Dr. Pepe’s Diploma Casebook: Case 72 – SOLVED!
Dear Friends,
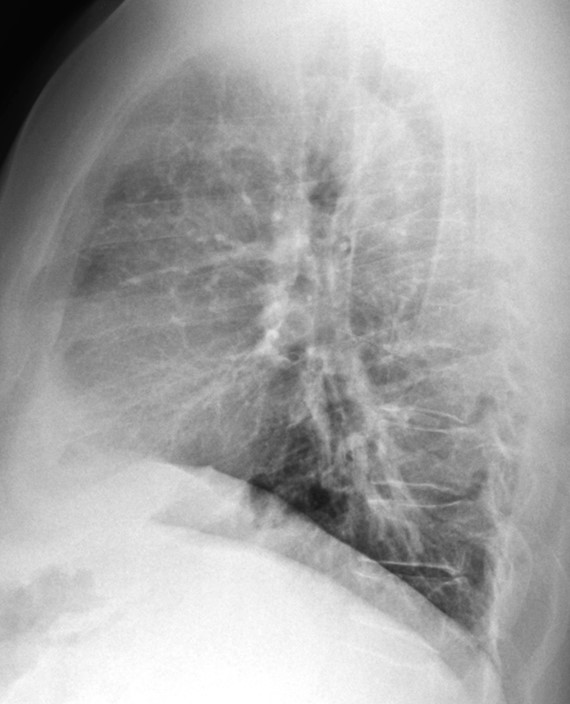
Today I am presenting radiographs of a 51-year-old man with low-grade fever and malaise. Previous history of car accident.
Do you see any abnormalities?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.

Findings: PA chest film shows thickening of the right paratracheal line (A, arrows). There is an old compression fracture at T-11, seen in the lateral view (not shown). Coronal and axial CT show large paratracheal lymph nodes (B,C arrows).
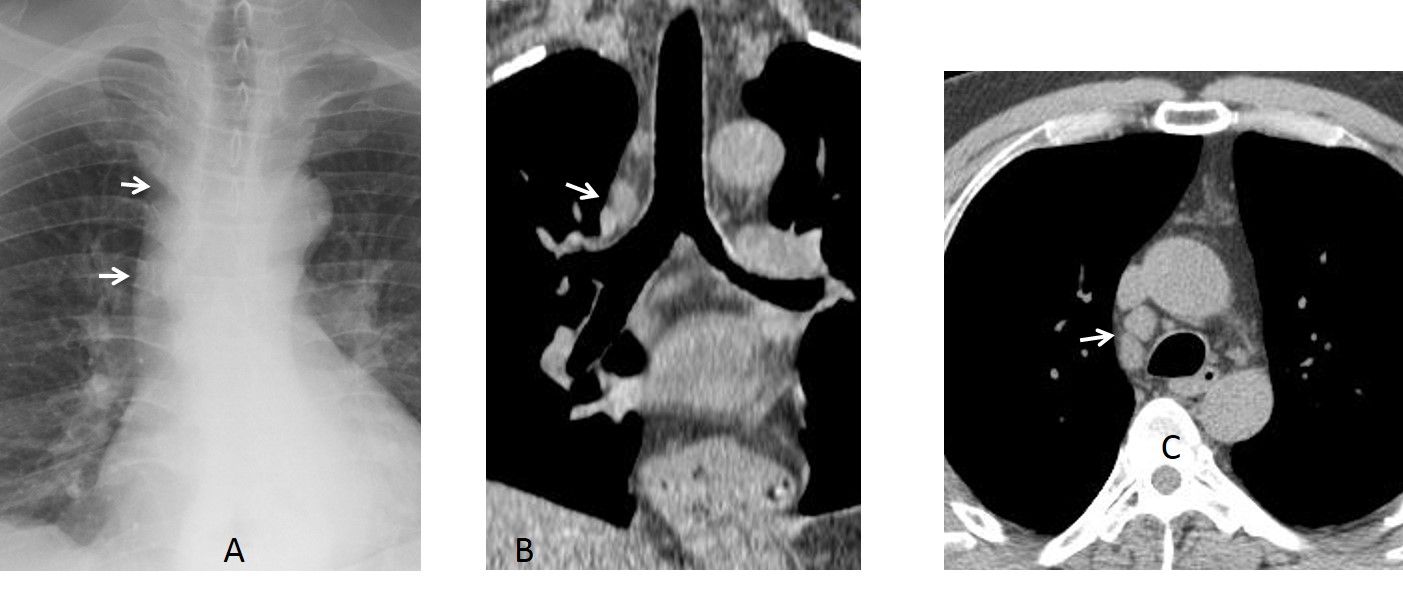
Final diagnosis: lymphoma
It is common knowledge that mediastinal masses are discovered on chest radiography and confirmed and diagnosed by cross-sectional studies. A problem arises when the abnormality is not obvious in the plain film, it is overlooked, and further imaging is not performed.
In this presentation, I’d like to discuss how to discover small masses that are not easily seen in the initial chest examination. To recognise subtle abnormalities, we have to be familiar with mediastinal anatomy, represented by the mediastinal lines.
Mediastinal lines derive from the relationship between air and the soft-tissue structures of the mediastinum. There are two types: lines and interfaces. True lines are outlined by air on both sides, whereas interfaces have air on only one side. This distinction is important for diagnostic purposes: abnormal lines become thickened, whereas interfaces are displaced outwards (Fig. 1).
