Dr. Pepe’s Diploma Casebook: Case 66 – SOLVED!
Dear Friends,
Today I am feeling magnanimous, because vacation is approaching. I have prepared an easy case of a 75-year-old man with cough and moderate fever. What would you diagnose?
1. Lobar pneumonia
2. Carcinoma
3. Tuberculosis
4. None of the above
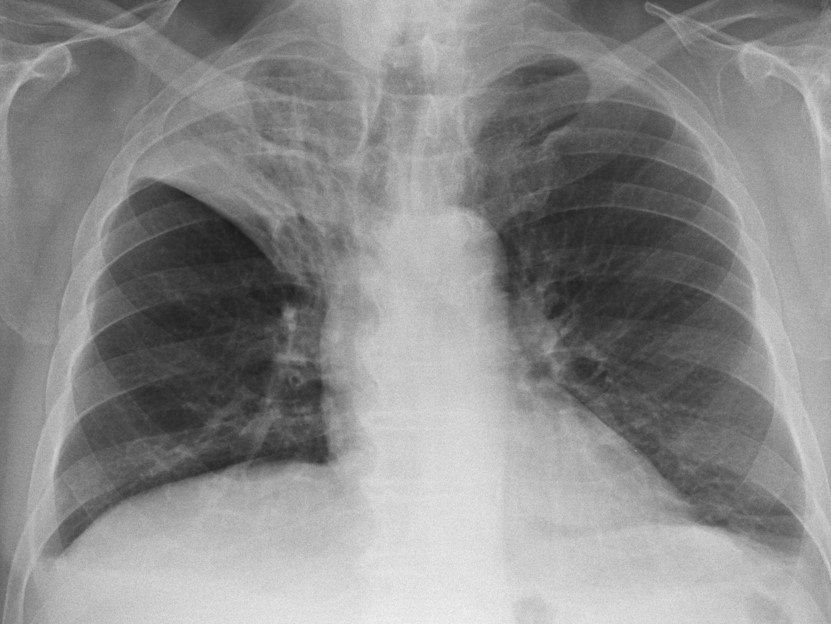
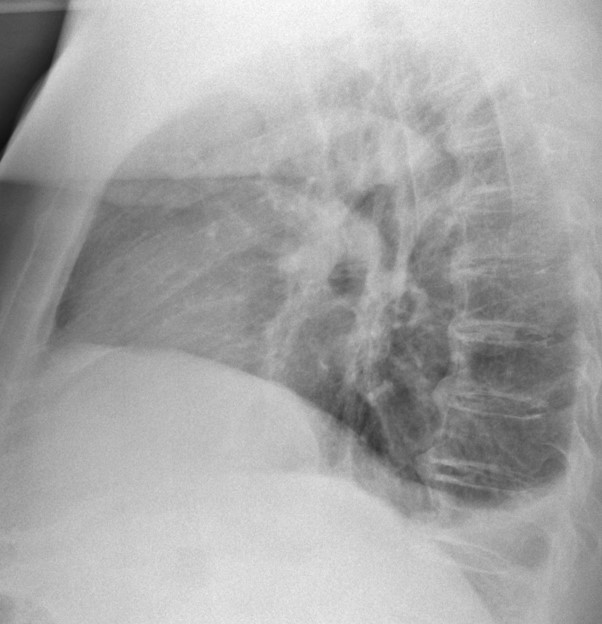
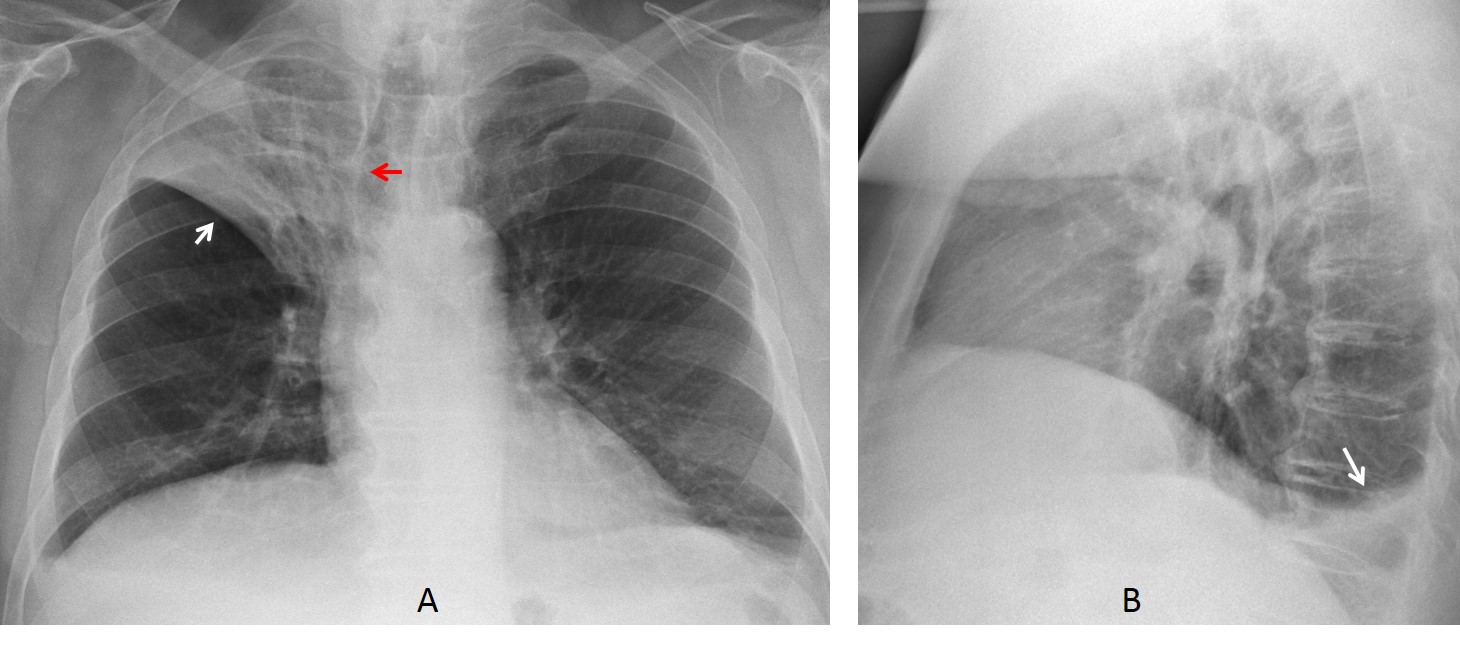
The main findings are seen in the PA radiograph, which shows RUL opacity with moderate elevation of the middle fissure (A, white arrow) and mild tracheal displacement (A, red arrow). There is a small right pleural effusion that is better seen in the lateral view (B, arrow). The findings are consistent with moderate RUL collapse, which is compatible with carcinoma of a RUL bronchus or lobar pneumonia. In this case CT should be done to exclude an endobronchial lesion.
