Dr. Pepe’s Diploma Casebook: Case 77 – SOLVED!

Dear Friends,
Today I am presenting images of a 72-year-old man with pain in the sternum. Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
Diagnosis:
1. Metastases
2. Chondrosarcoma
3. Osteomyelitis
4. Any of the above


Findings: There is a lytic lesion in the body of the sternum (A and B, arrows). The lesion has breached the cortical bone and has an aggressive appearance. Among the answers offered, osteomyelitis usually affects the sternoclavicular area and has a larger soft tissue component. Chondrosarcoma usually arises in the manubrium and has a calcified matrix. The most likely diagnosis is metastasis, which is the most common focal lesion of the sternum.

The PET-CT image shows marked uptake at the lesion (C, arrow). Further investigation discovered a primary carcinoma of the liver. On CT imaging obtained 6 months later, the sternal lesion has progressed (D and E, arrows).

Diagnosis: sternal metastasis from hepatocarcinoma
This case is presented to discuss disease affecting the sternum. The sternum may be the cause of chest symptoms and should be examined in the chest radiograph to exclude relevant disease. Sternal conditions are not visible in the PA view and may be overlooked if a lateral view is not obtained. When sternal pathology is suspected, it is imperative to obtain a CT.
Conditions that affect the sternum may be classified as:
1. Focal tumour
2. Infection
3. Arthritis
4. Fracture
5. Congenital malformation
Most tumours of the sternum are metastatic. As elsewhere in the skeleton, they may be lytic or blastic. The most common sources are: breast, lung, thyroid, kidney, colon, and lymphoma.
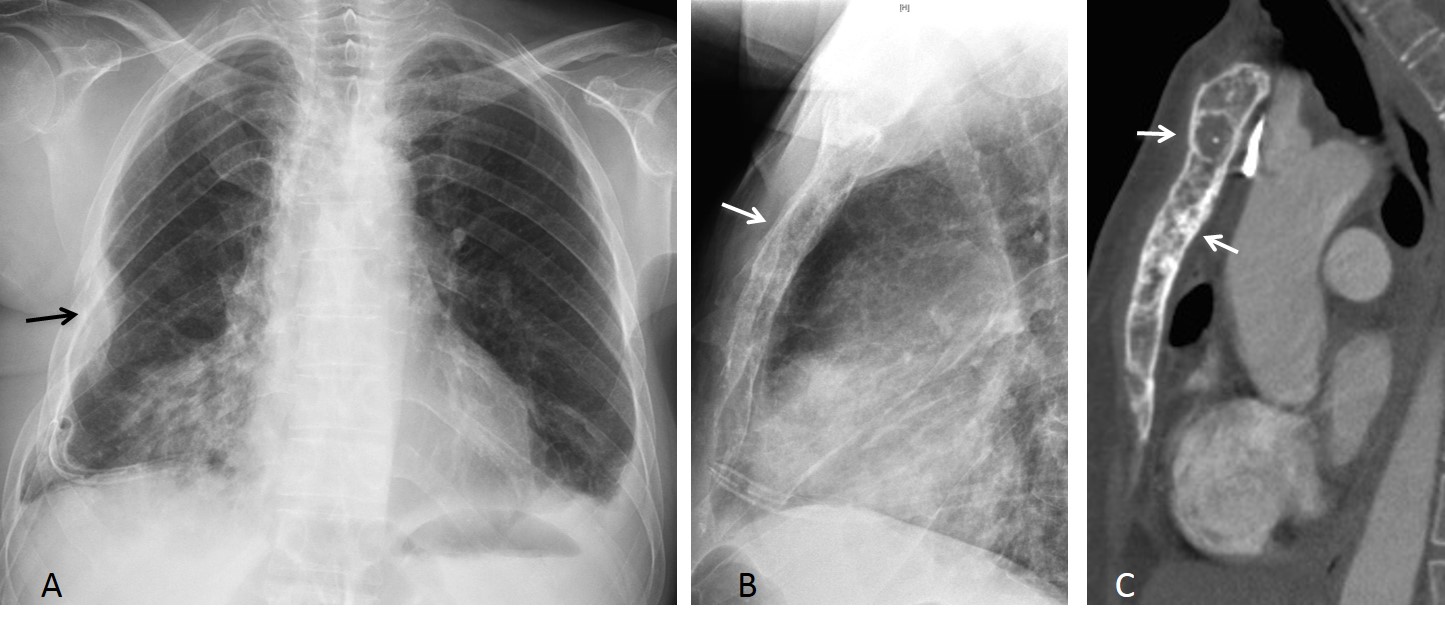
Fig. 1
Fig. 1: 51-year-old woman with metastatic breast carcinoma. PA chest radiograph shows a rib lesion with a soft tissue mass (A, arrow). Lateral view shows metastatic involvement of the entire sternum (B, arrow), better visualised in the sagittal CT, which shows lytic and blastic lesions (C, arrows).
