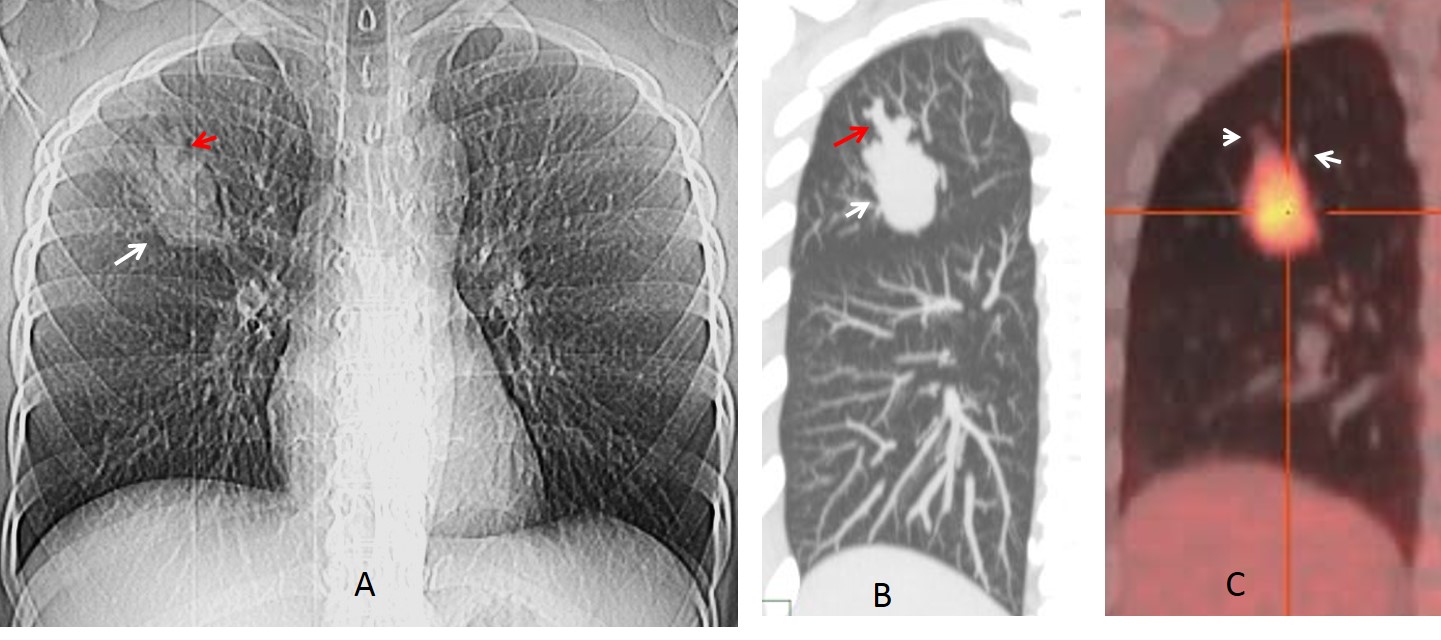
Fig. 3
Fig. 3: 42-year-old man with carcinoid presenting as a lung mass (A and B, white arrows). There are distal mucus impactions, visible in the scout film and sagittal CT (A and B, red arrows). PET-CT shows uptake of the mass, but no uptake of the impactions (C, arrows).
Hematogenous endobronchial metastases occur in malignancies arising in the colon, breast and kidney, as well as melanoma. On imaging study they simulate a primary lung tumor and may give rise to bronchial impactions (Fig. 4).
