Dr. Pepe’s Diploma Casebook: Case 71 – SOLVED!
Dear Friends,
After a short interlude, I am back with radiographs of a 71-year-old smoker with dyspnoea and haemoptysis. Previous history of TB. Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
PS. Good luck to everyone taking the European Diploma in Radiology examinations at ECR 2015 this week!
Diagnosis:
1. Active TB
2. Carcinoma of the lung
3. Bronchiectasis
4. None of the above

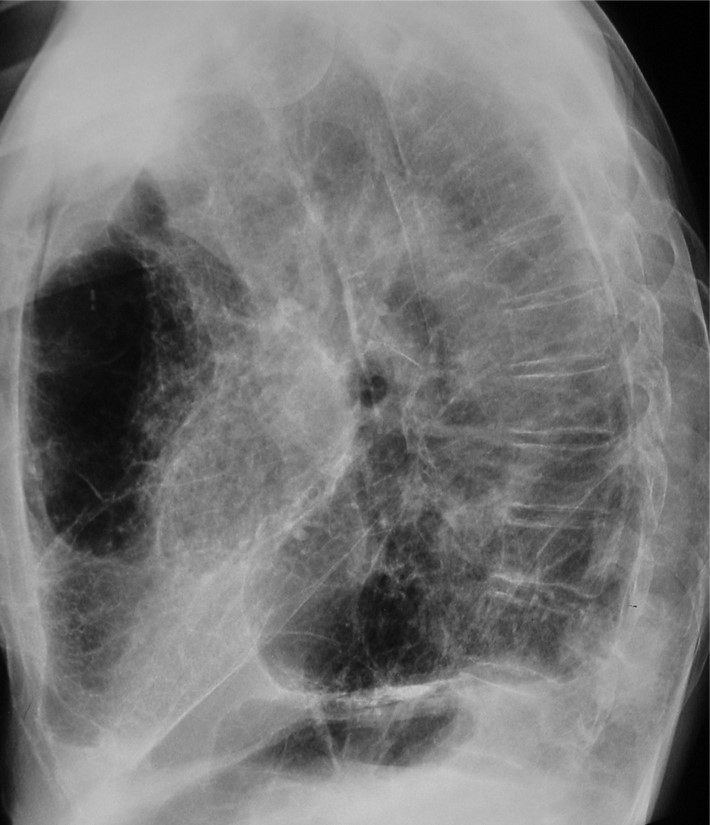
Findings: there are obvious signs of pulmonary emphysema and pleural calcification in the left hemithorax and hemidiaphragm (A,B white arrows), secondary to previous TB. The most important finding is a posterior lung mass easily seen in the lateral view (B, red arrows) and barely visible in the PA view (A, red arrow).
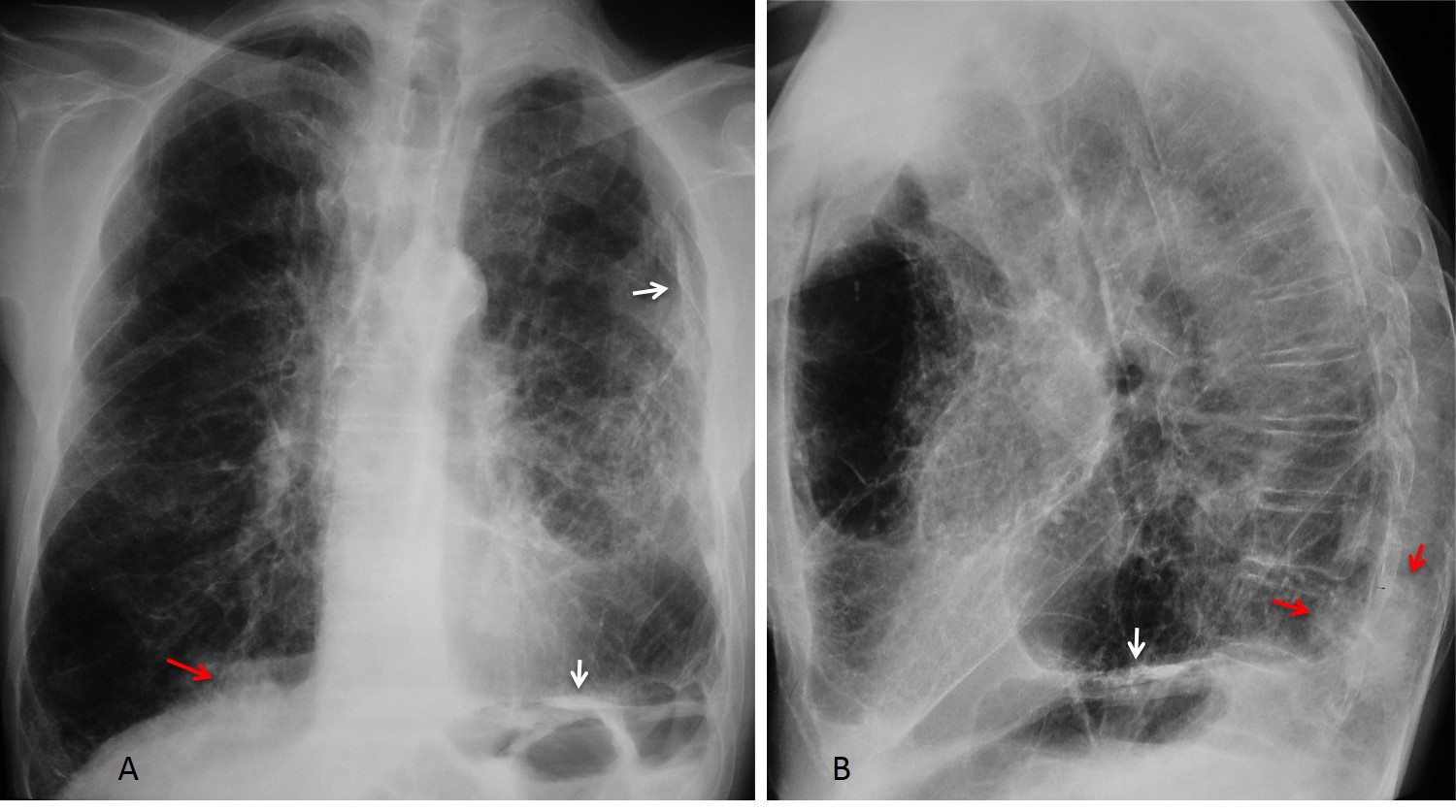
Coronal and sagittal confirm the emphysematous changes and the mass in the right lower lobe (C,D arrows). Needle biopsy demonstrated a carcinoma.