On coronal CT there is no RUL obstruction and no evidence of an endobronchial lesion. A follow-up radiograph taken one month later shows complete resolution of the RUL infiltrate.

Final diagnosis: lobar pneumonia of the RUL
This case is presented to discuss usual and unusual imaging presentations of acute pneumonia. The usual appearance is air-space disease with typical findings of indistinct borders, segmental location, and air bronchogram. An additional diagnostic criterion is rapid disappearance of the infiltrate after treatment (Fig. 1).
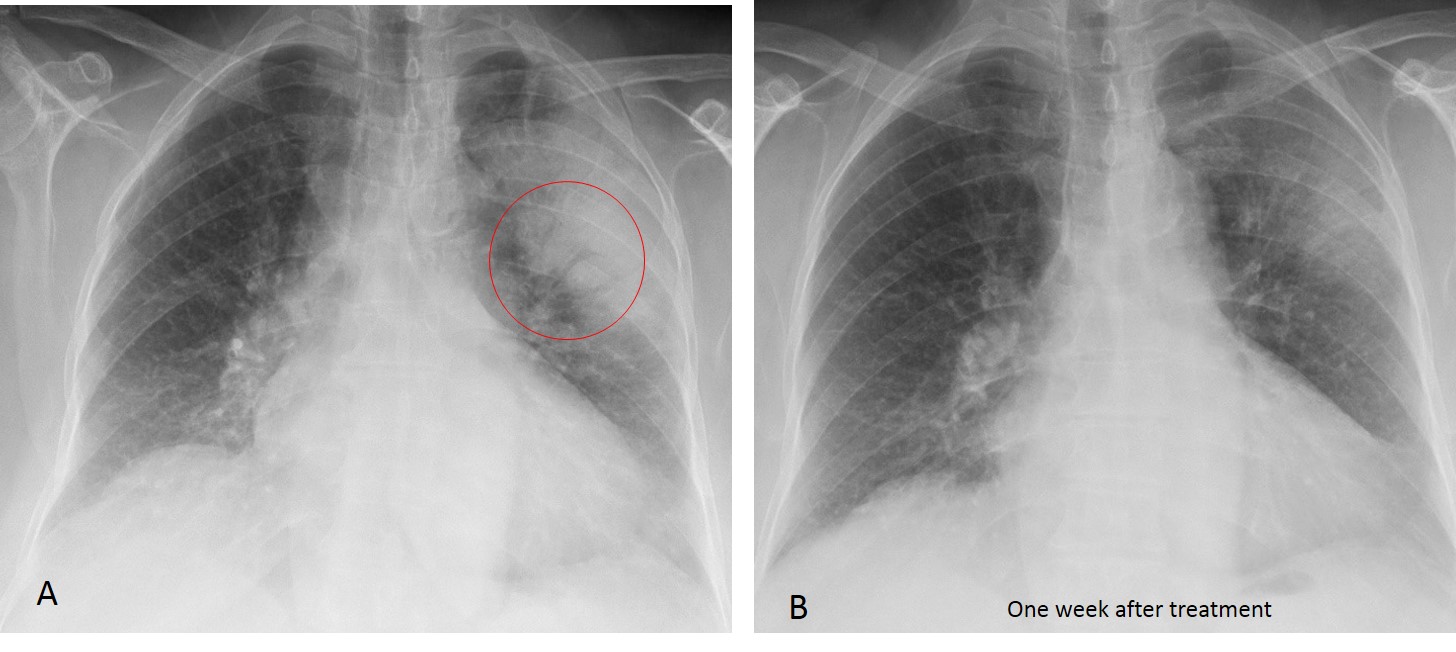
Fig. 1
Fig. 1: 65-year-old man with fever and cough. PA radiograph shows a segmental LUL infiltrate with indistinct borders and an air bronchogram (A, circle). Radiograph after one week (B) shows marked improvement.
Acute pneumonia that does not present this typical appearance may generate diagnostic problems. In my experience, the most common ones are related to the unusual appearance of the infiltrate (
round and lobar pneumonia), recurrence in the same location (recurrent pneumonia), and failure to visualise the infiltrate (occult pneumonia).
Round pneumonia mainly occurs in children, but can also develop in adults; it represents around 1% of coin lesions. The appearance is related to centrifugal spread of the infection, aided by underdeveloped pores of Kohn and channels of Lambert. It can vary from a small to large mass with ill-defined borders. Less than 20% have air bronchograms. Recognizing round pneumonia is important to avoid confusion with other processes, mainly lung carcinoma (Figs. 2 and 3).
