Dr. Pepe’s Diploma Casebook: Case 68 – SOLVED!
Dear Friends,
This week I am presenting the radiographs of a 50-year-old man with chest pain. Check the images below, leave your thoughts and diagnosis in the comments, and come back on Friday for the answer.
Diagnosis:
1. Multiple myeloma
2. Tumor of sternum
3. Fibrous tumour of pleura
4. None of the above

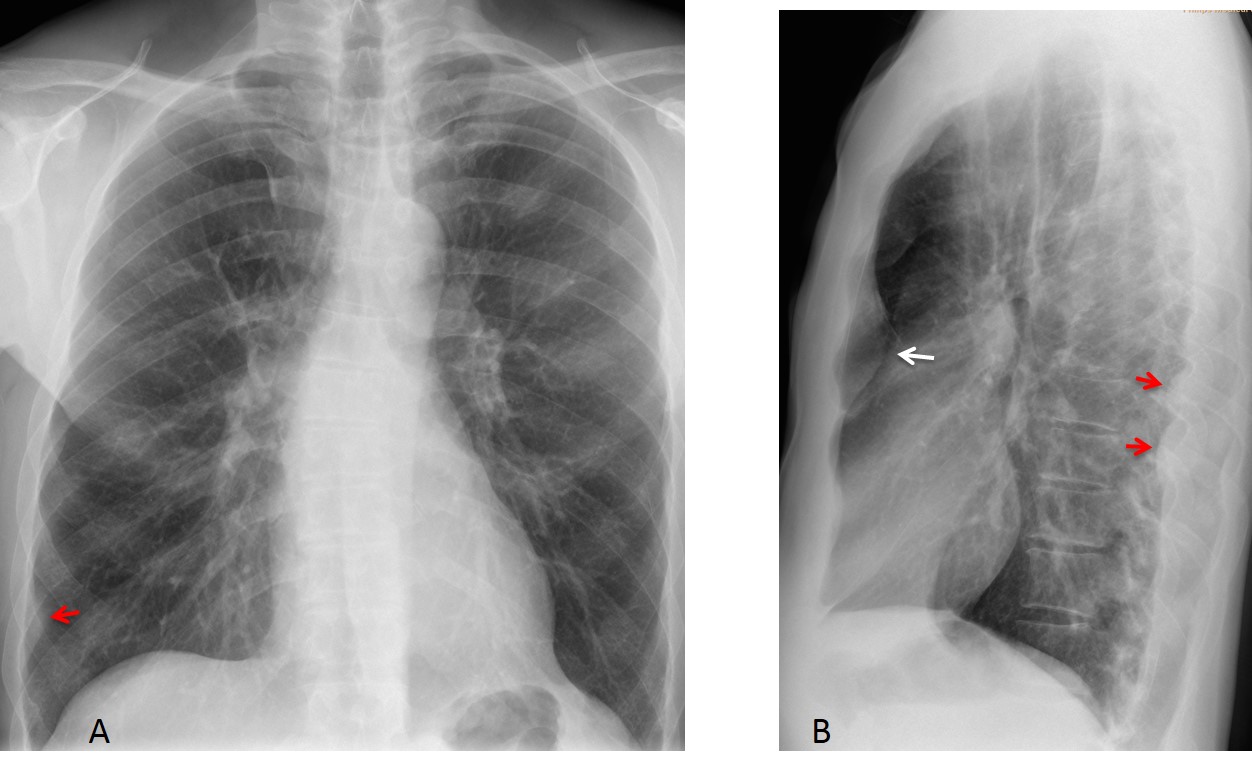
Findings: Lateral chest radiograph shows a large retrosternal extrapulmonary soft-tissue mass (B, white arrow), not seen in the PA view (A). In addition, there are smaller peripheral masses in the PA and lateral views (A,B, red arrows). Given the multiplicity of the lesions, fibrous tumour of pleura and sternal tumour can be excluded. The presence of several lesions is consistent with the diagnosis of multiple myeloma, which was later confirmed.
Comparison with follow-up radiograph after autologous transplant treatment shows complete disappearance of the lesions (A and B, circles).
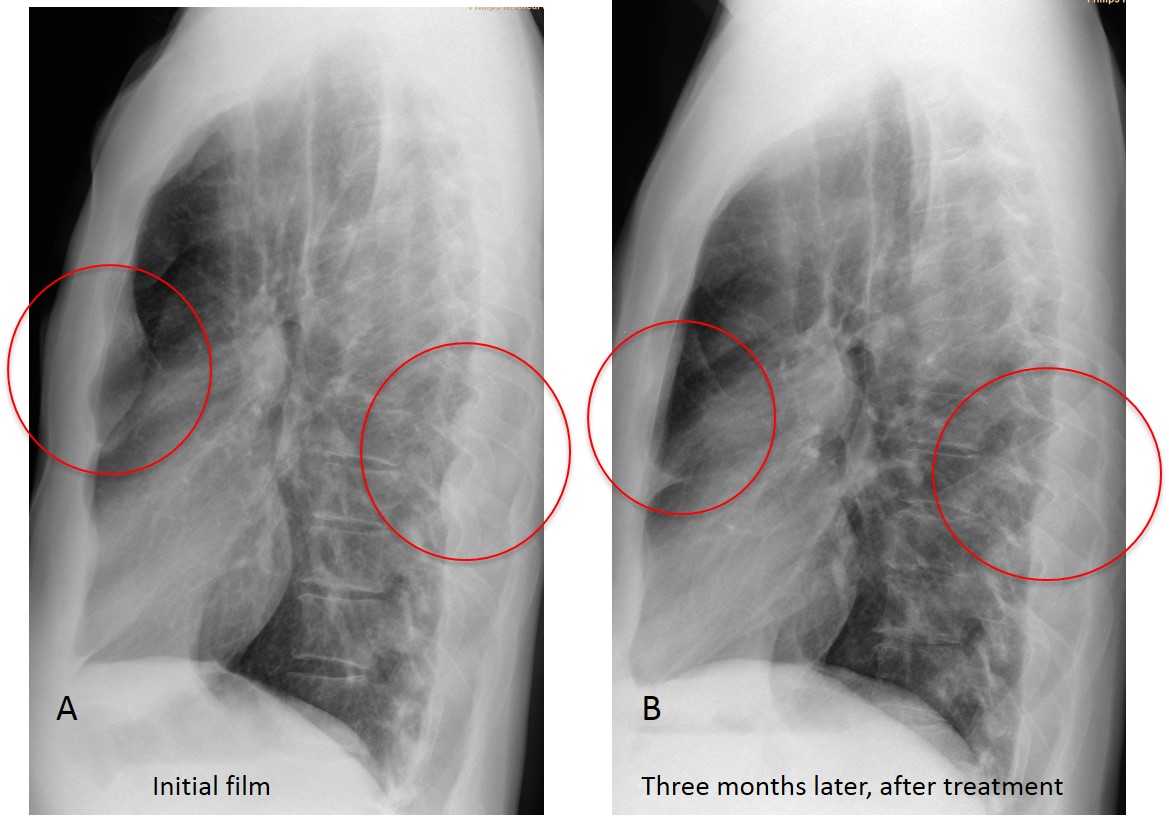
Diagnosis: IgD multiple myeloma.
