Dr. Pepe’s Diploma Casebook: Case 74 – SOLVED!
Dear Friends,
Today I am showing PA radiographs of a 52-year-old man with cough and mild fever. Take a look at the images below, leave me your thoughts in the comments section and come back on Friday for the answer.
Diagnosis:
1. Inferior accesory fissure
2. RLL collapse
3. Pneumonia of medial RLL segment
4. None of the above
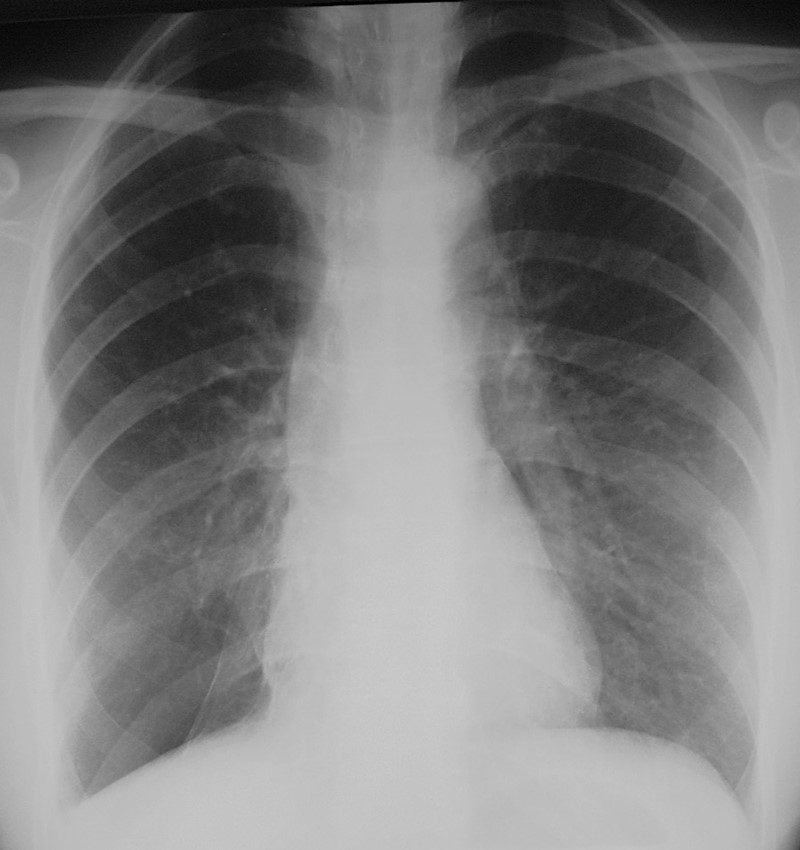
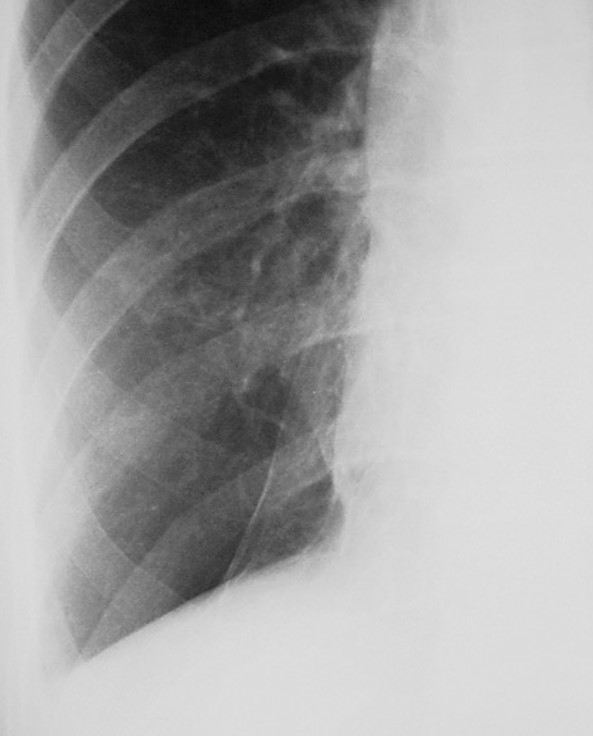
Findings: An oblique line at the right base (A, white arrow) simulates an inferior accessory fissure. However, the right hilum is markedly low (A, red arrow), indicating RLL volume loss. Coronal CT shows marked RLL collapse with bronchiectasis, outlined by the displaced major fissure (B, arrow).
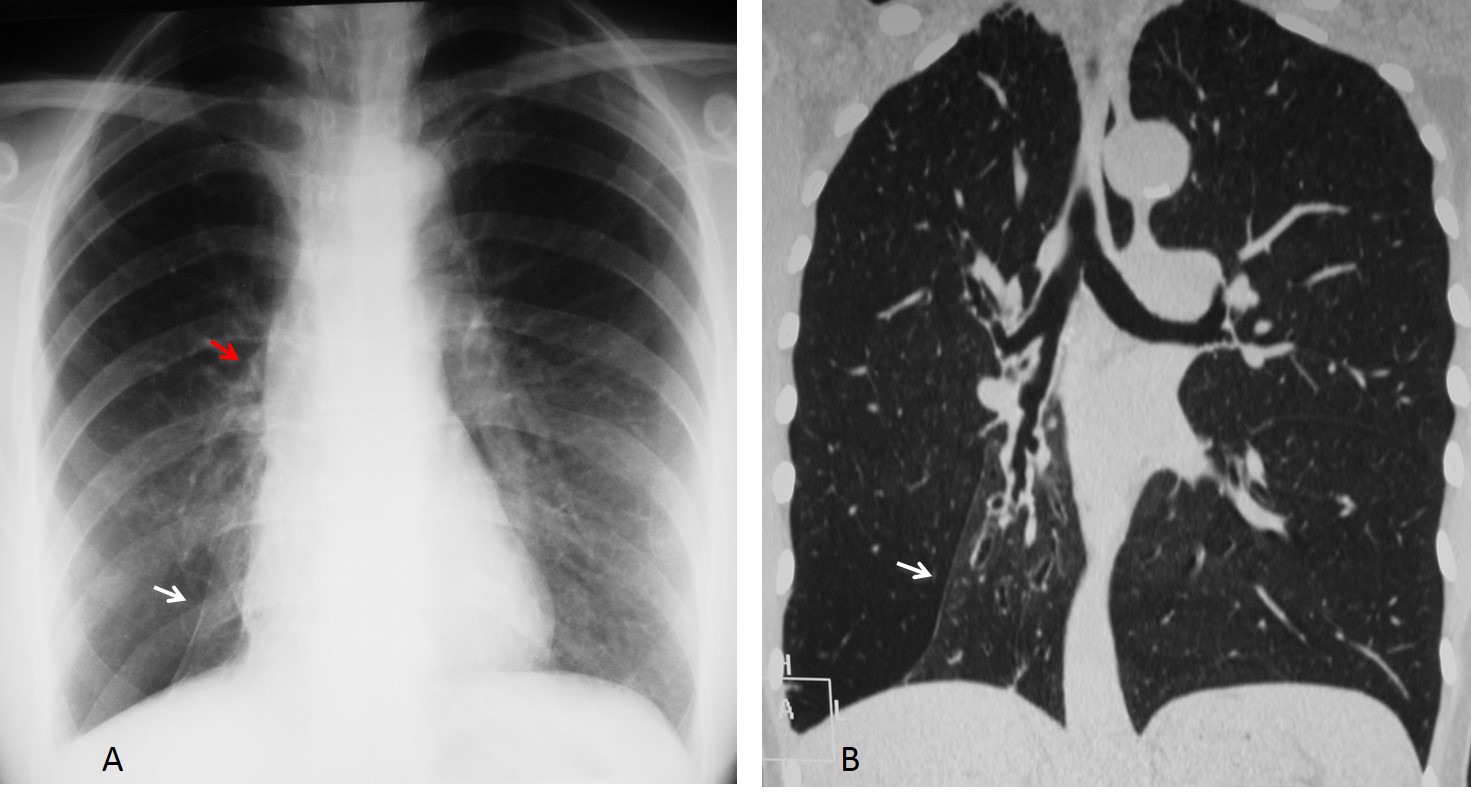
Final diagnosis: RLL collapse secondary to bronchiectasis
This case is presented to discuss lung fissures; that is, fine lines seen within the lungs that represent the pleural layers enfolding the lobes. There are two fissures in the right lung (major and minor fissure) and one in the left lung (major fissure). The minor fissure separates the right upper lobe from the middle lobe and is visible in the PA and lateral views as a straight line (Fig. 1 A & B). The major fissures of the right and left lungs are not visible in PA films because their course is not tangential to the x-ray beam (Fig. 1 A, curved dotted lines). However, they are both visible as oblique lines in the lateral view (Fig. 1 B).