Final diagnosis: Chronic lung disease and carcinoma of the lung.
This case is presented to discuss an area in the lateral chest radiograph known as the posterior clear space. This refers to the space between the oblique posterior diaphragm and the chest wall (A, shaded area). The posterior clear space is hidden in the PA view by the dome of the diaphragm (B, shaded area).
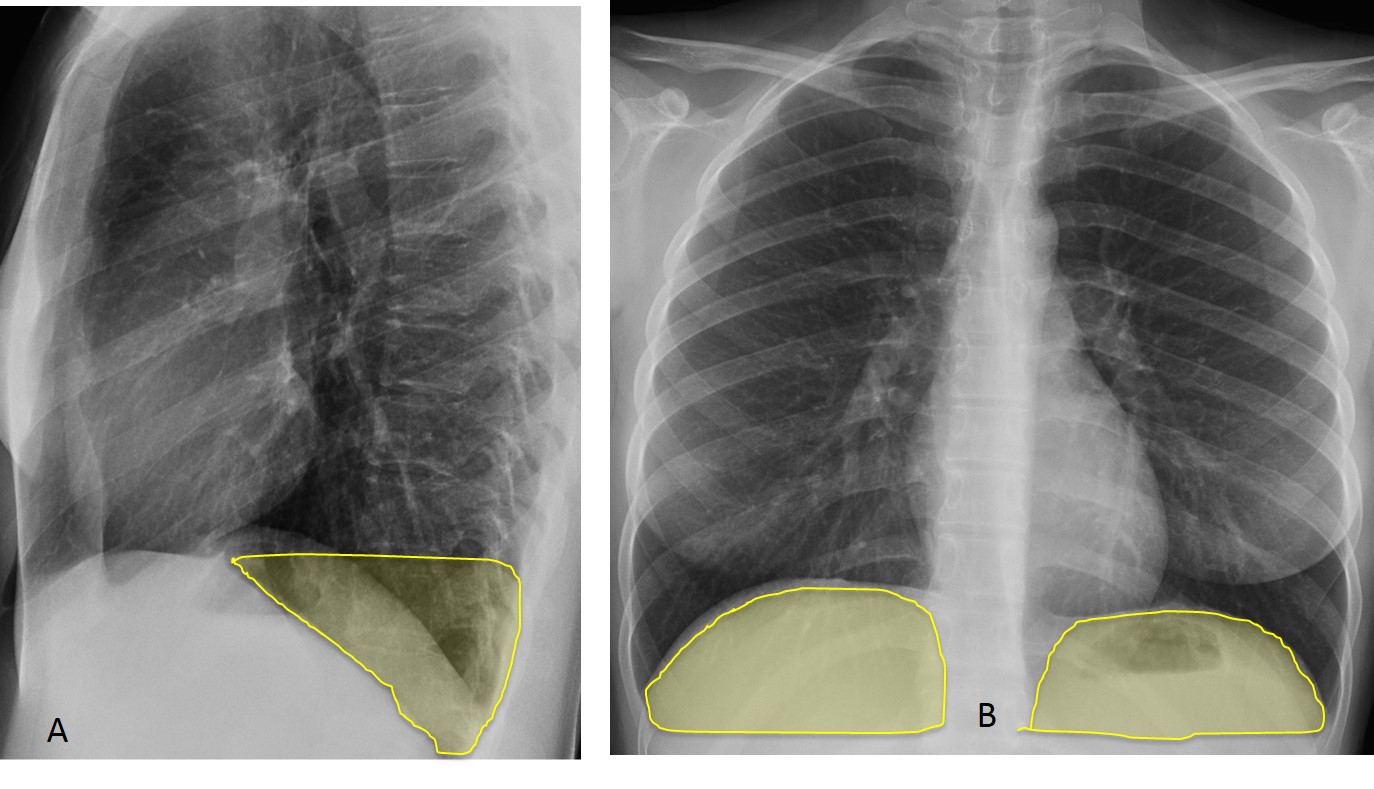
The posterior clear space is important because abnormalities in this area may not be depicted in the PA projection, being hidden by the diaphragm. The abnormal features may be easily visible in the lateral view.
Processes in the posterior clear space may arise from the lung, pleura, or diaphragm. Like the pulmonary apices, the posterior clear space is a narrow region, hence the origin of the abnormality may be difficult to determine. In most cases, CT is needed to confirm the finding and determine the origin.
In this presentation I have not included vertebral lesions and lower posterior mediastinal masses because these lesions can usually be suspected based on features in the PA view.
Pulmonary processes in the posterior clear space may be due to pneumonia, pulmonary infarction, or tumours. The most common cause is lower lobe pneumonia, which may not be visible in the PA view, but is easily discovered in the lateral view. The pneumonic infiltrate is seen as an ill-defined opacity of the lower lung with blurring of the posterior diaphragmatic contour (Figs. 1 and 2)

Fig. 1
Fig. 1: 30-year-old male with cough and fever. PA chest film (A) shows no significant findings.
The lateral view depicts a pulmonary opacity in the posterior clear space (B, arrow) that blurs the right diaphragmatic contour.
