Dr. Pepe’s Diploma Casebook: Case 69 – SOLVED!

Dear Friends,
Today I am showing radiographs of a 61-year-old woman who underwent surgery for ovarian carcinoma three years ago.
Examine the images below, leave your diagnosis in the comments section and come back on Friday for the answer.
Diagnosis:
1. Carcinoma of the lung
2. Metastases
3. Tuberculosis
4. None of the above
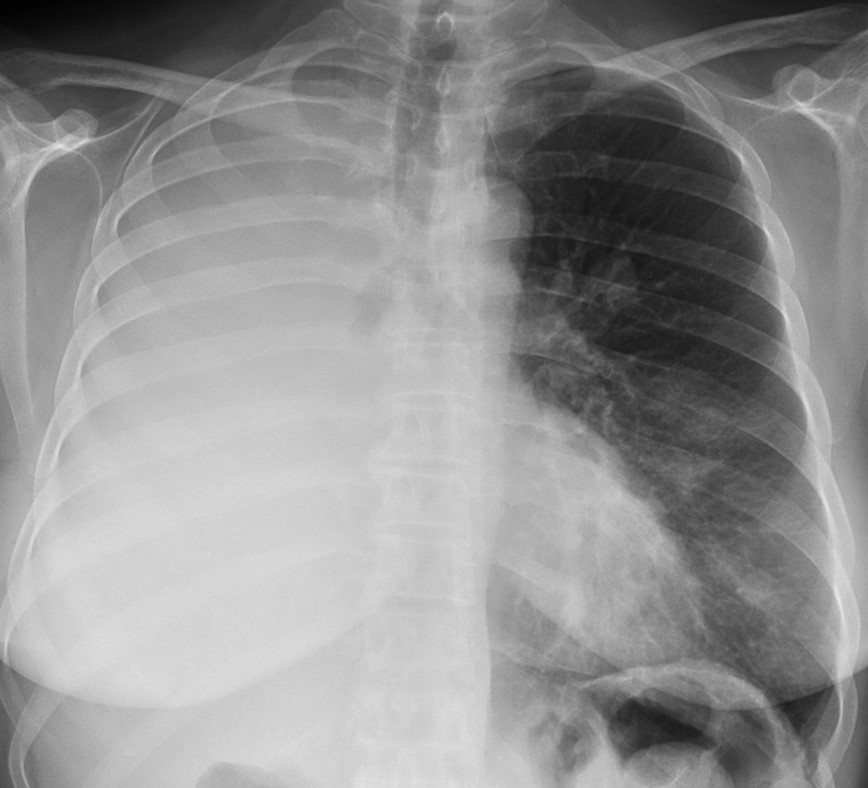
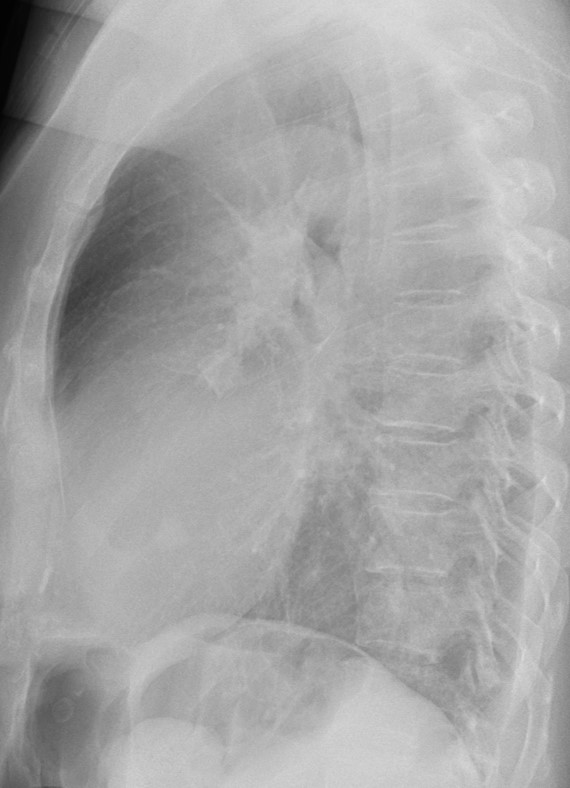
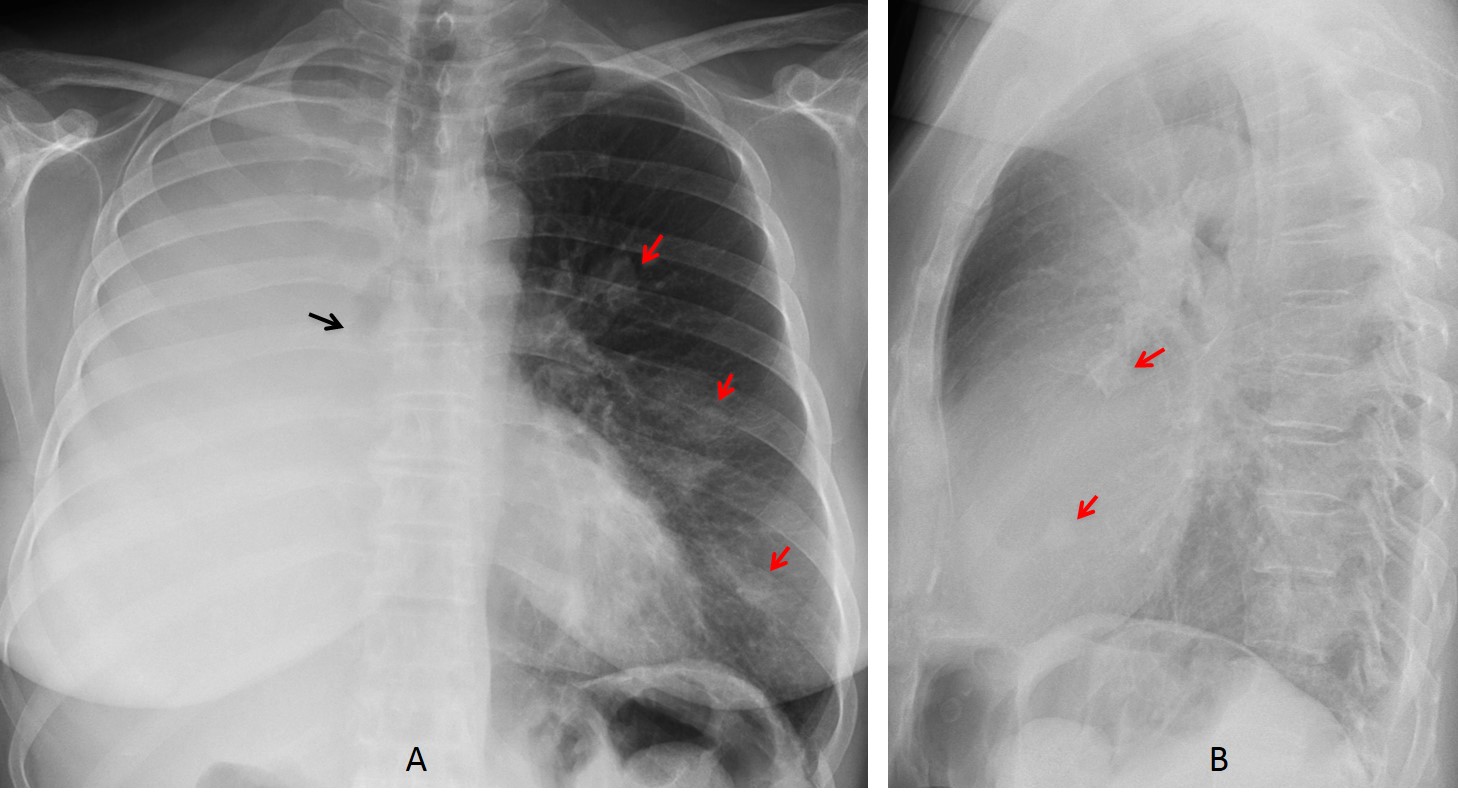
Findings: PA radiograph shows loss of volume of right lung with a stop in the right main bronchus (A, black arrow). There are several nodular lesions in the left lung (A,B red arrows). The lateral view (B) does not offer additional information.