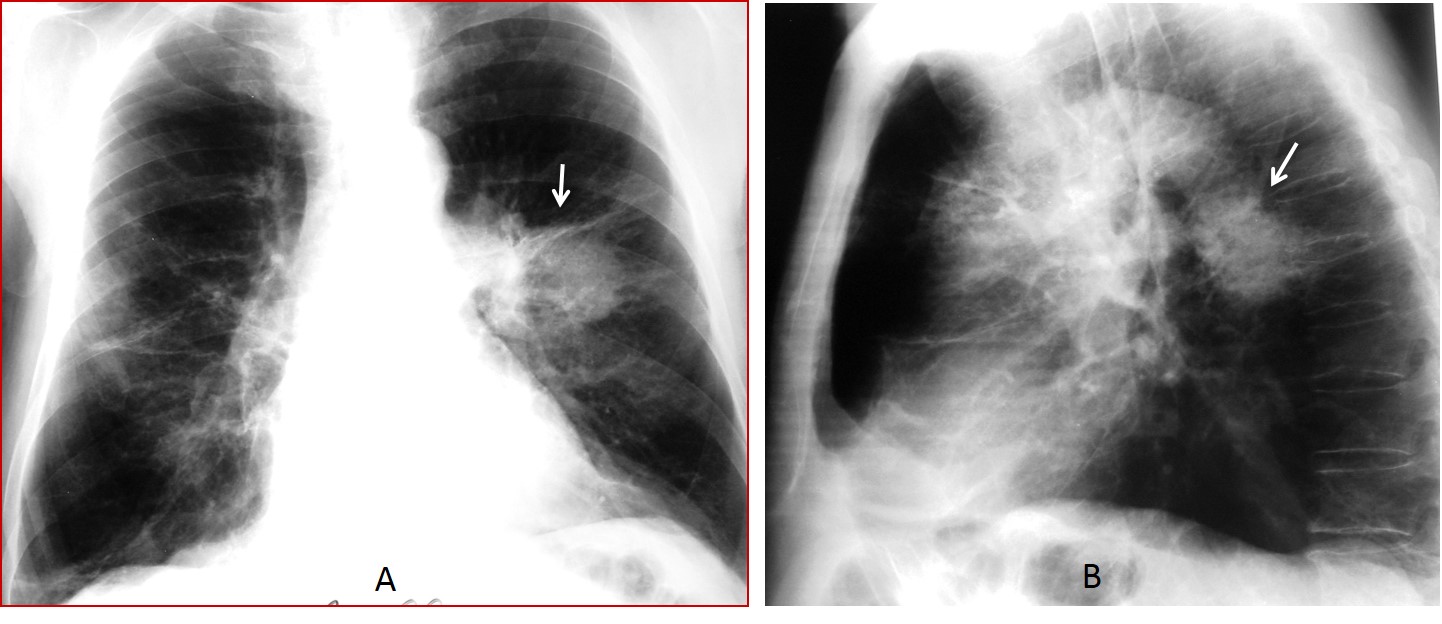
Fig. 2 A&B
Fig. 2: 68-year-old smoker with cough and high fever. Chest radiographs show a round lesion in the left lung suspected to be carcinoma (A and B, arrows). Because of the fever, antibiotic treatment was started. Seven days later the round lesion has disappeared (C and D). Diagnosis: round pneumonia.
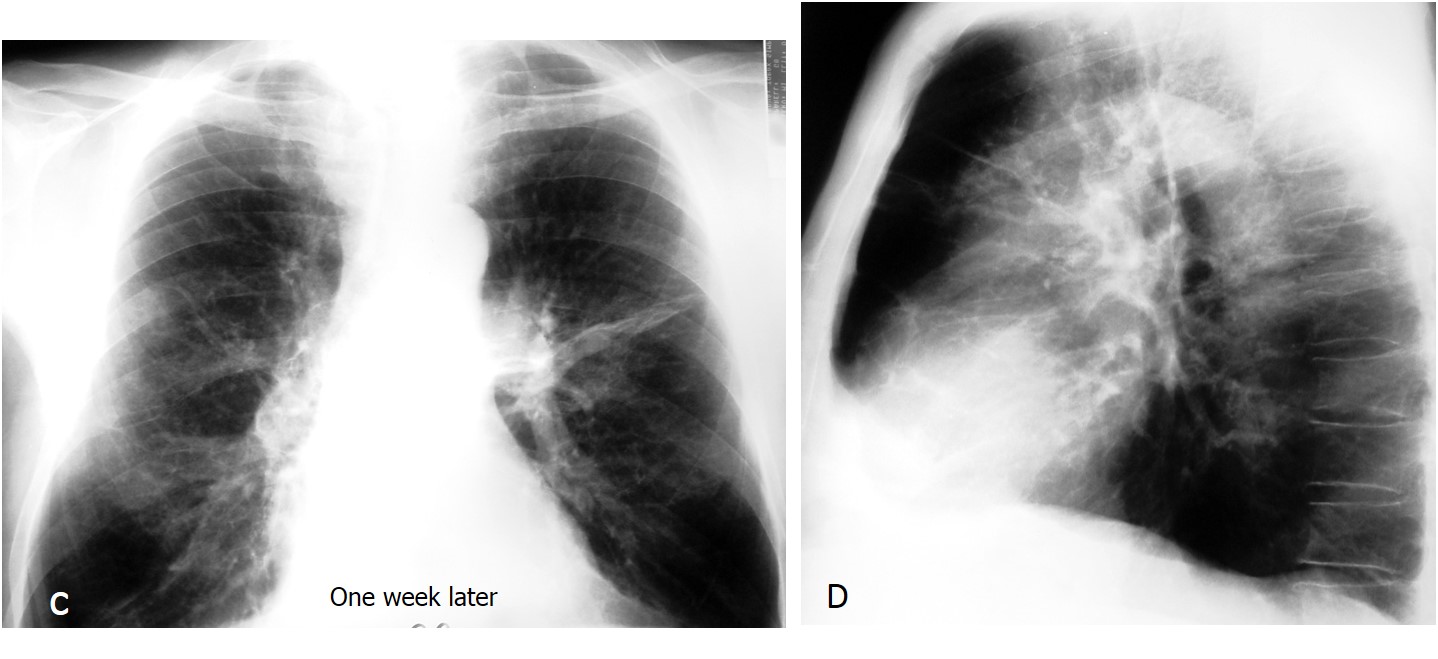
Fig. 2 C&D
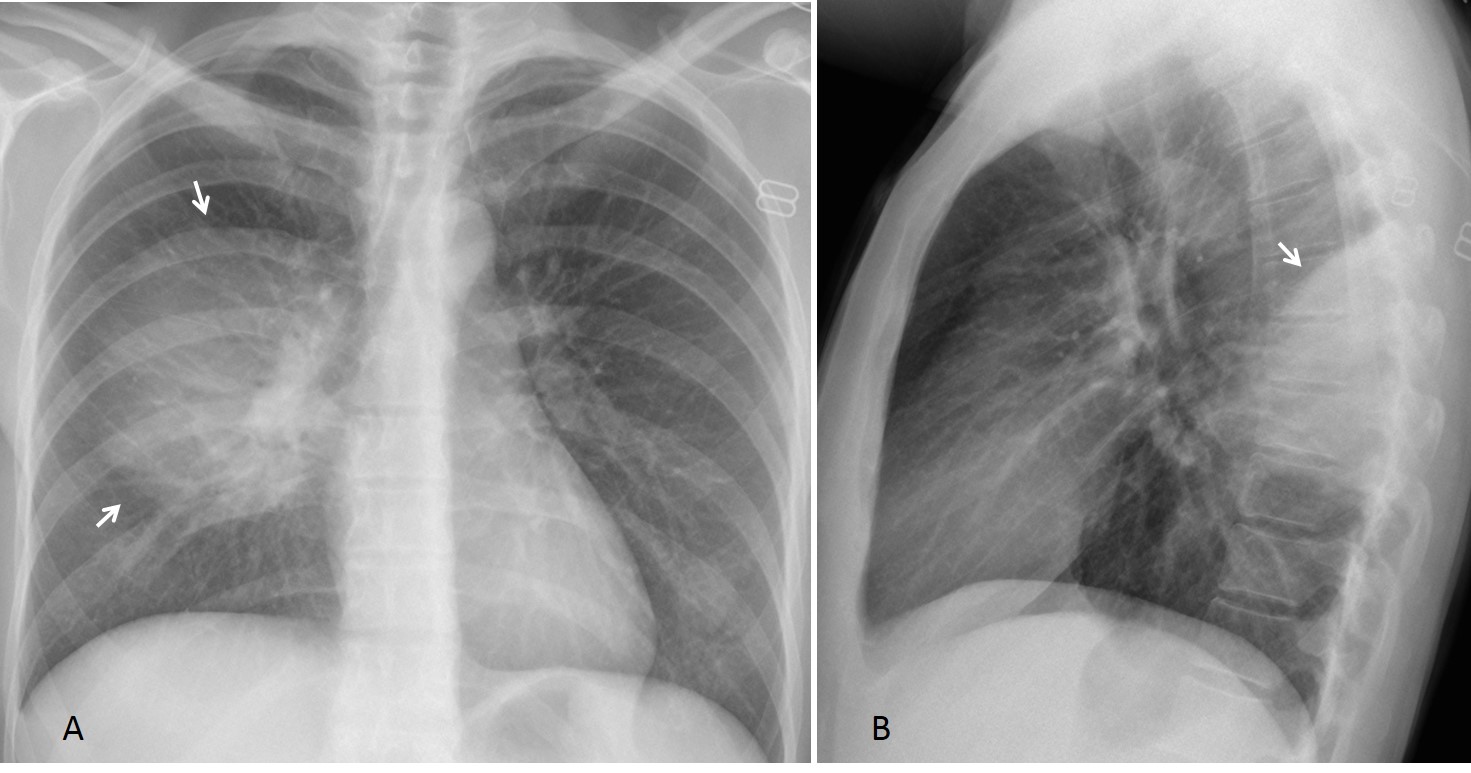
Fig. 3
Fig. 3: 20-year-old woman with round pneumonia. PA radiograph shows a poorly defined round opacity in the right middle lung (A, arrows). Lateral film shows a segmental opacity, well defined superiorly where it abuts the major fissure (B, arrow), raising the possibility of an extrapulmonary process. After treatment, chest films showed normal findings.