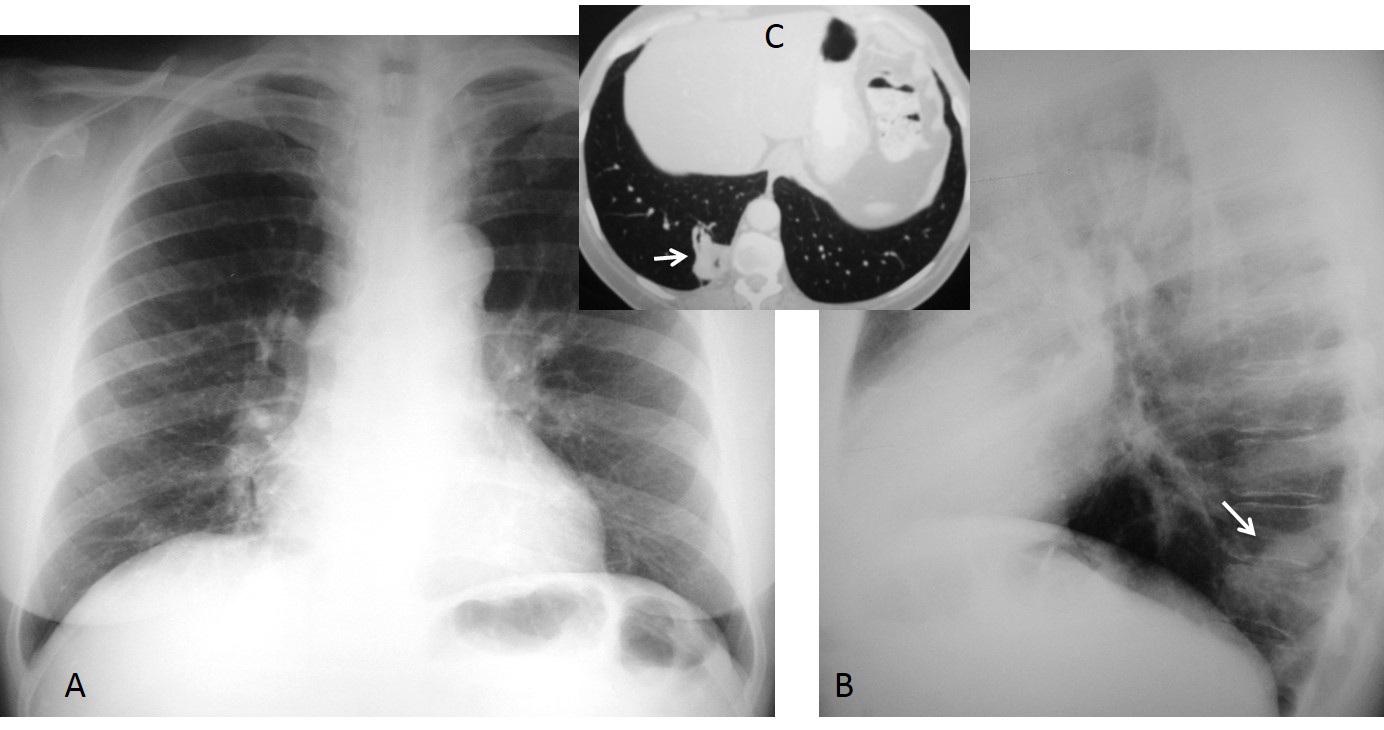
Fig. 2
Fig 2: 42-year-old man with carcinoma of the colon and fever. Lateral view shows a nodular opacity in the posterior clear space (B, arrow), not visible in the PA view (A). Axial CT confirms an irregular lesion in the RLL (C, arrow). A metastatic nodule was suspected, but the lesion disappeared with antibiotic treatment. Diagnosis: acute pneumonia.
Pulmonary infarction is usually located at the costophrenic sulcus and produces the typical Hampton hump sign. When the infarct is in the posterior costophrenic angle, it is not visible in the PA chest film, but is easily detected in the lateral film (Fig. 3).
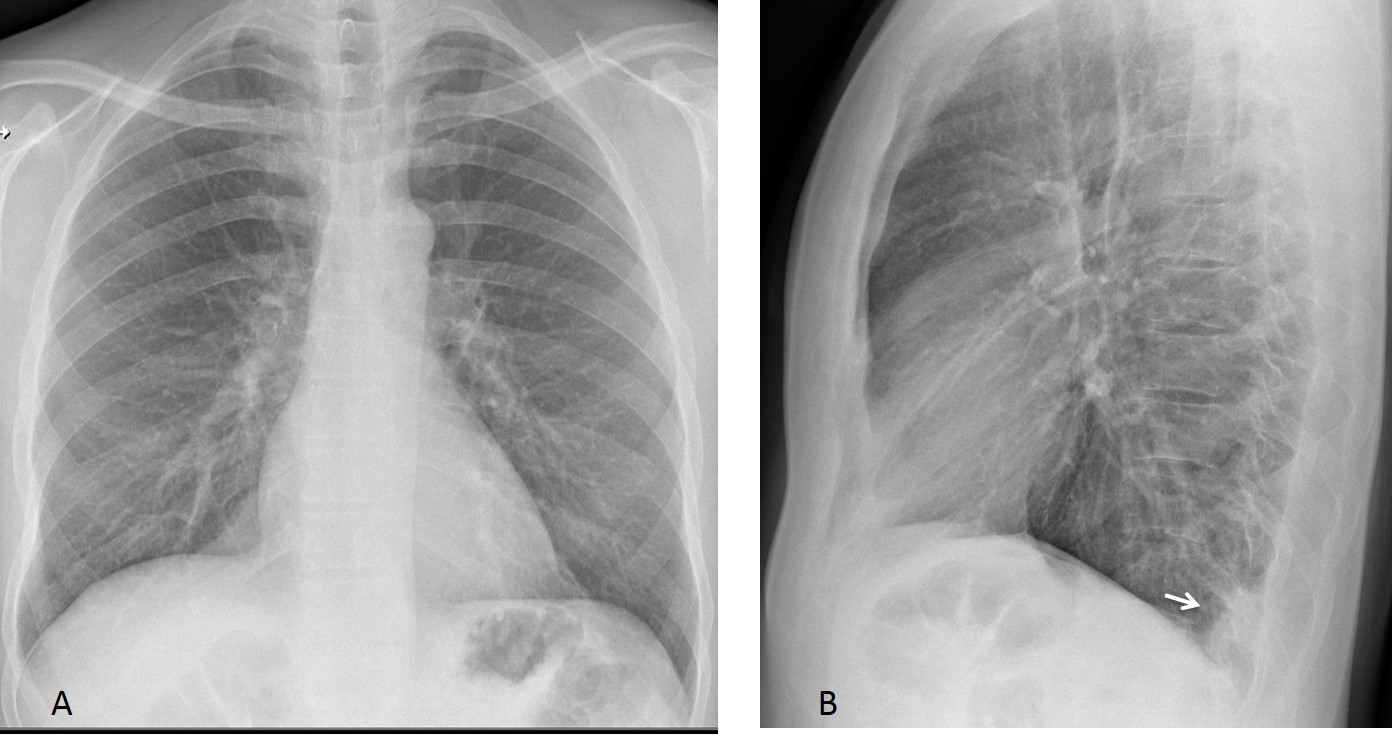
Fig. 3
Fig. 3: 54-year-old male with sudden chest pain. The PA chest (A) is unremarkable. The lateral view shows a Hampton hump in the posterior costophrenic sulcus (B, arrow).