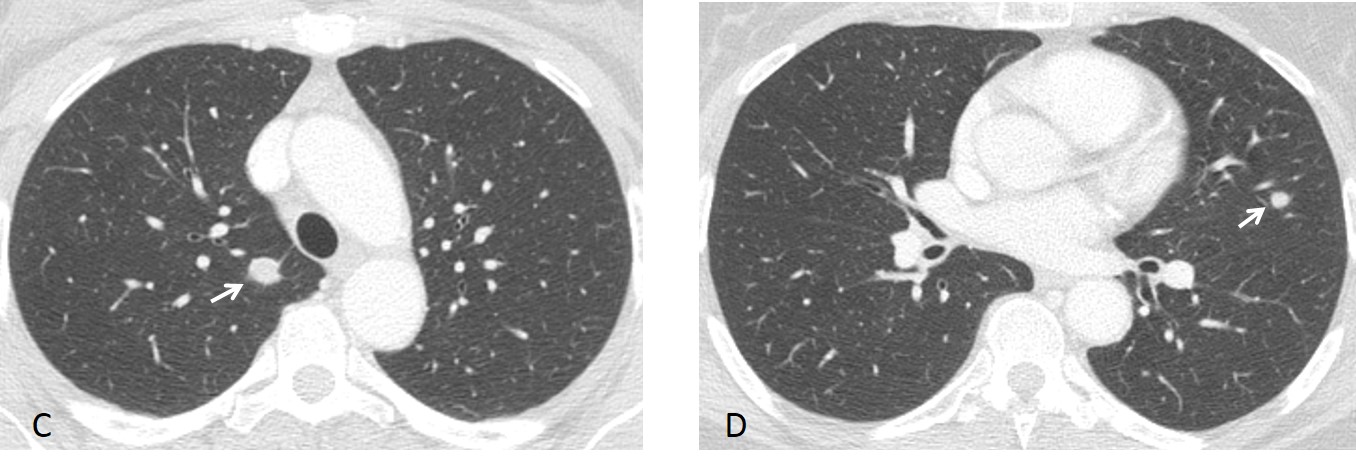
A previous CT shows nodular metastases in both lungs (C,D arrows). Bronchoscopy demonstrated a metastatic mass within the right main bronchus. The patient died a short time later.
Final diagnosis: metastases of ovarian carcinoma, one of them endobronchial.
Endobronchial lesions are not uncommon and can be suspected on plain films by signs of bronchial obstruction: collapse, mucus impaction, bronchiectasis, or recurrent local infection. CT confirms the endobronchial lesion and helps to determine its etiology, which is usually bronchogenic carcinoma.
Although bronchogenic carcinoma is relatively common, it is not the only cause of bronchial obstruction. Other tumours (benign and malignant) as well as non-tumoural entities may present as endobronchial lesions. In this presentation, I would like to review endobronchial lesions other than carcinoma and the contribution of CT to their diagnosis.
Malignant tumoural lesions are mainly metastases and carcinoids.
Endobronchial metastases represent about 2% of lung metastases. They simulate a primary lung tumour on plain films and CT, but are usually accompanied by nodular lung metastases, which help to suggest the correct diagnosis (Fig. 1). They may occur in association with any tumour, but the most common sources are colon, breast, kidney and melanoma.
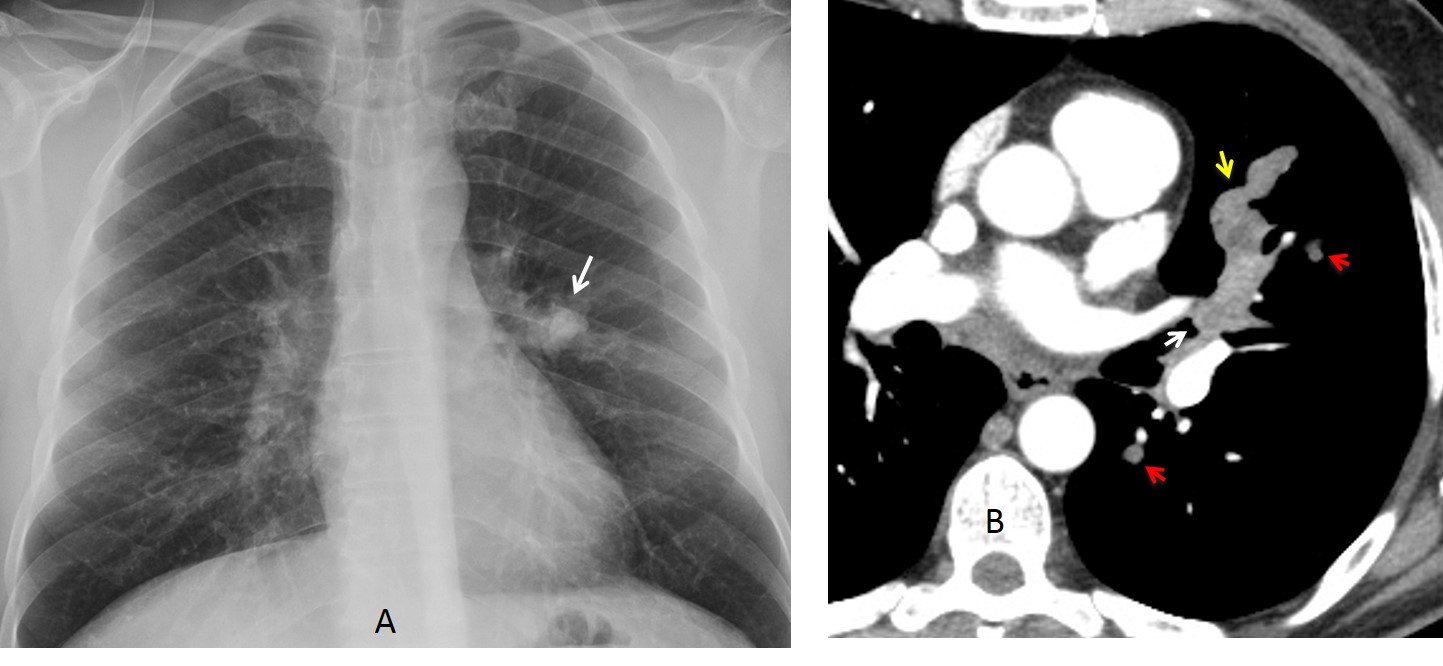
Fig. 1
Fig. 1: 45-year-old man with melanoma. PA chest film shows a nodule near the left hilum (A, arrow). CT depicts an endobronchial lesion (B, white arrow) with distal mucus impaction (B, yellow arrow); there are also nodular metastases (B, red arrows). Bronchoscopy confirmed a metastatic endobronchial melanoma.