Multiple myeloma and solitary plasmocytoma are the most common hematologic diseases that affect the sternum. The lesions are typically lytic and lack intrinsic calcifications. They may be expansive and may simulate lytic metastasis (Fig. 2)
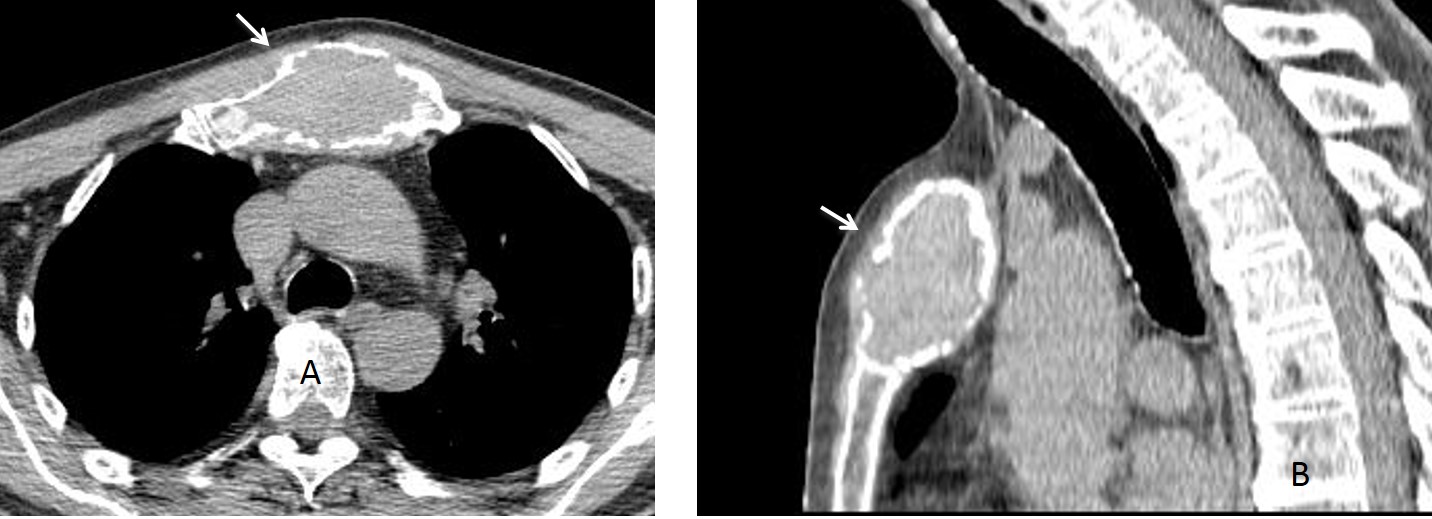
Fig. 2
Fig. 2: 53-year-old man with a solitary plasmocytoma of sternum. Axial and sagittal CT show an expanding lytic lesion affecting the manubrium (A and B, arrows).
Primary tumours of the sternum are rare, and in most cases, malignant. Benign tumours are very uncommon.
Chondrosarcoma, the most common sternal tumour, usually affects the manubrium. Patients commonly present with a large painless mass in the anterior chest wall. CT shows multiple stippled calcifications within the tumour, corresponding to the chondroid matrix (Fig. 3).
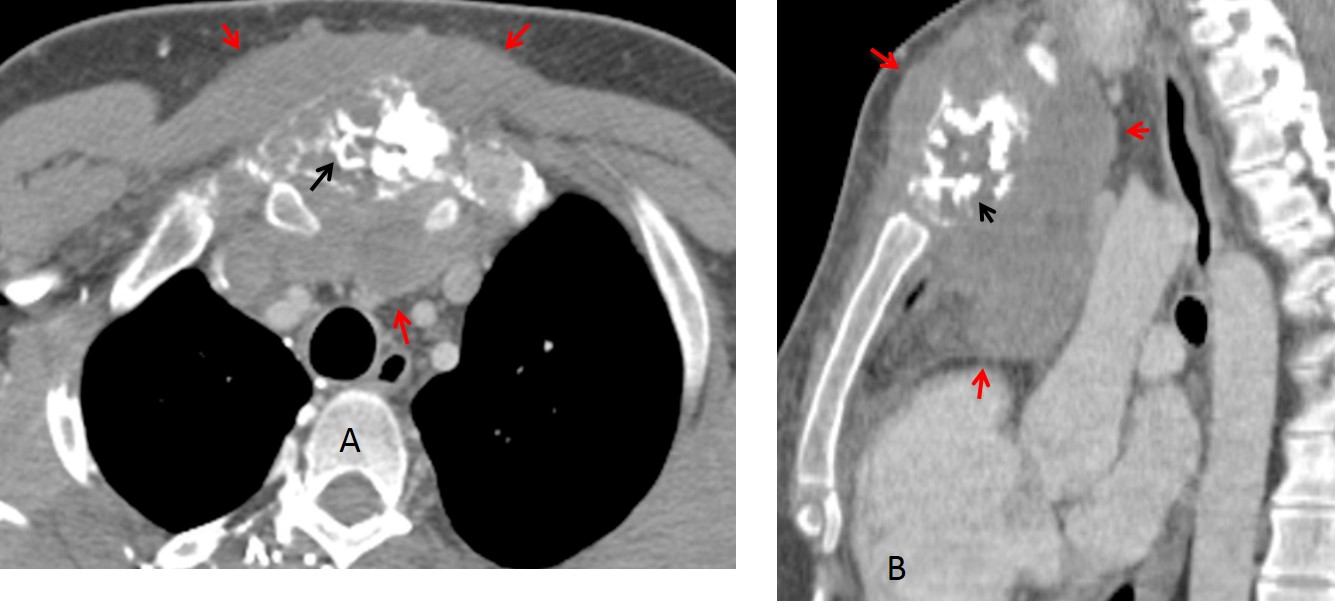
Fig. 3
Fig. 3: 67-year-old man with chondrosarcoma of the sternum. The tumour is affecting the manubrium and has a calcified matrix (A and B, black arrows). There are large accompanying masses (A and B, red arrows).