Enhanced sagittal CT confirms the Hampton hump (C, arrow) and the embolus in a segmental artery (D, arrow).
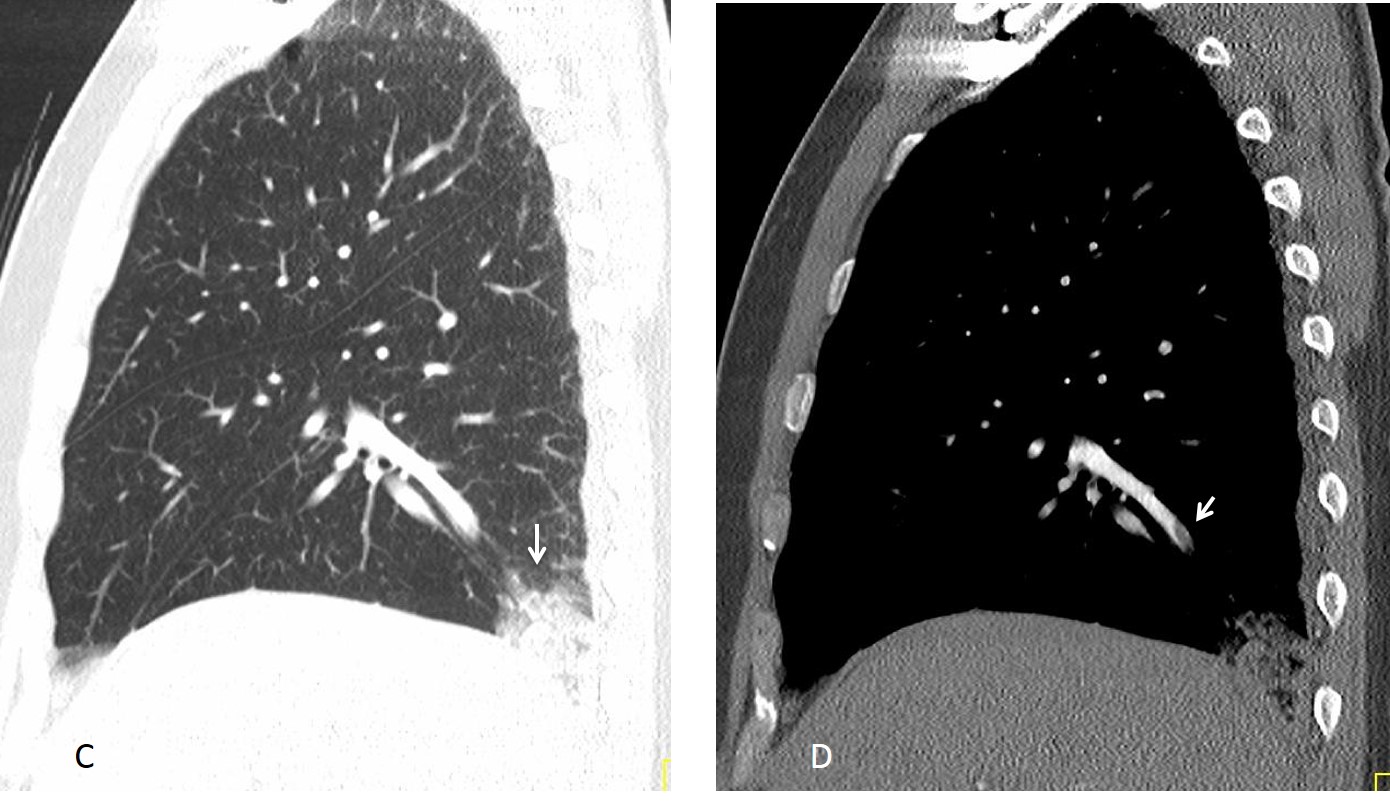
Fig. 3
Lung tumours occasionally lodge in the posterior costophrenic sulcus, as in the case shown initially. The images below show a similar case, in which the tumour was discovered in the posterior clear space (Fig. 4).
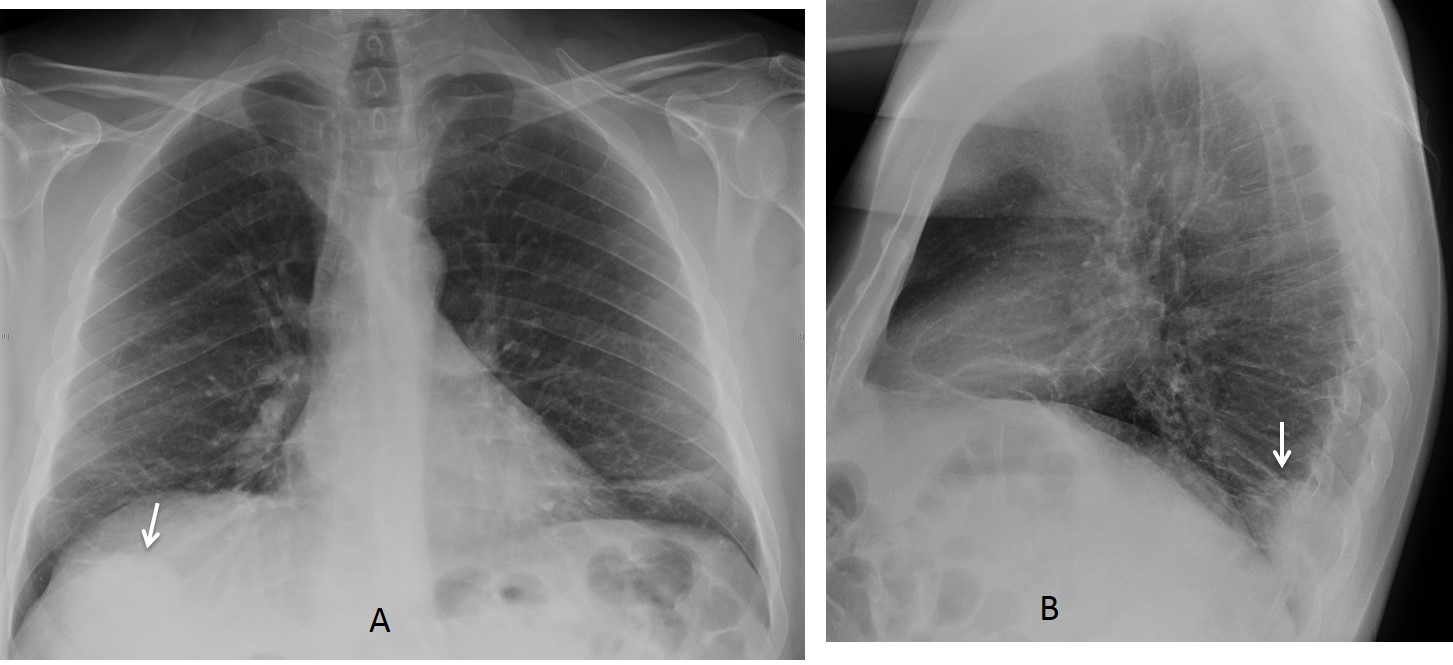
Fig. 4
Fig. 4: 56-year-old asymptomatic male. Lateral view of the chest shows an obvious mass in the posterior clear space (B, arrow), identified in retrospect behind the right hemidiaphragm (A, arrow).