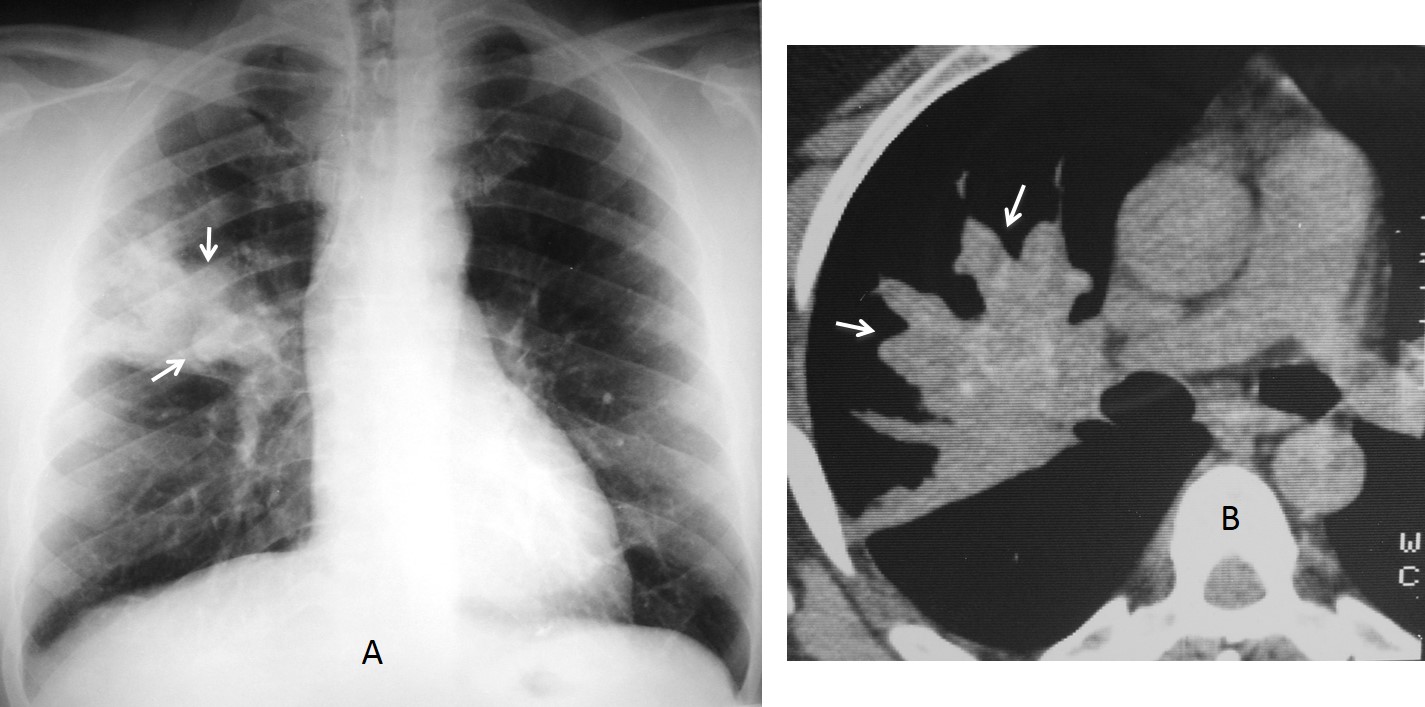
Fig. 4
Fig. 4: 54-year-old man with mucinous carcinoma of the colon and endobronchial metastases to the posterior segment of RUL. Note the impactions in the PA chest film (A, arrows), which are better seen on unenhanced axial CT (B, arrows). There are calcifications within the tumour.
Inflammatory granulomatous disease (TB in our setting) may cause bronchial stenosis. Caseum accumulates in the obstructed bronchus, resulting in bronchial impaction. Calcification is not infrequent in these cases (Figs. 5 and 6).
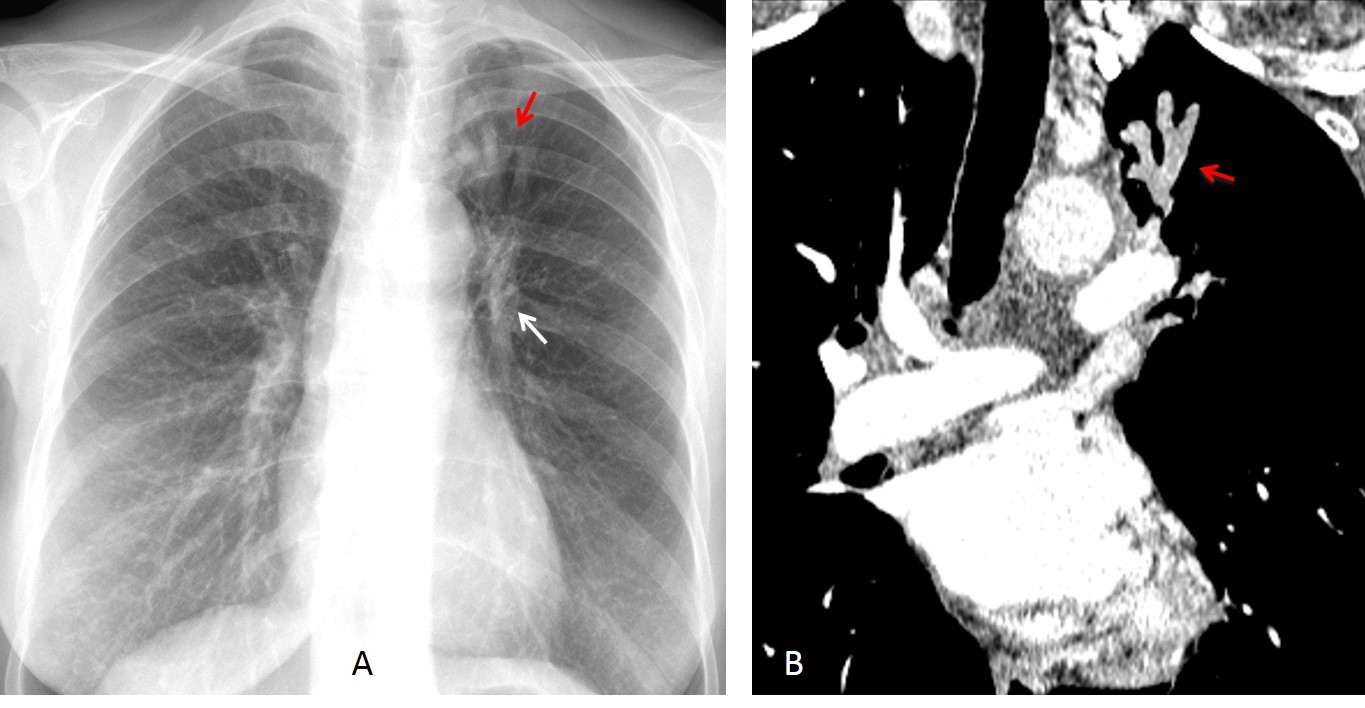
Fig. 5