In my experience, pneumonia occupying an entire lobe (lobar pneumonia) is uncommon. It appears sharply defined, being limited by the lobar fissure. There is volume loss due to plugging of peripheral bronchi (Fig. 4). An air bronchogram may be present. The imaging appearance simulates lobar collapse due an endobronchial obstruction, and CT may be needed to rule this out. Rapid improvement after treatment supports the diagnosis (Fig. 5) , although complete disappearance should always be confirmed (Dr. Felson).
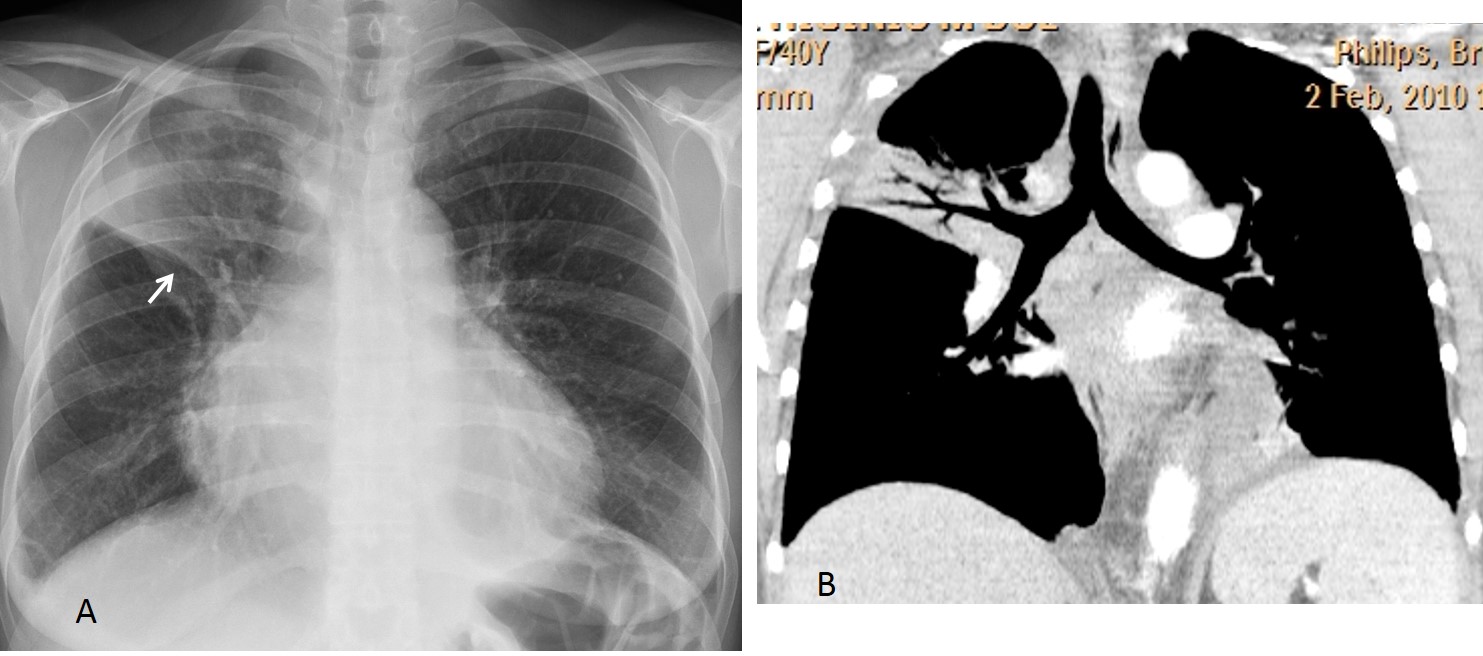
Fig. 4
Fig. 4: 40-year-old woman with lobar pneumonia. Note the volume loss, evidenced by the elevated and concave minor fissure (A, arrow). CT study (B) excluded an obstructed RUL bronchus.