Coronal and sagittal CT demonstrate a round-shaped necrotic lung tumour (C and D arrows). Final diagnosis: carcinoma of the lung.
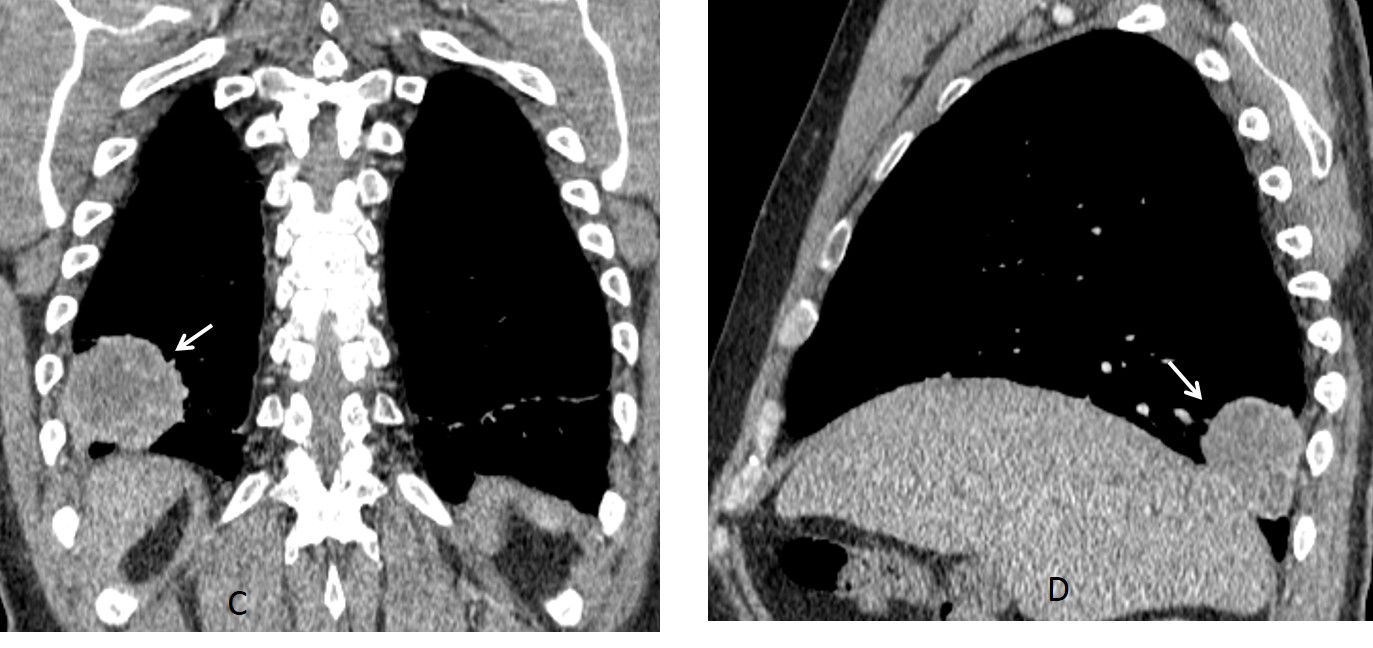
Fig. 4
Pleural fluid is the most common cause of obliteration of the posterior costophrenic sinus. Small amounts of fluid may be invisible in the PA view and easily seen in the posterior clear space in the lateral radiograph and recognized because of the typical concave shape (Fig 5).