Carcinoids are malignant neuroendocrine tumours. About 80% arise within central or segmental bronchi and yield findings related to bronchial obstruction. At CT, calcification is seen in up to 30% of endobronchial tumours (Fig. 2). Metastases occur in about 15% of cases (Fig. 3).
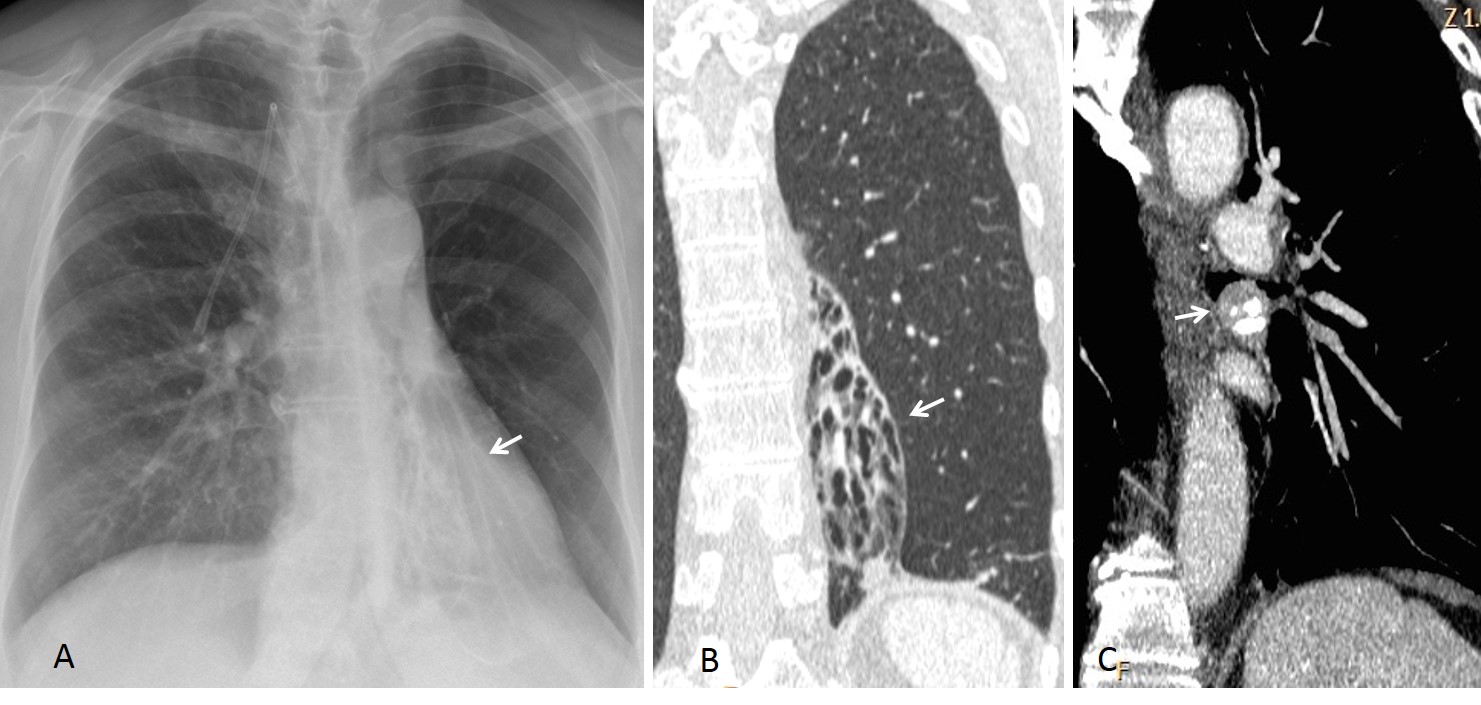
Fig. 2
Fig. 2: 52-year-old woman with chronic cough. PA chest radiograph shows LLL collapse and bronchiectasis (A, arrow). CT confirms the findings (B, arrow) as well as a tumour with coarse calcium at the origin of the LLL bronchus (C, arrow). Diagnosis: typical carcinoid
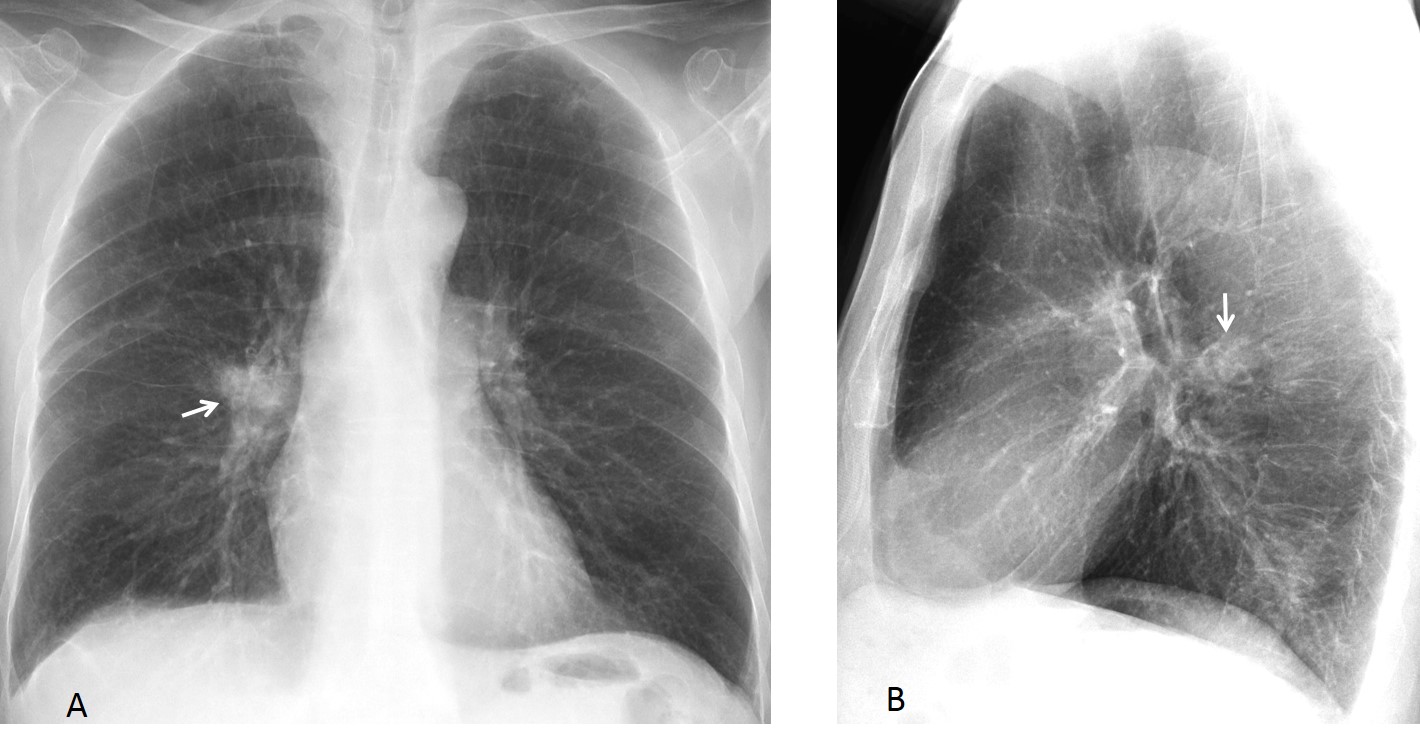
Fig. 3