This case is presented to illustrate the importance of looking at the anterior clear space; that is, the dark area behind the sternum in the lateral view. It is limited anteriorly by the sternum and posteriorly by vascular structures (ascending aorta and main pulmonary artery) (Fig. 1). The size of the anterior clear space depends on the body habitus and age. It is smaller in thin people and in those of advanced age because the elongated ascending aorta encroaches on the space.
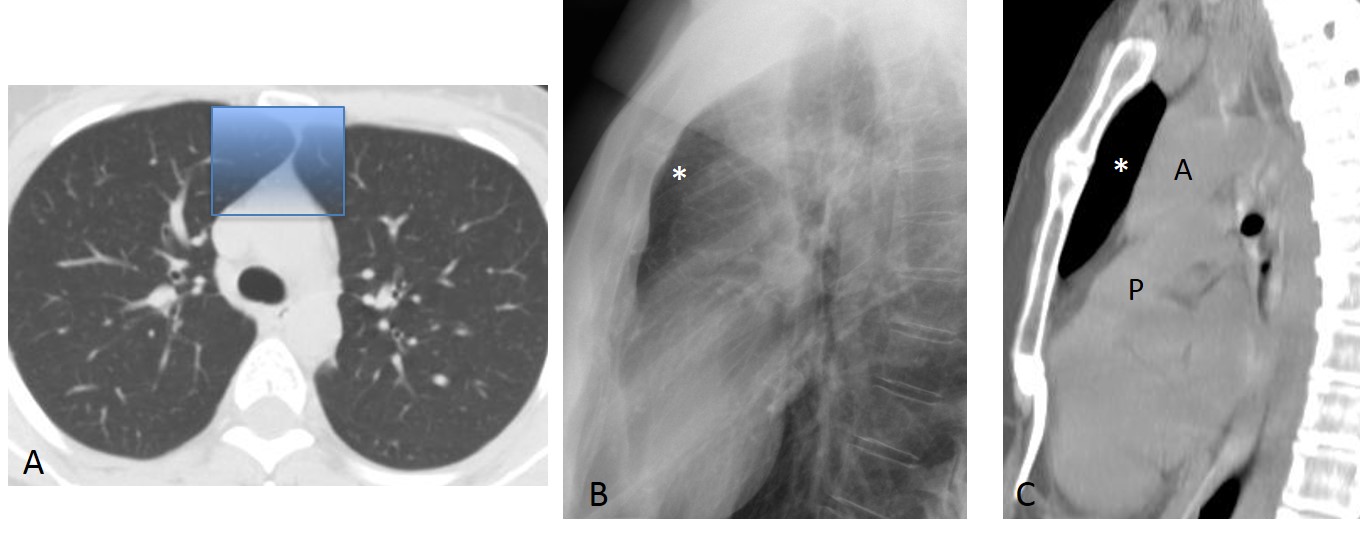
Fig. 1
Fig. 1: axial CT showing the area of lung hidden in the PA view (A, shaded rectangle), which represents the anterior clear space in the lateral view and the sagittal CT image (B and C, asterisks). A, aorta; P, pulmonary artery.
The anterior clear space is important because abnormal processes in this area may not be depicted in the PA projection, being obscured by the superior mediastinum, whereas they are easily visible in the lateral view. Abnormal processes in the anterior clear space may arise from the pleura/chest wall, mediastinum, or lung.
Extrapulmonary lesions (pleura/chest wall), usually arise from the sternum, pleura or mammary lymph nodes. They are well outlined and have obtuse angles with the characteristic appearance of extrapulmonary lesions. They are located immediately behind the sternum (Figs. 2 and 3).
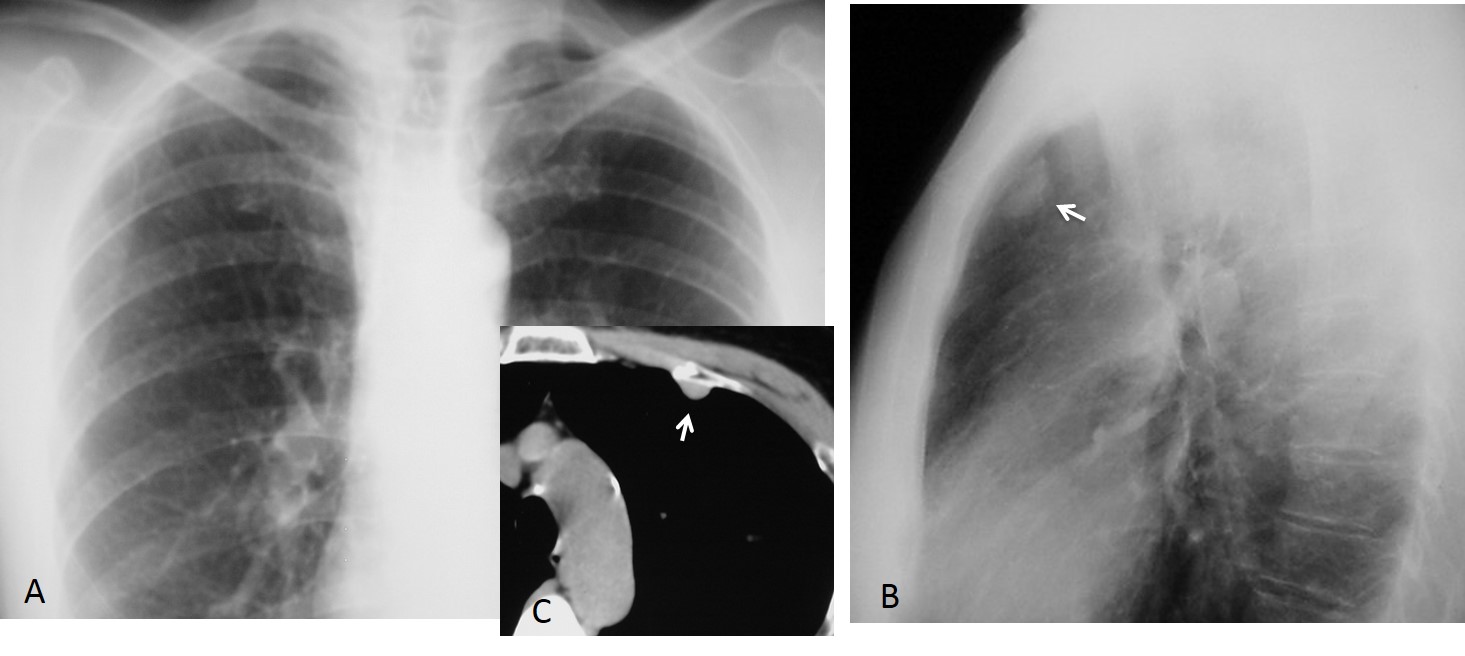
Fig. 2
Fig. 2: 45-year-old woman with breast carcinoma. Routine control chest radiographs show an extrapulmonary lesion in the anterior clear space that is visible in the lateral chest view (B, arrow), but not in the PA film (A). Unenhanced CT shows the extrapulmonary lesion (C, arrow). Surgical diagnosis: fibrous tumour of pleura.
