Dr. Pepe’s Diploma Casebook: Case 75 – SOLVED!
Dear Friends,
Today I am showing radiographs of a 48-year-old woman, native of Central America, with endometrial carcinoma. Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
Diagnosis:
1. Lung metastases
2. Pneumonia
3. Parasitic disease
4. None of the above


Findings: PA radiograph shows an ill-defined opacity in the left lung, running from top to bottom (A, white arrows). The opacity extends towards the neck (A, red arrow), which suggests that it is external to the lung. A photo of the patient (B) confirms that a long braid is the cause of the opacity. The two nodules in the lower lungs are the nipples (A, yellow arrows).
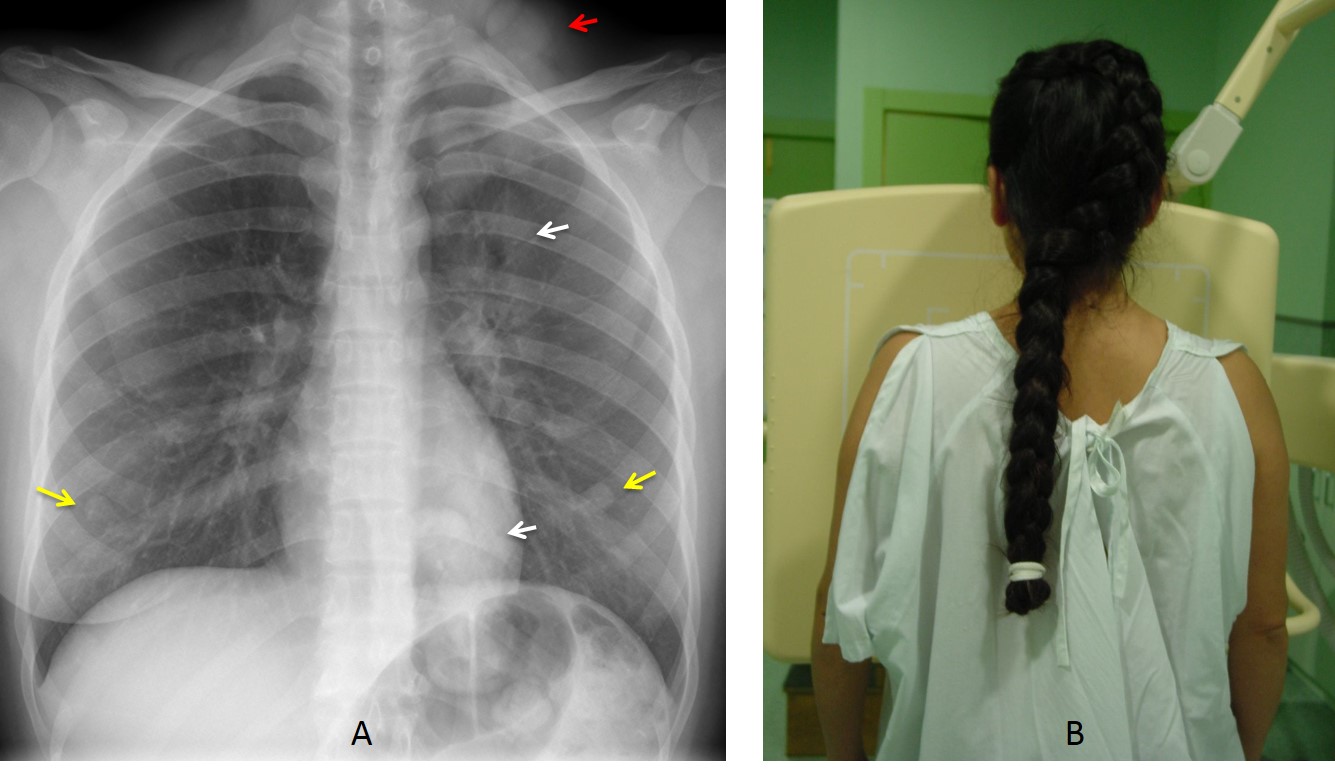
Final diagnosis: hair braid simulating a pulmonary infiltrate
The purpose of this presentation is to discuss elements in or about the chest wall that may cause abnormal shadows on chest radiography. Those related to the thoracic skeleton were shown in Dr. Pepe’s Diploma Casebook Case #57.
These elements may be classified as external to the body (hair, garments) or within the soft tissues of the chest wall (cutaneous nodules and nipples, foreign bodies, calcified breast implants).
Long hair may project over the upper lung, simulating apical disease. Braids may be confused with pulmonary nodules or infiltrates (Figs. 1 and 2). Strands of loose hair may simulate linear fibrotic infiltrates (Fig. 3). The clue to the diagnosis lies in recognizing that the abnormality extends to the neck.