Primary sternal infections are uncommon and are usually located at the sterno-clavicular joint, affecting the manubrium and/or the head of the clavicle. Bone changes are accompanied by purulent soft tissue collections (Fig. 4).
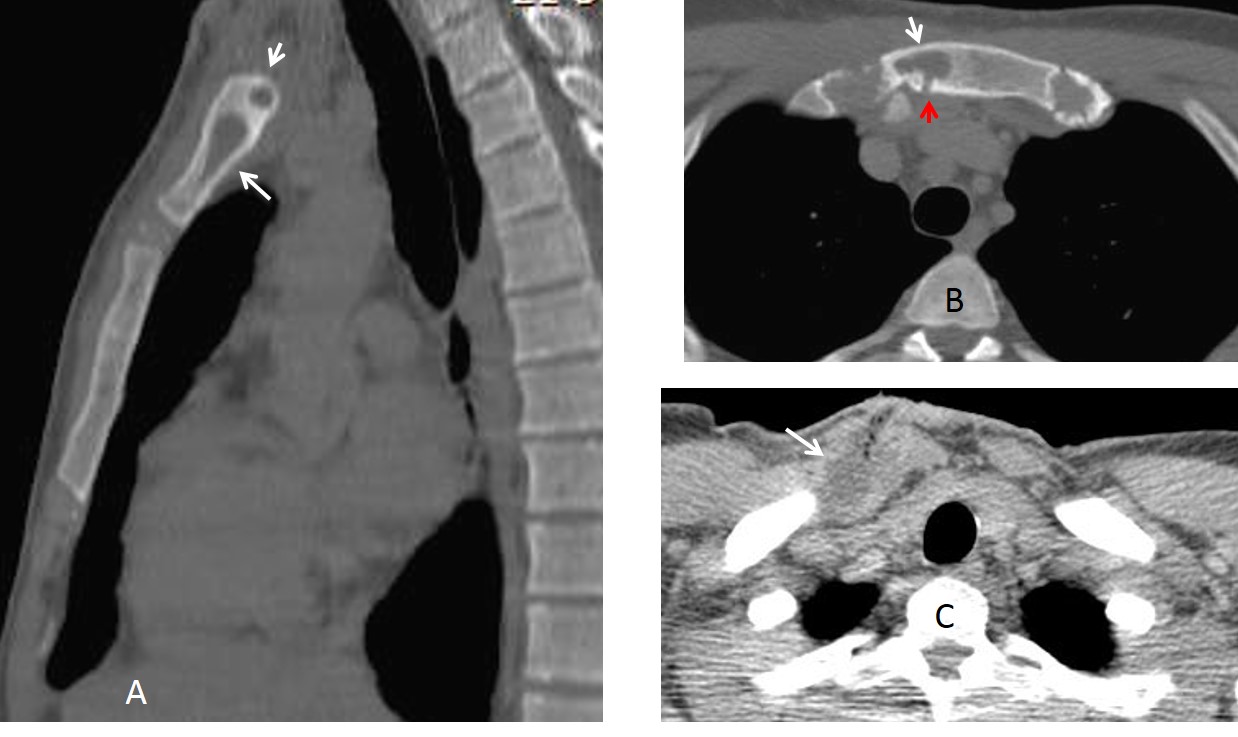
Fig. 4
Fig. 4: 27-year-old drug abuser with osteomyelitis of sternum. Sagittal and axial CT show lytic areas in the manubrium (A and B, white arrows) with a draining sinus (B, red arrow). There is purulent collection in the soft tissues (C, arrow).
Most sternal infections occur secondary to surgery, and are seen in up to 2% of sternotomies. They are accompanied by infected collections in the soft tissues, a potentially severe complication because of the risk of mediastinitis. CT is the imaging examination of choice when this complication is suspected (Fig. 5).