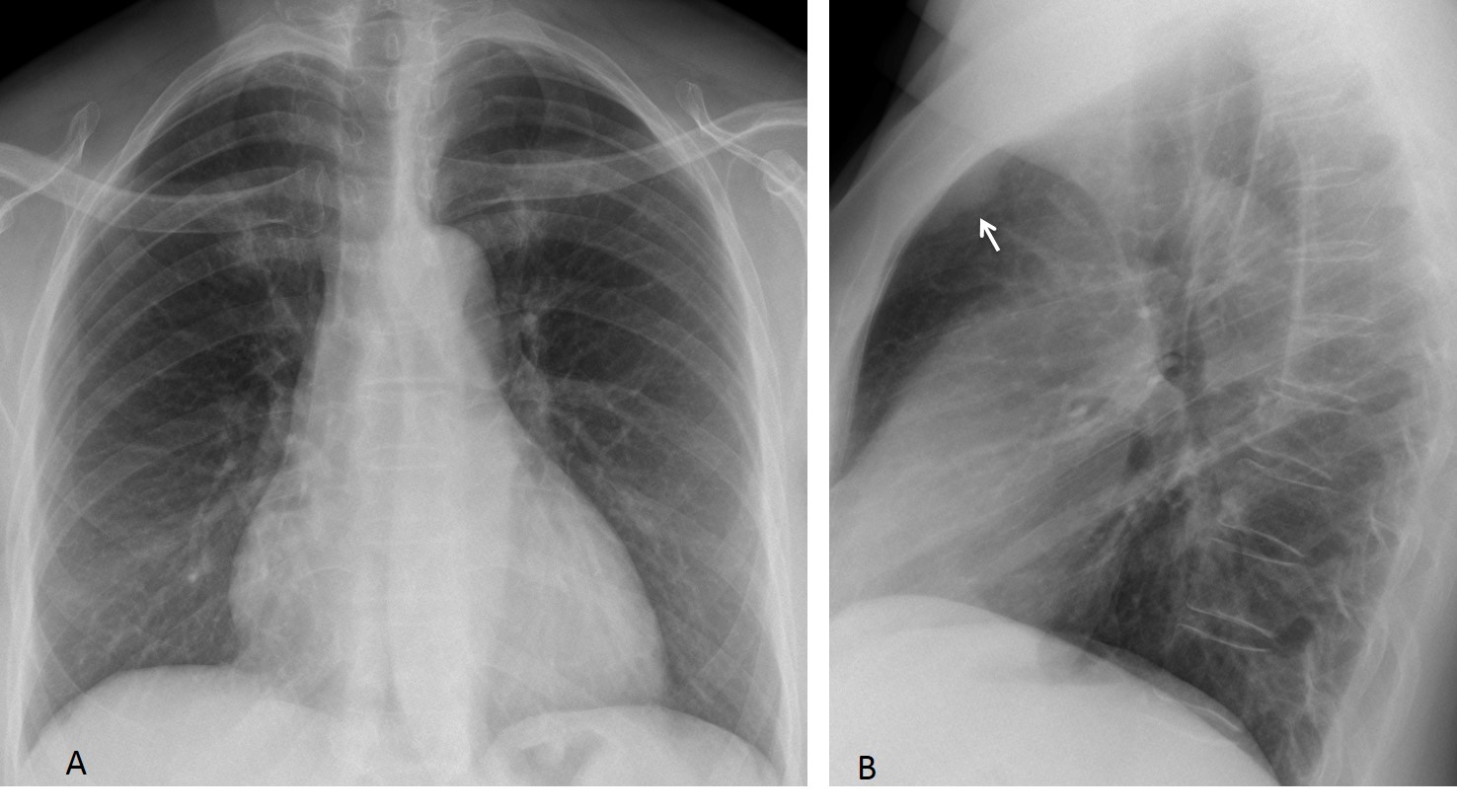
Fig. 3
Fig. 3: routine follow-up chest films in a 54-year-old woman who had undergone surgery for breast carcinoma. The lateral view shows an extrapulmonary mass in the anterior clear space (B, arrow) that was not visible in the PA radiograph (A).
Comparison with previous radiographs taken a year earlier shows that the mass was present, albeit smaller (C and D, arrows). Sagittal CT confirms the extrapulmonary mass (E, arrow). Surgical diagnosis: metastatic internal mammary lymph nodes.