Fig. 3: 45-year-old man with haemoptysis. Chest radiographs show a nodular lesion behind the right hilum (A,B, arrows).
CT depicts obstruction of a segmental bronchus, with mucus impaction (C, arrow). PET-CT confirms the obstructing tumour (D, arrow), as well as multiple liver metastases (E, arrows). Diagnosis: carcinoid
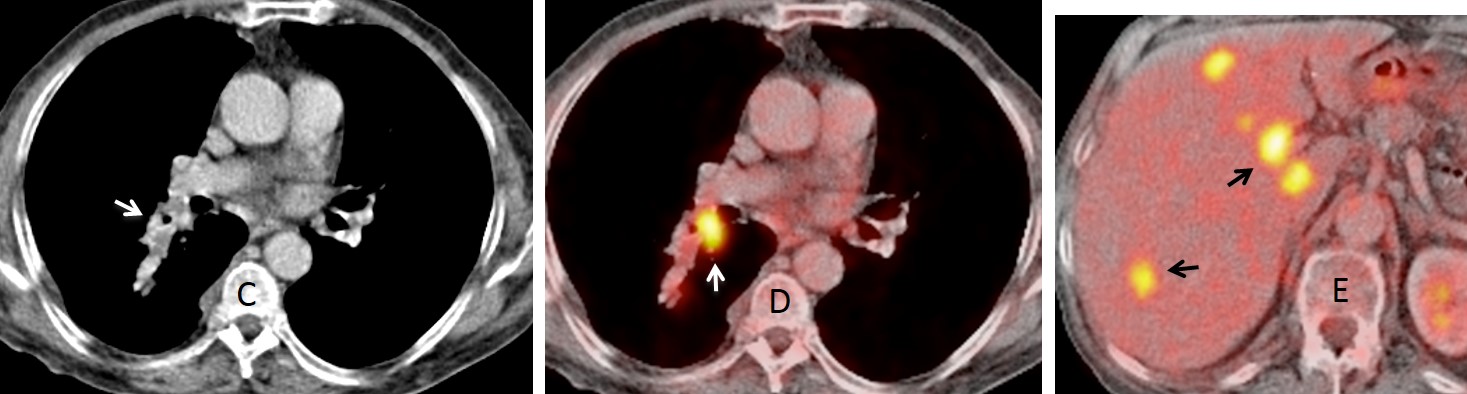
Fig. 3
The main benign endobronchial tumours are hamartomas and lipomas. Hamartoma is the most common benign tumour of the lungs. The great majority appear as solitary pulmonary nodules, and less than 10% are endobronchial. They produce signs of bronchial obstruction on plain films. In about half of them, calcium or fat is visible on CT, which helps in their identification (Fig. 4).