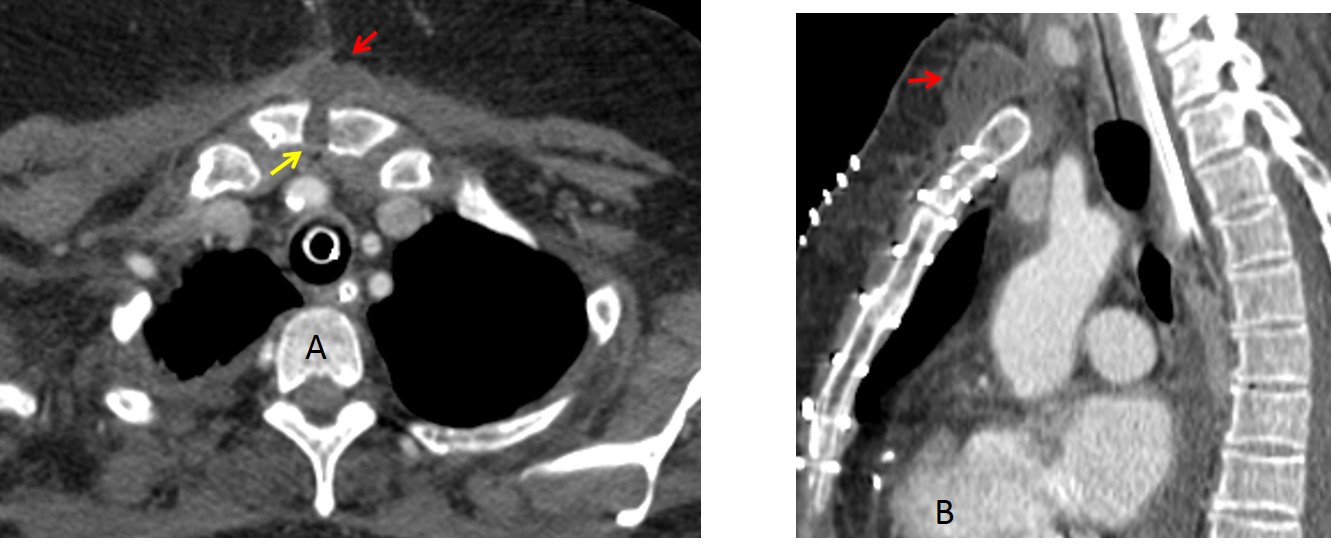
Fig. 5
Fig. 5: sternal infection after a sternotomy. Enhanced axial CT image shows dehiscence of sutures (A, yellow arrow). A purulent collection is seen in the pre-sternal tissues (A and B, red arrows). There is no evidence of mediastinitis.
Sternal fractures are common in car accidents, resulting from an impact with the steering wheel. The fractures usually involve the sternal body. They are important because of their association with pulmonary and cardiac trauma. Minor fractures may go unrecognised and cause chronic chest pain (Fig. 6).
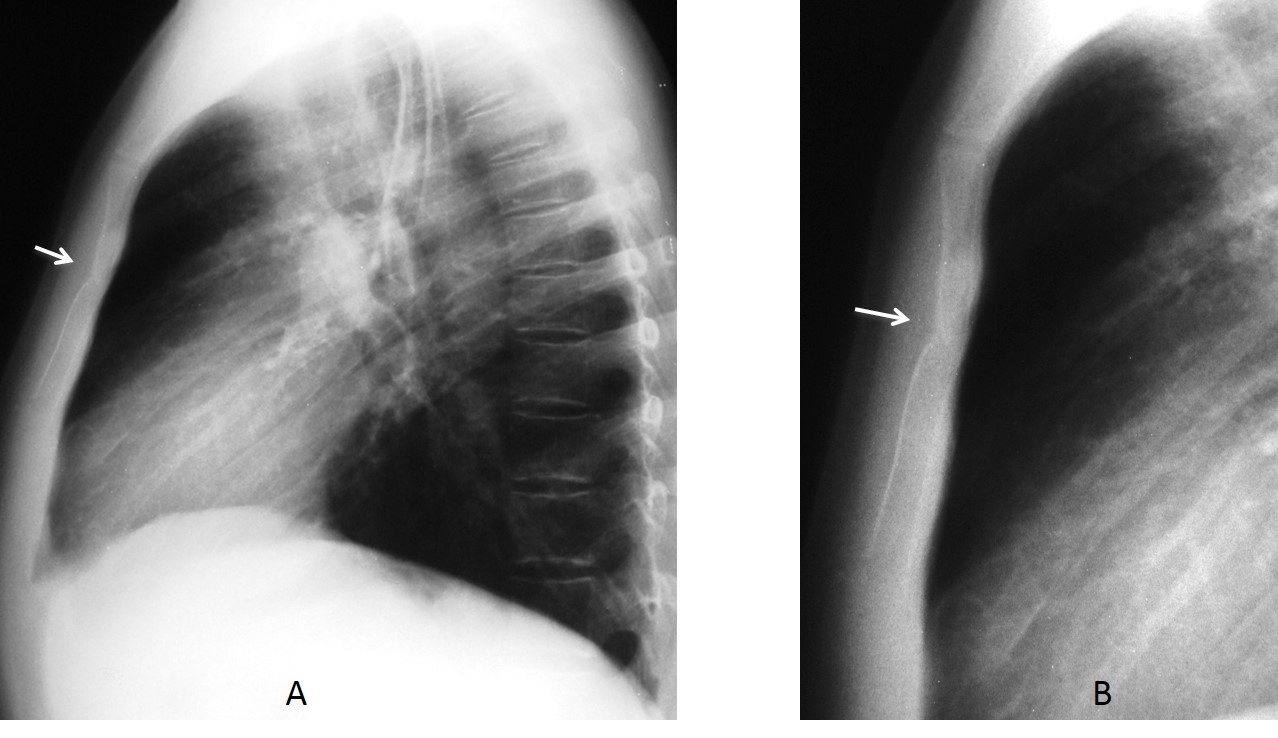
Fig. 6
Fig. 6: 32-year-old man reporting chest pain three weeks after a car accident. Lateral view of the chest shows a small depressed fracture of the body of the sternum (A, arrow). The findings are more evident in the cone down view, which shows sclerosis (B, arrow).