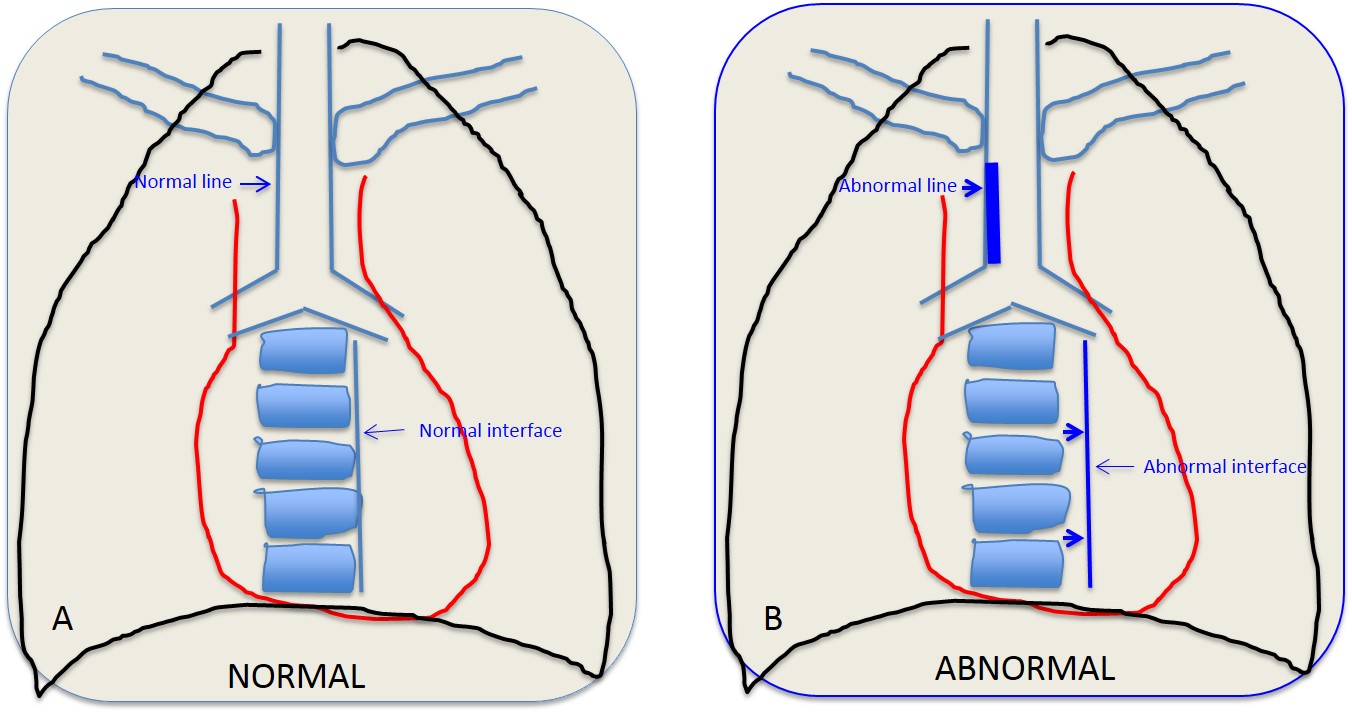
Fig. 1
Fig. 1: Drawings depicting normal and abnormal lines and interfaces. In A, the paratracheal line is thin and the paraspinal interface is close to the spine. In B, the paratracheal line is thick and the paraspinal interface is separated from the spine.
True mediastinal lines are located in the upper mediastinum. In the PA view, the most common are the anterior and posterior junction lines and right paratracheal line (Fig. 2), and in the lateral view, the posterior tracheal line.
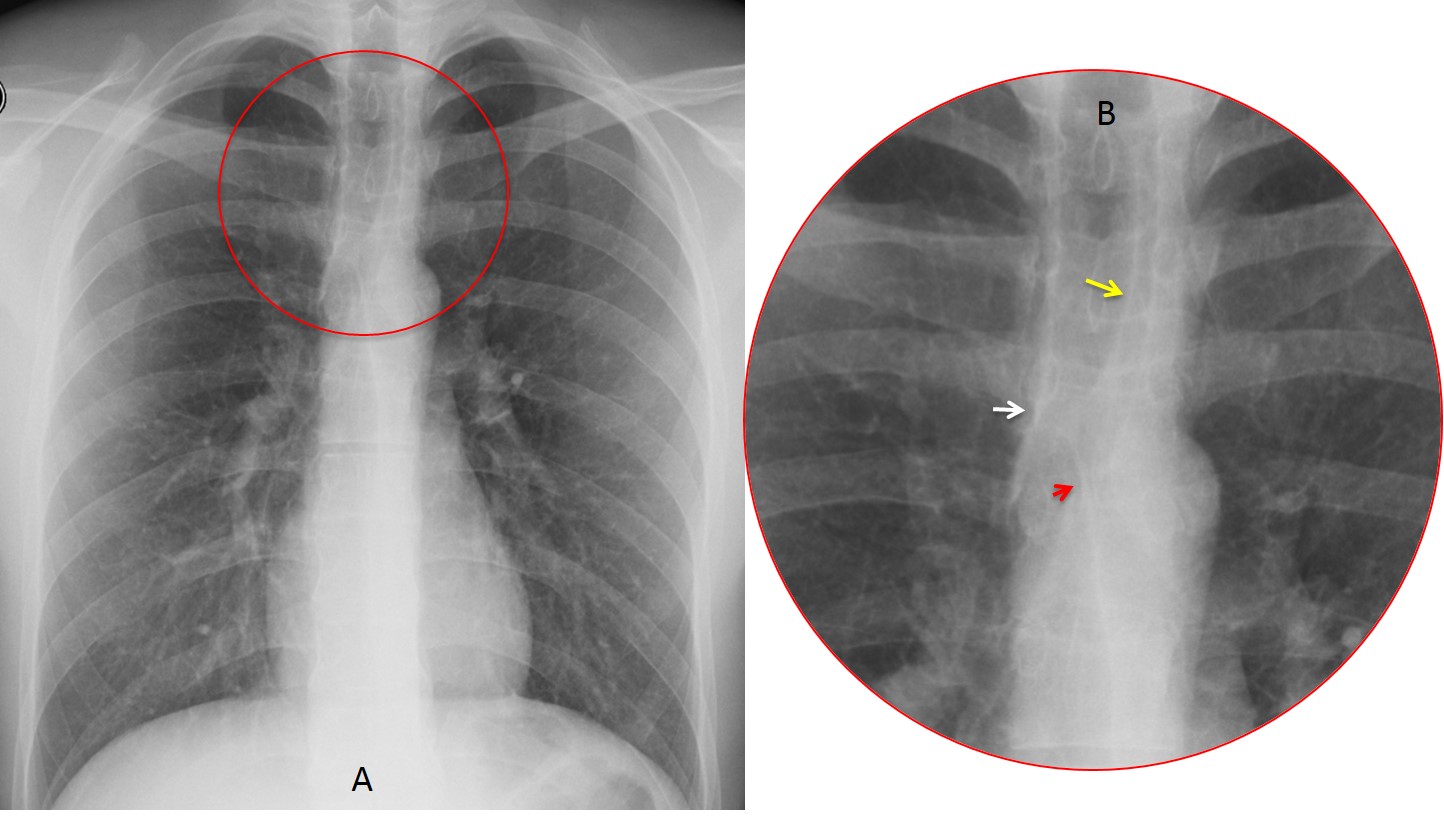
Fig. 2
Fig. 2: Cone down view of upper mediastinum showing the paratracheal line (B, white arrow), anterior junction line (B, red arrow) and posterior junction line (B, yellow arrow).
The anterior and posterior junction lines mark the union of the two upper lobes in front and behind the mediastinum. They are projected over the trachea and are seen in 30-40% of PA radiographs. They can be differentiated because the anterior junction line never runs above the plane of the clavicles. These lines are usually thin unless there is intervening mediastinal fat (Fig. 3).