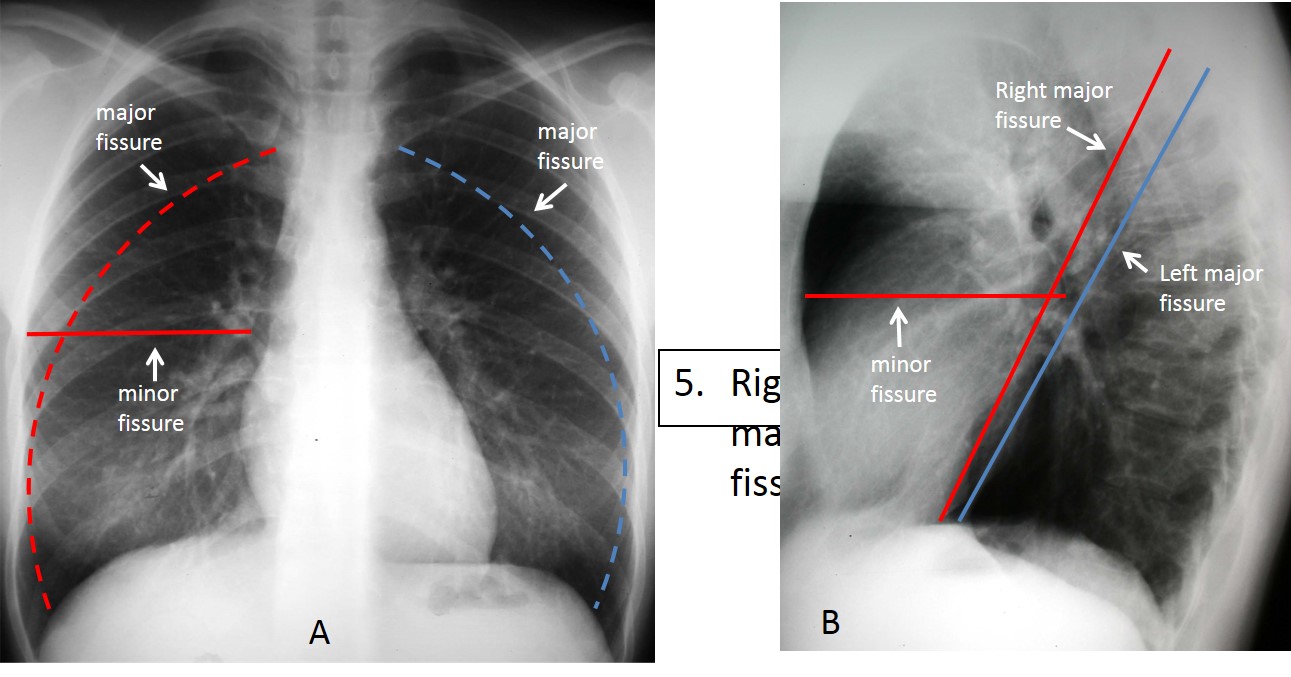
Fig. 1
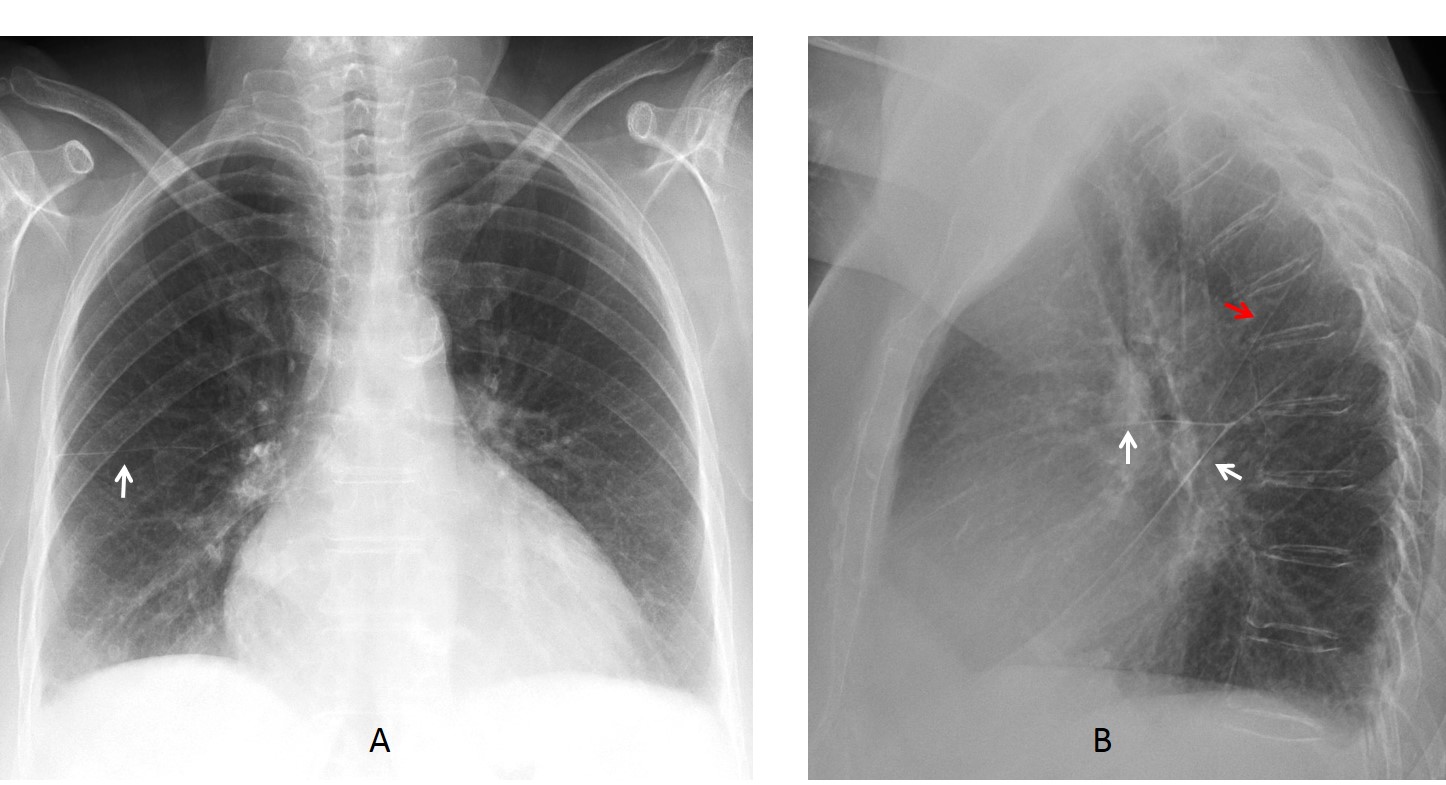
Fig. 2
Fig. 2. PA radiograph showing the minor fissure (A, arrow). The lateral view shows the minor and major fissure of the right lung (B, white arrows), and above, the major fissure of the left lung (B, red arrow).
The fissures are important landmarks to note when investigating disease on plain films. From the diagnostic viewpoint, there are three types of fissure abnormalities:
1. Displacement
2. Masses within the fissure
3. Overall thickening
Fissure displacement indicates loss of volume of the affected lobe (Fig. 3). It can have several causes, but the most important in adults is a central bronchogenic tumour, which should be always ruled out (Fig. 4). Other causes of displaced fissures are endobronchial lesions, fibrotic TB, bronchiectasis, and rounded atelectasis (Fig. 5).