Another cause of sternal fracture is a previous surgical procedure, usually performed in lung transplantation. Transverse sternotomies have a typical appearance and may help to interpret bizarre lung images (Fig. 7).
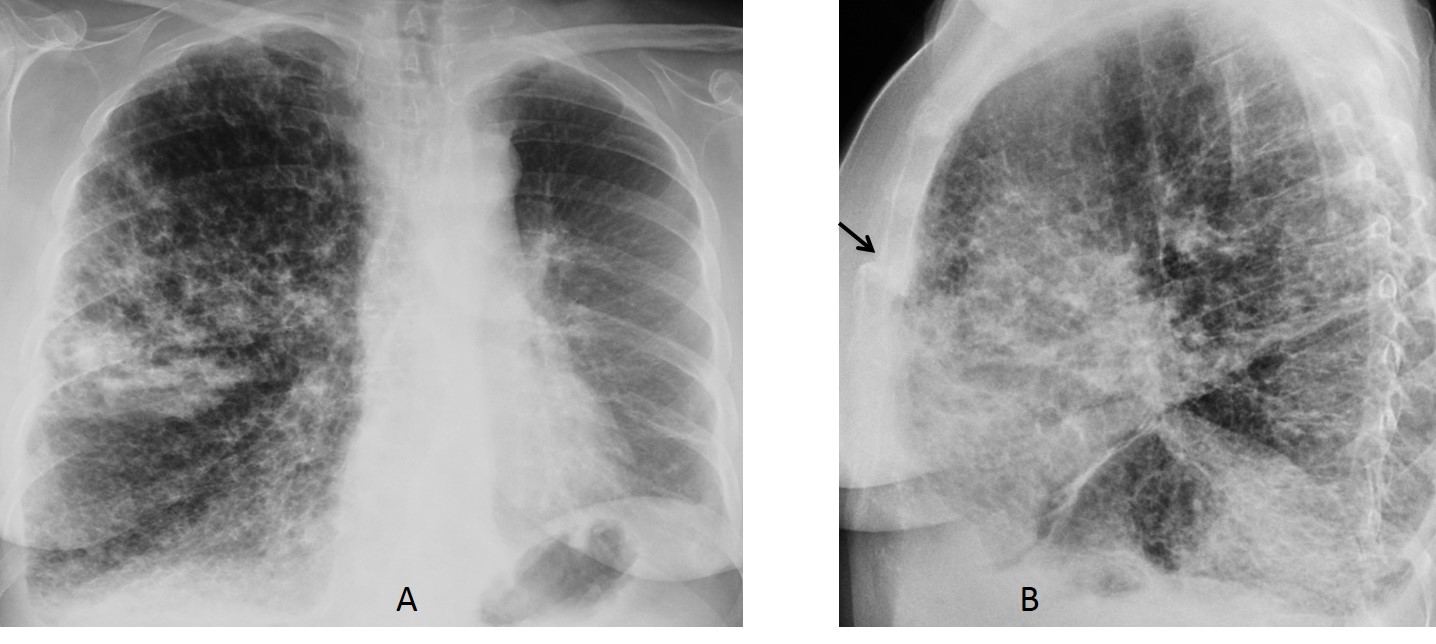
Fig. 7
Fig. 7: 48-year-old woman after a unilateral left lung transplantation. The appearance of the chest can be puzzling if the history is not known. The transverse surgical fracture of the sternum (B, arrow) suggests the previous transplant surgery.
Arthritis, most commonly degenerative osteoarthritis, may affect the sterno-clavicular joints. An unusual condition is SAPHO syndrome, which involves the SC joint in 65%-90% of cases. The characteristic findings are hyperostosis and bone sclerosis (Fig. 8).