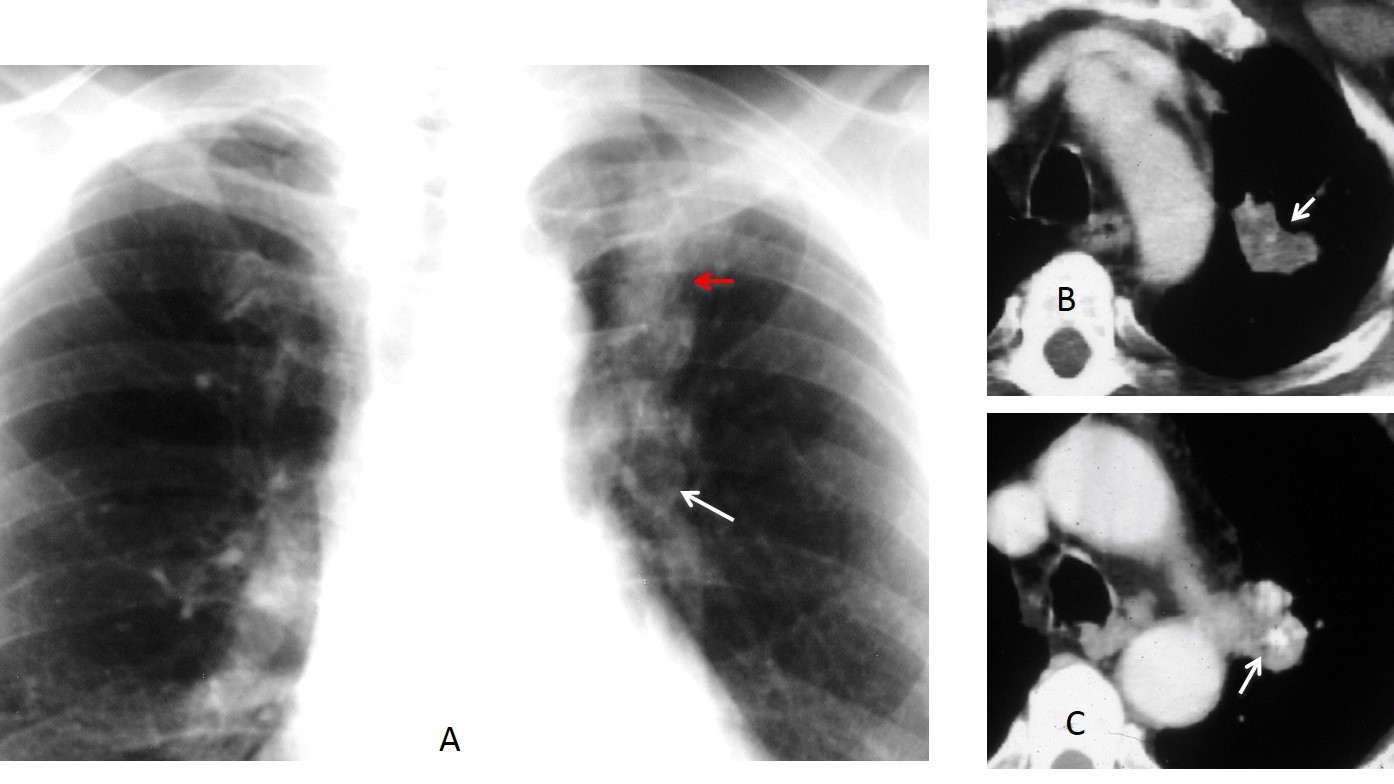
Fig. 4
Fig. 4: 52-year-old man with cough. PA chest film shows elevation of the left hilum (A, white arrow) and bronchial impaction (A, red arrow). Axial CT shows the impacted mucus (B, arrow). A caudal CT depicts the tumour, which contains calcium and fat (C, arrow). Diagnosis: hamartoma.
Endobronchial lipomas, also called lipomatous hamartomas, are tumours mainly comprised of fat. They are easily diagnosed at CT, which readily shows the tumour’s fatty component (Fig. 5). They are usually discovered accidentally in patients with chronic infiltrates or infections (Fig. 6).
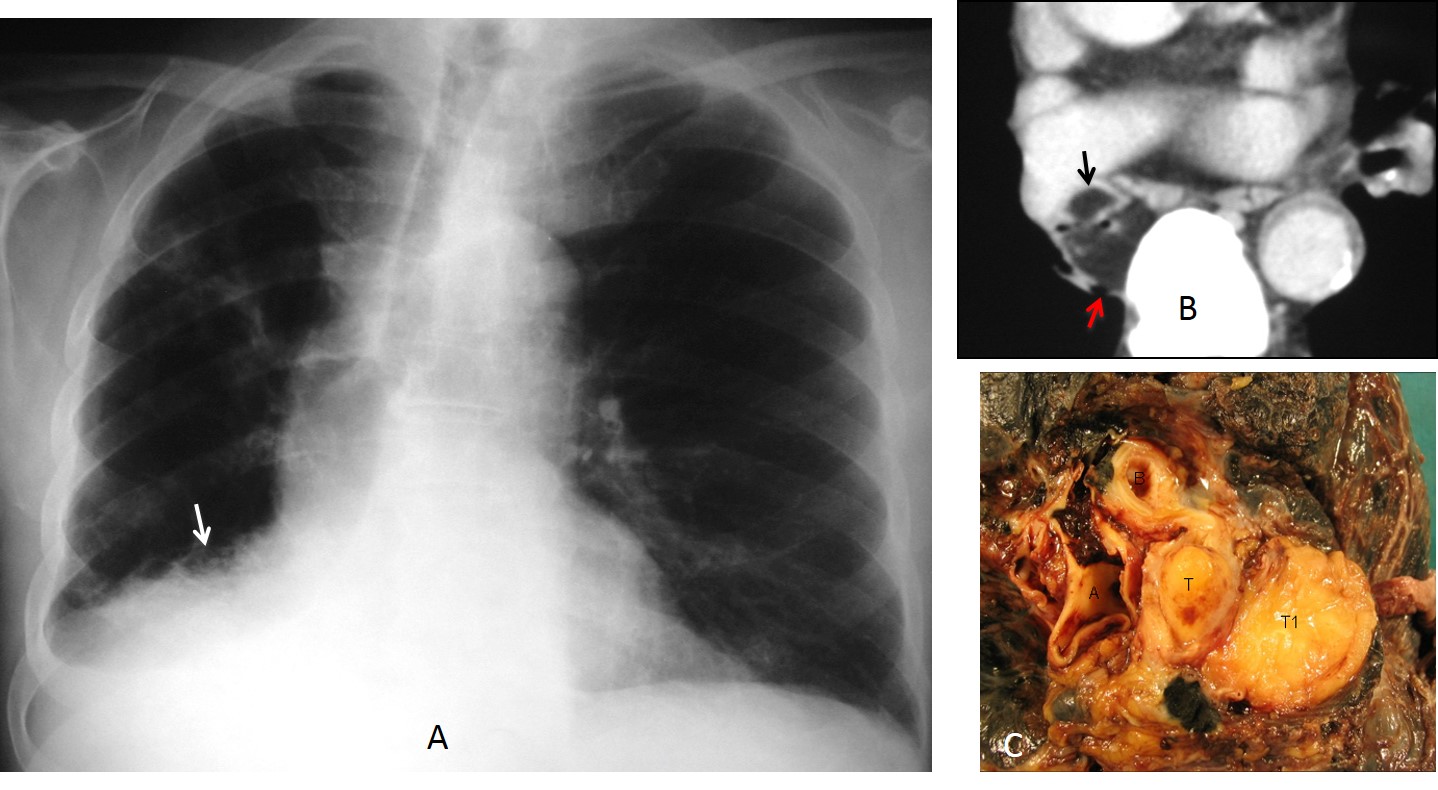
Fig. 5
Fig. 5: 68-year-old man with repeated RLL infections. PA chest film shows a RLL infiltrate (A, arrow). On axial CT, the RLL bronchus is occupied by a fatty tumour (B, black arrow). There is also mediastinal fat (B, red arrow). Specimen (C): T, tumour; T1, mediastinal fat.