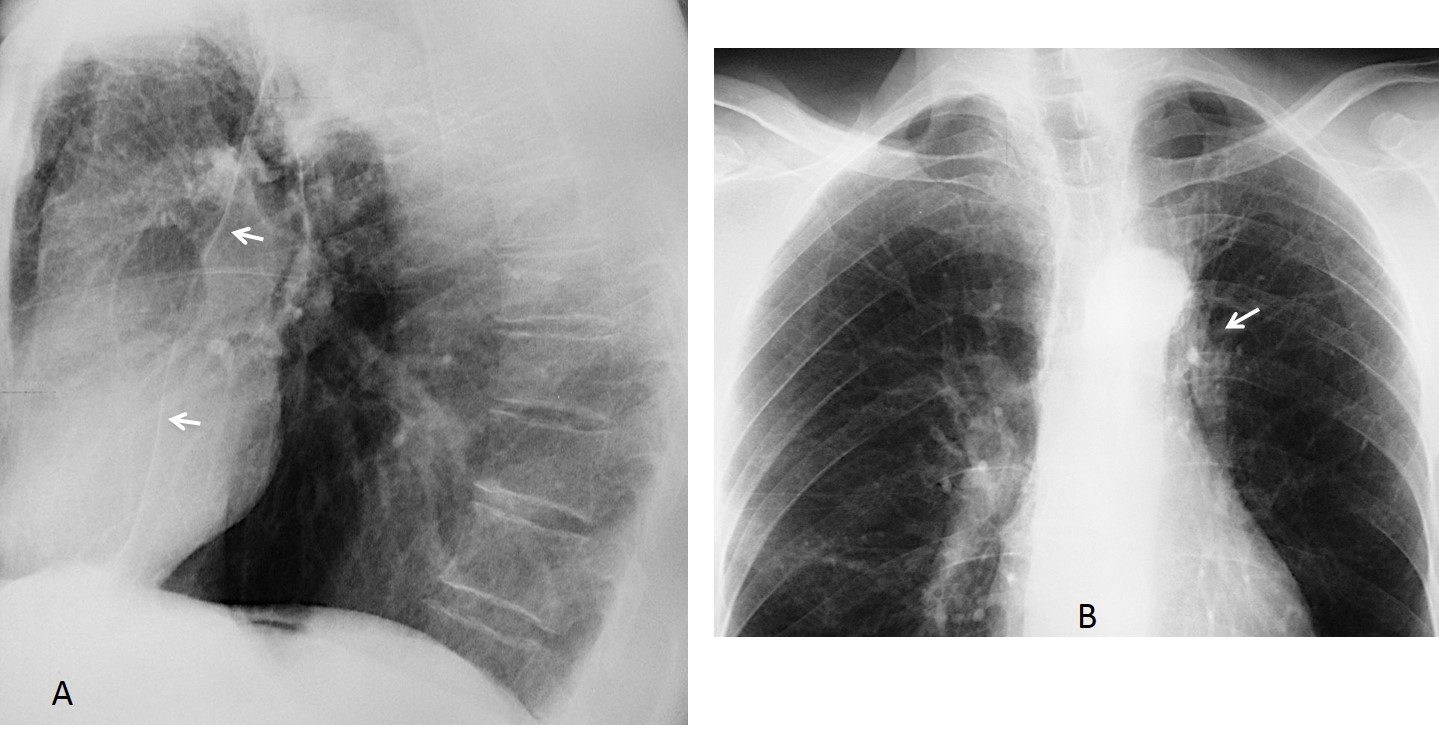
Fig. 3
Fig. 3. 56 y.o. man with previous TB. Lateral radiograph shows forward displacement of the left major fissure (A, arrows), indicating partial LUL collapse. PA view depicts markedly elevated left hilum (B, arrow), secondary to fibrotic TB.
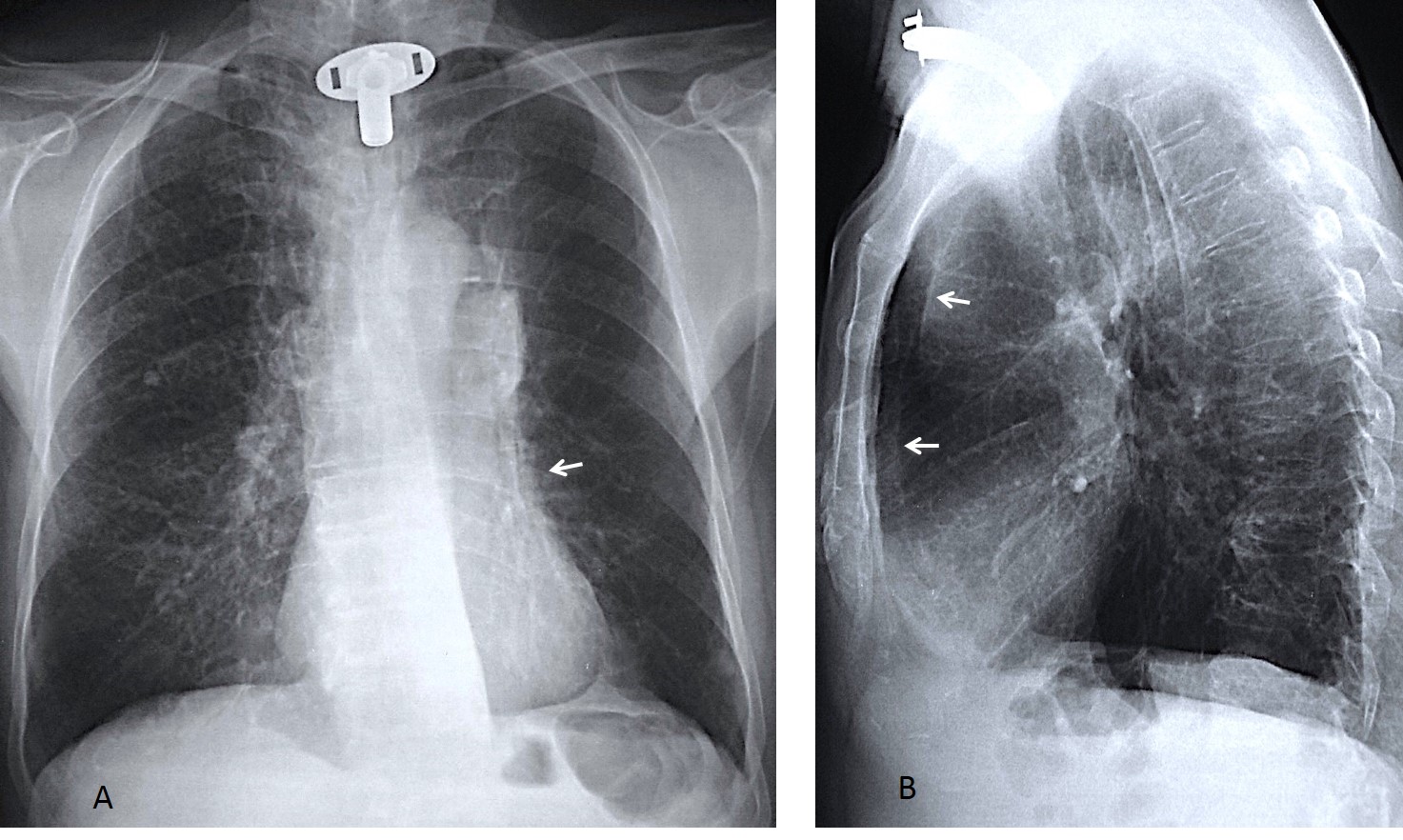
Fig. 4
Fig. 4. Routine follow-up film in an 82 y.o. man who had undergone surgery for carcinoma of larynx 10 years previously. PA radiograph shows abnormal right hilum and blurring of the left cardiac contour (A, arrow). Lateral view depicts marked forward displacement of the left major fissure (B, arrows) indicating severe LUL collapse.