Fig. 5: 43-year-old woman with previous TB. There is marked left hilar retraction (A, white arrow). Gloved fingers are seen in the LUL (A, red arrow). Coronal CT gives a better depiction of the impaction (B, red arrow). Note flecks of calcium within the bronchi.
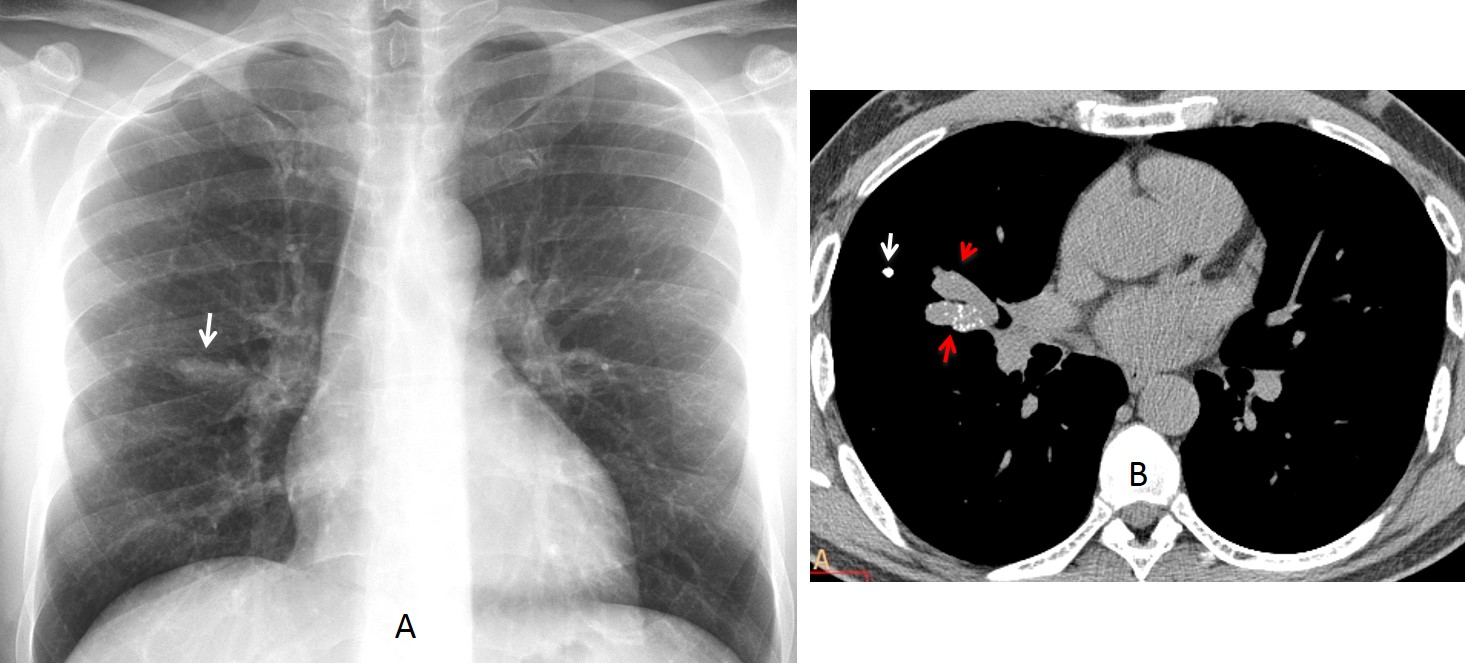
Fig. 6
Fig. 6: PA chest film in a 52-year-old man showing a bronchial impaction (A, arrow). Unenhanced axial CT confirms the impaction (B, red arrows) and depicts calcium in the bronchus. Bronchoscopy demonstrated changes compatible with healed TB. Note the calcified granuloma in the periphery of the lung (B, white arrow). No change after two years of follow-up.