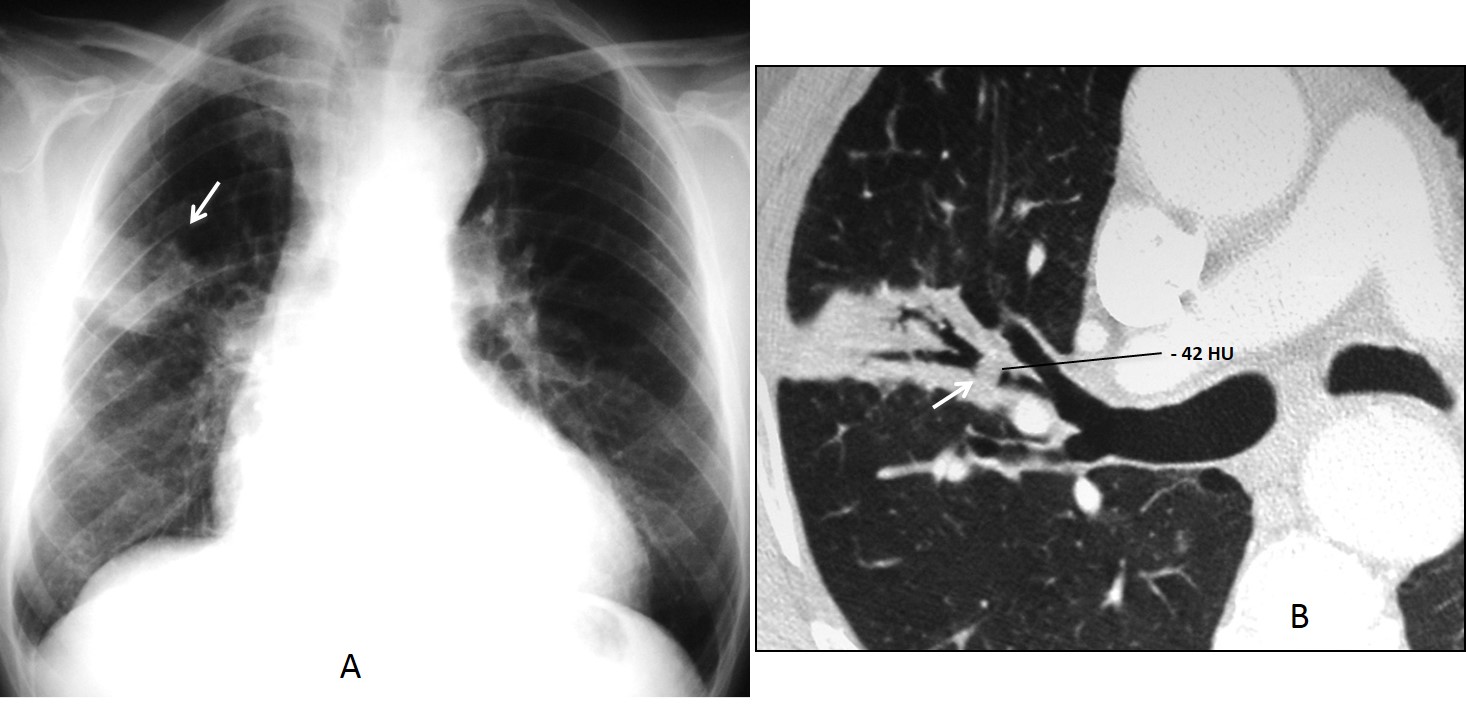
Fig. 6
Fig. 6: 62-year-old man with recurrent RUL infection. PA chest film depicts segmental infiltrate of the RUL (A, arrow). Enhanced axial CT shows a small endobronchial tumour, measuring -42 HU (B, arrow), with distal airspace disease. Diagnosis: lipoma.
Non-tumoural endobronchial lesions are rare. The most common are broncholiths and inhaled foreign bodies. Broncholiths are chunks of calcified lymph nodes that erode the bronchial wall and enter the lumen. They occur in granulomatous diseases (TB, fungal infection, sarcoid, silicosis). CT depicts them as solid calcium within a bronchus, usually accompanied by calcified mediastinal nodes (Fig. 7).
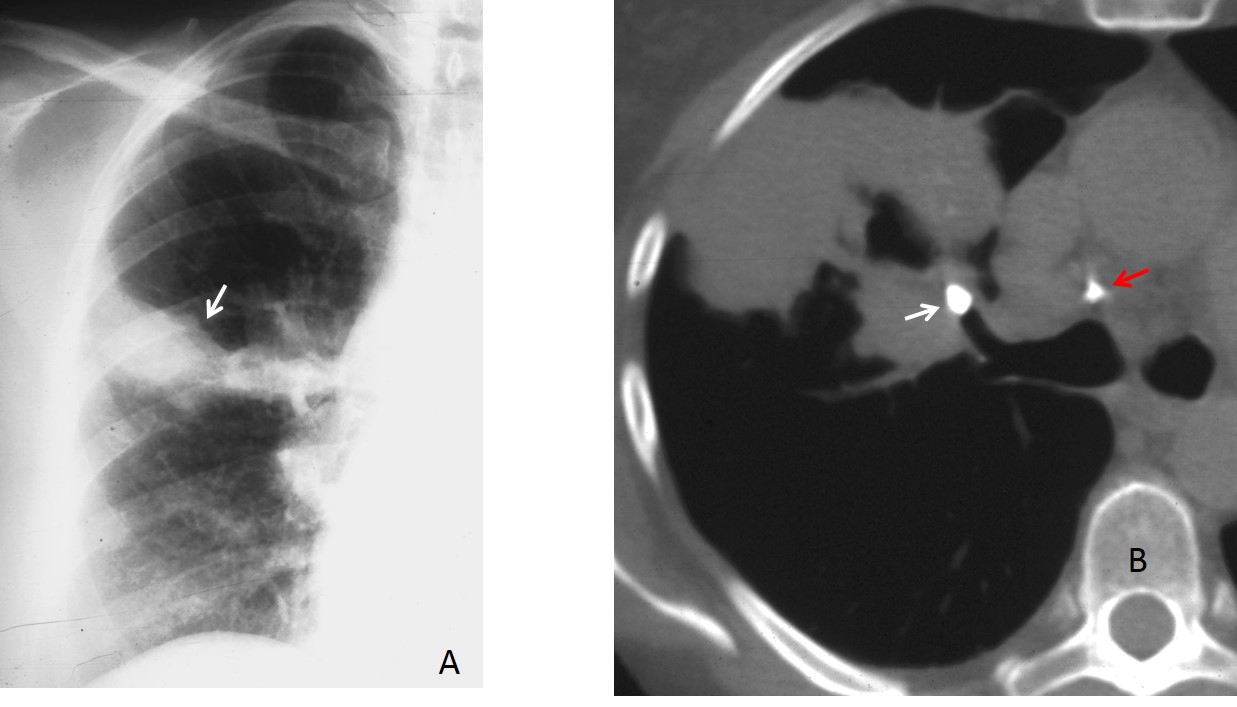
Fig. 7
Fig. 7: 48-year-old man with previous TB and chronic RUL infection. PA chest film shows a segmental RUL infiltrate (A, arrow). Axial CT depicts a broncholith (B, white arrow) obstructing the anterior segmental bronchus. Note calcified mediastinal lymph node (B, red arrow).