Unenhanced axial CT confirms the marked LUL collapse (C, white arrow) secondary to an endobronchial obstruction (C, red arrow). CT taken one year earlier shows an endobronchial lesion (D, red arrow) and discrete forward displacement of the major fissure (D & E, white arrows). These changes were overlooked. Surgical diagnosis: bronchogenic carcinoma
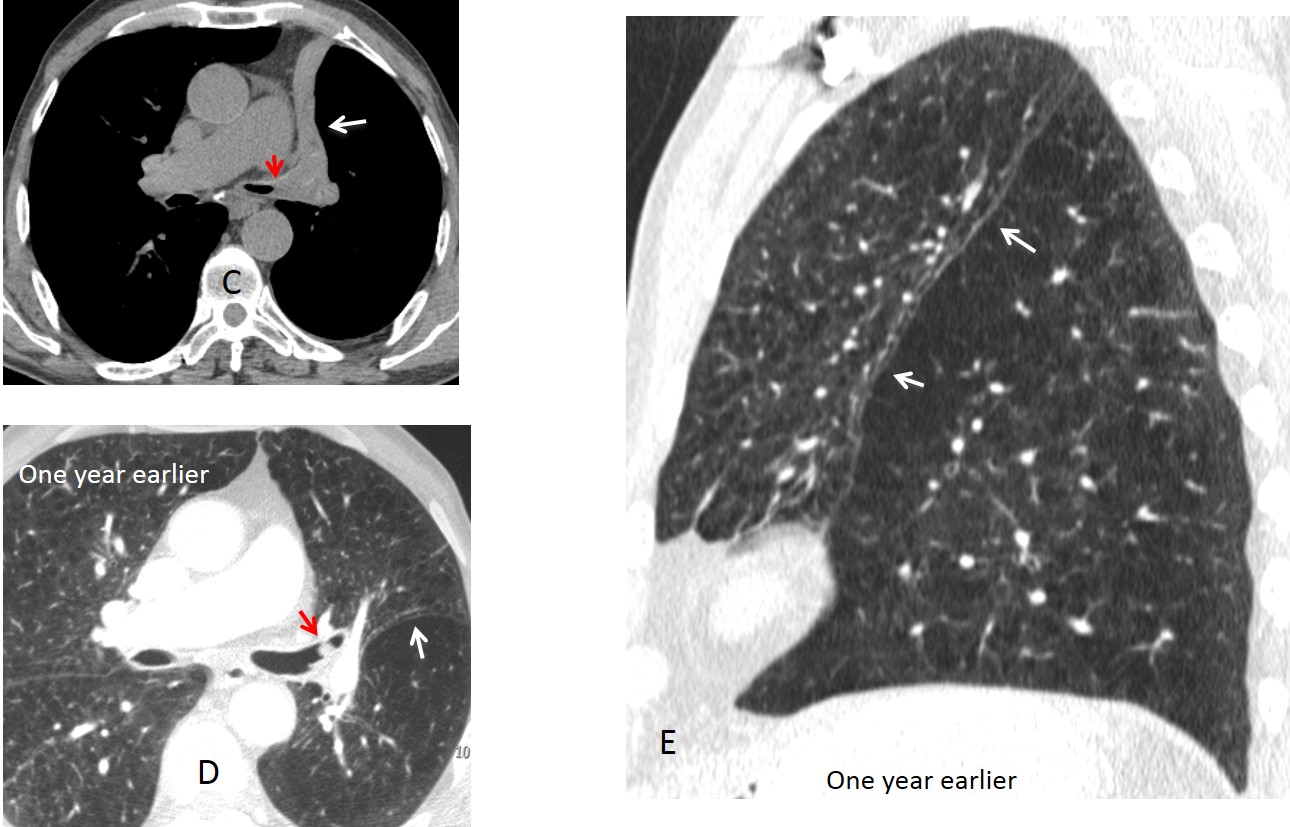
Fig. 4
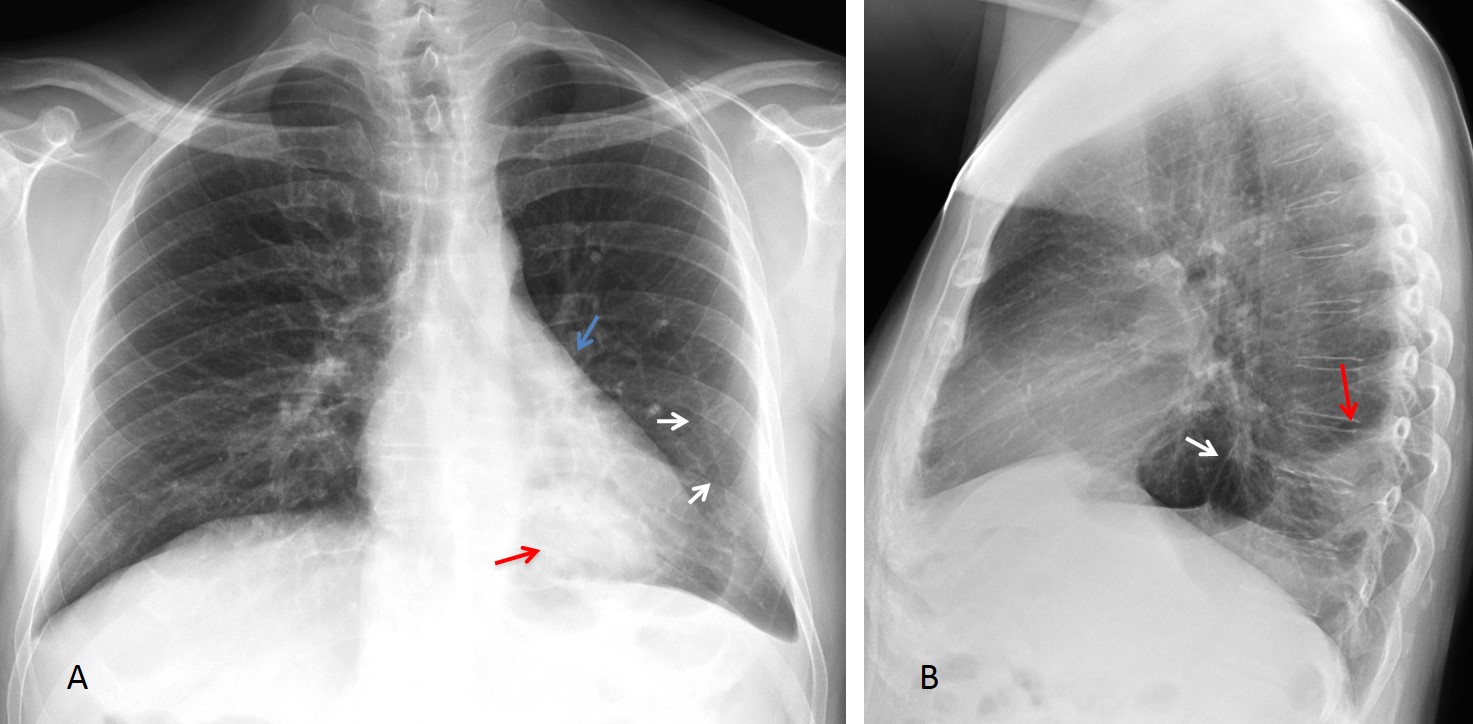
Fig. 5
Fig. 5. 58-year-old. man with moderate dyspnea. The left major fissure is visible in the PA radiograph (A, white arrows), indicating LLL volume loss, confirmed in the lateral view (B, white arrow). This is corroborated by downward displacement of the hilum (A, blue arrow). There is a rounded peripheral opacity in the LLL (A & B, red arrows).
Coronal and axial views show displacement of the major fissure (C & D, red arrows), pleural thickening, and curving of the RLL vessels (C, yellow arrow). Diagnosis: rounded atelectasis with LLL volume loss .
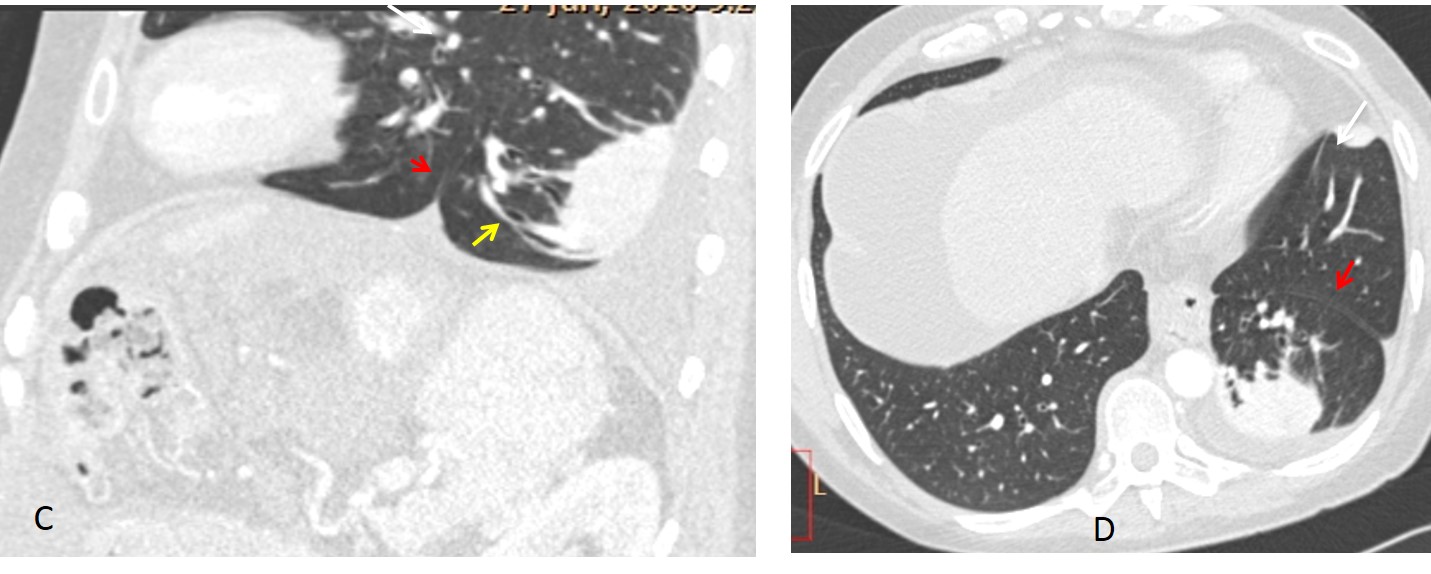
Fig. 5
Masses within a fissure have a typical ovoid shape with tapering ends. When located in the minor fissure they are easily identified as such in both chest projections (Fig. 6). Masses in the major fissure may give a deceptive appearance in the PA view, but they are easily identified in the lateral view (Fig. 7).