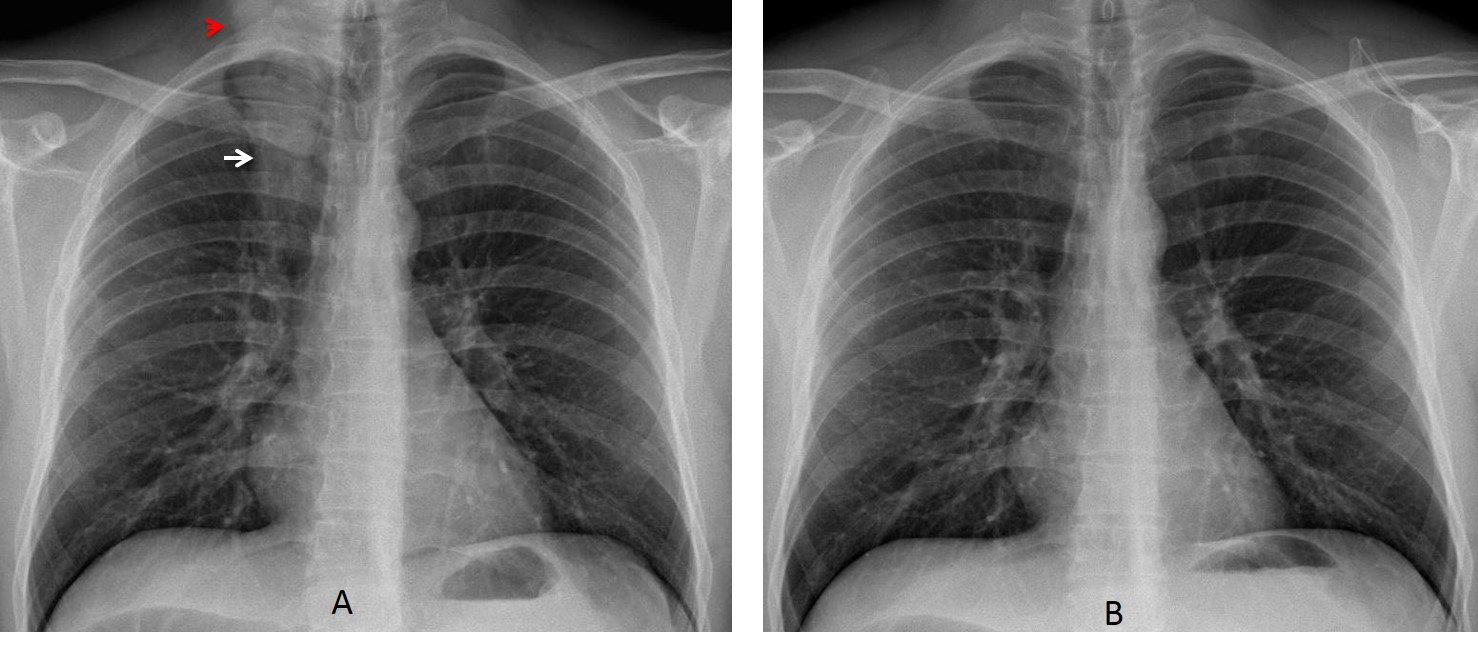
Fig. 1
Fig. 1: 25-year-old man with braided hair simulating a LUL infiltrate (A, arrow). The opacity extends to the neck, giving away the diagnosis (A, red arrow). After raising the braid, the chest looks normal (B). Remember that men also wear their hair long.
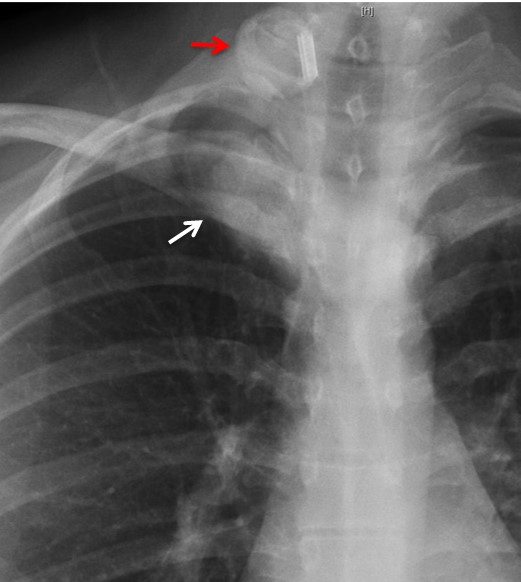
Fig. 2
Fig. 2: Braid simulating an apical pulmonary nodule (white arrow). The rubber band (red arrow) suggests the correct diagnosis.
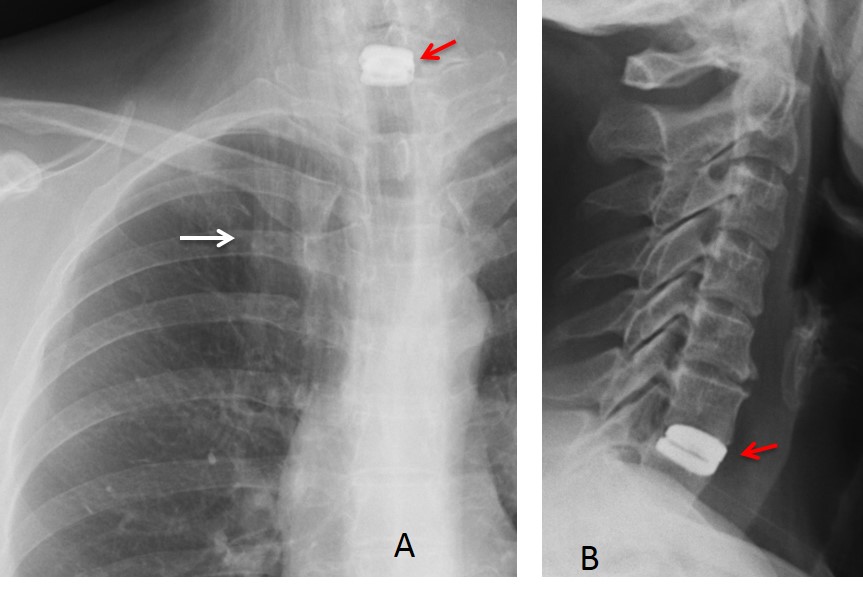
Fig. 3
Fig. 3: Loose hair simulating a linear infiltrate or fibrosis in the right apex (A, white arrow). The opaque rounded opacity that looks like a hair clasp (A, red arrow) is a surgical prosthesis replacing a cervical disc (B, red arrow).
Clothing artifacts occur when the technician does not ask patients to remove garments that have logos or images on them. This usually happens with women, out of respect for modesty or for religious reasons (Figs. 4 and 5).