It is not unusual for patients with broncholithiasis to cough up some of the calcium. This can be documented by querying the patient or comparing current images with previous CT examinations (Fig. 8).
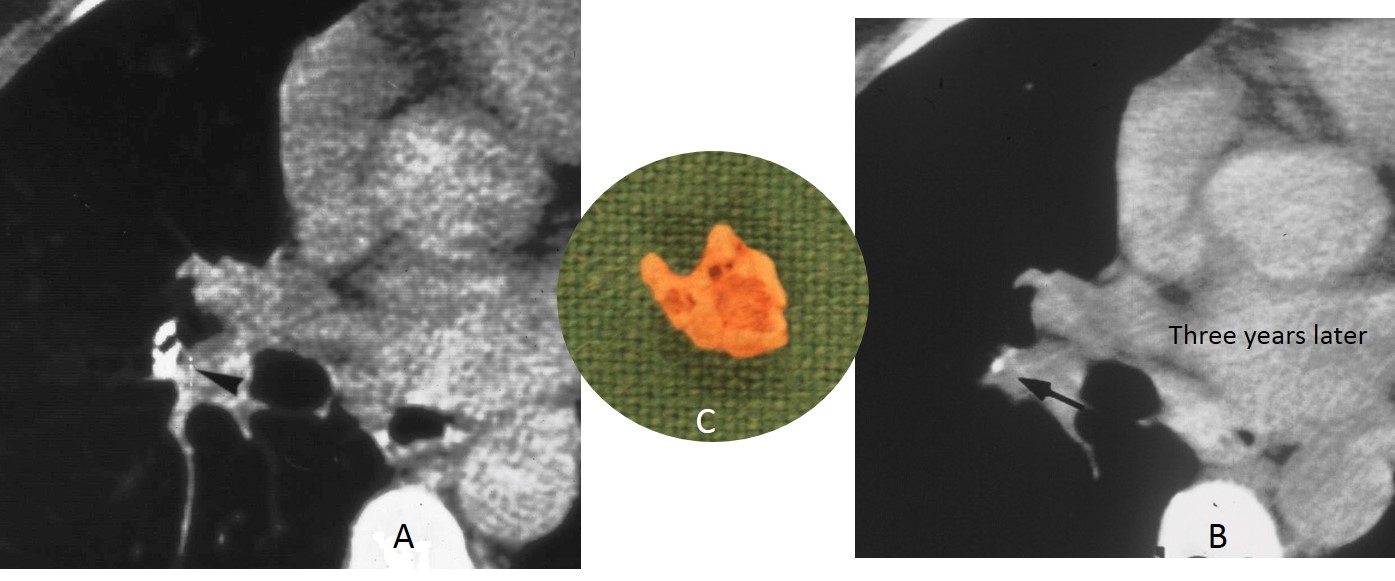
Fig. 8
Fig. 8: axial CT in a patient with healed TB shows calcification in the right hilum (A, arrow). Three years later, most of the calcium has disappeared (B, arrow). The insert (C) shows the broncholith the patient coughed up.
Foreign body inhalation usually occurs in childhood, but it can also happen in adults. The inhaled object usually affects the lower lobe bronchus and causes chronic infection. Foreign body identification is easy when the object is radio-opaque (Fig. 9-10).
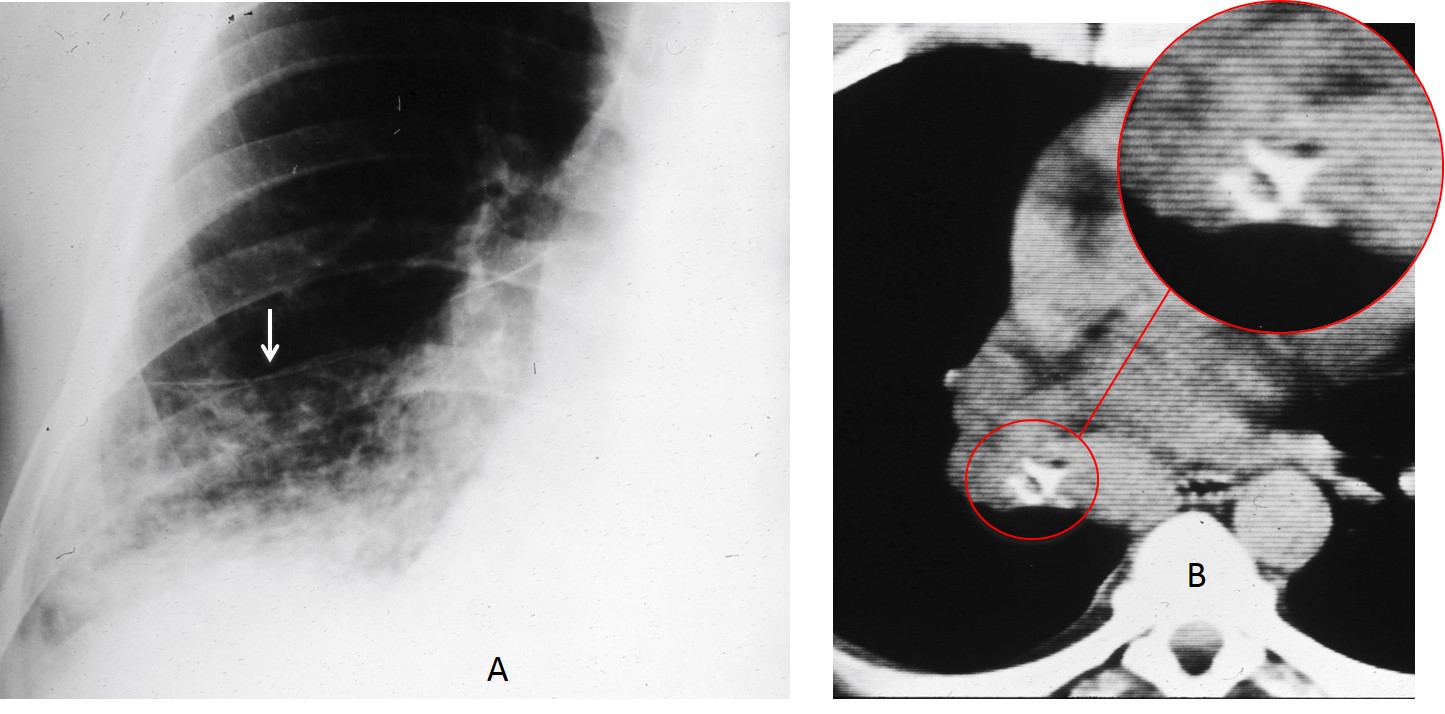
Fig. 9
Fig. 9: 63-year-old patient with chronic RLL infection. PA chest film shows a RLL infiltrate with partial collapse (A, arrow). Axial CT demonstrates a calcified foreign body in the RLL bronchus (B, circle), which, on close inspection corresponds to the vertebra of a small mammal (insert).