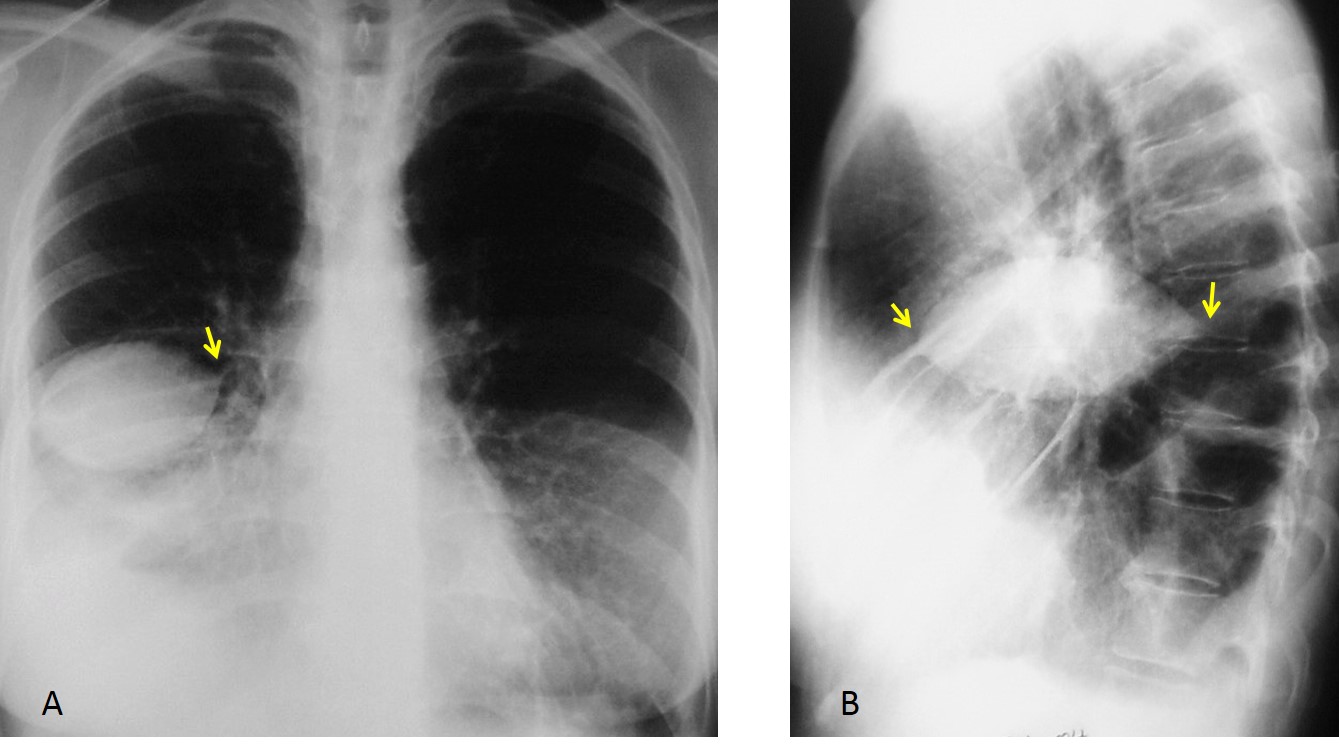
Fig. 6
Fig. 6. 48-year-old woman with right pleural effusion and loculated fluid in the minor fissure. Note the typical fusiform appearance and tapering edges (A & B, arrows).
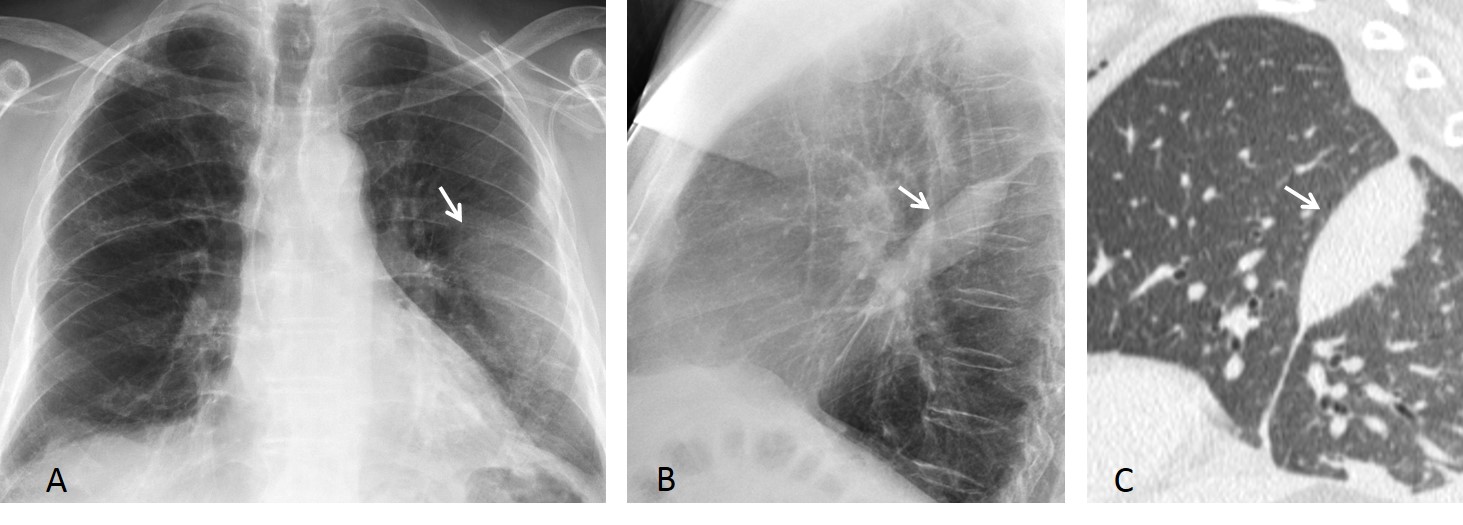
Fig. 7
Fig. 7. 59-year-old man with loculated fluid in the left major fissure. The PA film shows a nondescript opacity in the left lung (A, arrow). Lateral view depicts the typical appearance of a lesion within the fissure (B, arrow). Sagittal CT confirms the findings (C, arrow).
The most common etiology of a fissure mass is heart failure, in which pleural fluid may collect within the fissures (Fig. 8). In rare cases, air may be seen, giving an air-fluid level that should not be confused with a cavitated lung nodule (Fig. 9).
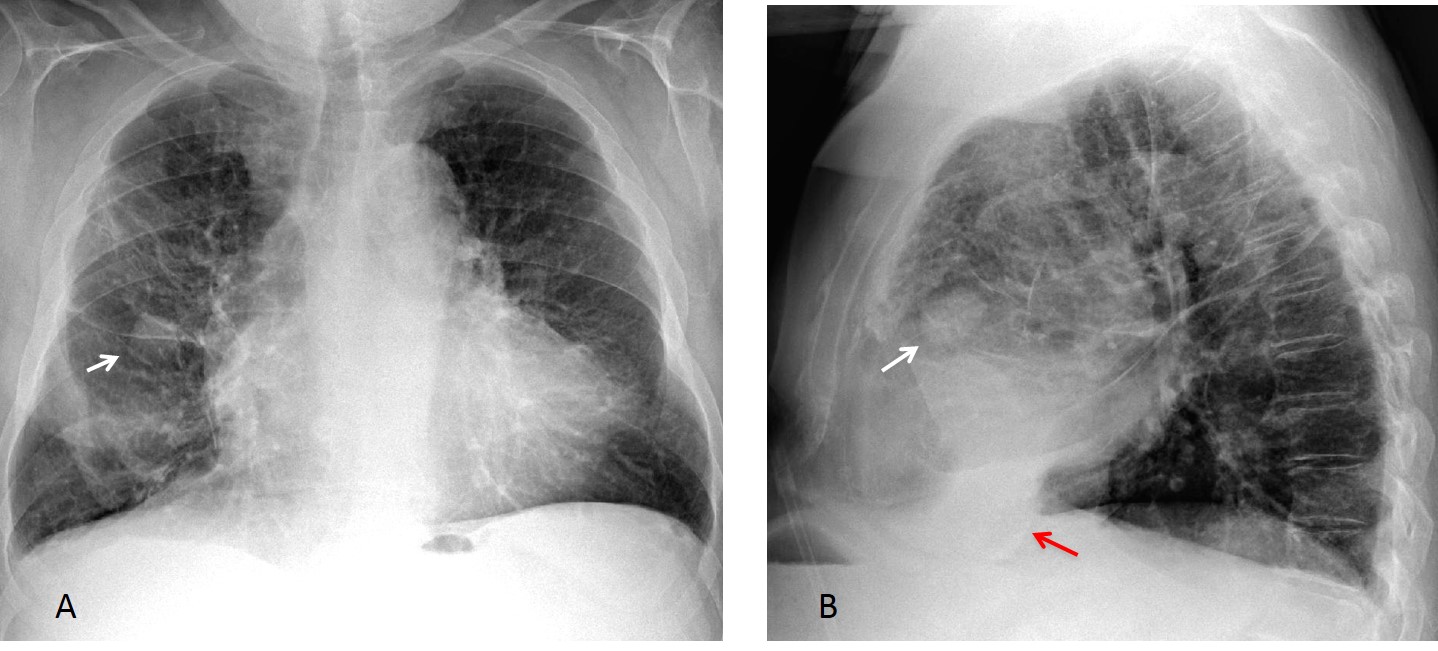
Fig. 8
Fig. 8. 65-year-old man with heart failure. PA and lateral views show a nodule in the area of the minor fissure (A & B white arrows). There is also fluid in the lower right major fissure (B, red arrow).