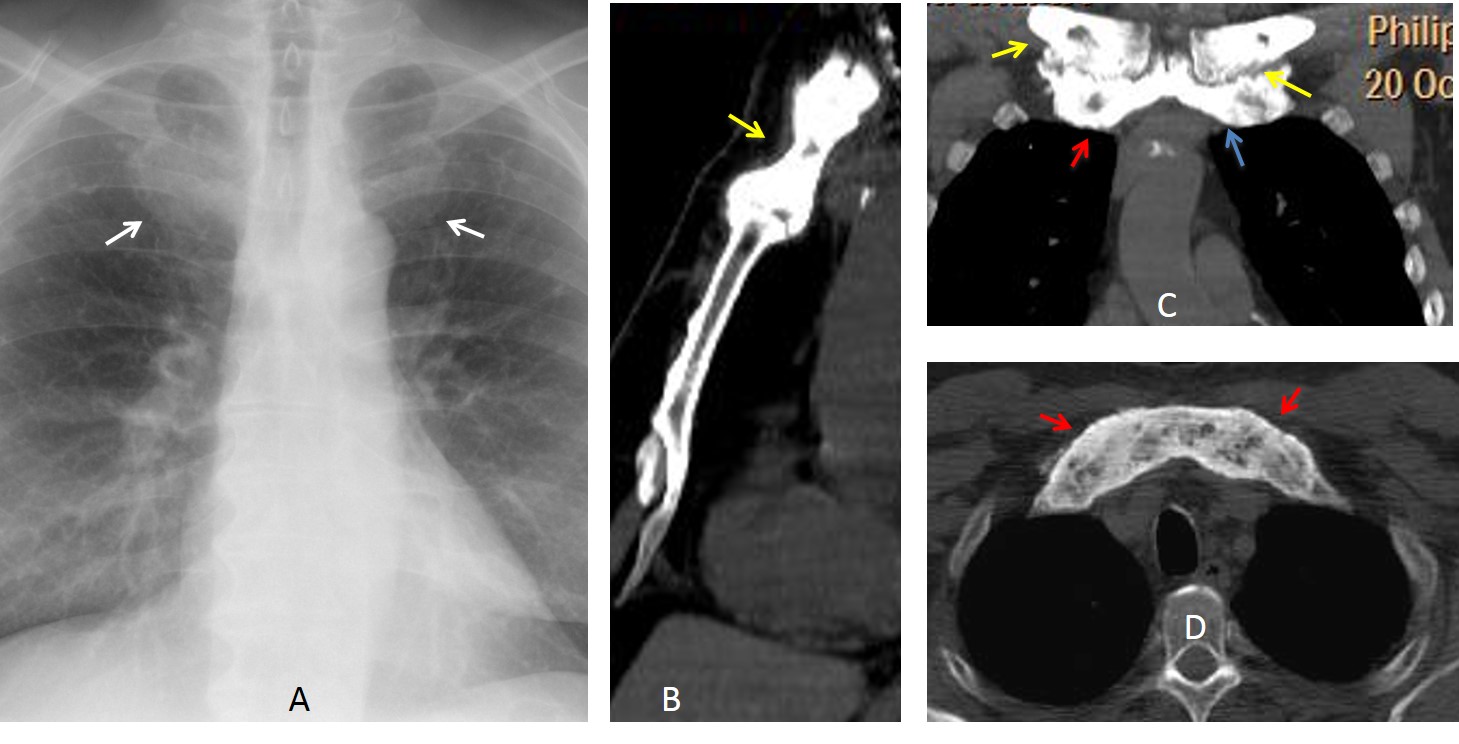
Fig. 8
Fig. 8. SAPHO syndrome in a 68 y.o. woman. PA chest radiograph shows a rounded haziness at the the first costochondral junctions (A, arrows). CT depicts marked sclerosis of the sternal manubrium (B, arrow), proximal clavicles (C, yellow arrows) and first costochondral junction (C and D red arrows). On clinical examination, there were pustular lesions on the soles of the feet.
Pectus excavatum is a common congenital deformity of the sternum. Usually asymptomatic, it may displace the heart towards the left, simulating right middle lobe disease or cardiomegaly. The vertical orientation of the anterior ribs is a clue to suspecting this anomaly in the PA view, which is easily diagnosed with a lateral view. Severe pectus may cause respiratory and cardiac symptoms that may be an indication for surgical correction. For adequate surgical planning, CT should be performed (Fig. 9)
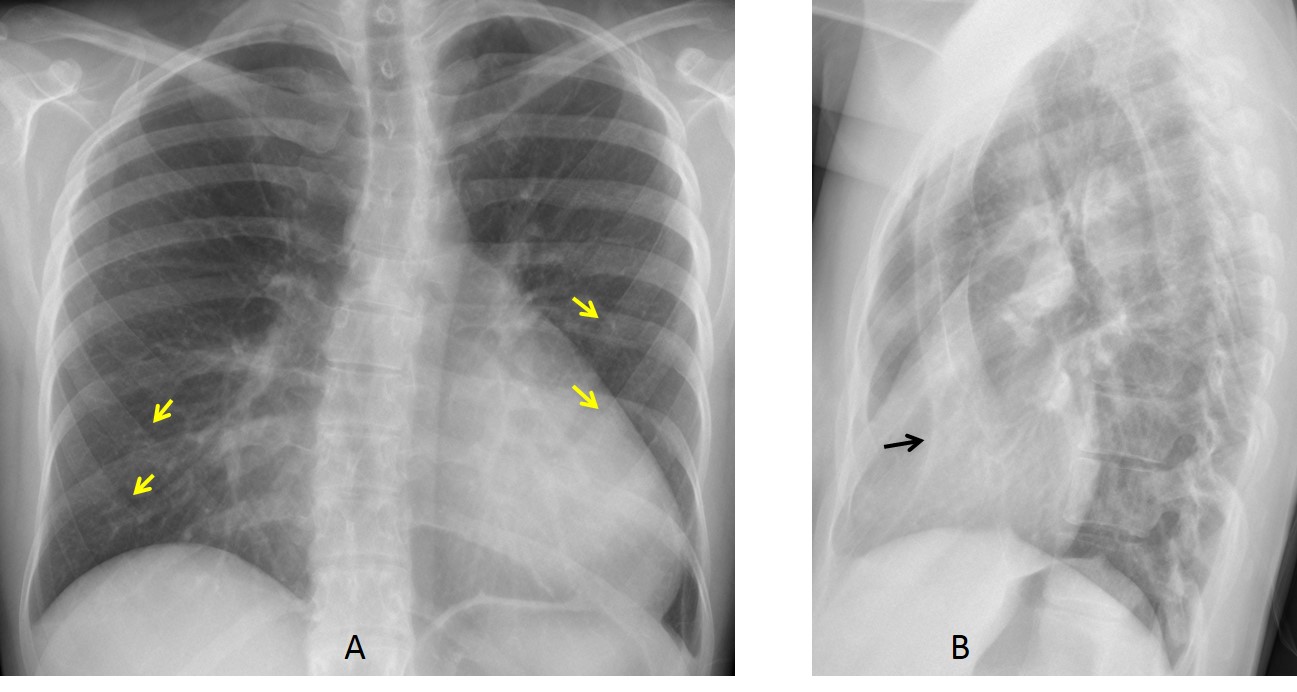
Fig. 9
Fig. 9: 22-year-old man with pectus excavatum simulating cardiomegaly in the PA view. Note the vertical orientation of the anterior ribs (A, arrows). The lateral radiograph confirms the pectus (B, arrow).