In my experience, congenital bronchial atresia is not an infrequent cause of mucus impaction. In addition to the gloved fingers sign, air trapping helps to identify this entity (Fig. 7). Bronchoscopy confirms the diagnosis by demonstrating absence of a segmental bronchus. Other non-malignant causes of mucus impaction are foreign bodies, broncholiths, and benign tumours.
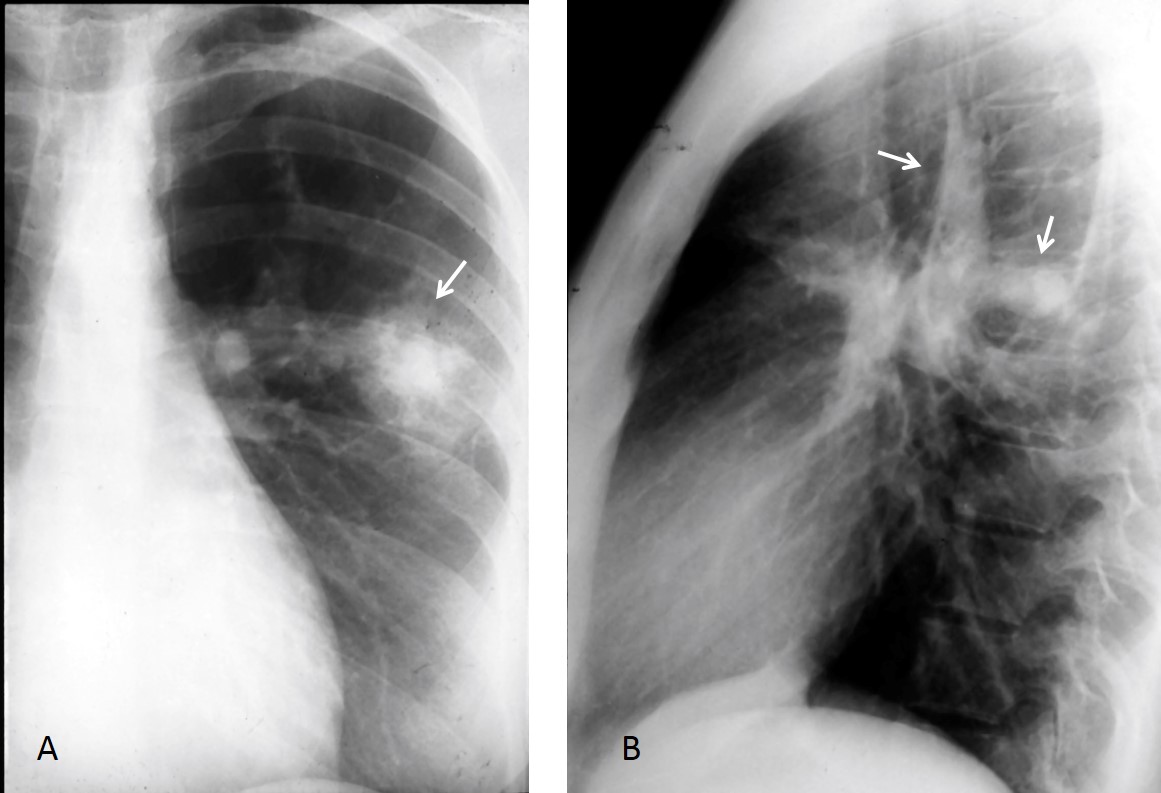
Fig. 7
Fig. 7: 21-year-old man, asymptomatic. PA chest film shows a nondescript infiltrate in the LUL (A, arrow) and increased lucency of the upper lung. Lateral view shows obvious mucus impactions (B, arrows). Axial CT confirms the impactions (C, arrows) and emphysema of the apical-posterior segment of LUL. Diagnosis: congenital bronchial atresia.