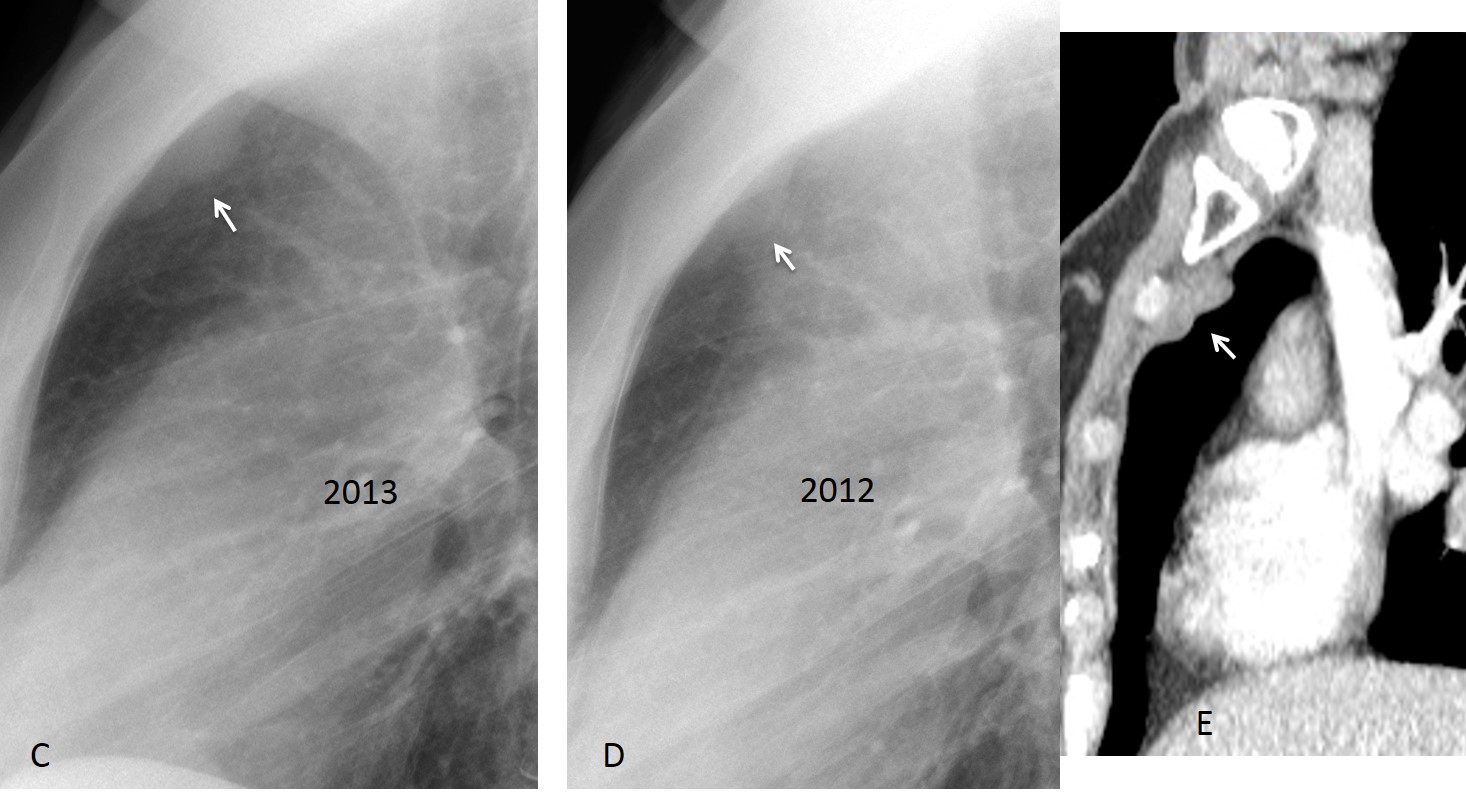
Fig. 3
Anterior mediastinal masses may also occupy the anterior clear space. They are located in the posterior aspect of the space, adjacent to the mediastinum. They are round and not as well defined as extrapulmonary lesions. They may reach a significant size and still not be visible in the PA view (Figs. 4 and 5). The majority arise from the thymus.
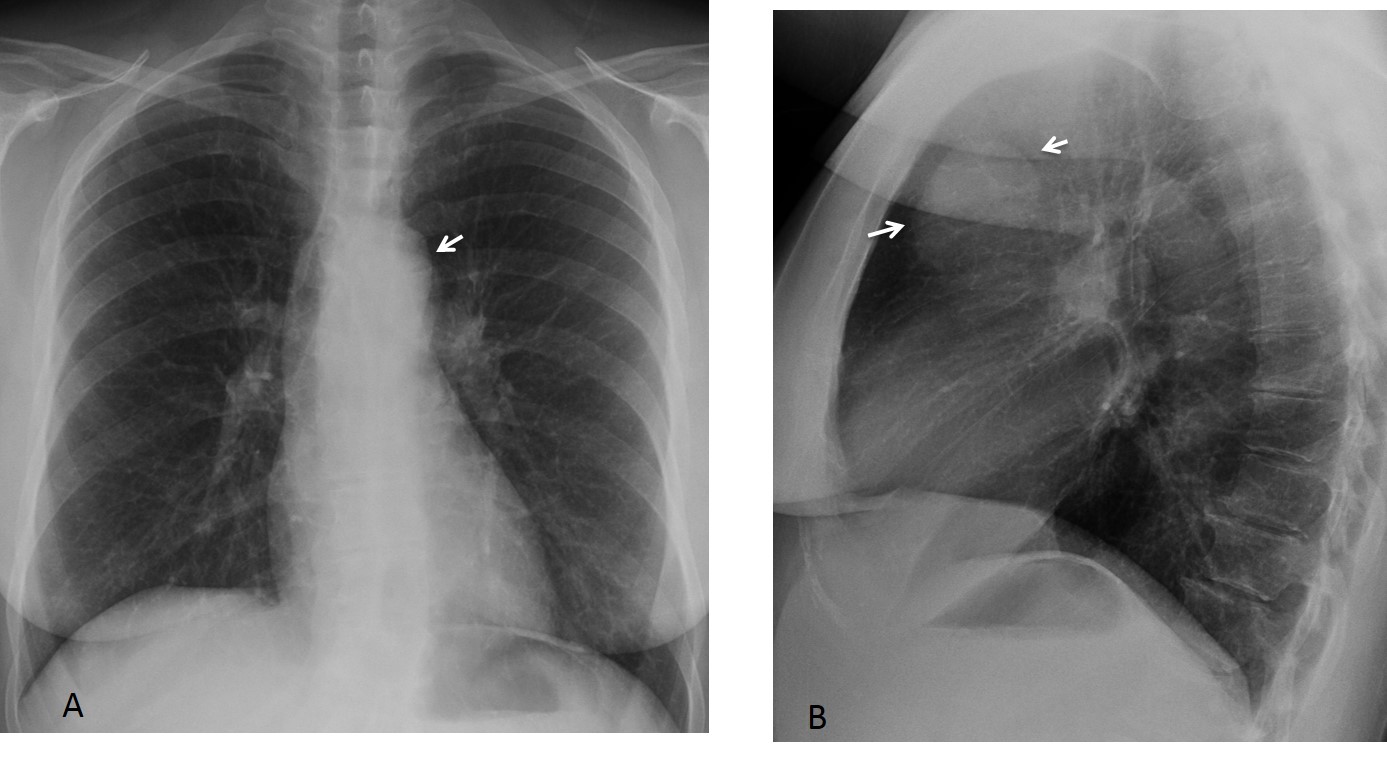
Fig. 4
Fig. 4: 57-year-old woman with myasthenia gravis. PA radiograph shows double contour of the aortic knob (A, arrow). In the lateral view, a large round mass is seen in the anterior clear space (B, arrows).