Because of the patient’s respiratory symptoms, a CT study was performed. Sagittal and axial CT confirm the marked pectus excavatum (C and D, arrows). CT enables measurements to be taken, to determine whether surgical correction is indicated.
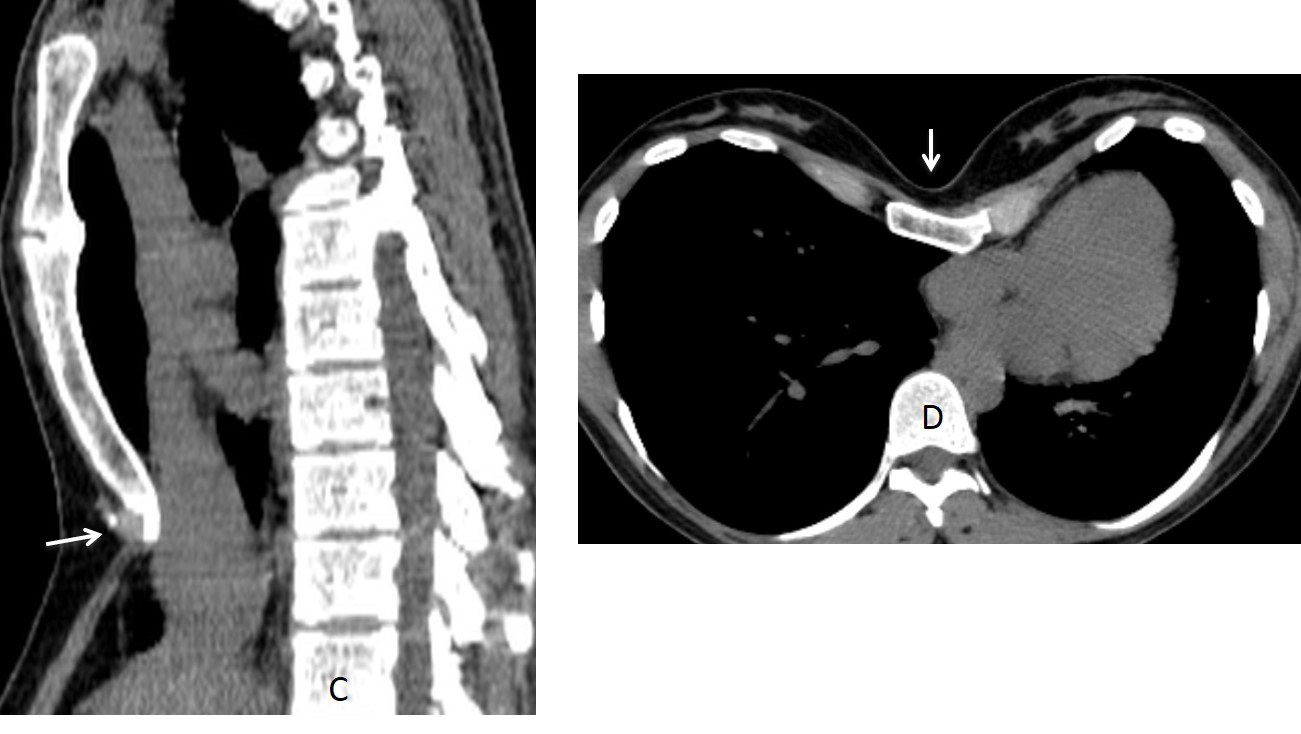
Fig. 9
In pectus carinatum, the sternum is displaced anteriorly (Fig. 10). It is less common than pectus excavatum and is more frequent in males than in females. More than one third are associated with scoliosis and a small percentage have concurrent heart disease.