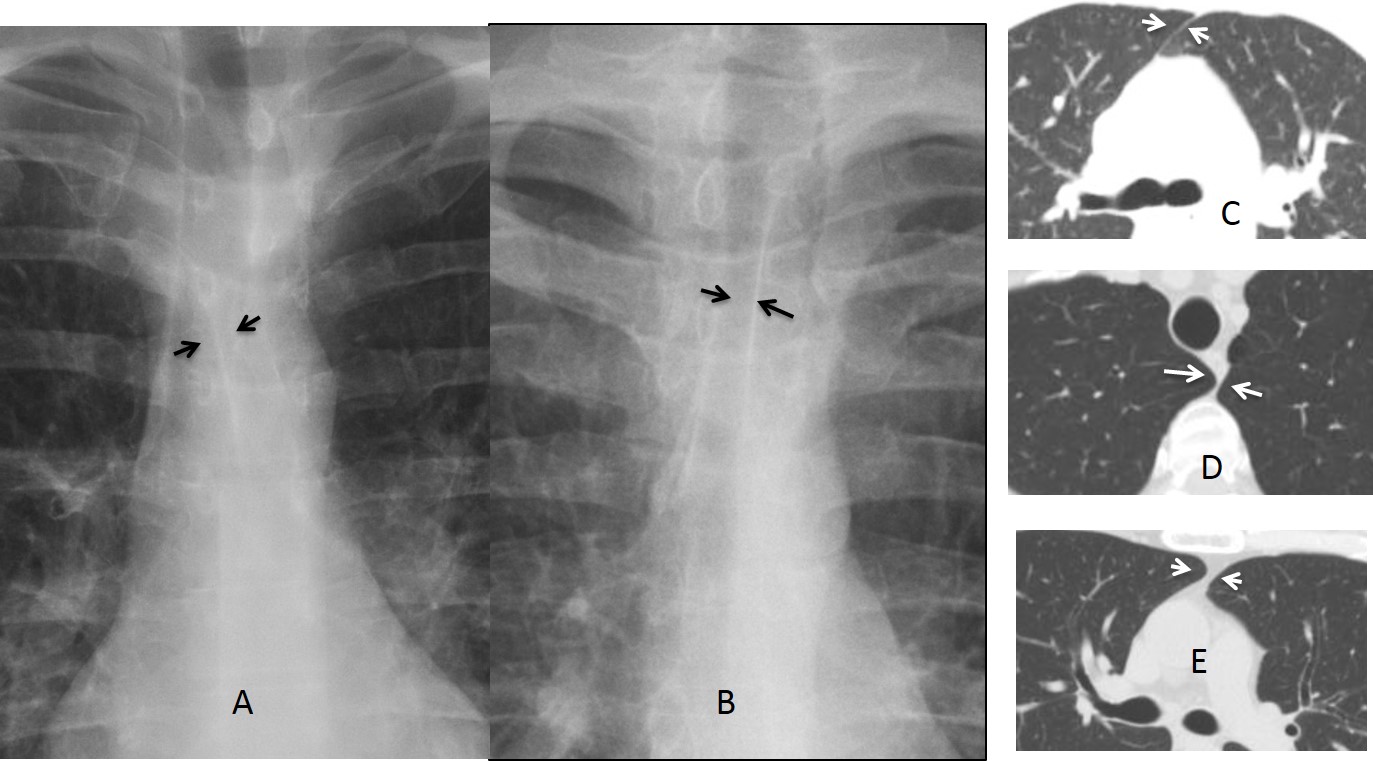
Fig. 3
Fig. 3: Anterior (A, arrows) and posterior (B, arrows) junction lines and their CT counterparts (C and D arrows). In E, intervening fat makes the line thicker (E, arrows).
Since junction lines can vary in thickness, they are not very helpful for discovering mediastinal disease. When they are displaced, they are useful to confirm increased volume of one lung or tension pneumothorax (Fig. 4)
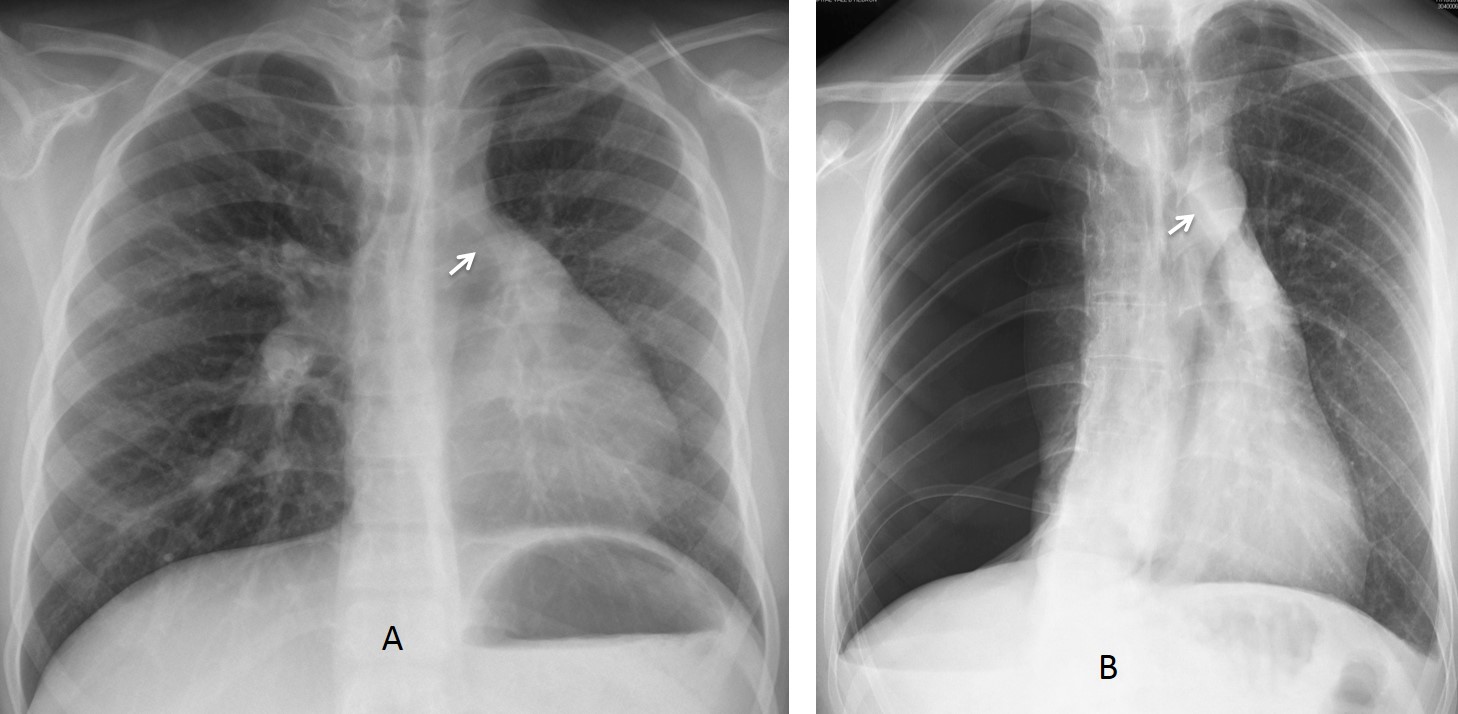
Fig. 4
Fig. 4. Emphysematous right lung displacing the anterior junction line towards the opposite lung (A, arrow). In B, there is marked displacement of the anterior line by a tension pneumothorax (B, arrow).
The right and posterior paratracheal lines are depicted by air within the trachea and the right lung (Fig. 5). The right paratracheal line is seen in more than 95% of PA chest films. Any increase in width over 3 mm should be investigated. The most common cause is enlarged lymph nodes (Figs. 6 and 7). Other causes are: mediastinal fat, tumours, or tracheal wall thickening.