Axial and sagittal CT images show that the nodule represents fluid within the minor fissure (C & D, white arrows). There is also fluid in the major fissure (C & D, red arrows). The fluid moves freely within the fissure: it is located downwards in the upright chest image (B, red arrow) and posteriorly in the recumbent CT (C & D, red arrows)
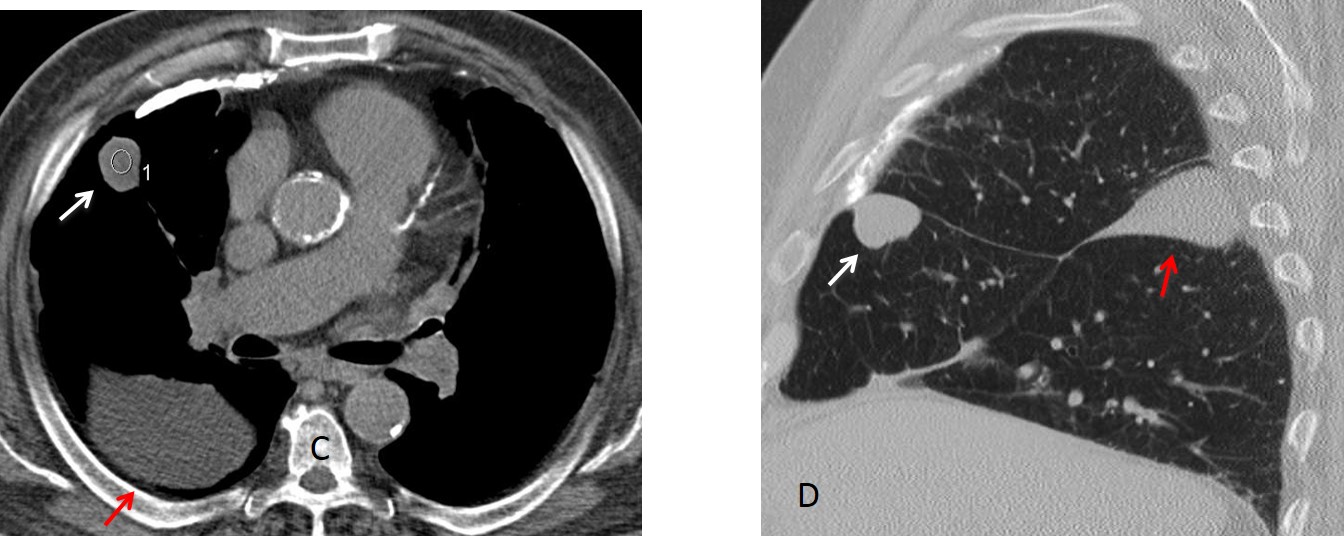
Fig. 8
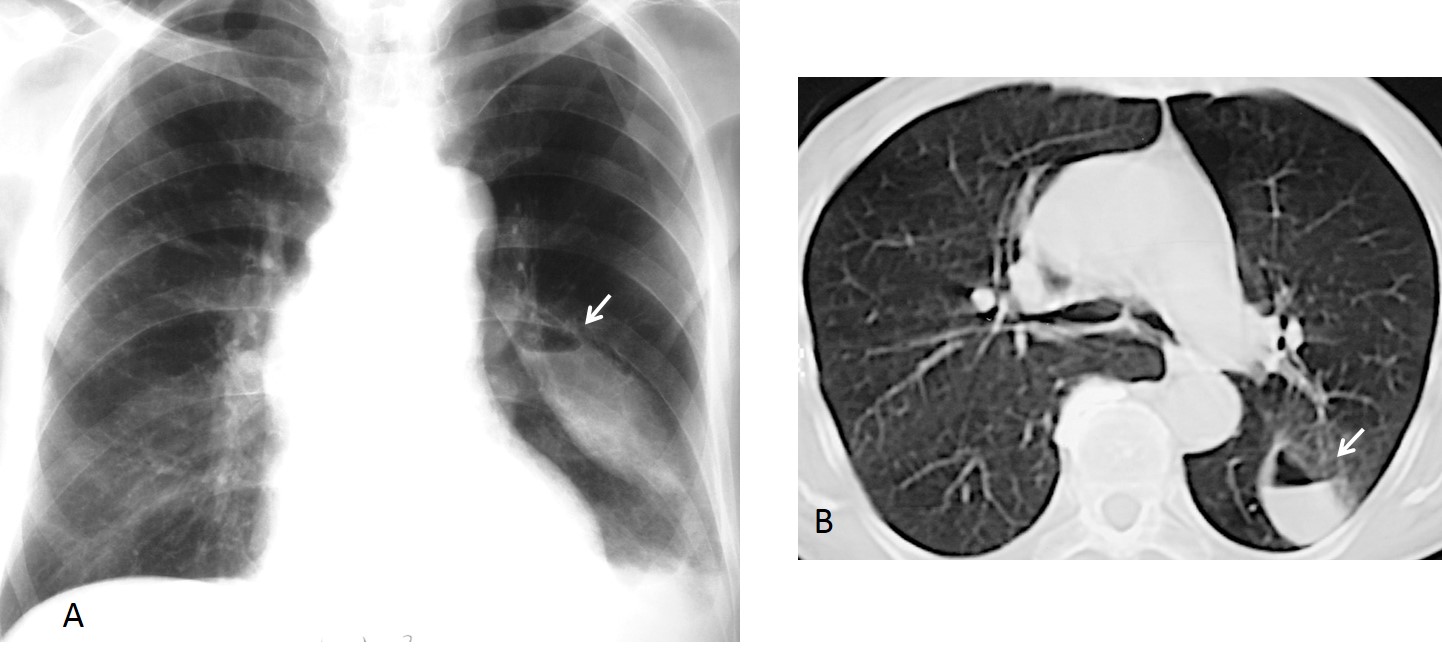
Fig. 9
Fig. 9. Air-fluid level in the left major fissure (A, arrow), confirmed with CT (B, arrow). Should not be confused with a cavitated lung lesion.