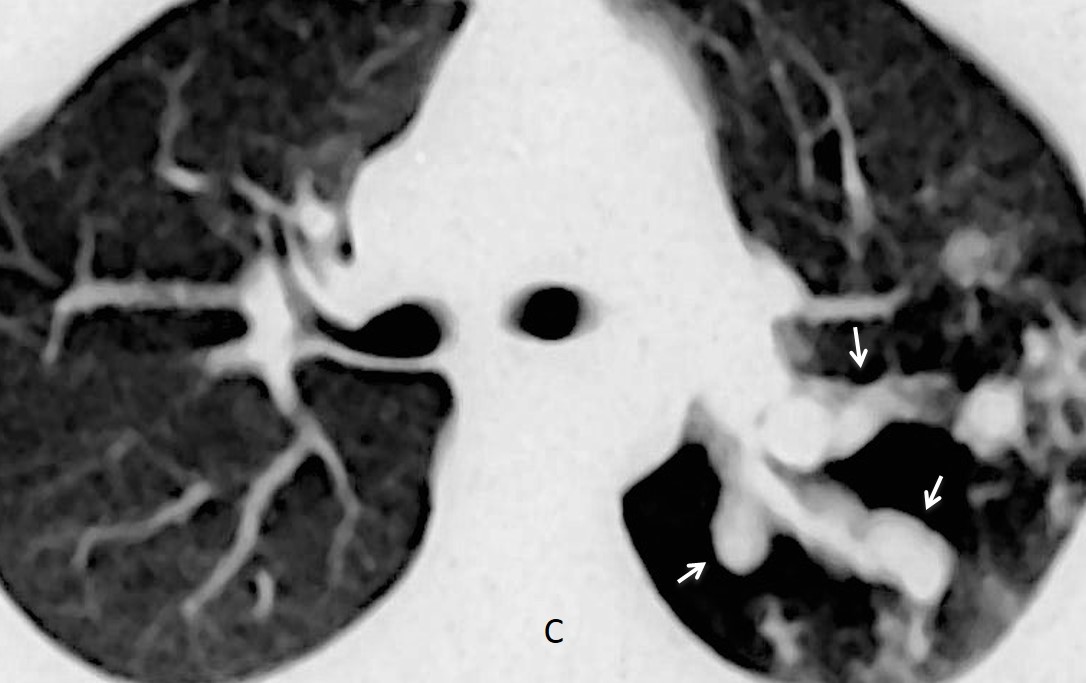
Fig. 7
Multiple areas of mucus impaction are usually non-obstructive and related to pulmonary conditions that cause bronchial dilatation and inspissated mucus. Asthma and/or allergic aspergillosis are the most common cause of multiple areas of mucus impaction (Fig. 8). In allergic aspergillosis it is not uncommon to find areas of high-density mucus, a very reliable sign to suggest the diagnosis (Fig. 9).
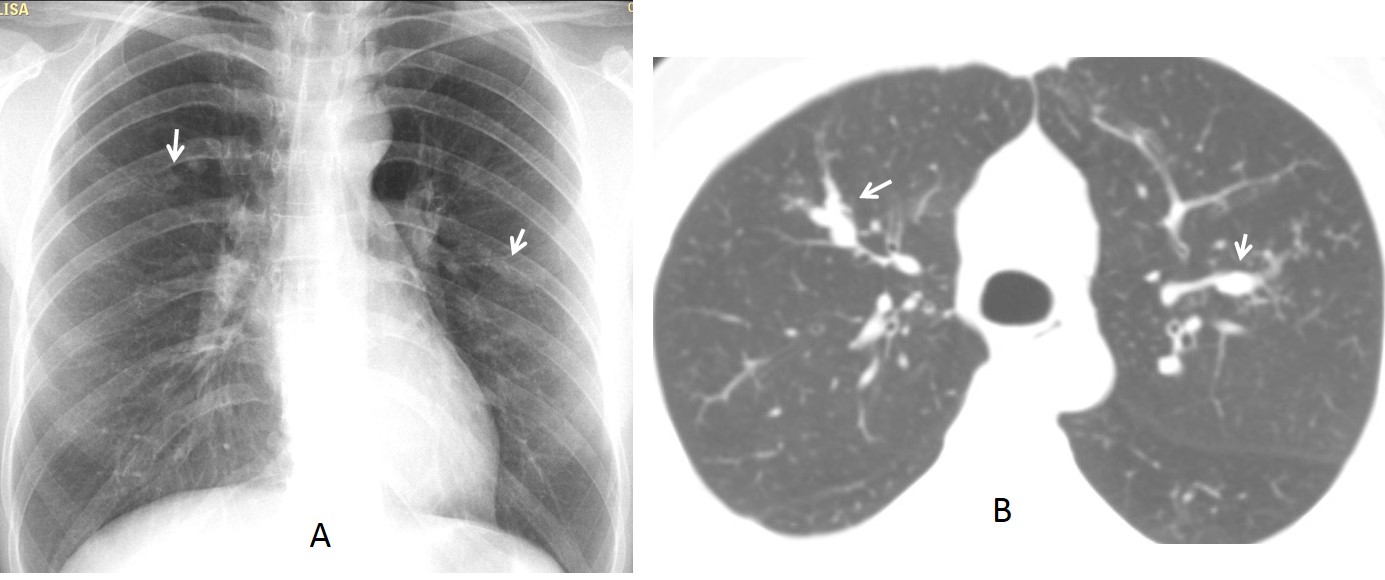
Fig. 8