Axial and sagittal unenhanced CT images show an anterior mediastinal mass (C and D, arrows).
Surgical diagnosis: thymoma.

Fig. 4
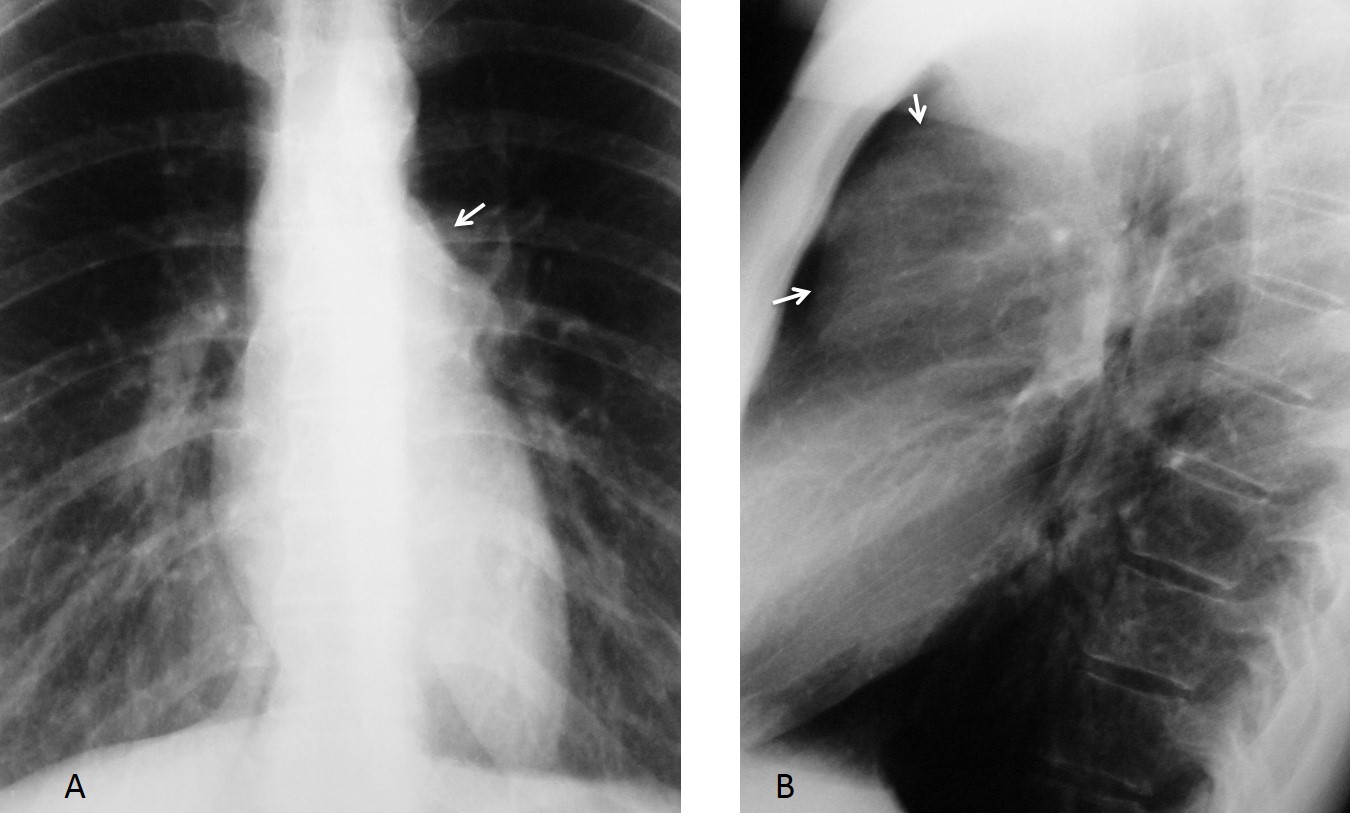
Fig. 5
Fig. 5: 51-year-old woman with asthenia. The PA view show a doubtful double contour at the level of the left hilum (A, arrow). In the lateral view, a large mass is seen in the anterior clear space (B, arrows).
MRI confirms the mass in the anterior mediastinum (C, arrow). A posterior pleural implant is visible on MRI (D, arrow) and CT (E, arrow).
Diagnosis: malignant thymoma.
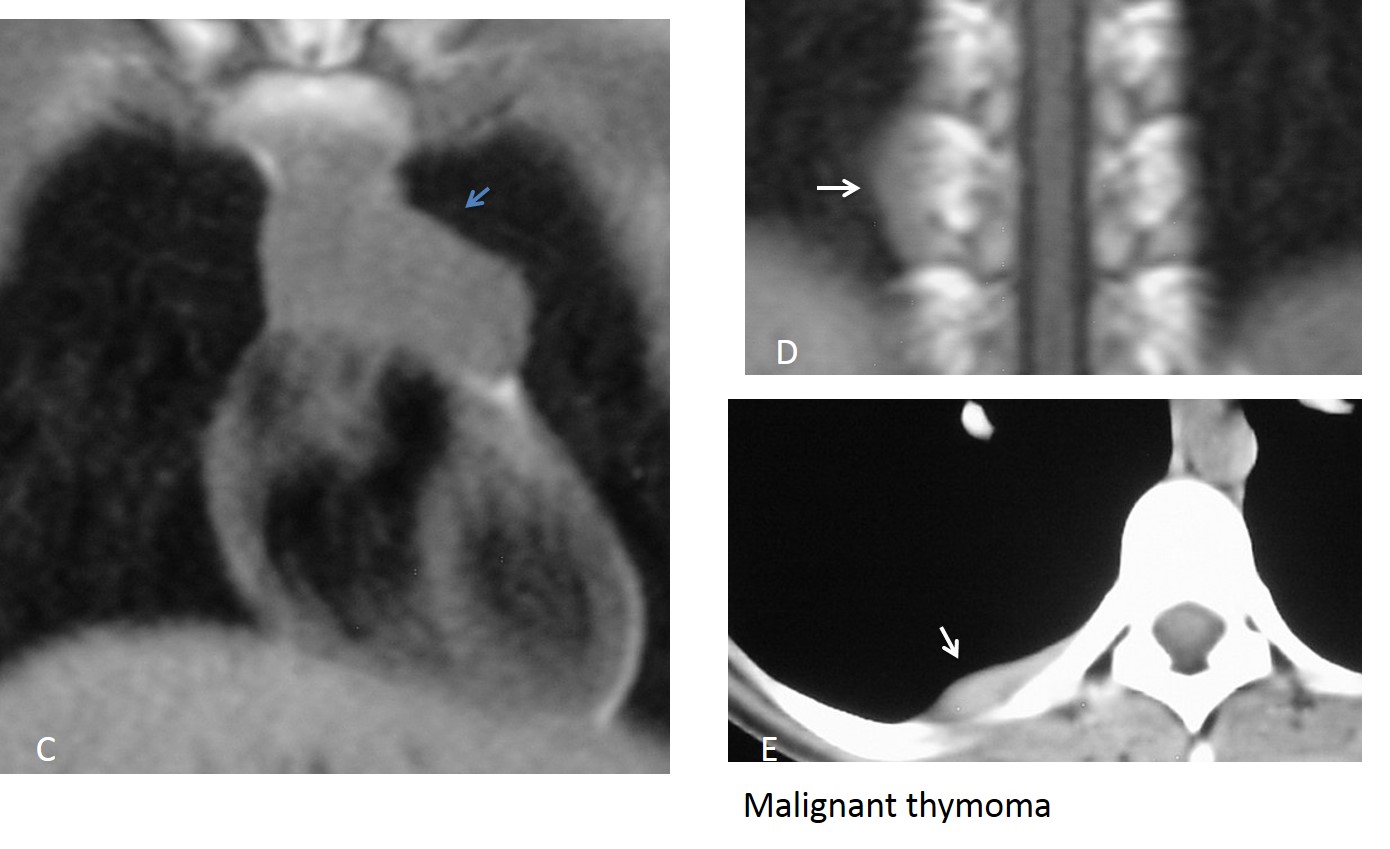
Fig. 5
The retrosternal area is occupied by the medial segments of both upper lobes, separated by the anterior junction line. Pulmonary infections or tumours can occur in this area. In my experience, it is not rare to see pulmonary lesions in the anterior clear space, unsuspected in the PA view. They are usually well seen because they are surrounded by air (Figs. 6-8).