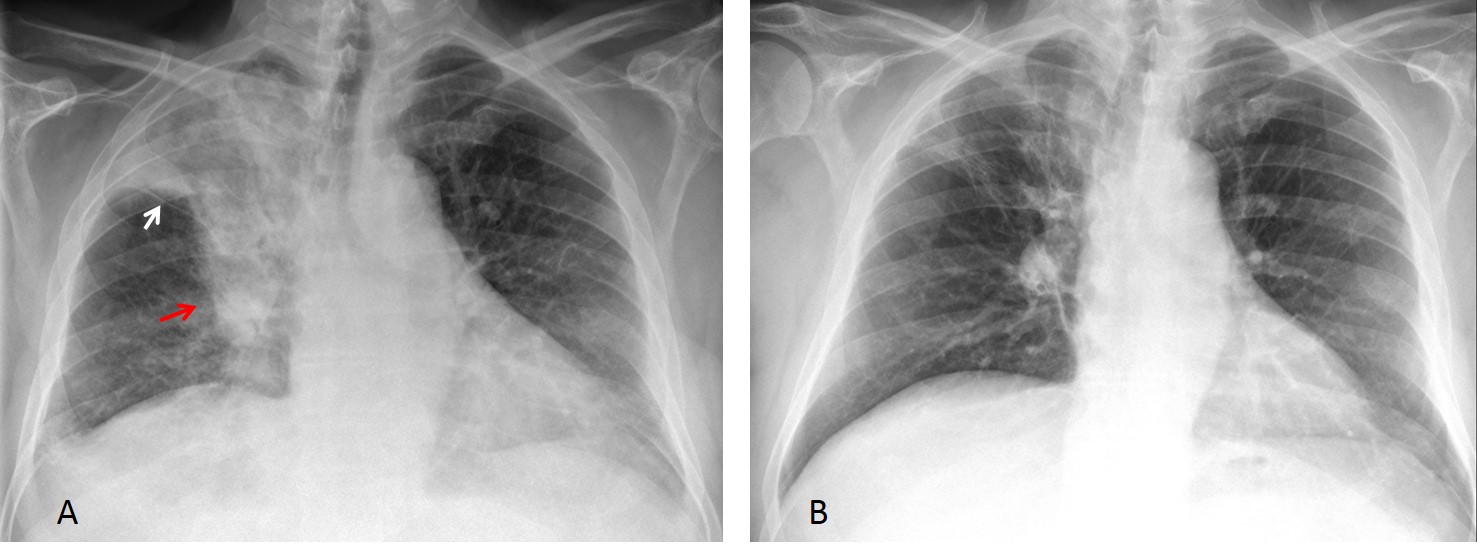
Fig. 5
Fig. 5: 62-year-old man with RUL pneumonia simulating a neoplasm. Initial film shows RUL opacity, elevation of the minor fissure (A, white arrow), and a possible mass in the hilum (A, red arrow). PA chest film after treatment (B) shows marked improvement.
Recurrent pneumonia is defined as two of more episodes of infection within an interval of 18 months. When it recurs in the same location, a focal abnormality should be suspected (local bronchiectasis, endobronchial lesion, or congenital lesion). Bronchiectasis and congenital lesions favor the lower lobes. CT should be done to explore these possible etiologies (Figs. 6 and 7).
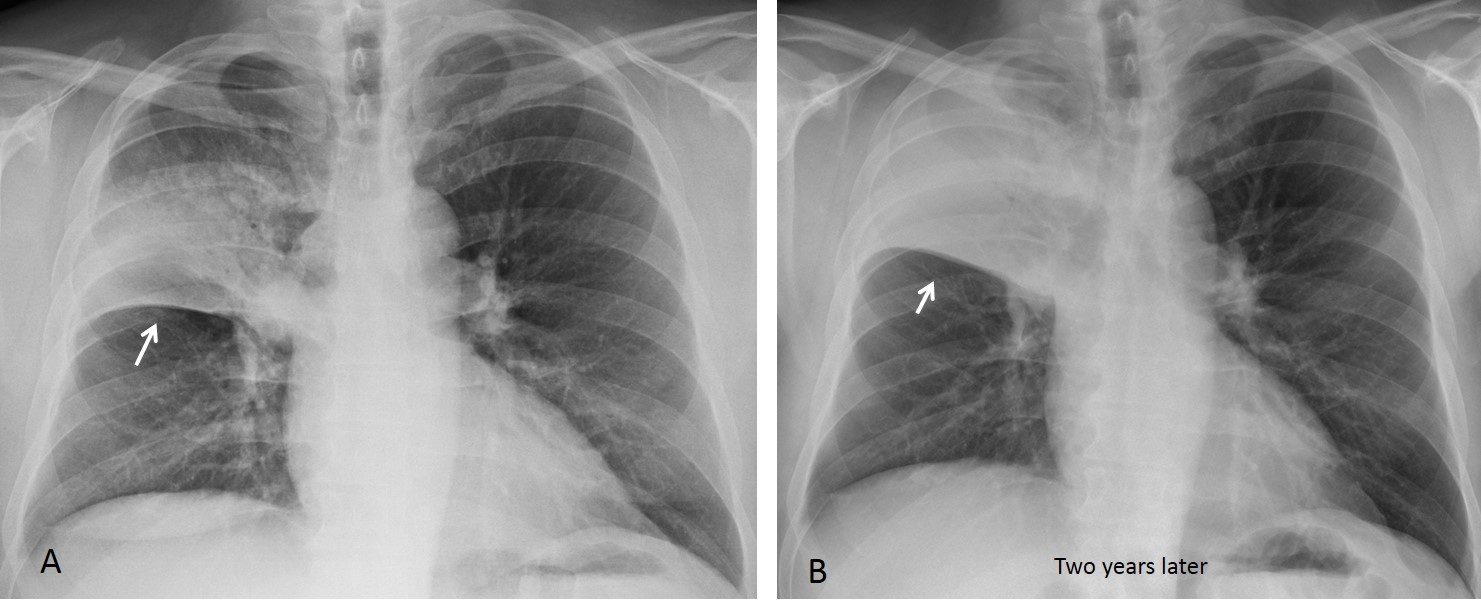
Fig. 6 A&B
Fig. 6: 59-year-old man who experienced RUL pneumonia twice within a two-year interval (A and B, arrows). Recurrence in the same region prompted a CT study.