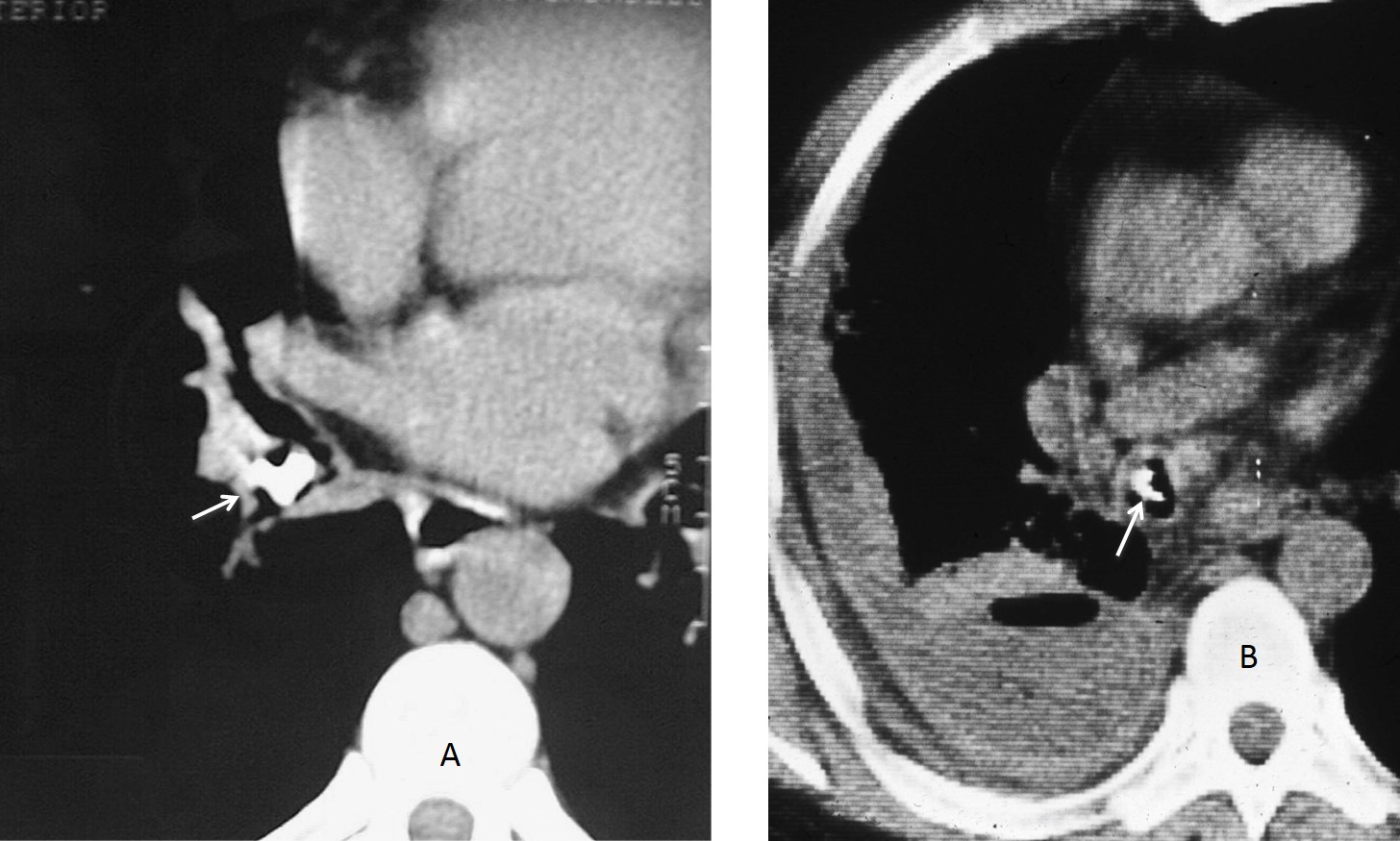
Fig. 10
Fig. 10: two different patients with radio-opaque foreign bodies in a RLL bronchus: a bone (A, arrow) and a pistachio shell (B, arrow).

Follow Dr.Pepe’s Advice:
1. Bronchogenic carcinoma is, by far, the most common endobronchial lesion.
2. Carcinoid and endobronchial metastases are the second malignant cause.
3. Fat in a tumour suggests hamartoma or lipoma.
4. Foreign bodies and broncholiths are non-tumoral endobronchial lesions.


4
Laconic
– there is complete radiopacity of the right lung with out shifting to the left or to the right of mediastinum (pleural efiusion – collaps))
– swelling of the right hilum
– pulmonary nodes on the left.
that make me suspicious is that, i think i can see both diaphragms on the lateral view.
my First choice is 2 Metastases
meigs syndrome
Meigs syndrome disappear after ovary tumor resection and it is associated with begin ovary tumors.
I agree with Gus’s description. Also there is an amputation of the right main bronchus. I cannot rule out a primary lung cancer protruding into right main bronchus with collapse and pleural effusion.
Gus clearly describe findings:)
but I’m not sure that metastases could cut off bronchus like that.
I think it’s probably carcinoma of the lung in right bronchi with metastases in left lung.
Any endobronchial lesion (metastases, carcinoid, etc.)
may give the same appareance than a primary lung carcinoma. Of course, carcinomas are more frequent.
…..regola KISS….CR ovarico…..atelettasia polmone dx( da metastasi endbronchiale)….metastasi polmonari a sx…..
Congratulations, my friend. Seems you are finally applying the KISS approach!
…grazie MITICO Professore, sopratutto per i meravigliosi insegnamenti !!!!!!!
I could not appreciate the right diaphragmatic copula in both PA and lat views, with rather homogenous opacification of the right hemithorax with cutting off the right main bronchus, and no shift of the mediastinum, for me concomitant right lung resection with the ovarian intervention is the reasonable clue, vote for 4!
No previous surgery. Sorry.
A complete ‘white out’ of the right lung slight tracheal shift to the right. i think there is a lesion occluded the right main bronchus; TB? Tumour?FB?
complete obstruction of the right main bronchus as a bronchus ca
Endobronchial tuberculosis
2
Late on Thursday I can tell that the diagnosis is enodbronchial metastases. More informationa baout endobronchial lesions tomorrow.
Congratulations to Gus, who suggested the diagnosis a few hours after the case was posted.
I Belive that the option 2 (metastases) Is right.
professor can you give me an hint about the kiss approach?