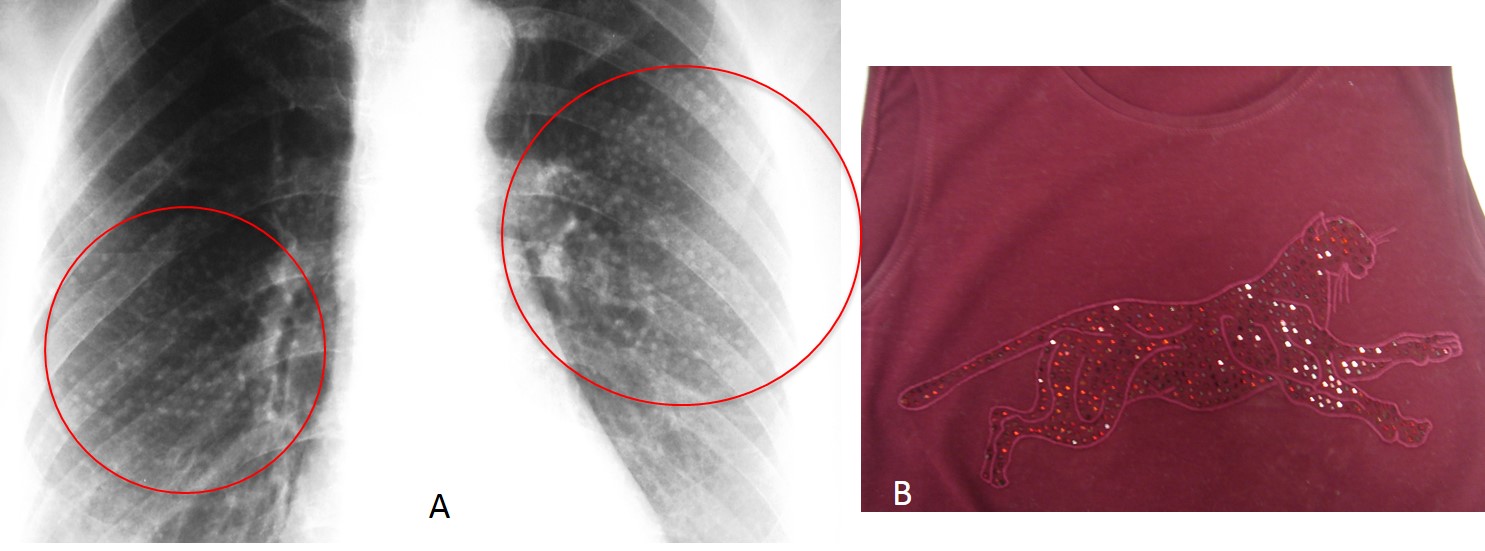
Fig. 4
Fig. 4: 27-year-old woman with multiple miliary nodules in both lungs (A, circles). The opacities result from a jeweled panther on the shirt she was wearing (B).

Fig. 5
Fig. 5: A veil worn by a Muslim woman causes multiple metallic artifacts in the upper lungs.
The most common cause of false lung nodules are skin lesions and nipple shadows. In skin nodules, visual inspection of the chest will demonstrate the lesion and confirm the diagnosis (Fig. 6). If there is any doubt, a marker can be used.
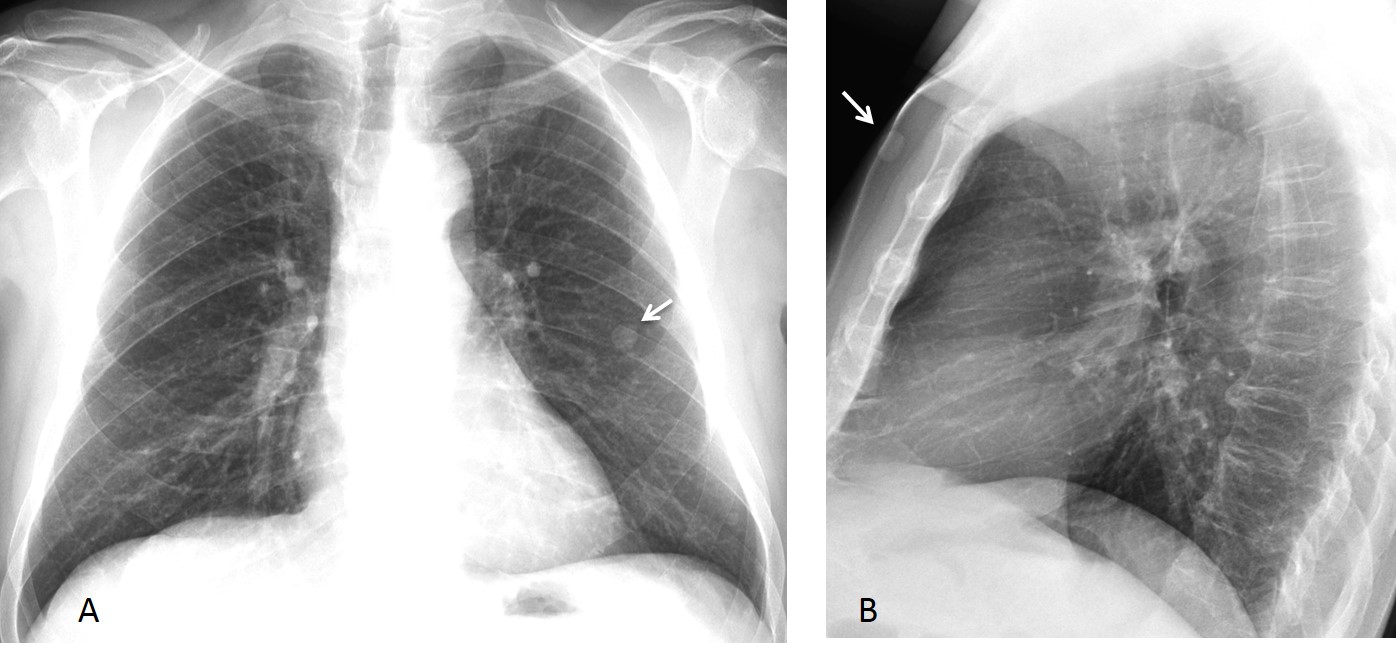
Fig. 6
Fig. 6. Chest wart simulating a lung nodule in the PA film (A, arrow). Lateral film shows the wart in the skin of the anterior chest wall (B, arrow). The wart is higher in this view because the upheld arms elevate it.