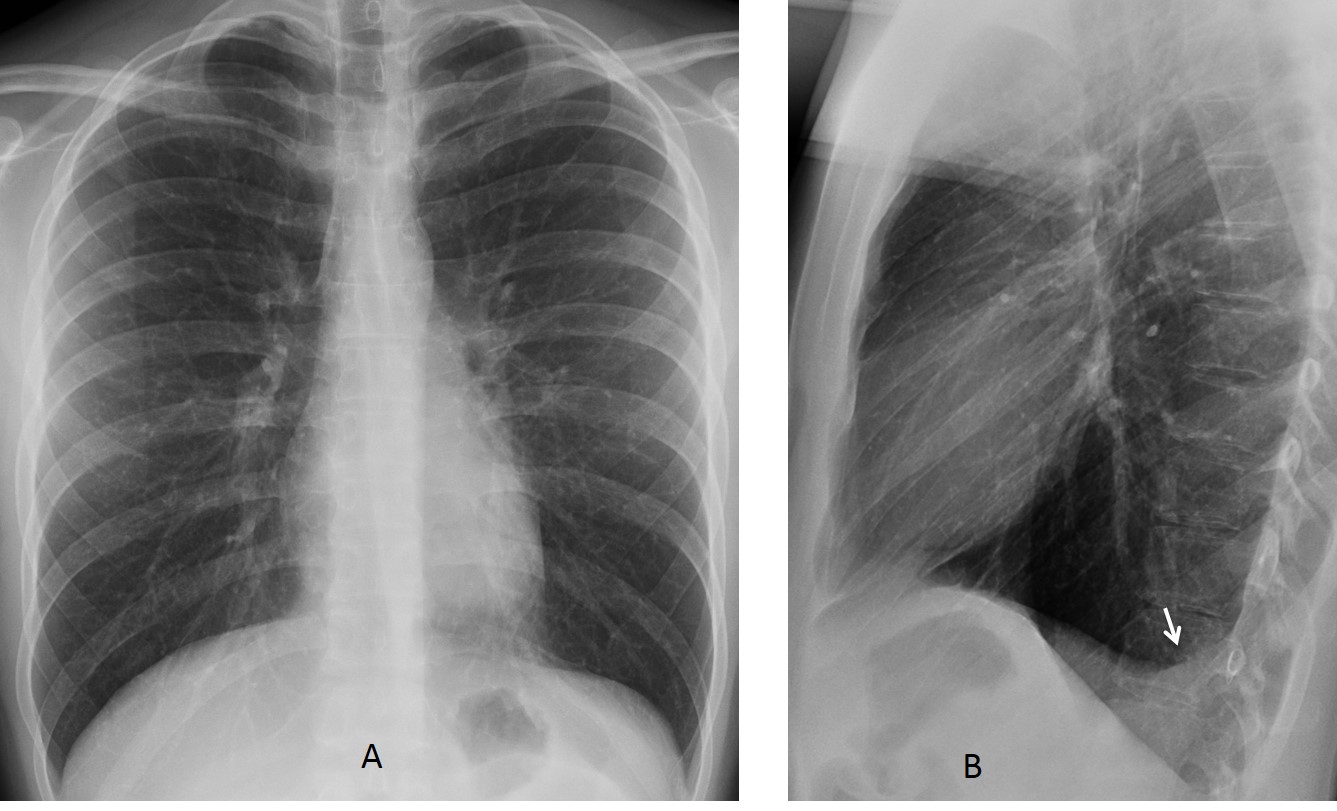
Fig. 5
Fig. 5: 29-year-old male with pleuritic pain. PA view (A) is unremarkable. Lateral view (B) shows the typical appearance of free pleural fluid in the posterior sulcus (arrow).
In rare cases, isolated pleural tumours may be located in the posterior clear space. As was mentioned earlier, CT is needed to determine the origin of the tumour (Fig. 6).

Fig. 6
Fig. 6: 48-year-old man with renal carcinoma. The lateral chest radiograph shows a round opacity in the posterior clear space (B, arrow), that was not visible in the PA view (A).
Lung metastasis was suspected. Sagittal CT shows a posterior extrepulmonary lesion (C, arrow) that did not enhance on PET-CT (D, arrow). Surgical diagnosis: fibrous tumour of pleura.
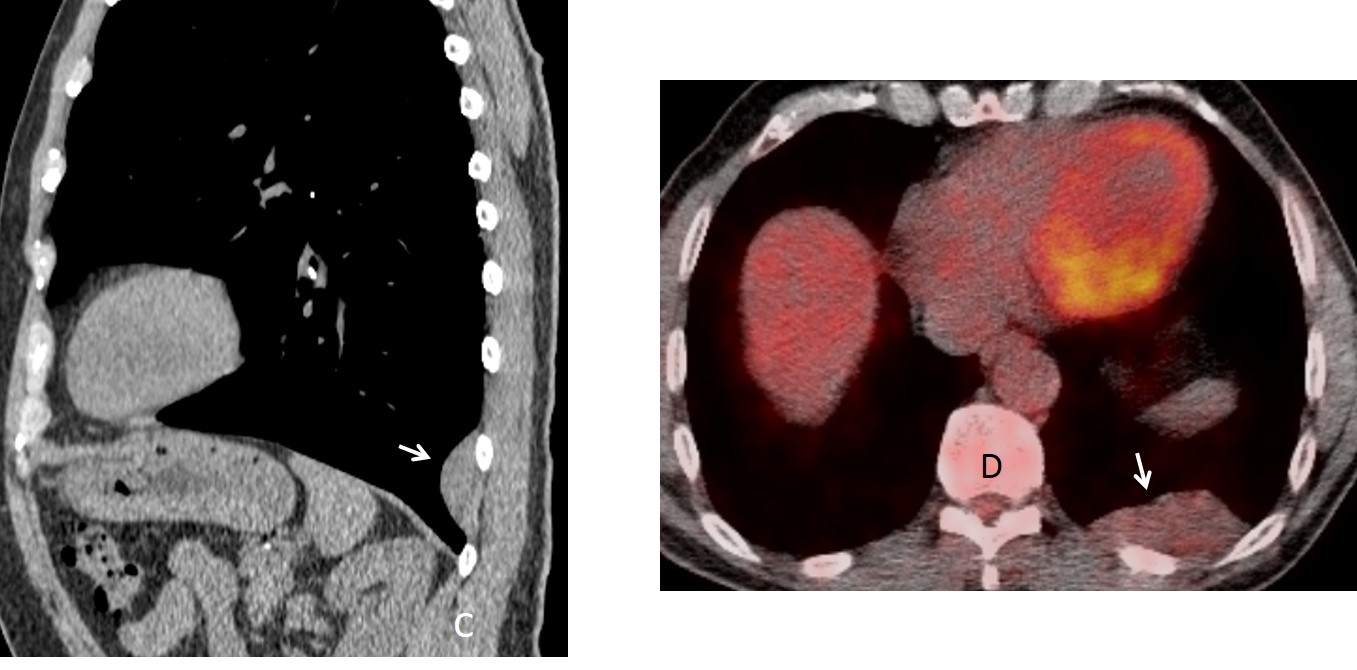
Fig. 6
Posterior Bochladek hernias are a common cause of opacities in the posterior clear space. The hernias result from weakening of the muscle fibers of the diaphragm, with protrusion of abdominal fat. The incidence increases with age. Bochladek hernia occurs in up to 10% of elderly individuals (Figs. 7 and 8).