Fig. 8: 40-year-old woman with asthma attacks. PA chest film shows faint areas of increased opacity (A, arrows) that correspond to mucus impactions in the axial CT (B, arrows). Diagnosis: allergic aspergillosis.
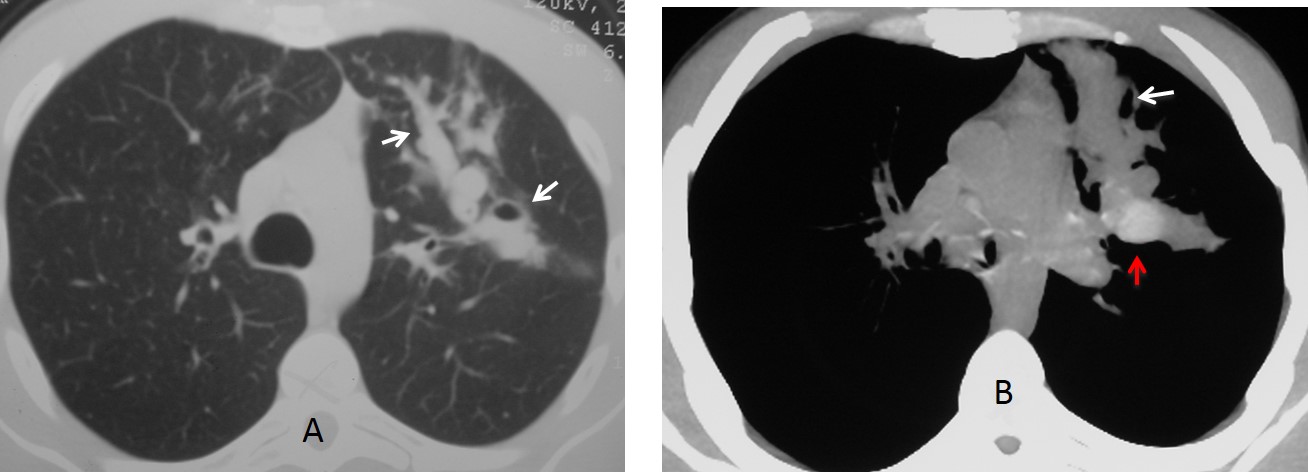
Fig. 9
Fig. 9: Patient with allergic aspergillosis and impactions (A and B, white arrows). Note the area of increased opacity in B (red arrow), typical of this entity.
Cystic fibrosis is another cause of disseminated impaction. Chronically dilated bronchi are usually air-filled and coexist with mucus-filled bronchi. Note associated pulmonary emphysema.