Axial CT shows an endobronchial tumor at the origin of the RUL bronchus (C and D arrows).
Final diagnosis: chondromatous hamartoma.
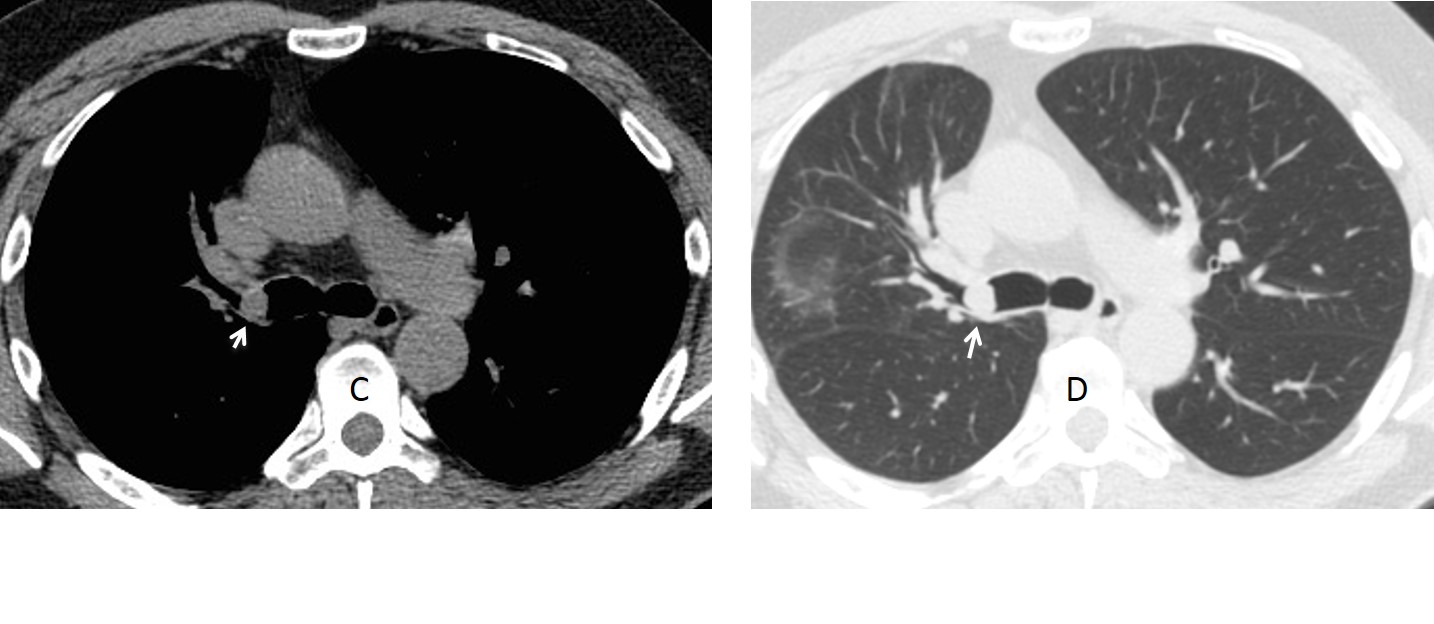
Fig. 6 C&D
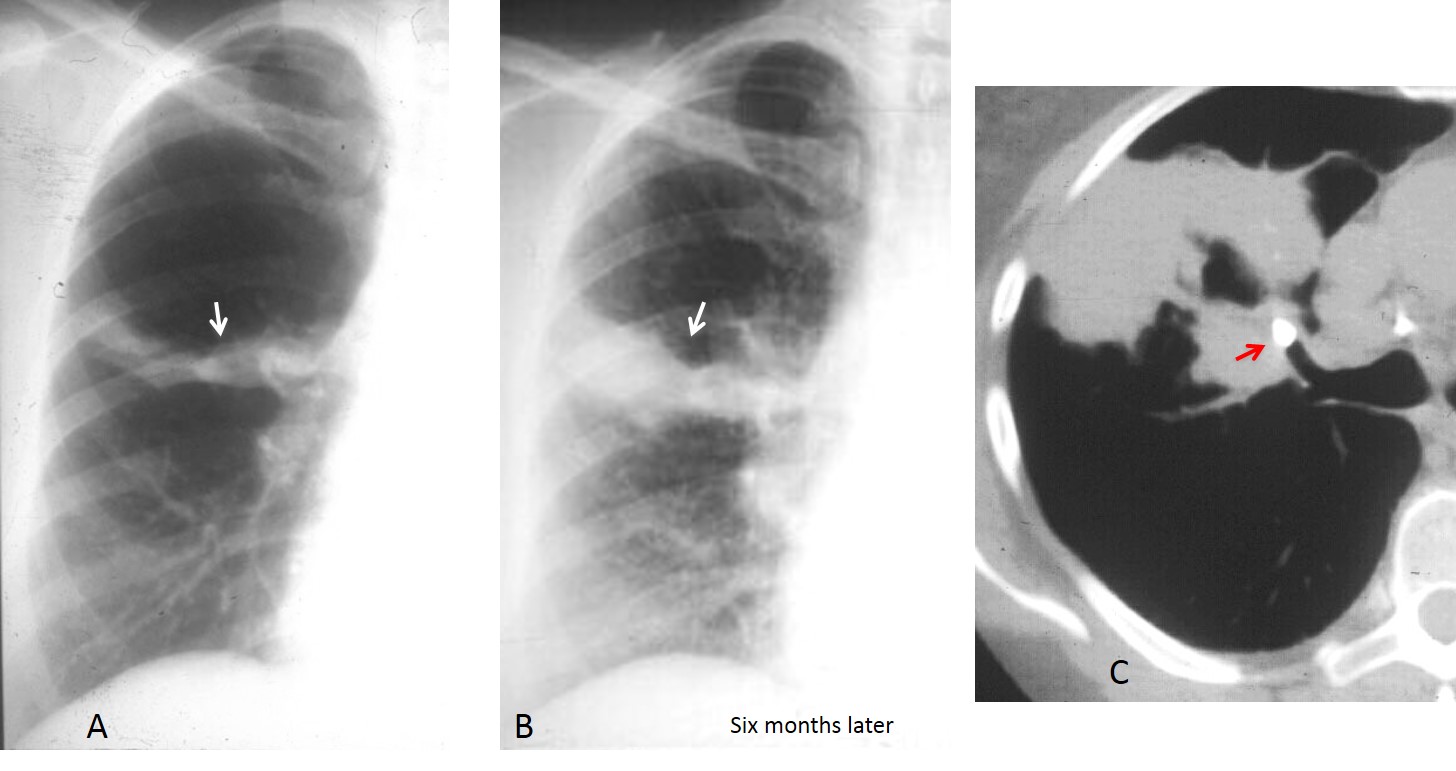
Fig. 7
Fig. 7: 56-year-old man with recurrent RUL pneumonia (A and B arrows). Unenhanced CT shows a calcification at the origin of the anterior segment of the RUL bronchus (C, arrow). Diagnosis: broncholith
An infection that is not visible in the PA radiograph is considered an occult pneumonia. As around 25% of the lung is hidden by the mediastinum and diaphragm in the PA film, these infections are usually seen in the lateral film (Fig. 8). Pneumonia of the RML or lingula is also difficult to see because the borders are not parallel to the X-ray beam. These infections are also better visualized in the lateral view (Fig. 9). These considerations illustrate the importance of obtaining a lateral radiograph in all patients with suspected pneumonia in whom the PA view does not provide helpful information.