Nipple shadows are seen in 3% to 10% of PA chest radiographs. In about 10% of these patients, the identification may raise doubts. Comparison with previous films will confirm the stability of the nodules (Fig. 7). In case of doubt, nipple markers should be placed. Routine use of nipple markers has been proposed in oncologic patients.
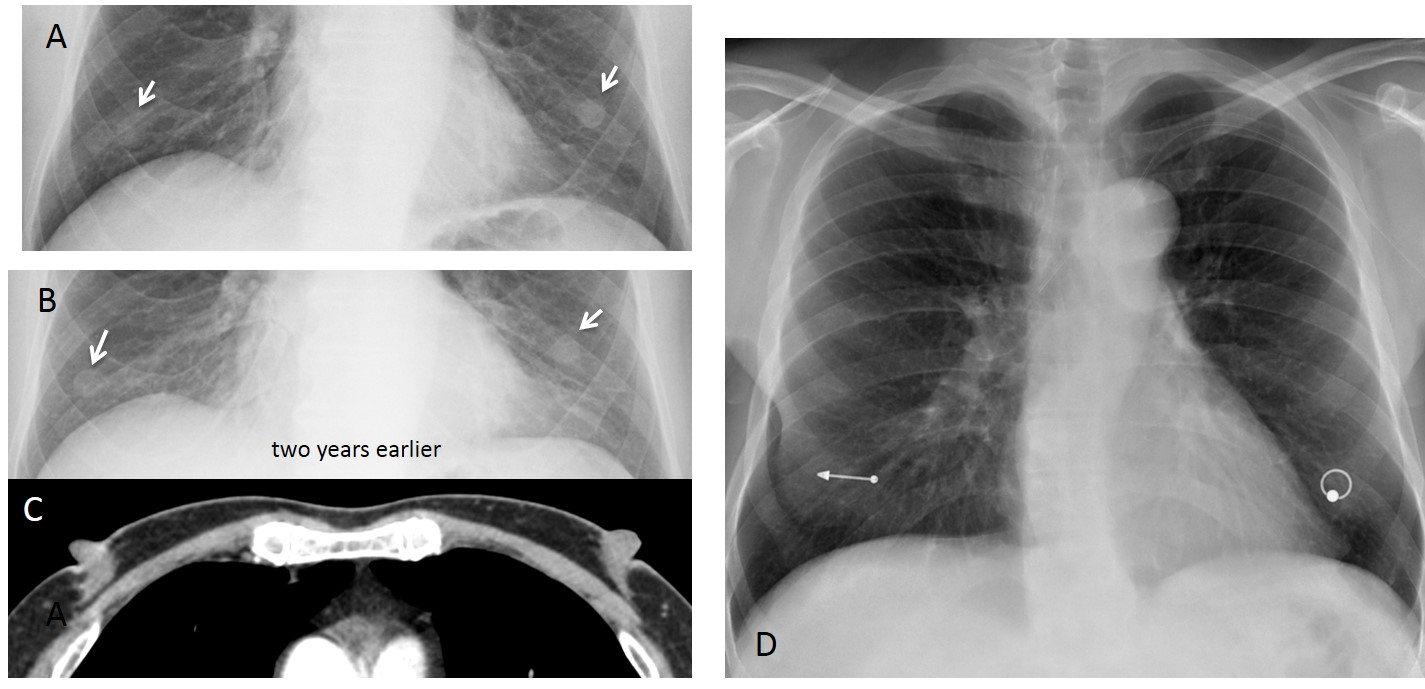
Fig. 7
Fig. 7: 58-year-old man with typical bilateral nipple shadows (A, arrows), unchanged in comparison with a previous film (B, arrows). Nipples are well seen on axial CT in the same patient (C). Nowadays, patients may come with their own nipple markers! (D).