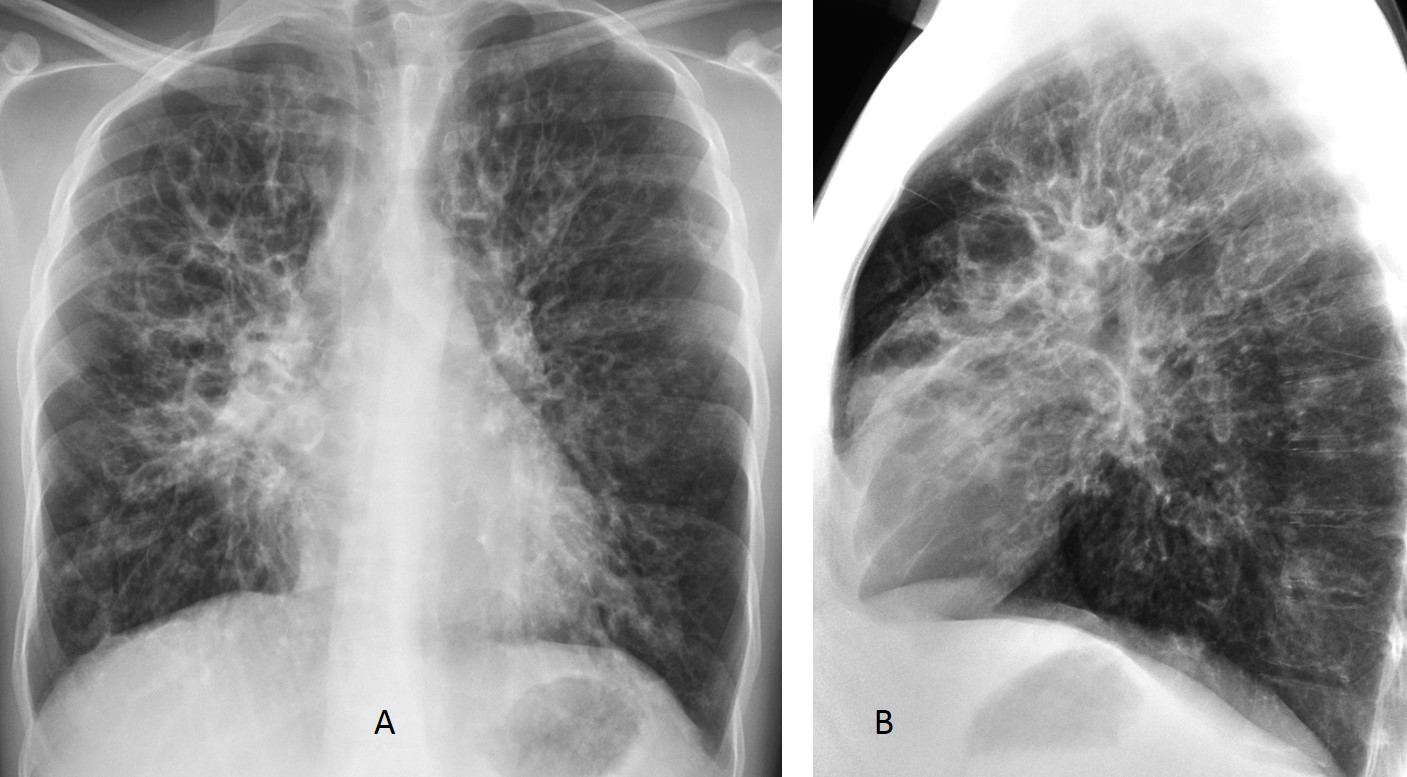
Fig. 10
Fig. 10: 19-year-old man with cystic fibrosis. Chest radiographs depict multiple air-filled dilated bronchi and pulmonary emphysema.
Coronal and sagittal CT show multiple dilated bronchi, most of them filled with mucus and air, and some with mucus impaction (C and D, red arrows).