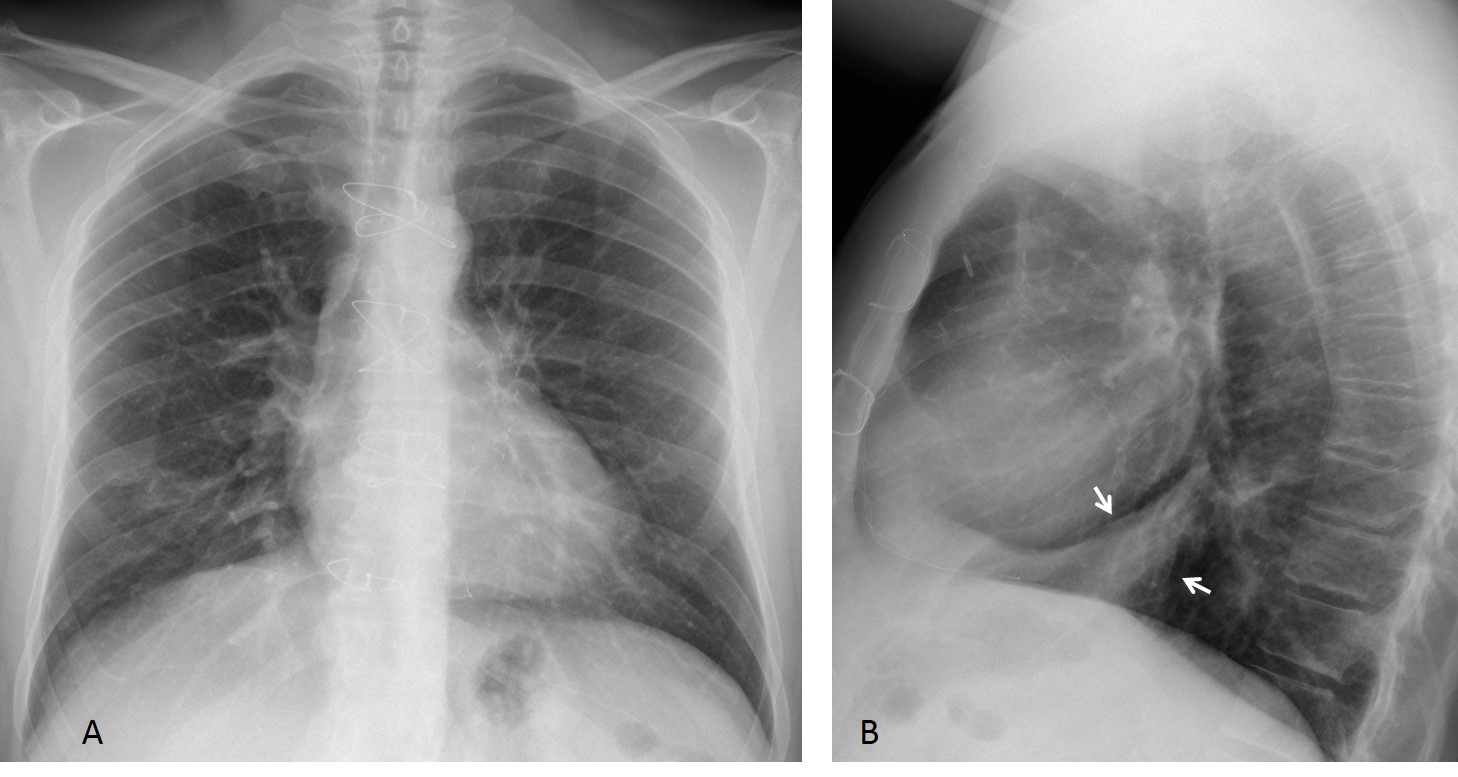
Fig. 8
Fig. 8: 35-year-old man with cough and fever. PA radiograph (A) does not show any abnormalities, aside from the previous sternotomy. Lateral view shows an obvious opacity in the anterior segment of RLL (B, arrows). Diagnosis: acute pneumonia
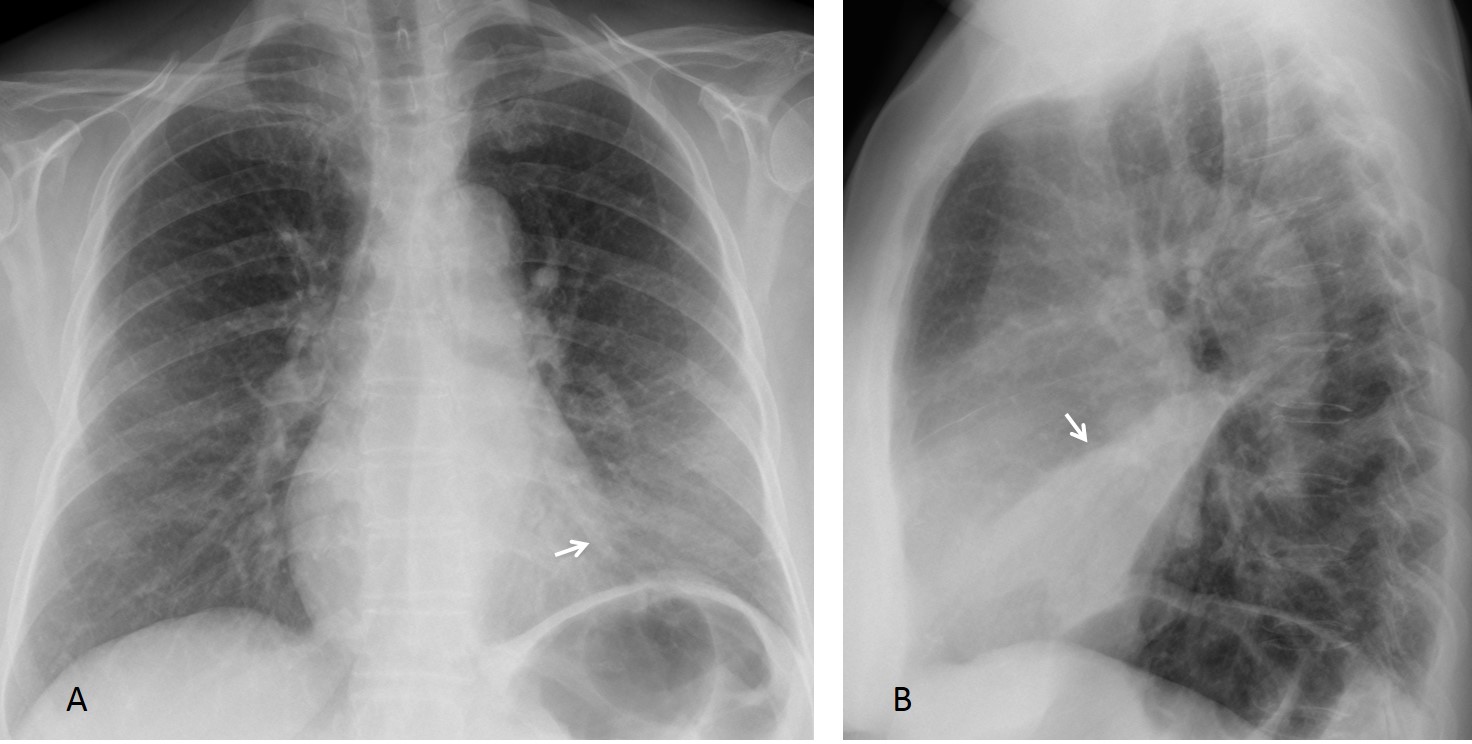
Fig. 9
Fig. 9: 42-year-old woman with lingular pneumonia. PA film shows a discrete increase of density in the lower left lung and haziness of the lower left heart border (A, arrow). The lateral view clearly depicts the lingular infiltrate (B, arrow).

Follow Dr.Pepe’s Advice:
1. Round pneumonia can occur in adults. Do not confuse it with lung masses.
2. Lobar pneumonia is less common than believed. If it does not clear with treatment, CT should be done to exclude an endobronchial lesion.
3. Recurrent pneumonia in the same location requires CT study to exclude a local abnormality.
4. Occult pneumonia in the PA film is easily discovered by taking a lateral view.


Hypovenstilated right upper lobe + elevation of the horizontal fissure caused by RUL atelectasis+ may be there is an assiciated pneumonia.
Right pleural effusion on the lateral view.
Nice description. If asked by the patient’s physician, what would you say?
Nice description. What will you tell the patient’s physician if she/he asks you your diagnosis?
Golden S sign + donuts sign …suspicious for a bronchogenic carcinoma.
atelectasia + derrame = carcinoma.
Carcinoma
There is a triangular right apical opacity on the frontal view, with elevation of the minor fissure displaying a convex contour cranially, tracheal deviation to the right and elevation of the right hemidiaphargm. These signs suggest upper right lobe collapse. The minor fissuere looks like the S-sign of Golden and is suggestive of a neoplastic etiology causing atelectasis of the right upper lobe.