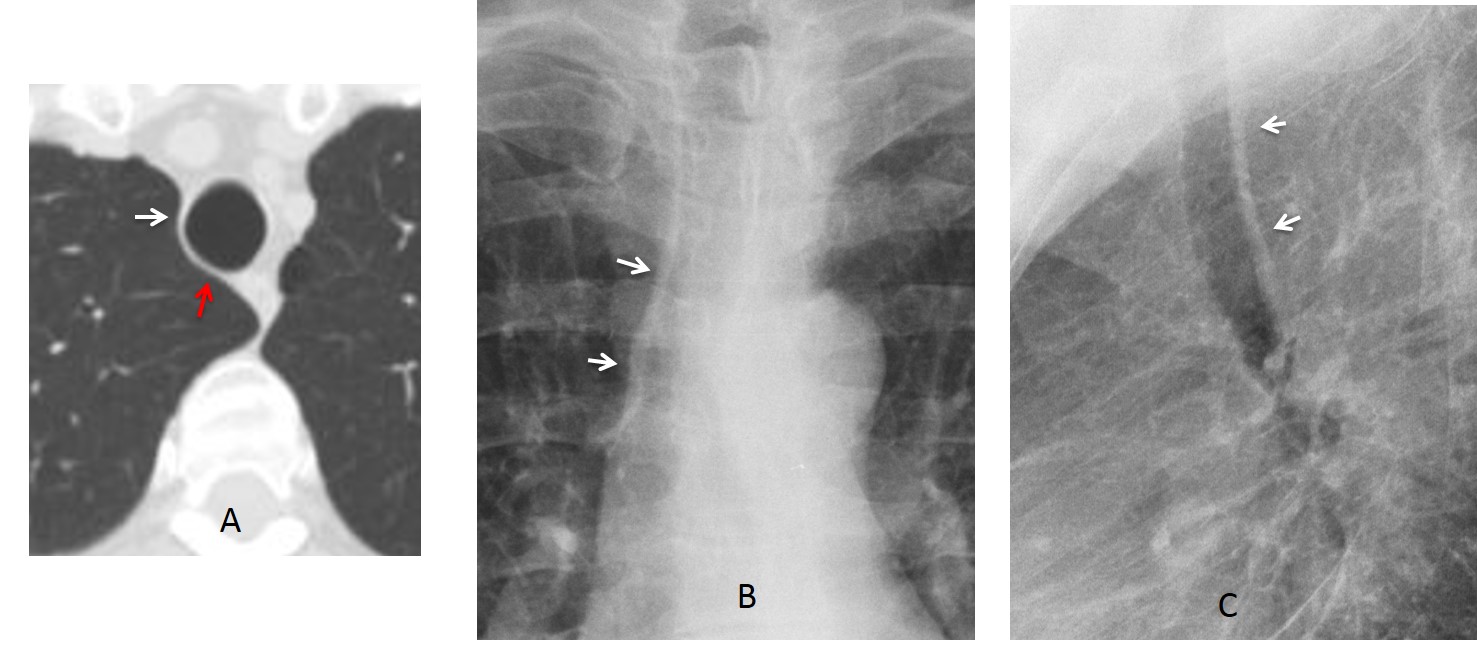
Fig. 5
Fig. 5. Axial CT showing the position of the right paratracheal line (A, white arrow) and posterior tracheal line (A, red arrow), which are well demonstrated in the PA (B, arrows) and lateral (C, arrows) views.
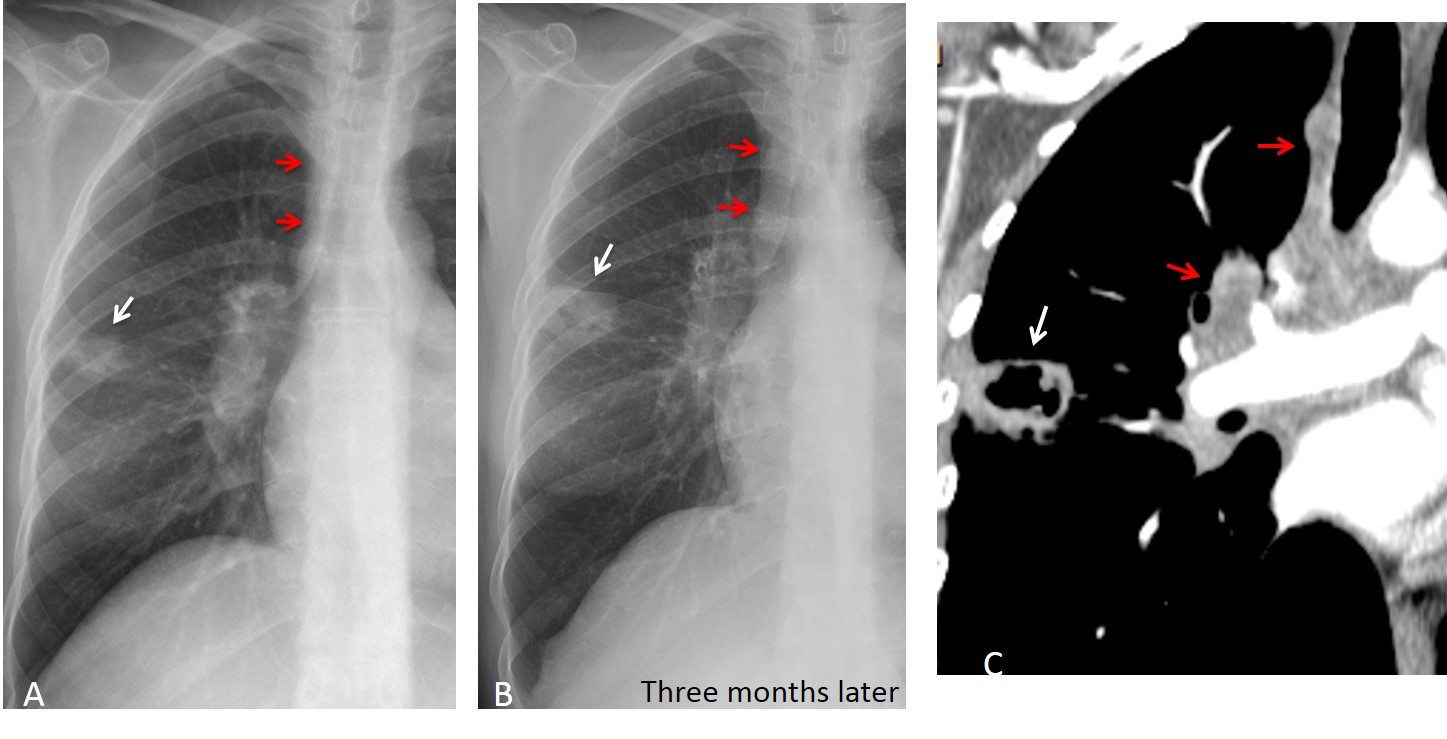
Fig. 6
Fig. 6: 47-year-old man with fever. The initial film shows a small peripheral opacity (A, white arrow) and thickening of the paratracheal line (A, red arrows), which were overlooked. Three months later, the opacity has increased in size (B, white arrow), and the paratracheal line is thicker (B, red arrows). CT shows a cavitated lesion (C, white arrow) and hilar and paratracheal nodes (C, red arrows). Diagnosis: carcinoma of the lung.