Pleural tumours may locate in a fissure. The appearance is similar to loculated fluid minus the signs of heart failure. The most common is fibrous pleural tumour. It is usually asymptomatic and discovered accidentally. It should be removed because of its malignant potential (Figs. 10 & 11)
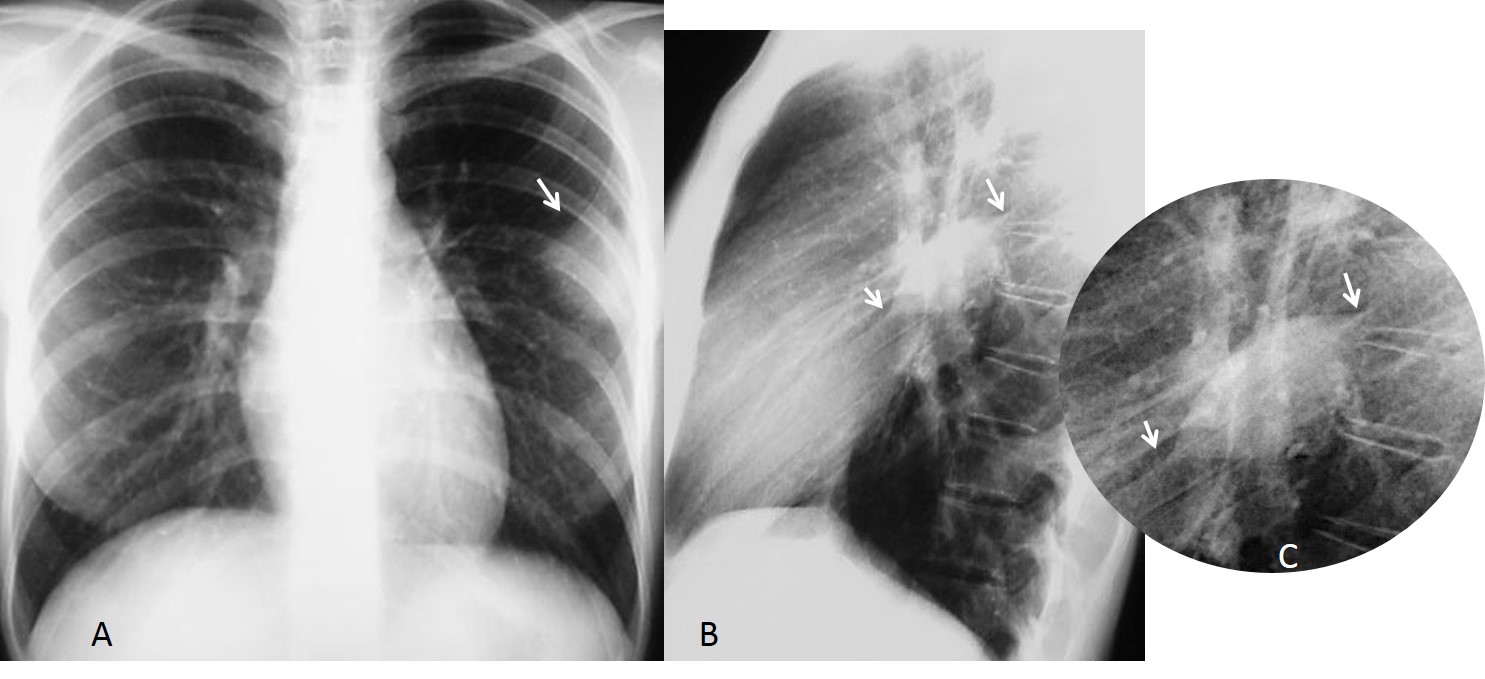
Fig. 10
Fig. 10. 35-year-old woman with fibrous tumour of left major fissure. PA radiograph shows an ill-defined peripheral opacity (A, arrow). Lateral view demonstrates the typical ovoid shape and tapering edges, better seen in the cone-down view (B & C, arrows).
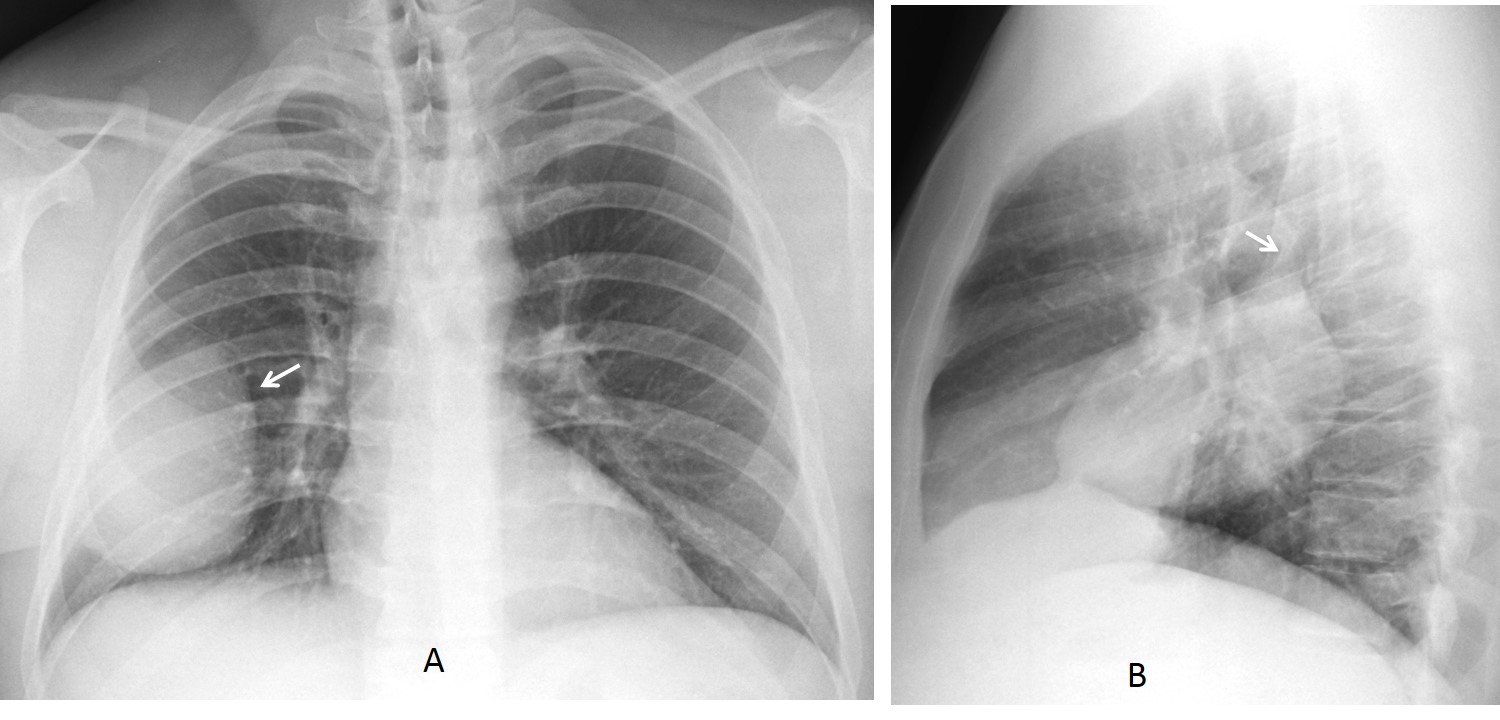
Fig. 11
Fig. 11. 44-year-old asymptomatic man. PA radiograph shows a rounded opacity in the right lower lung (A, arrow). In the lateral view it has a lenticular shape and a tapering edge above (B, arrow). The appearance is highly suggestive of a fissure mass.
Coronal and sagittal CT show a soft tissue mass (C & D, white arrows), with a lower tapering edge that fuses with the right major fissure (D, red arrow). Surgical diagnosis: fibrous tumour of pleura
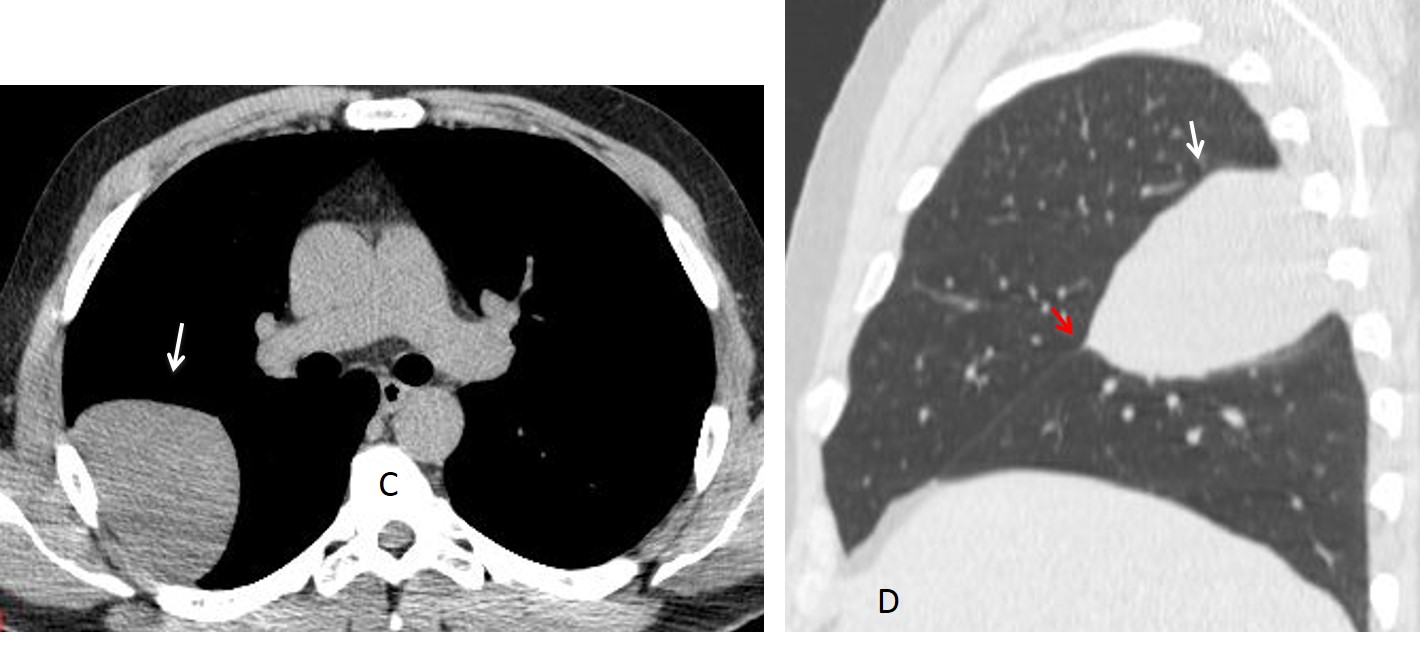
Fig. 11
Overall thickening of fissures usually occurs in pulmonary oedema of any cause (Fig. 12). It may also accompany diffuse chronic lung disease, although it is an ancillary finding in these cases, as the lung changes are far more obvious (Fig. 13).