Unilateral enlarged nipple shadows are suspicious findings. Visual inspection should be done to confirm that the nipple is indeed enlarged (Fig. 8). Occasionally, a true lung nodule may simulate a nipple shadow, even with nipple markers. In such cases, CT should be performed (Fig. 9)
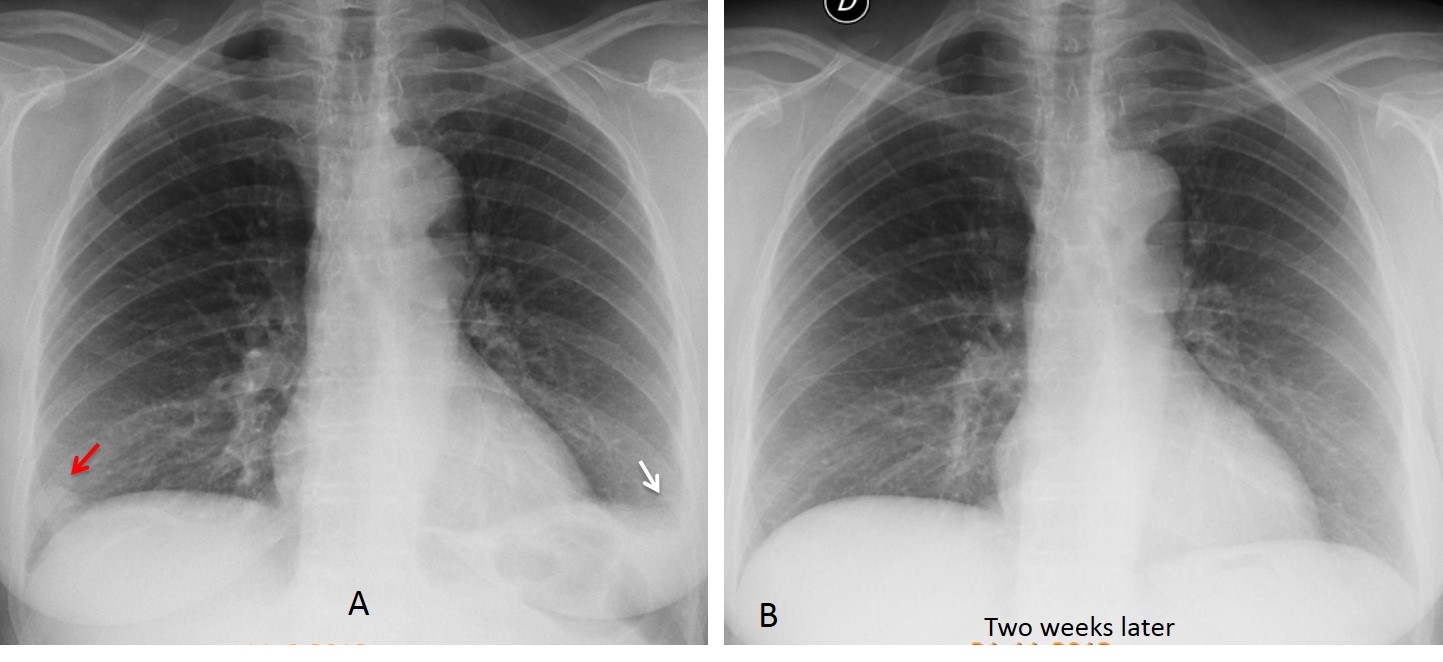
Fig. 8
Fig. 8: 61-year-old woman with left pleuritic chest pain. PA chest film shows a small amount of left pleural fluid (A, white arrow) and a nodule at the right costophrenic angle (A, red arrow). Visual inspection showed a large right nipple as the cause of the false nodule. Two weeks later, the pleural effusion has disappeared and the nipple shadow is no longer seen.
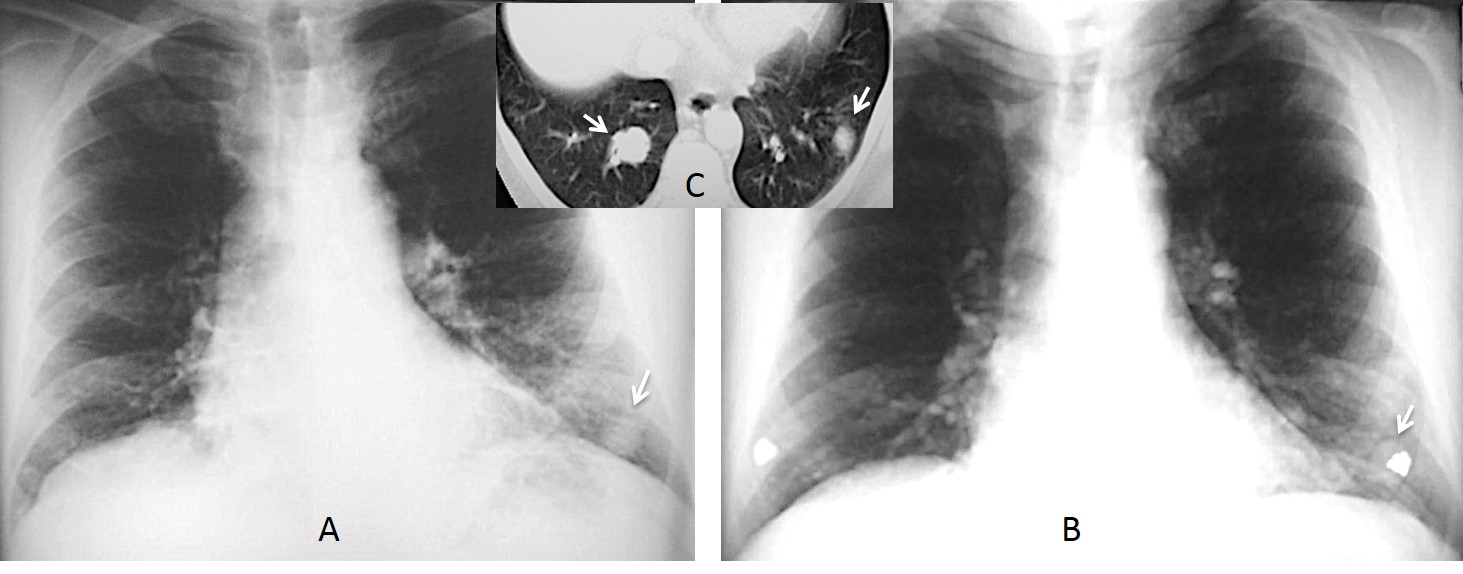
Fig. 9
Fig. 9: 54-year-old man with a renal tumour. PA film shows a nodule in the LLL (A, arrow) that simulates a nipple, even with a nipple marker (B, arrow). Axial CT shows a metastatic nodule in the LLL and a larger one in the RLL, not seen in the PA chest radiograph (C, insert, arrows).
Metallic opacities in the subcutaneous tissues are usually caused by surgical sutures (Fig. 10 A). Occasionally, broken acupuncture needles may be visible in the soft tissues of the chest (Fig. 10 B).