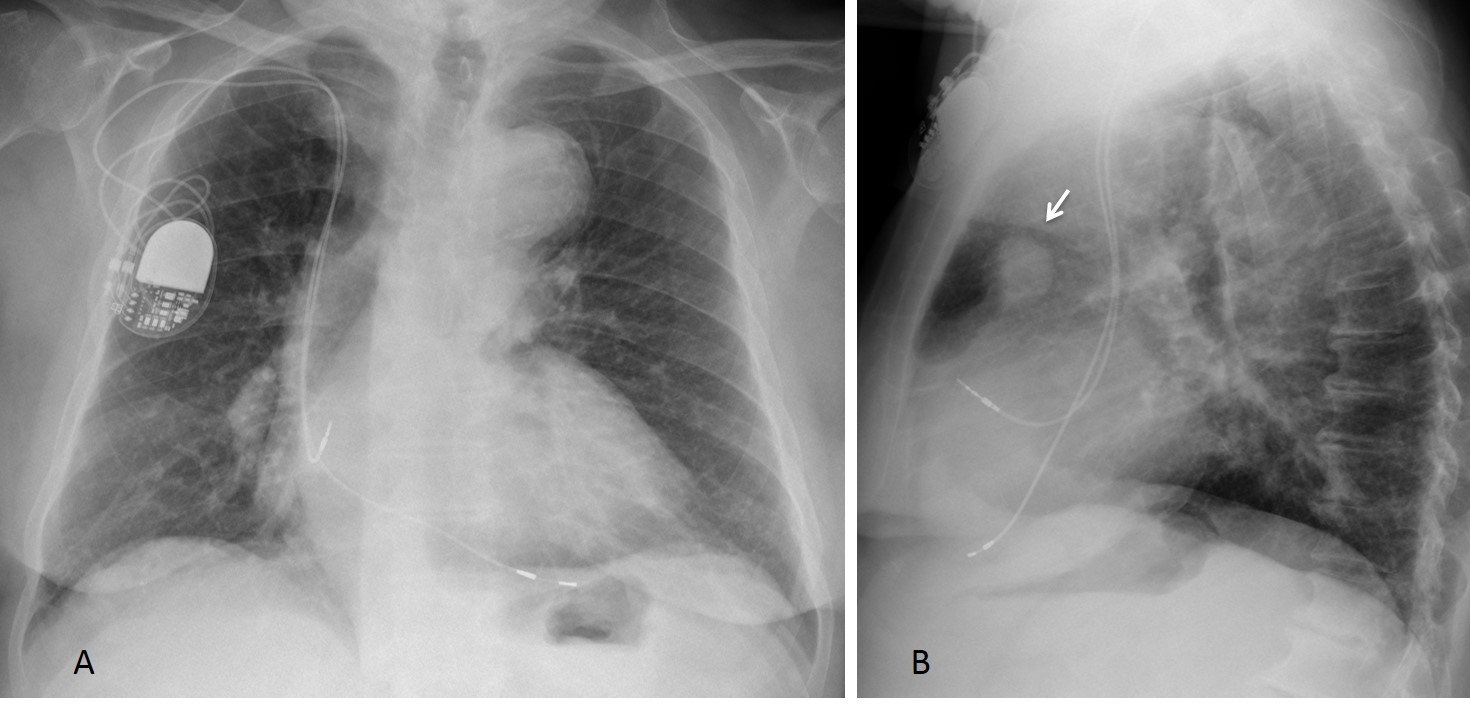
Fig. 6
Fig. 6: 84-year-old man with dyspnea. Lateral chest radiograph shows a pulmonary nodule in the anterior clear space (B, arrow) that was not visible in the PA chest film (A).
Sagittal and axial CT confirm the presence of the nodule, which shows a calcium deposit (C, arrow) and fat (D, arrow). Hamartoma was suspected. Due to the patient’s advanced age, no further procedures were undertaken.