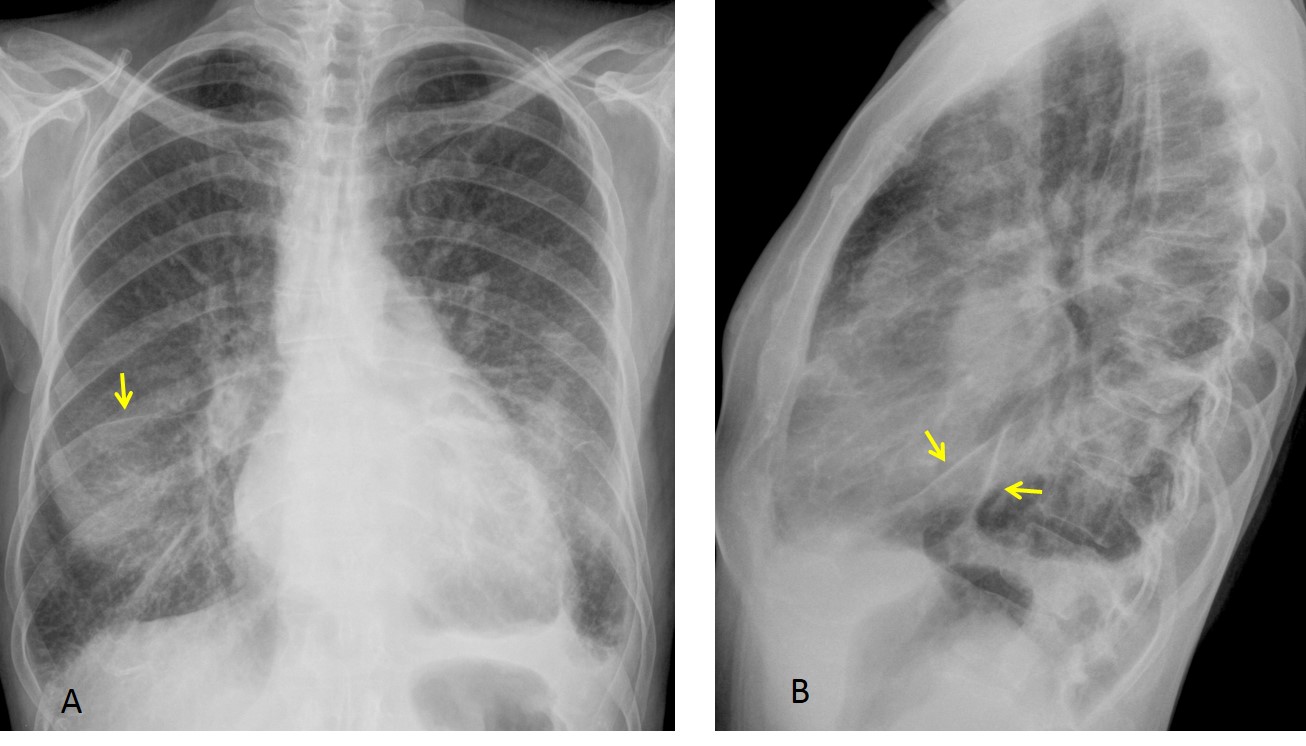
Fig. 12
Fig. 12. 42-year-old man with pulmonary oedema secondary to mitral disease. Aside from the pulmonary changes, there is overall thickening of fissures secondary to pleural fluid (A & B, arrows).
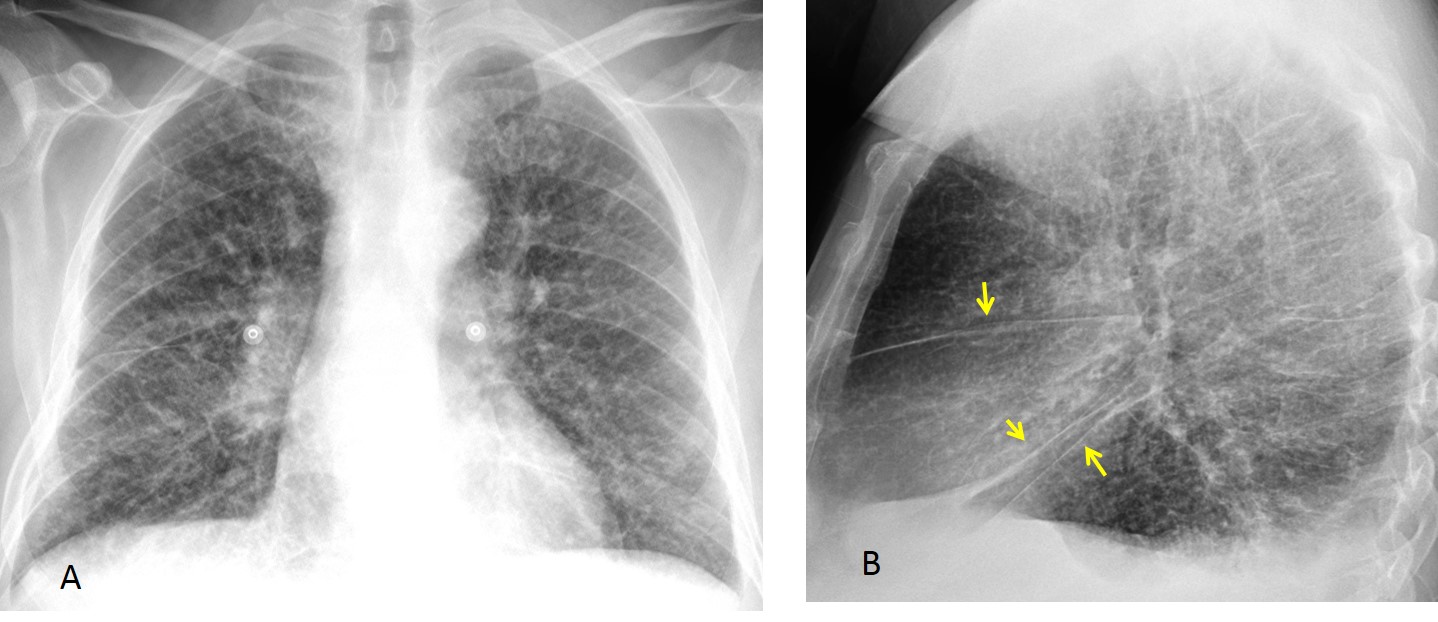
Fig. 13
Fig. 13. 52-year-old man with interstitial lung disease. Note the thickening of fissures, more evident in the lateral view (B, arrows). Diagnosis: lymphangitic carcinomatosis.
Follow Dr.Pepe’s Advice:
1. Fissure displacement indicates loss of volume of the affected lobe
2. Masses within a fissure have a typical ovoid shape with tapering edges. They correspond to either loculated fluid or a fibrous tumour of pleura.
3. Overall fissure thickening is due to pulmonary oedema or chronic lung disease.


I think A inferior accessory fissure.
RLL collapse is unlikely because there is no volume loss in right hemithorax.
there is no loss of silhouette of the right heart border, therefore i think RLL pneumonia is not likely.
Sorry to disagree: RLL disease does not alter the right heart contour
i think it is a LRL collapse
Hello,
there is obvious fissure going from the right hilum to middle part of right diaphragm. Also there is increased lucency in most part of right lung. I suppose some overdistension of lung lobes with alteration of fissure.
Maybe some chronic state?- RLL hipoplasia.
Or partially collapse RLL- there could be (but I’m not so sure:) lost of medial part of diaphragm and poor visualization of descending right lower lobe pulmonary artery.
I think there is a partial RLL collapse in combination with right inferior accesory fissure
– There is decreased right lung density
– There is a triangular lung density adjacent to the right heart border without loss of clarity (no silhouette sign)
– i think there is also blunting of the right costophrenic angle.
There is an overdistention of the RUL. Right hilum is poorly visible, no interlobar artery on the right site.
There is no siluette sign so the RML colaps is excluded.
It could be RLL colaps or some kind of RLL hypoplasia.
Excellent description and correct diagnosis.
….<<<<<<<<polmone iperlucente omolaterale o S.S.J McLeod
Excellent case!
Thank you very much
Want to congratulate those of you who mentioned the right diagnosis: Mahmoud zaki (first one),Borsuk, Gus (hesitating) and specially Ivette.