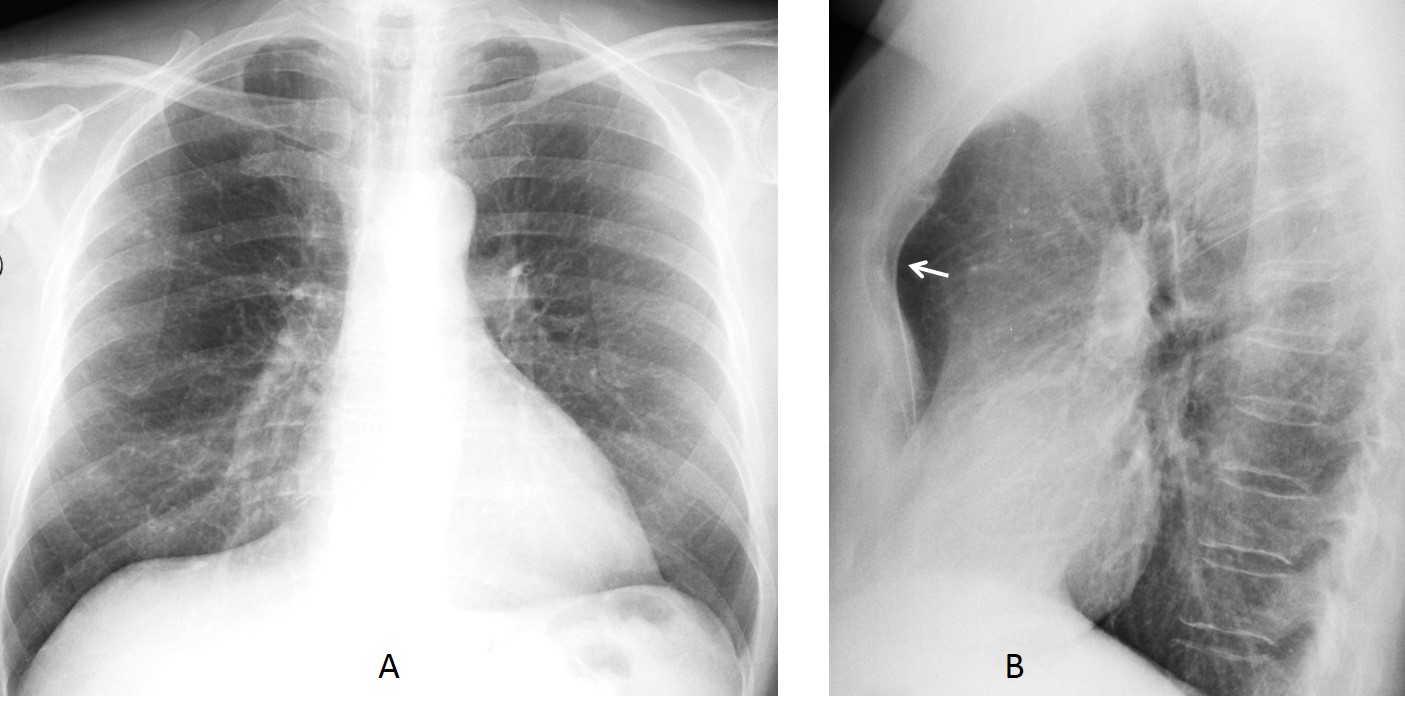
Fig. 10
Fig. 10. Pectus carinatum, only visible in the lateral chest radiograph (B, arrow). The patient did not have any associated malformations.
Follow Dr.Pepe’s Advice:
1. Sternal pathology is better studied with CT.
2. Most focal lesions of the sternum are malignant.
3. Sternal infections usually affect the sternoclavicular joints.
4. In a young asymptomatic patient with apparent cardiomegaly, always exclude pectus excavatum.


Osteomyelitis
…metastasi….c’è un’altra immagine, simile e più piccola inferiormente… l’ilo di sx mostra una formazione solida sospetta per cr ilare… complimenti x il triplete….saluti alla prossima finale !
lack of calcification or surrounding soft tissue swelling goes against, although does not completely rule out chondrosarcoma and osteomyelitis, respectively. Metastasis is the most probable diagnosis.
Hello,
I think correct answer is 4- any of the above.
There is finding in a middle part of sternum with scalloping of endosteum and defects in cortical layer and little of soft tissue occupation nearby.
Any of possible diagnosis could be found in this age group and could provoke pain.
Maybe chondrosarcoma is little less possible because of lack of calcification- but it isn’t patognomonic.
4.any of the above
Four answers and three choices. Good!
i say any of the above but my first choice is metastasis.
The patient has gynecomastia, pericardiac fat deposition and parasternal lymph nodes .
i can see pericardial calcification on the level of sternal mass on sagital view.
Lucent lesions of the sternum should be considered malignant until proven otherwise.
For the age of patient we consider metastasis as first DD.
Mets in this age group unless proven otherwise…
All answers are posible in this case.
Metastasis is the first possibility
I think I will go for Mets (age group)
lack of chindroid matrix mineralization can somehow exclude chondrosarcoma
while absence of adjacent soft tissues significant inflammatory reaction is not In the favour of osteomyelitis
agree
Lytic lesion in the body of the sternum: DDx metastatic lesion, myeloma/plasmacytoma, lymphoma, infection (osteomyelitis).
any of the above
Mets
Metástasis si te best choice.
1. Metastases
Dear friends, I believe most of you are right. Although any of the conditions is possible, metastases should be the most likely diagnosis.
See differential diagnosis tomorrow, as well as other processes.
Have a nice weekend.
Special mention to Genchi Bari: no more football until August!
….grande dr Pepe, come il grande BARCA !!!!!!
chondrosarcoma