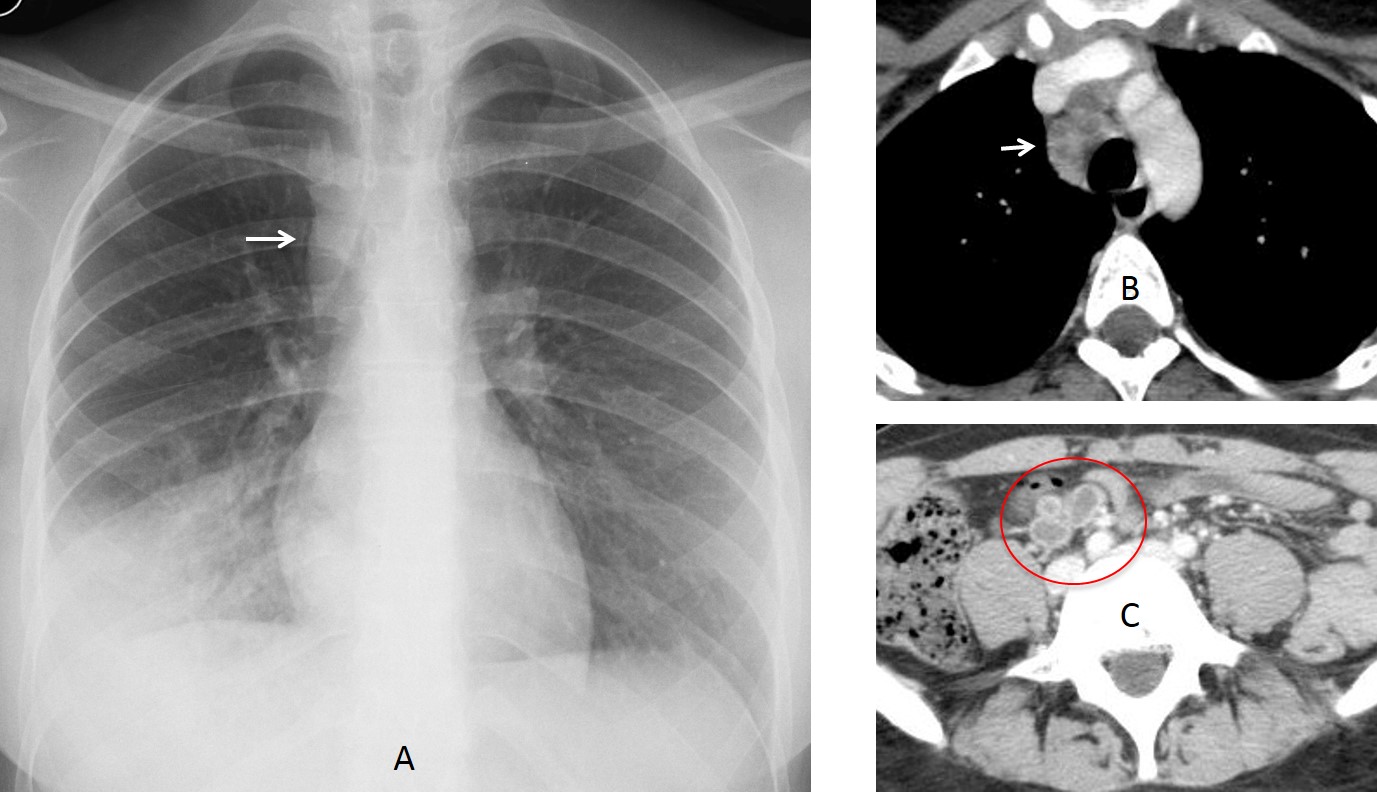
Fig. 7
Fig. 7: 38-year-old woman with fever. PA chest film depicts a RLL infiltrate . There is also widening of the paratracheal line (A, arrow). Enhanced axial CT shows a lymph node with necrotic center (B, arrow). Abdominal CT depicts similar findings (C, circle). Diagnosis: tuberculosis.
The posterior paratracheal line is visible in about 40% of lateral films. It is usually 3mm thick, but may measure up to 5mm if it comes in contact with the oesophageal wall. The most common lesions that thicken or blur this line are oesophageal disease and congenital aortic arch abnormalities (Figs. 8 and 9).
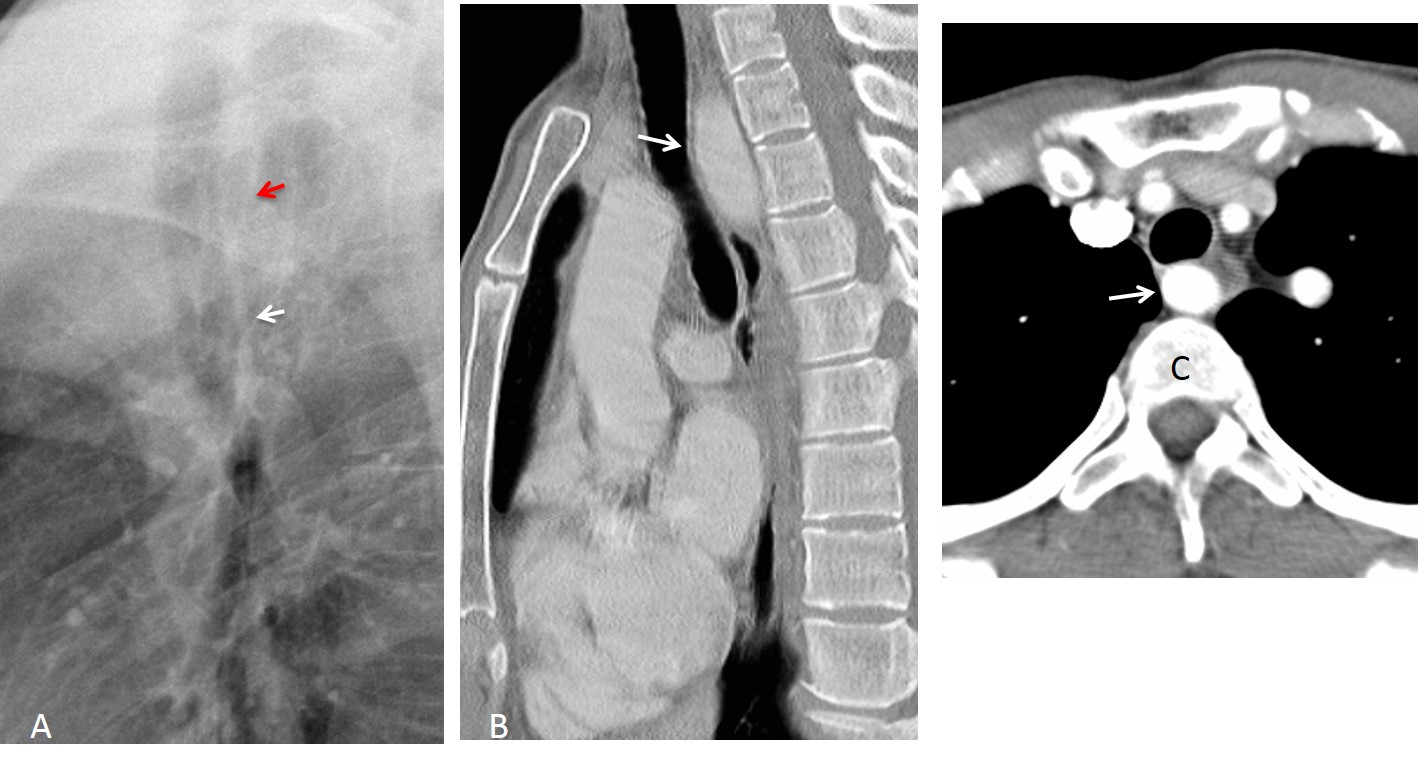
Fig. 8
Fig. 8: Normal posterior line (A, white arrow) that disappears at mid-trachea level (A, red arrow). Sagittal and axial enhanced CT show an aberrant right subclavian artery that runs behind the trachea (B and C arrows).