Fig. 6
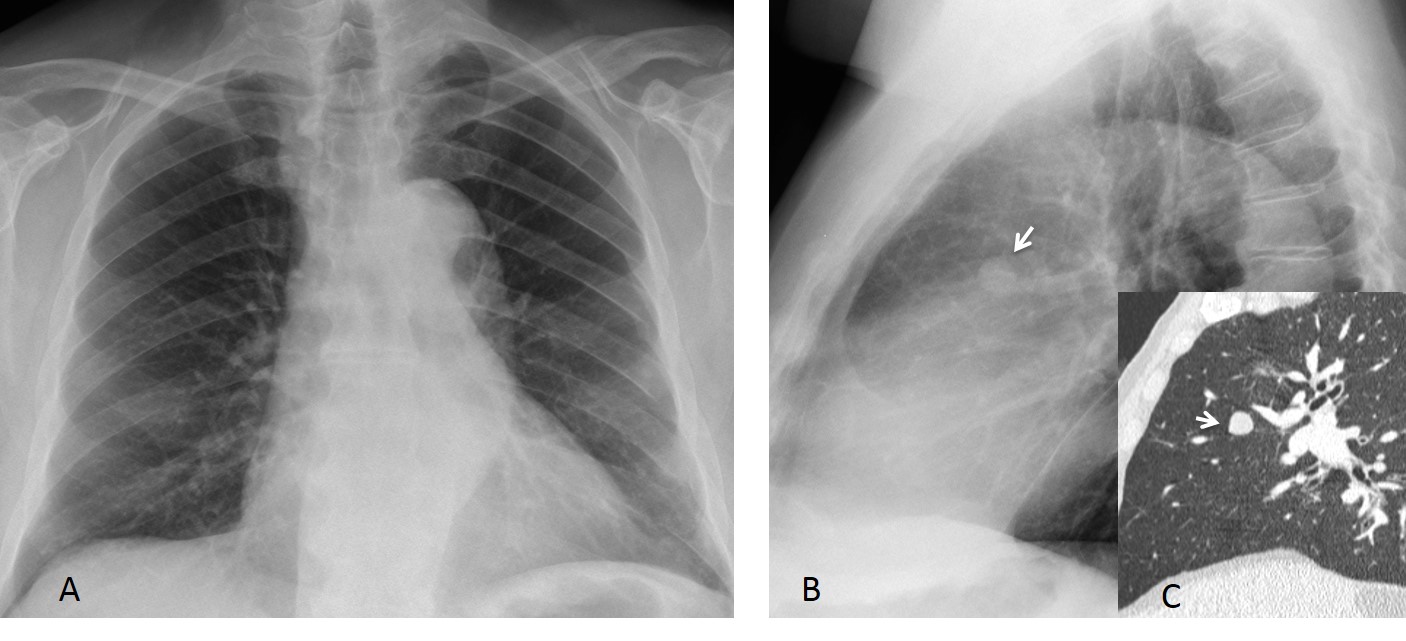
Fig. 7
Fig. 7: 72-year-old man with moderate dyspnea. Lateral film discovers a pulmonary nodule in the anterior clear space (B, arrow) that is not visible in the PA film (A). The nodule is confirmed with CT (C, arrow).
Final diagnosis: adenocarcinoma.
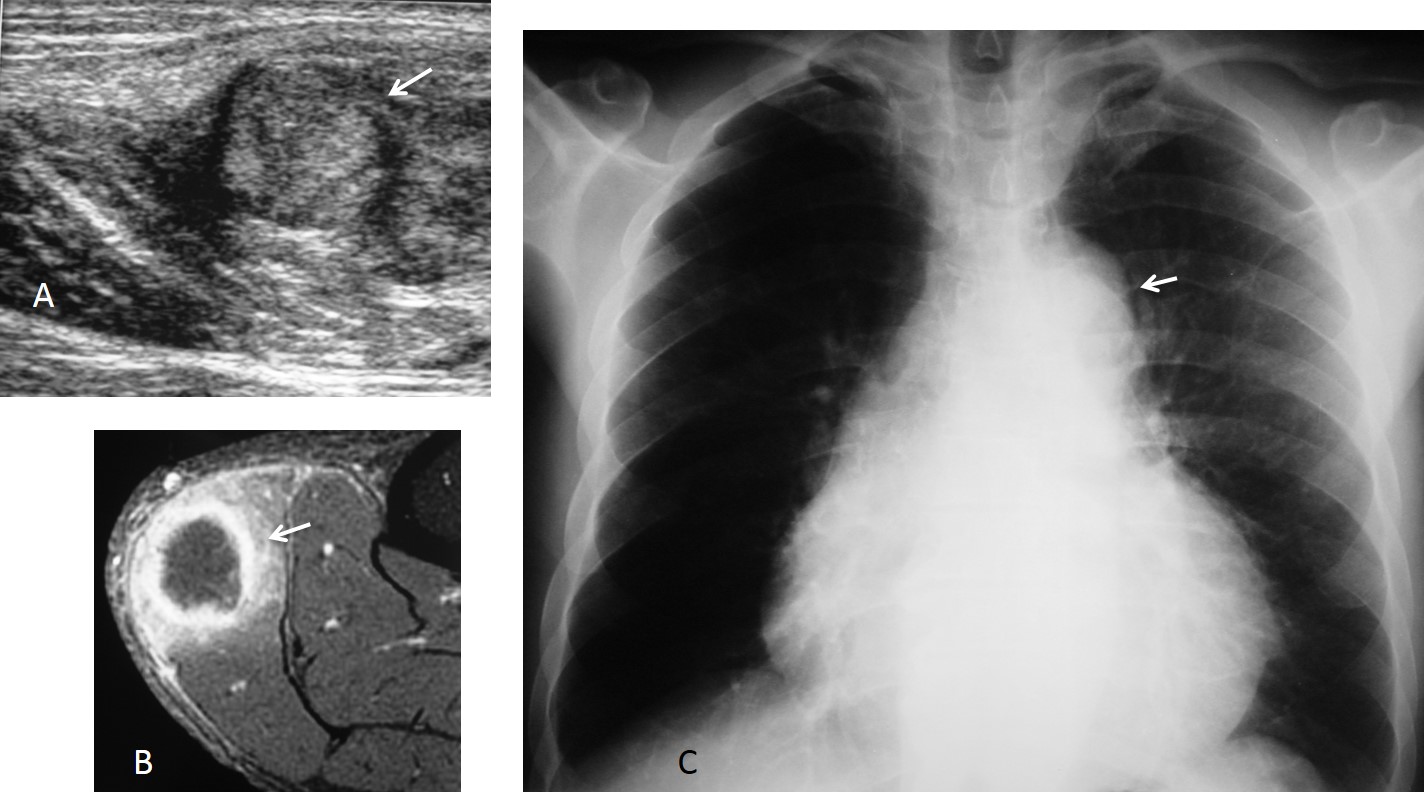
Fig. 8
Fig. 8: 58-year-old man with a painful mass in the left gastrocnemius muscle for the last two months, visible on US and MRI (A and B, arrows). PA chest film shows a double contour of the aortic knob (C, arrow) that was overlooked in the initial interpretation.
Lateral film shows a large mass in the anterior clear space (D, arrows), confirmed with CT (E, arrow). Final diagnosis: adenocarcinoma of lung with soft tissue metastasis.