Cicatrical RUL atelectasis. It could be tuberculosis, maybe with activation (right pleural effusion).
heterogeneous opacity of the right upper lung lobe partially solid and partially showed air bronchogram, with mass effect in the form of shifting of the trachea to the right side and transverse fissure upwards, most likely of carcinoma, yet TB could not be totally excluded.
…male il Bari in” campionato”…..male ANCHE nella classifica del mitico Professore…..proviamo a fare risultato almeno qui…..è una lesione con “riduzione di volume” , come si può osservare, dalla risalita della piccola scissura, del diaframma e “shift” della colonna d’aria tracheale….la “chiave” di lettura è nei broncogrammi aerei , che nel caso di una atelettasia sono ristretti, mentre in una “carnificaqzione TB con allargati: in questo caso l’opacità “retrattile” ha bronchi ampi….pertanto la diagnosi è il numero 3:TBC….con la stima di sempre da Bari!!!!
bronchiectasis partial atelectasis consolidation RUP lobe
pneumonia TB
how about endogenous foreign body in pneumonia?
A sophisticated diagnosis. It is more common than that.
TB
Would coexistence od TB and cancer be possible? Just a thought… Something is not right with that atelectasis- I think ropy and nodular densities are visible…
Well, i think mostly of options 1) and 3).
Definitely the loss of lung volume at the RUL should raise the possibility of carcinoma. However I don´t figure an exact S at the horizontal fissure, neither an hilar mass.
By other hand the clinical scenario given is compatible with tuberculosis, and so is the image, so I would go for option 3)
Abraço Hugo
At this time of the week, I can say that all of you are correct. Carcinoma, lobar pneumonia and TB (in order of frequency) can all give this appearance. So, you all can get credit.
This case is shown to present uncommon apperances of pneumonia (lobar pneumonia does not happen as often as the textbooks say).
Than you for participating!