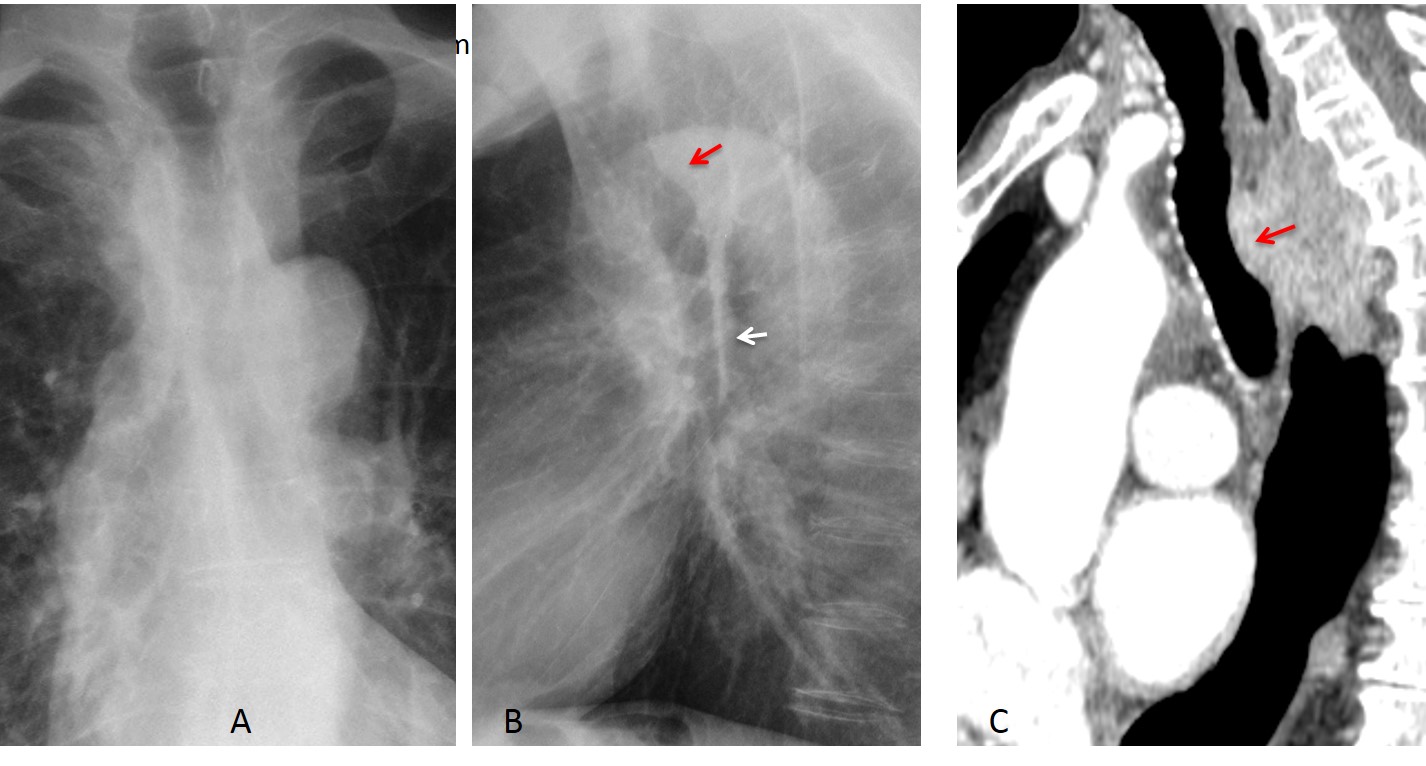
Fig. 9
Fig. 9: 65-year-old man with dysphagia and weight loss. PA chest film (A) is unremarkable except for discrete tracheal narrowing. Lateral film shows a normal inferior line (B, white arrow) that disappears in the middle third of the trachea, which is pushed forward (B, red arrow). Sagittal CT shows a large oesophageal mass behind the trachea, obliterating the posterior line (C, arrow). Diagnosis: carcinoma of oesophagus.
Mediastinal interfaces are located in the lower mediastinum and are created by lung air in contact with mediastinal structures. When an interface is abnormal, it is displaced outwards. The most useful are the azygoesophageal interface and the right and left paraspinal interfaces. The paraesophageal interface is made by contact of the right lung with the oesophagus. In most PA chest radiographs, it is seen as an oblique line projected over the spine (Fig. 10).