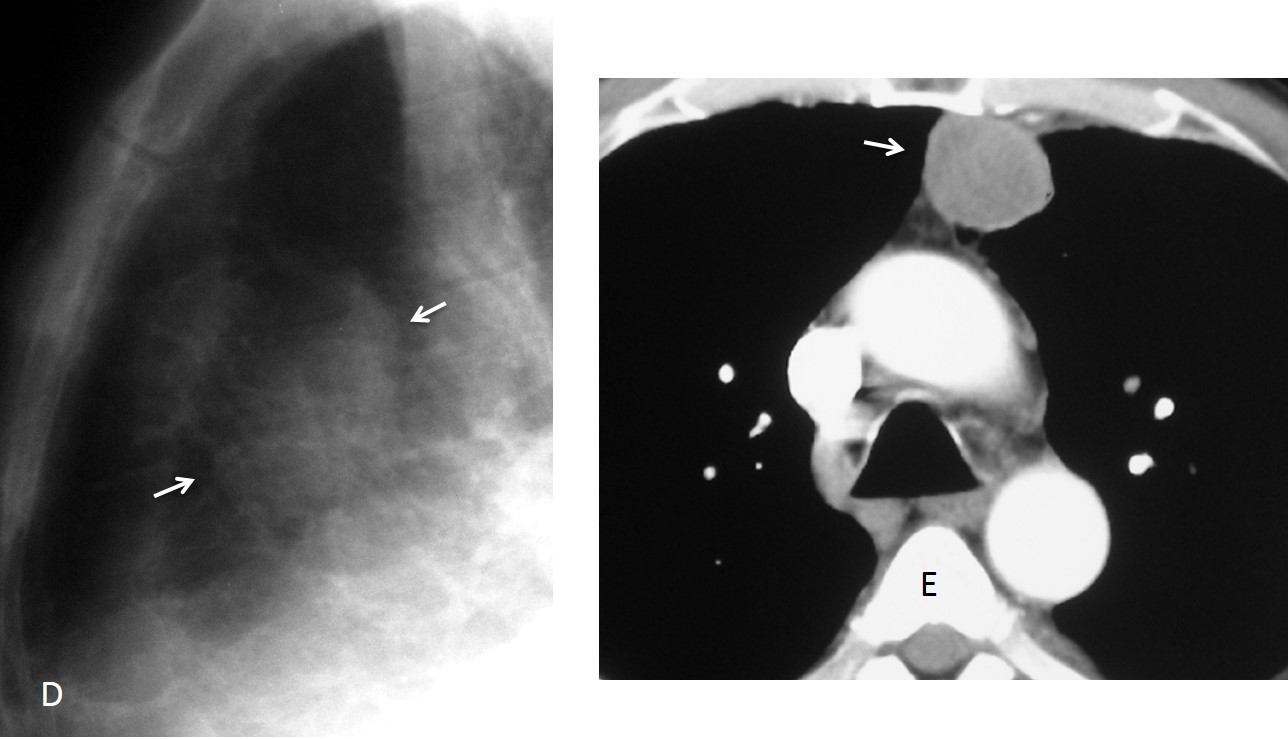
Fig. 8

Follow Dr.Pepe’s Advice:
1. It is important to look at the anterior clear space in the lateral view because some lesions are only visible in that projection.
2. Extrapulmonary lesions are located behind the sternum and have sharp borders and obtuse angles
3. Mediastinal tumours are round and are located in the posterior part of the space.
4. Pulmonary lesions are usually well seen because they are surrounded by air.


Fibrous tumor of pleura
tumor of sternum
I go with answer no 3 fibrous tumour of pleura
none of the above
Multiple myeloma
3. Fibrous tumour of pleura
4. None of the above.
Dilated internal mammary artery – due to aortic stenosis?
Besides scoliosis of the thoracic spine and fibrotic findings of the RUL on the frontal view, I also see expansion of the sternal manubrium and an extrapulmonary lesion projecting behind the body of the sternum on the lateral view.
Perhaps there is expansion of the anterior part of a rib on the lateral view also..Multiple myeloma cannot be easily exclued from the differential diagnosis. Increased density of TH7 is also noted.
I would also like to add that the left pectoralis major is absent….Poland syndrome?
I think is more than one lesions sub sternal,on posterior and lateral thoracic wall without bone involvement.
i believe it’s pleural origin lesions(obtuse angle with the chest wall) but i am not sure if it is Fibrous tumour of pleura, (i know it’s solitary tumors).
so a CT… is necesary 🙂
You are contradicting yourself when you say that fibrous tumor is solitary and at the same time state that the lesions are multiple
i say there is multiple pleural origin tumors.that make’s unusual the presentation of a fibrous tumor.
i vote CT 🙂 4
only sqolioz…
Fibrous tumor Of the pleura.
There is a mass behind the sternal body, which change its form in the lateral projection, and form open angles with the chest wall.
….riduzione del DAP toracico, rispetto al DT toracico, con riduzione dello spazio r.c. Ed “apparente” cardiomegalia……si associa dismorfismo sternale, con lobulazioni (adipose?) retrosternali…..BACK STRIGHT S., con prolasso della mitrale che può’ spiegarmi dolori toracici….
Costochondritis- Tietze syndrome
Despit all the pleural soft tissue lesions and scoliosis but a Straight Dorsal Syndrom could be the cause of chest pain in this case.
I would also like to add that the left pectoralis major is absent….Poland syndrome?
left pectoralis is OK. I think the increased density of T7 is due to superposition.
Chest radiograph of adult male. Multiple smooth thickening lesions along the pleural lining bilaterally, broad base towards the pleura giving undulating appearance. No calcifications within these lesion. No pleural effusion.
Lungs and heart are otherwise normal. No loss of lung volume.
Bones show diffuse osteopenic changes, but no focal lytic lesion or bone destruction.
My answer is 4 – none of above. ?Pleural metastasis? Suggest CT Thorax and tentatively for pleural biopsy.
None of the above.
It’s an extra pulmonary lesion, no underlying bone destruction.
Opacity of lesion is less than soft tissue density, no calcification.
Multiple pleural plaques. Asbestosis ?
Mass: localized mesothelioma?
What do you think?
It is always a possibility, but fibrous mesothelioma is not related to asbestos. Asbestos-related mesothelioma usually gives pleural effusion and/or pleural thickening.
I selected this case to talk about the anterior clear space in the lateral view. Plus to test your “satisfaction of search”. If you look carefully, there are at least two additinal posterior pleural bumps in the lateral view(congratulations to Gus and J.D.). The most likely diagnosis are myeloma or metastases.
Full answer tomorrow.
GREAT Magister!!