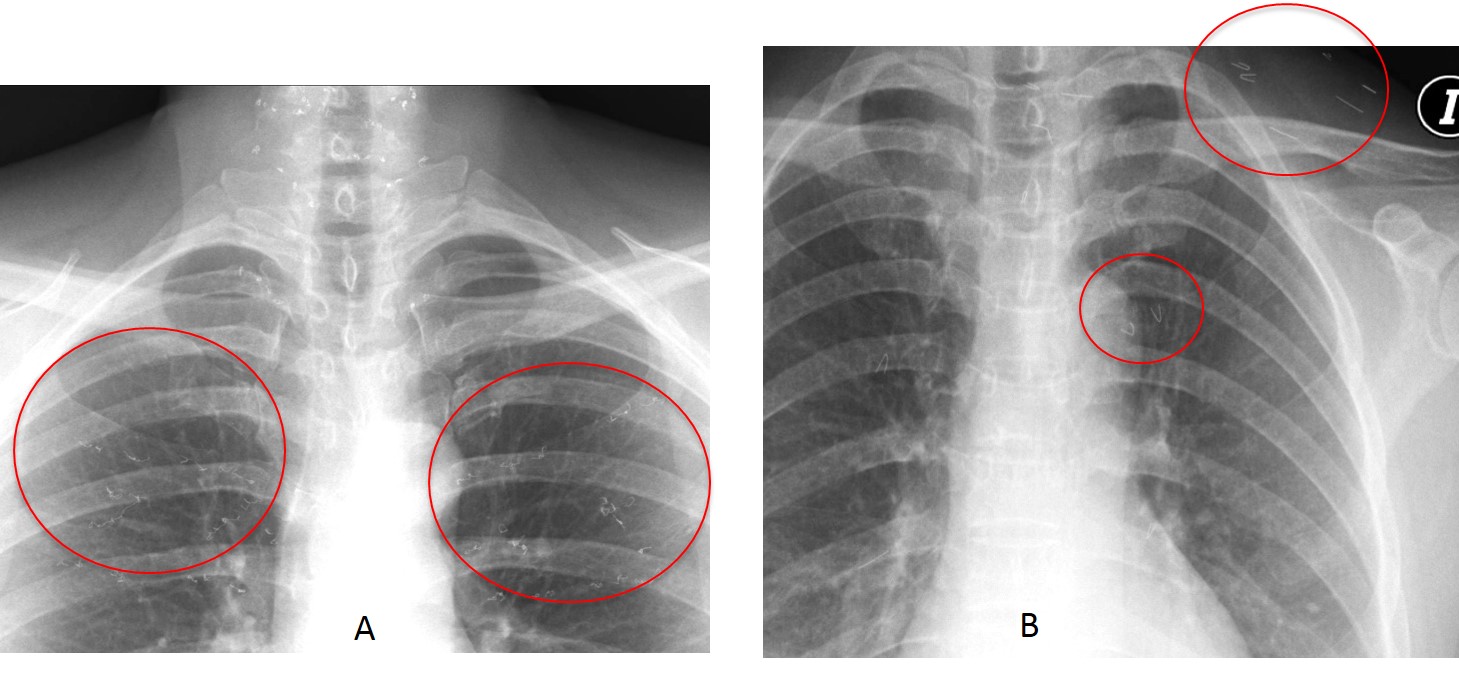
Fig. 10
Fig. 10: Gold threads implanted in the subcutaneous tissue of the neck and cleavage (A, circles). This is not an uncommon procedure in plastic surgery to correct sagging skin. (B) Straight and bent metallic opacities in the soft tissues, some of them projected over the lung fields, represent fragments of acupuncture needles (B, circles).
An uncommon cause of metallic opacities are shotgun pellets. These are low-velocity missiles that usually remain in the soft tissues. They have a characteristic appearance. Occasionally, some of the pellets may penetrate a vessel and lodge in the heart or peripheral viscera (Fig. 11). Management of the pellet embolus depends on the location and symptoms.
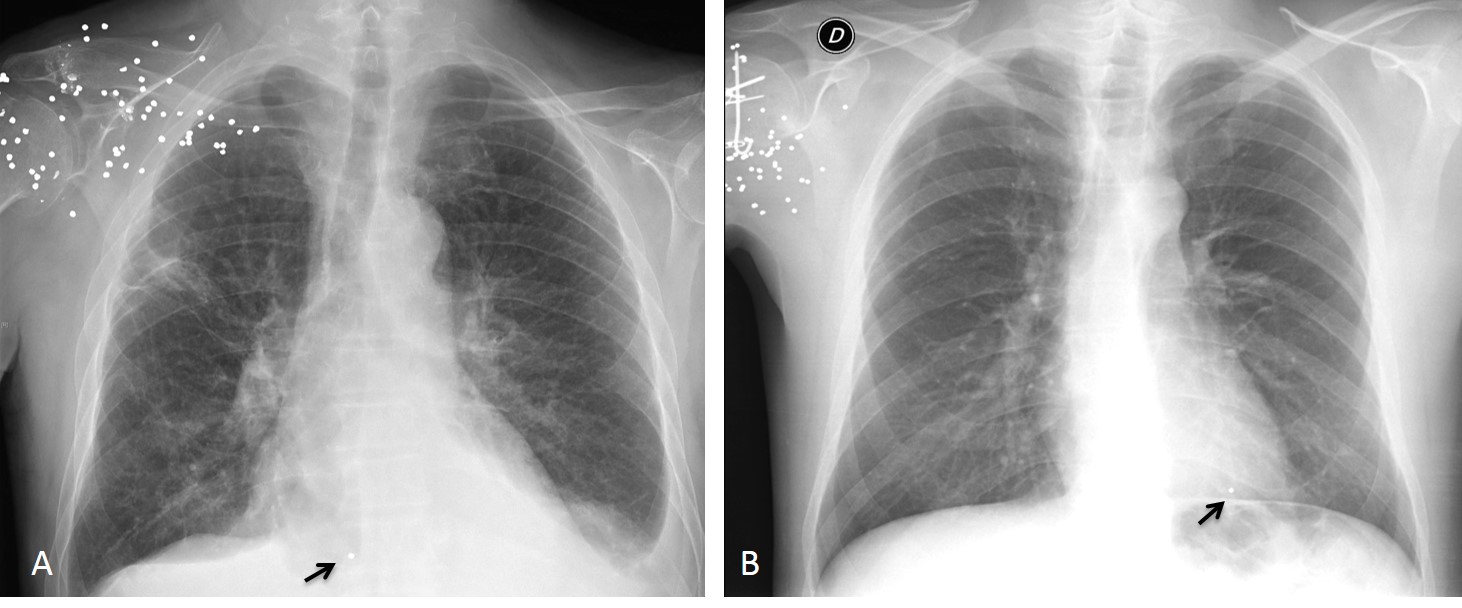
Fig. 11
Fig. 11. Two patients after a shotgun injury. The pellets are visible in the soft tissues of the right shoulder. In both patients, a single pellet has migrated to the heart (A and B, arrows). Lateral view (not shown) confirmed the intracardiac location.