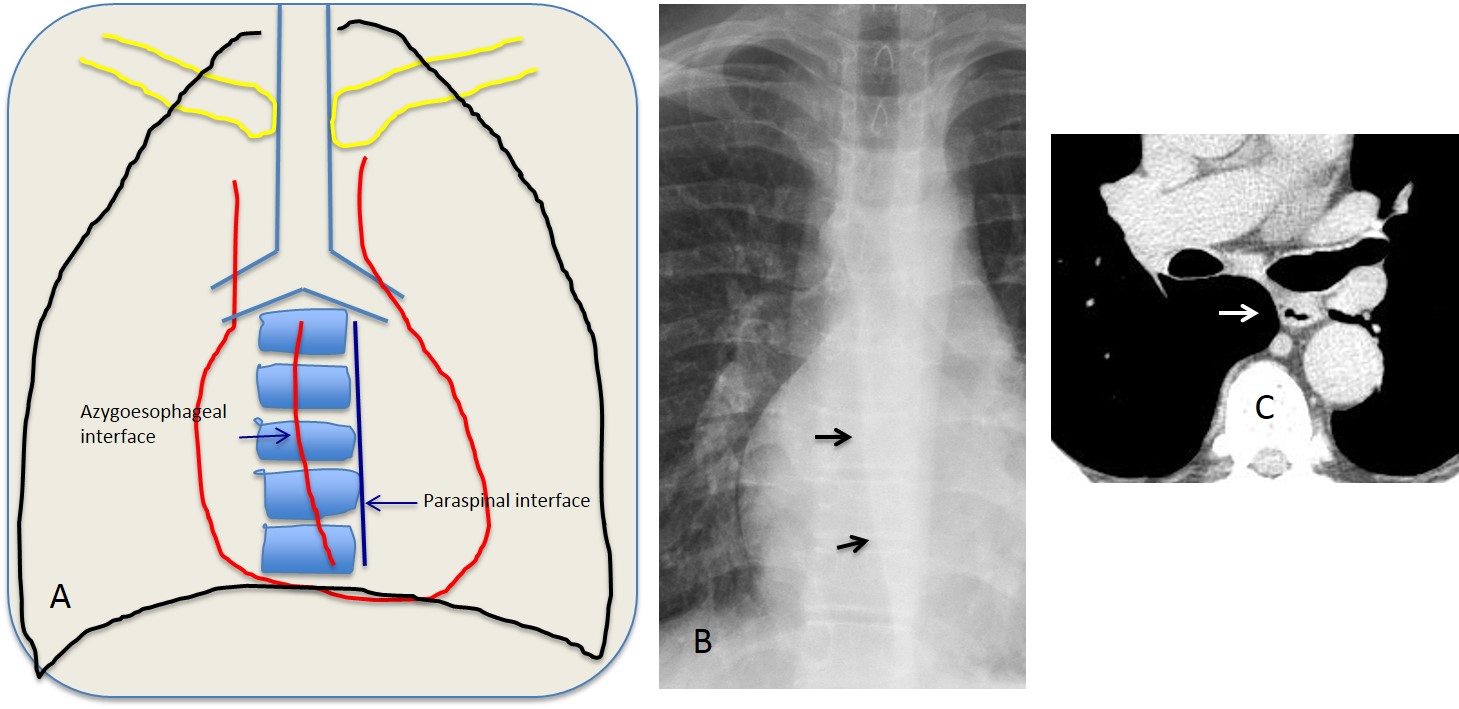
Fig. 10
Fig. 10: The drawing (A) shows the location of the azygoesophageal and left paraspinal interfaces. The azygoesophageal interface is visible in the PA chest film (B, arrows). It results from contact of the right lower lung with the oesophageal border (C, arrow).
The azygoesophageal interface may be displaced focally or in its entirety. In the first case, displacement may be due to an enlarged lymph node, oesophageal tumour, or mediastinal cyst. Displacement of the entire interface suggests oesophageal dilatation (Fig. 11).
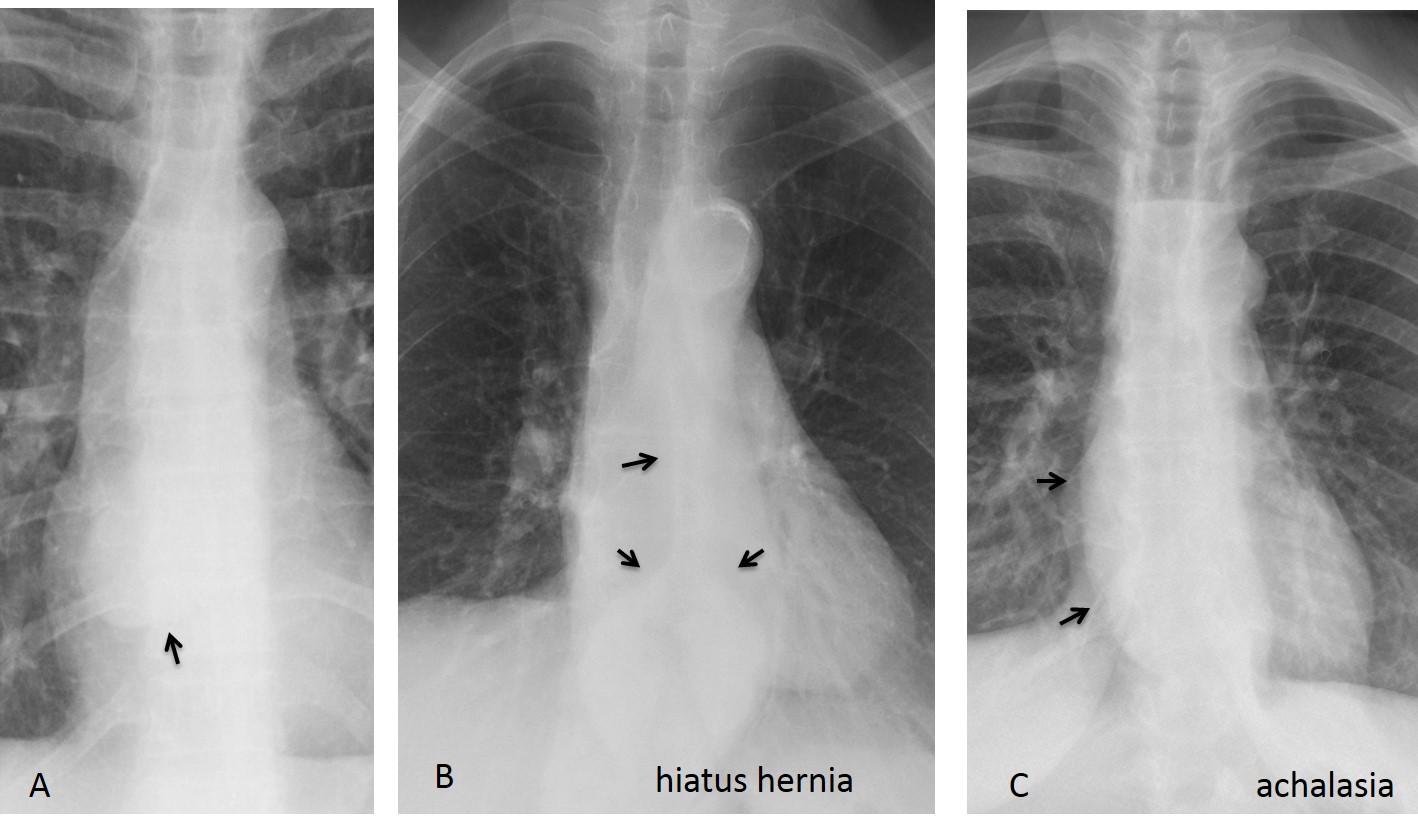
Fig. 11
Fig. 11: Focal bulging of azygoesophageal interface due to mediastinal cyst (A, arrow). Hiatus hernia at the distal oesophageal interface (B, arrows). Protrusion of the entire oesophageal interface due to achalasia (C, arrows).
The paraspinal interfaces are seen as vertical lines at both sides of the spine (Fig. 12). They represent the interface of the lower lungs with the pleural reflections around the spine. Most common causes of overall displacement are osteophytes on the right side and elongated aorta on the left.

Fig. 12
Fig. 12: Paraspinal interfaces displaced outwards, the right interface by osteophytes (A and B, white arrows) and the left by an elongated aorta (A and B, red arrows).