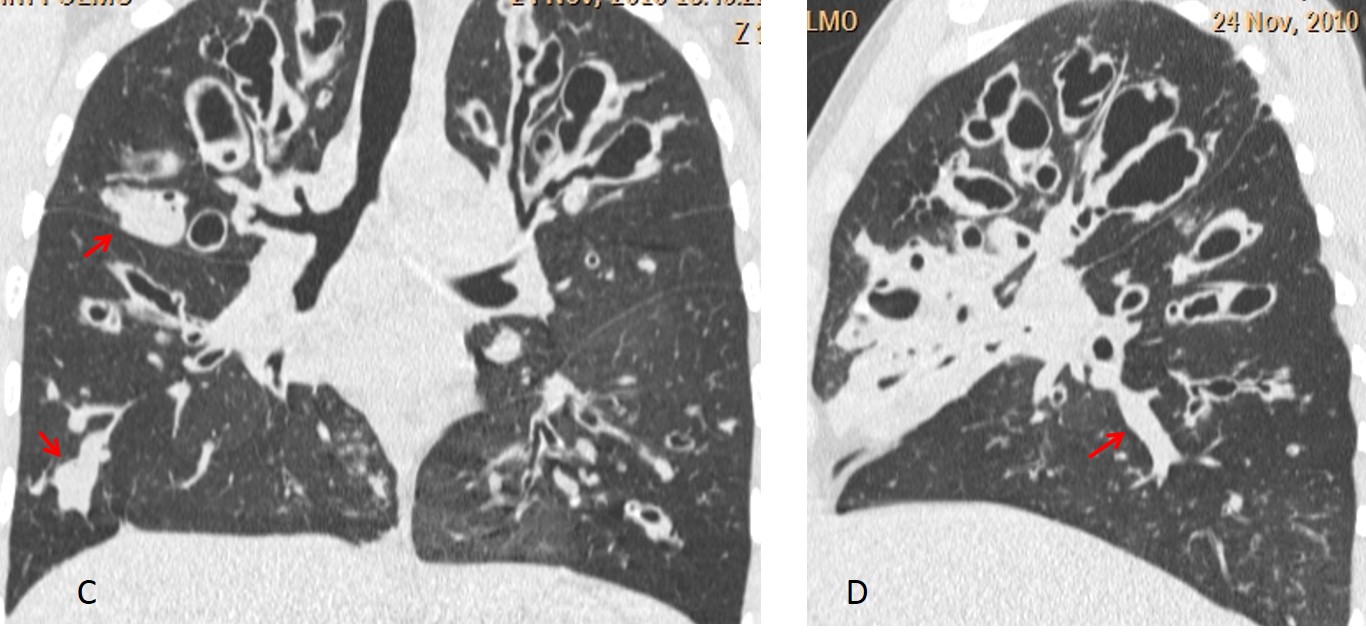
Fig. 10

Follow Dr.Pepe’s Advice:
1. Finger-like opacities are the hallmark of mucus impaction.
2. Localised impactions are secondary to segmental bronchial obstruction. Malignancy is the most common cause.
3. Widespread impactions are related to bronchiectasis and thick mucus: asthma/allergic aspergillosis and cystic fibrosis.
4. Dense mucus impaction suggests allergic aspergillosis


Congenital lesion, but CT I would do mainly for excluding carcinoma. No percutaneous biopsy for now as the lesion may be vascular.
congenital lesion
I think that two important DD are ; AVM or Bronchocele
Well defined, uniform density, branching, and most probably vascular mass, located anterolateral from the right hilum in female aged between 55-60 years old. It seems that she has no symptoms.
The first diagnosis is Pulmonary Arteriovenous Malformations.
Congenital
Lobulated opacity at the right middle lung zone, on lateral view seen superimposed on the hilum, oblong in shape,no air bronchogram ,no calcium could be suggestive of arteriovenous malformation for CT evaluation.
Arteriovenous malformation?
4
Right mid zone tubular branching opacity On frontal radiograph
Retro sternal space shows overlying Tortuous vessel ending on to opacity
Suggest Pulmonary AVM.
.. fare una biopsia polmonare senza fare “prima” una TC? La tc servirà sopratutto a stabilire la natura liquida e-o solida della formazione ed a fare una ricostruzione coronale della lesione…è se fosse una MAV come sostenuto da alcuni, cosa succederebbe ? Penso comunque che la formazione possa essere anche una Bronchiectasia ” a dito di guanto rovesciato”, per intasamento mucoide….resta valida l’ipotesi di un broncocele, ma “isolato” nel parenchima?Saluti da BARI…..
Congenital lesion, most propably AV malformation.
4
AVM
congenital -is the answer
dr.balachandran
AVM
Congenital lesion. Bronchial atresia.
Bronchial atresia
Pulmonary arteriovenous malformation but first a CT is necessary.
If it is an AV malformation, where are the afferent and efferent vessels?
There is not…..
Bronchogenic cyst?
Do bronchogenic cysts have V shape?
mucoid impaction
Anomwlia congenita: Atresia bronquial y broncocele
BRONCHIAL ATRESIA
Finger in glove sign? ABPA
As always, a correct interpretation is the clue to a correct diagnosis. The “V” shape pointing towards the hilum is indicative of mucous impaction. This appearance may occur in the three proposed options. Therefore, the correct diagnosis is 4. All of the above.
To diagnose a congenital lesion, a zone of surrounding hyperlucency is needed (see CT in the answer)
Congratulations to Drs. Ele and CT
and me also 🙂 ….I meant by bronchocele is a mucoid impaction in a broncheole
My apologies. Credit belongs to you, too.
any of the above.Brochocele, mucus impaction