Calcifications in the soft tissues of the chest may be seen in systemic diseases. More common are calcifications related to breast implants, occurring in the surrounding fibrous capsule as the implant ages (Fig. 12). These sometimes generate diagnostic problems for those unaware, especially in cases of unilateral or small calcifications (Fig. 13).
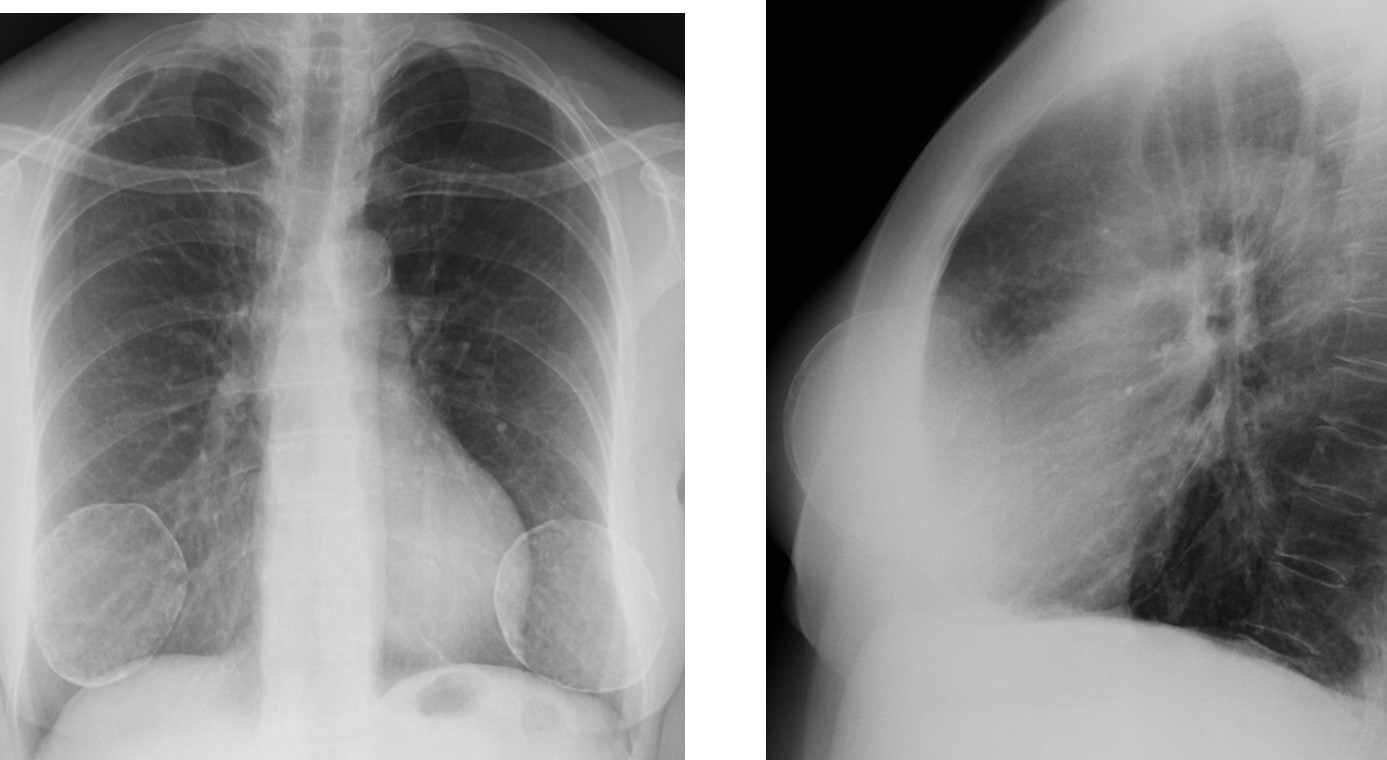
Fig. 12
Fig. 12: Obvious calcified breast implants in PA and lateral views.