Neurogenic tumours are a common cause of unilateral focal displacement. Bilateral focal bulging is usually due to enlarged lymph nodes or spinal processes that generated soft tissue masses (Fig. 13).
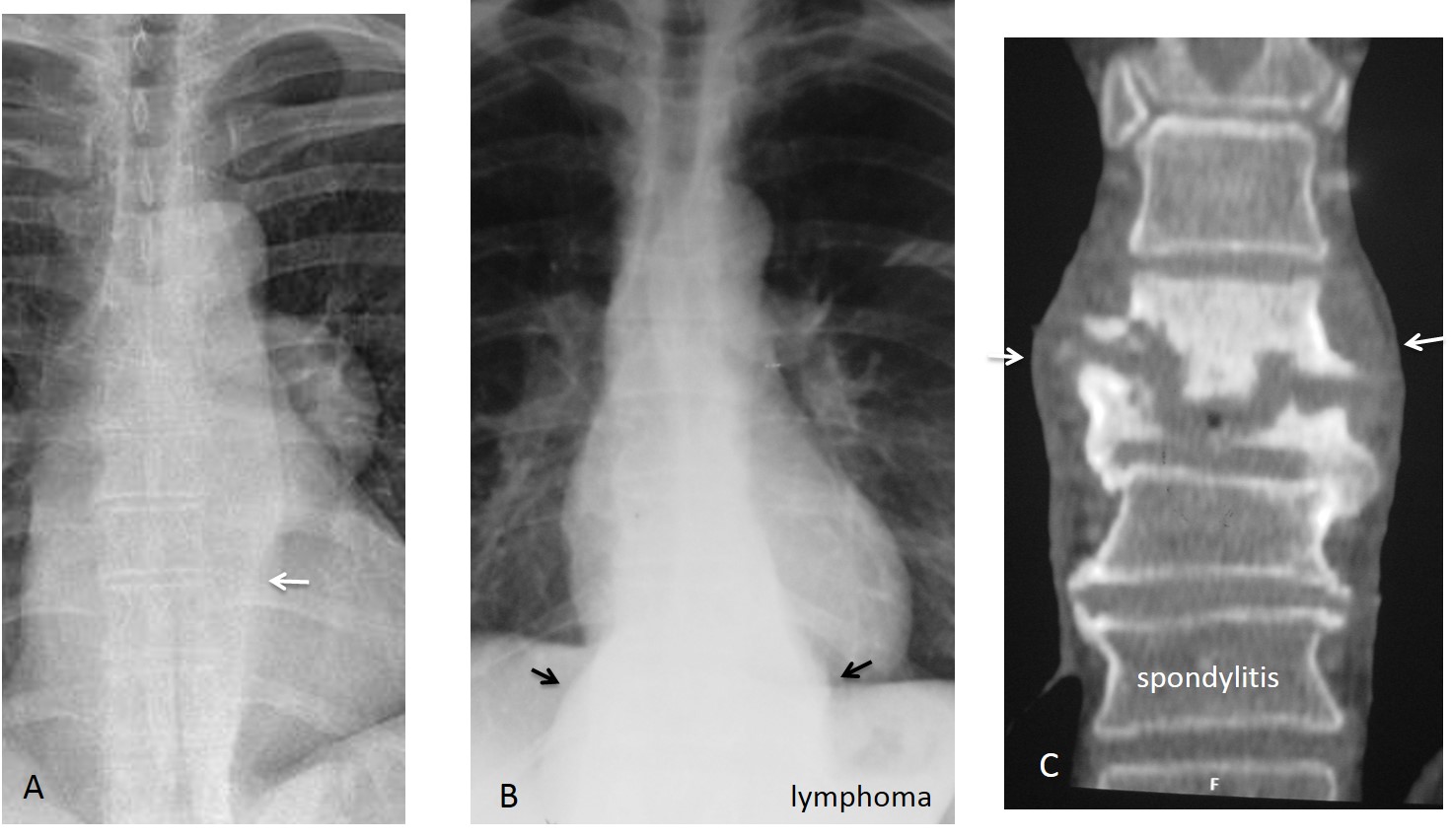
Fig. 13
Fig. 13: Neurogenic tumour displacing the left paraspinal interface (A, arrow). Bilateral displacement of both paraspinal interfaces in lymphoma (B, arrows) and spondylitis (C, arrows).

Follow Dr.Pepe’s Advice:
1. A right paratracheal line more than 3mm wide should be investigated
2. A displaced azygoesophageal interface suggests oesophageal disease
3. The most common causes of displacement of paraspinal interfaces are osteophytes on the right and elongated aorta on the left
4. Focal bulges in the paraspinal interfaces are due to neurogenic tumours or spinal disease.


Hiatus hernia – bronchiectasis
Dear Gus, I expect better from you!
Hay dos cosas que me llaman la atención. En la lateral no veo bien el espacio claro anterior y en la Pa las líneas mediastinicas (además de por la hernia) no me parecen normales.
El accidente es reciente?
Tu apreciación del espacio claro anterior es correcta: no se ve bien.
El accidente ocurrió hace siete años.
…ernia traumatica diaframmatica anteriore dx, a contenuto epato-omentale….chiave di lettura:non si vede in tutto il suo decorso , il profilo diaframmatico anteriore dx in LL e la pseudolobulazione della cupola diaframmatica dx in AP…Con stima …..
Sorry professor. let me try again
enlargment of heart size prominent pulmonary vessels
On the lateral view along of the frontal borders of the heart on the sub sternal space its a band like radiopacity.
( pericardium thickening ?)
it a long time from the accident and i can’t see fat pad sign or calcifications. hot or cold? 🙂
Cold, sorry.
I couldn’t tell anything special about these images, maybe two theories.
1. Could it be some kind of encapsulation of lung contusion, or something similar (looks to me like a small consolidation in the left lower field)
2. Interstitial pneumonia 🙂
on lateral radiograph, there is loss of anterior heights of probably D7 and D10 vertebral bodies with ill definition of the superior endplates of the respective vertebrae. Mild reduction in disc height is seen at D9-10 level. Obliteration of the retrosternal lucency noted in the lower third region.
On frontal radiograph a fusioform thoracoabdominal opacity is seen in the posterior mediastinum. Also an ill-defined haziness in seen in the periphery of the left lower zone, obscuring the cardiac apex.
Unifying diagnosis in the setting of fever and malaise is tubercular osteomyelitis with paraspinal abscess. The lingular consolidation could point out to atypical mycobacterial infection.
Clinoid deformation of IX thoracic vertabrae.
Compresed. f raacture of vertebral body IX thoracic verthebrae.
Post traumatic left diaphragm small intestinal herniation (post traumatic trough rib fracture ? / congenital ?).
Left lower lobe early stage consolidation ( explaining the symptoms )maybe because of chronic passive atelectasis.
Left anterior thickening of the pleura, most probably post-traumatic pahipleuritis.
Was the impact left antero-lateral ?
Heart great vessels and rigt lung look normal
Left heart and diafragma contour are not clear.
I suspected from mucus impaction on lateral film
My DDx: left lower lobe pneumonia/subsegmenter atelectasia