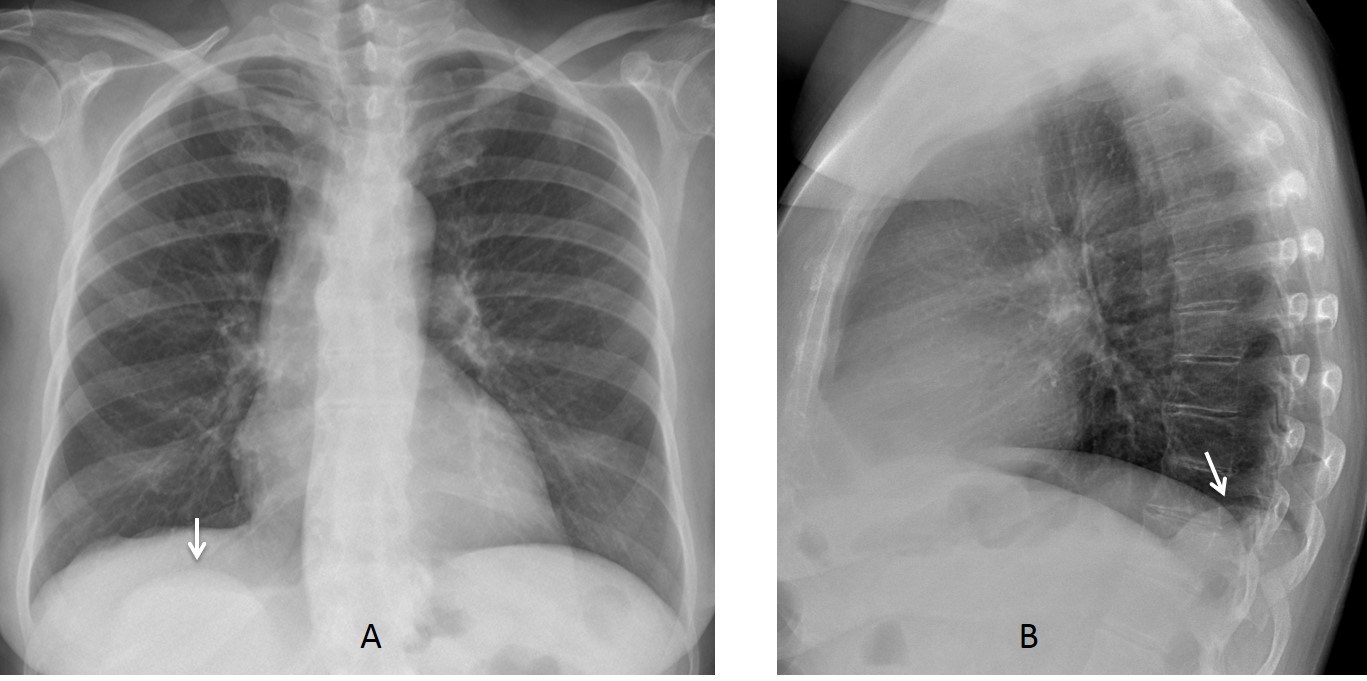
Fig. 7
Fig. 7: 72-year-old woman with a round opacity in the posterior sulcus (B, arrow), visible in the PA view behind the diaphragmatic shadow (A, arrow).
Unenhanced axial CT shows that the opacity is composed of fat (C, arrow). Sagittal CT confirms fat herniation through a hiatus in the diaphragm (D, arrow).
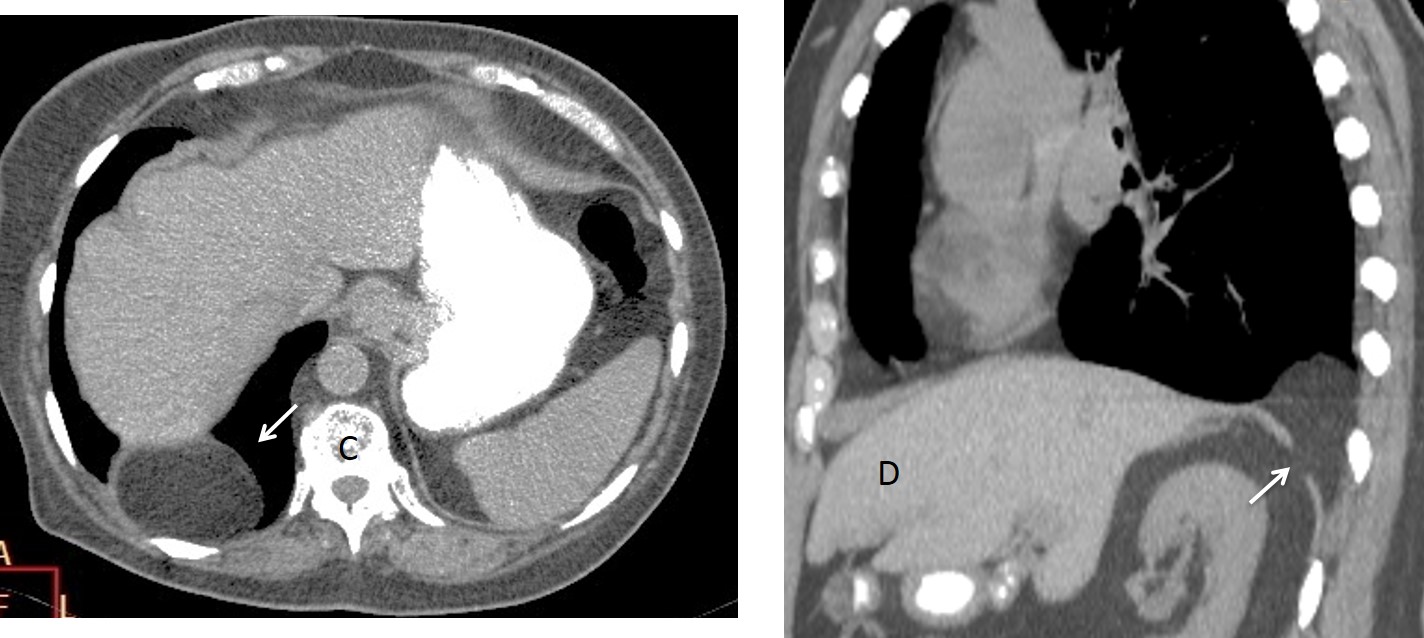
Fig. 7
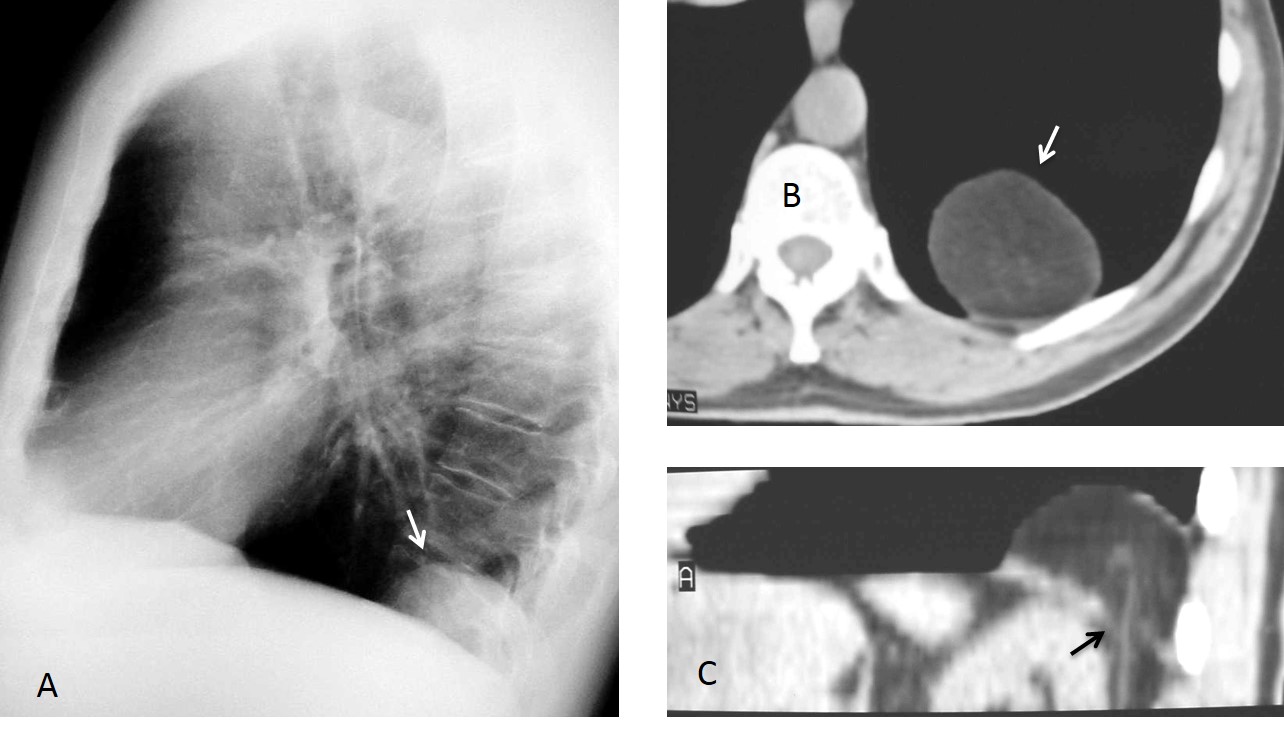
Fig. 8
Fig. 8: 65-year-old asymptomatic man with Bochladek hernia. Lateral chest film depicts a posterior mass (A, arrow). Axial CT demonstrates fat (B, arrow), which is herniating through a defect in the posterior diaphragm (C, arrow). Note the retroperitoneal vessel passing through the breach.

Follow Dr.Pepe’s Advice:
1. It is important to look at the posterior clear space in the lateral view because some lesions are only visible in that projection.
2. Lesions in the posterior clear space may arise from the lung, pleura or diaphragm.
3. Due to the narrowness of the space, CT is usually needed to determine the origin of the lesion.


1. Active TB
Active TB
Bronchiectasis
active TB
ACTIVE TB
active tuberculosis
Carcinoma probably of the lung which is seen on the lateral projection near the vertebra
none of the above
Seems that most of you selected active TB. Why?
A mí me parece que este paciente tiene una paquipleuritis izquierda probablemente secundaria a TBC antigua y por ello vemos las calcificaciones pleurales y la afectación parenquimatosa de aspecto crónico cicatricial en hemitórax izquierdo. Además se observa una hiperclaridad pulmonar derecha que indica enfisema. No veo indicios de TBC activa puesto que no hay imágenes cavitadas ni ningún infiltrado que indique diseminación broncógena que sería indicativo de TBC activa.
Tampoco veo ningún nódulo ni masa que me sugiera que el paciente tiene una neoplasia.