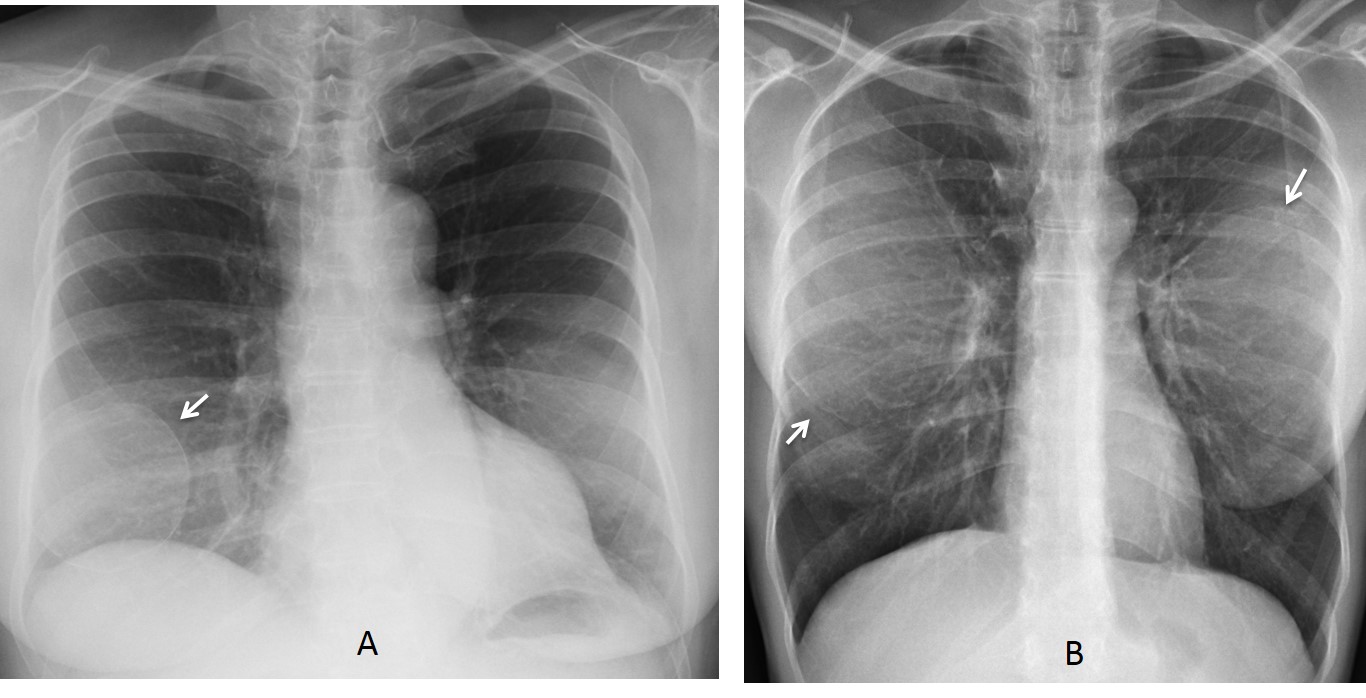
Fig. 13
Fig. 13: 52-year-old woman with unilateral calcified implant (A, arrow) which could raise the doubt of a cystic lesion of the right lower lung. In the second patient, bilateral implants appear as ill-defined opacities with faint rim calcification (B, arrows).
Follow Dr.Pepe’s Advice:
1. If a hair artifact is suspected, look at the soft tissues of the neck.
2. Garments may create weird lung shadows.
3. Unilateral nipple shadows may generate diagnostic problems.
4. Metallic opacities are caused by surgical sutures and occasionally, shotgun pellets.


4.
NF2- interstingly confined to the left side in majority.
4. Left mastectomy. Pony tail towards the left side?
Left mastectomy.Breast cancer recurrence? parasternal und supraclavicular nodes?
left upper lobe consolidation.
+ vascular anomaly?
Hello,
A patient is post left mastectomy and there are supra and infraclavicular nodes outside lung on left side. I suppose reccurence of breast cancer in metastatic lymphadenopathy.
..contro l’ombra cardiaca , in basso, a sx, si proietta opacità ovalare, a margini netti, con alcuni inclusi più rx-opachi( cutanea ?)….immagine osteosclerotica, sul margine anteriore della 5 costa sx…in LL formazione rx-opaca all’interno dell’apparato gastrointestinale….
Saludos Dr. Pepe!!! Veo una imagen nodular silueteada con el mediastinicos superior a nivel derecho y prominencia del hilio izquierdo, veo que no hay la mama derecha tampoco así que me voy por la numero 4 creo son ganglios metástasicos
In my opinion, there are multiple osteosclerotic lesions in the ribs.
As mentioned, there is also loss of left breast tissue, suggesting left mastectomy.
There are also retrocardiac opacities but im not sure what are those.
The gastric bubbles are abnormally large and is displaced near to heart suggesting maybe splenomegaly secondary to mets or gastric outlet obstruction?
In lateral view, there is lymphadenopathy ‘doughnut sign’ surrounding the bronchus.
Se observa incremento de la densidad de tejidos blandos superficiales en región cervicotoracica izquierda de aspecto linfoide agregando incremento de la anchura de la linea paramediastinal superior en la confluencia de la VCI las características sugieren una infección aguda asociada a enfermedades tropicales(leismaniasis, chavas etc)sin embargo por los antecedentes de CA se tendrían que caracterizar los ganglios.
Left Mastectomy – Left supraclavicular LN
Lateral view without any special anomalies. On PA view there is an opacification along spine on the left side, it is visible in soft tissue above the ribs and also below the diaphragm. So it is in soft tissue or on the skin -braid of hair?
I don’t think the lady is after mastectomy. There is a round opacification on the anterior part of the 5th rib – This is the left nipple, almost at the same level as the right, densities of both lungs are the same only the border is not so sharp as on the right.
Nice discussion. And you are right. Patient has both breasts.
Hi!
At first, after looking on the PA view, I would’ve considered those nodular opacities to be most likely lung metastases associated with lymphadenopathy (in the mediastinum and laterocervical). But when I saw the lateral view, I know they aren’t in the lungs at all, but in the superficial soft tissues. In my opinion, they seem to indicate most likely a congenital condition, which obviously includes benign soft tissue tumours, like neurofibromatosis. I’m looking forward to see more investigations or clues. I would like to add that this post showed me once again the importance of chest lateral views.
left mastectomy
? lymphangitis carcinomatosa
ok endometrial carcinoma metastatic L.nodes
You try too hard. Use your common sense.
As this time of the day, I can give you the right answer: braided hair.
This is important case, because hair and other artifacts may simulate other pathologies. At least to a few of you!
Congratulations to Lola la Piconera and Yvette.
She is from matsu picchu no? 🙂
now is obvious!!!!
The whole idea is to avoid repeating the same mistake
4. non of above