En cuanto a las bronquiectasias, yo optaría por esta opción. Sinceramente no sé verlas en esta radiografía pero con los cambios crónicos secundarios a la TBC es muy probable que este paciente tenga bronquiectasias por tracción. Así que recapitulando, las 3 causas más frecuentes de hemoptisis son TBC, neoplasia y bronquiectasias, descartando las 2 primeras me quedo con ésta última.
Has mirado bien?
Blunting of Ltd cannot angle suggest active disease
Central ca
rcinoma of the left lung
None of the above
….CARISSIMO PROFESSORE….NON SI PUO’ RISPONDERE ALLE TRE IPOTESI DIAGNOSTICHE DA TE AVANZATE SULLA BASE DI SEMPLICI RADIOGRAFIE, IN QUANTO TUTTE E TRE LE IPOTESI , IN QUESTO CASO SONO VALIDE….ECCO PERCHE’ , IN QUESTI Casi la TC è FONDAMENTALE !!!! Con stima da Bari….
Dear friend, sorry to disagree with you. Looking carefully may give an answer
Carcinoma of the lung.On the lateral projection, down, after vertebta Th9 – opacity.
Hola
Hay zonas fibrocicatriciales supongo que por la TB antigua. También veo áreas quisticas de pared fina que me parecen muy grandes para ser bronquiectasias y que no tienen nivel por lo que no están sobre infectadas ni veo consolidaciones así que una TB activa tampoco me lo parece.
Ademas veo un nódulo/masa retro cardíaco que no puedo descartar que se trate de una neo de pulmón.
Por ultimo hay una perdida de volumen del pulmón izquierdo, que creo que es crónico.
Me quedo con la 2 carcinoma de pulmón
Despite all the fibrotic and emphysematous changes I think Left- sided empyema should be considered…
Pleural empyema…
Also retrocardiac tumor is possible
Bronchiectasis
2. Carcinoma of the lung
The most significant finding is a large nodule in the posterior clear soace in the lateral. Carcinoma of the lung is the most likely diagnosis. More information tomorrow.
Congratulations to Madzia, who was the first to mention the right diagnosis
bronchiactasis