Dr. Pepe’s Diploma Casebook: Case 78 – SOLVED!
Dear Friends,
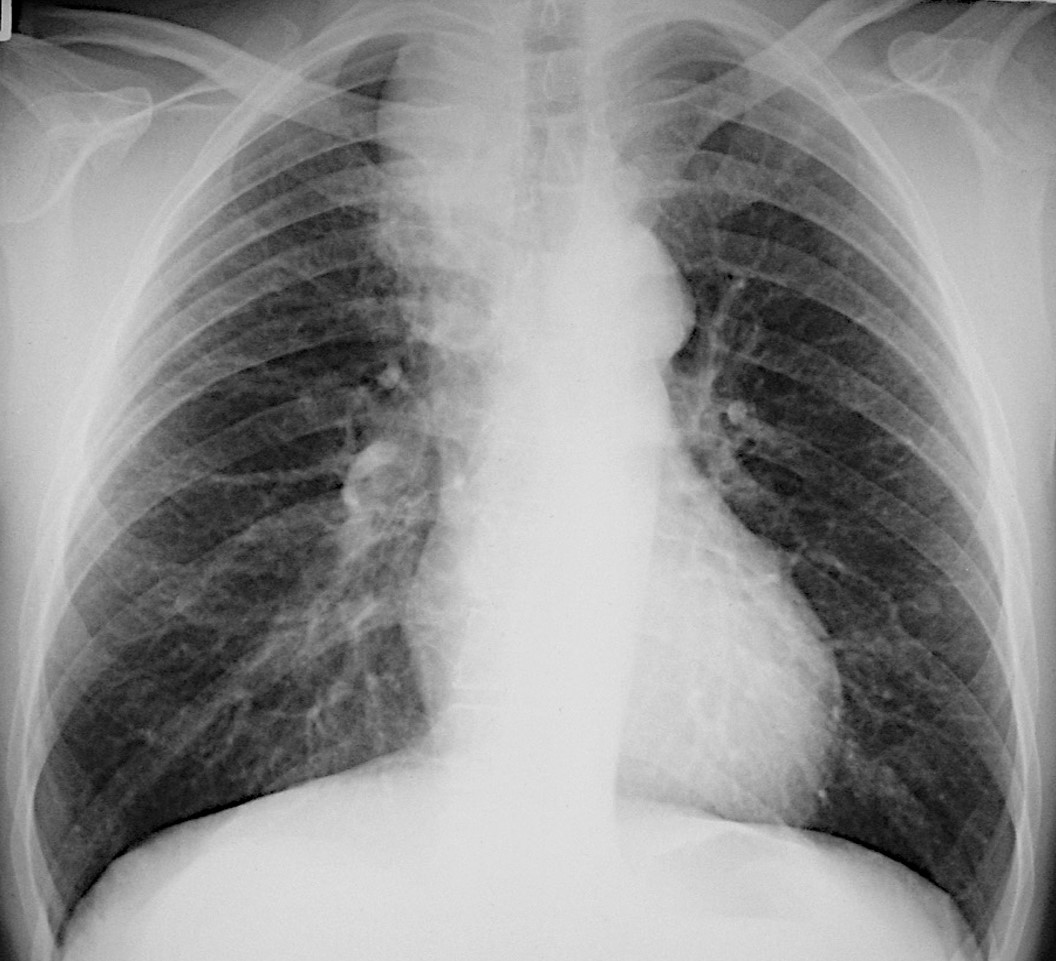
Today I’m showing a PA radiograph of a 49-year-old man with cough. Check out the image below, leave your thoughts and diagnosis in the comments section and come back on Friday for the answer.
Diagnosis:
1. Mediastinal lesion
2. Pulmonary lesion
3. Both
4. Can’t tell
Findings: PA radiograph shows a paramediastinal opacity in the upper lung (A, arrow) that is well defined superiorly and less so lower down, creating confusion about the origin of the opacity (mediastinum or lung). Axial CT demonstrates a pulmonary mass within an azygos lobe (B-C, arrows). The azygos fissure is responsible for the well-defined upper portion of the mass.
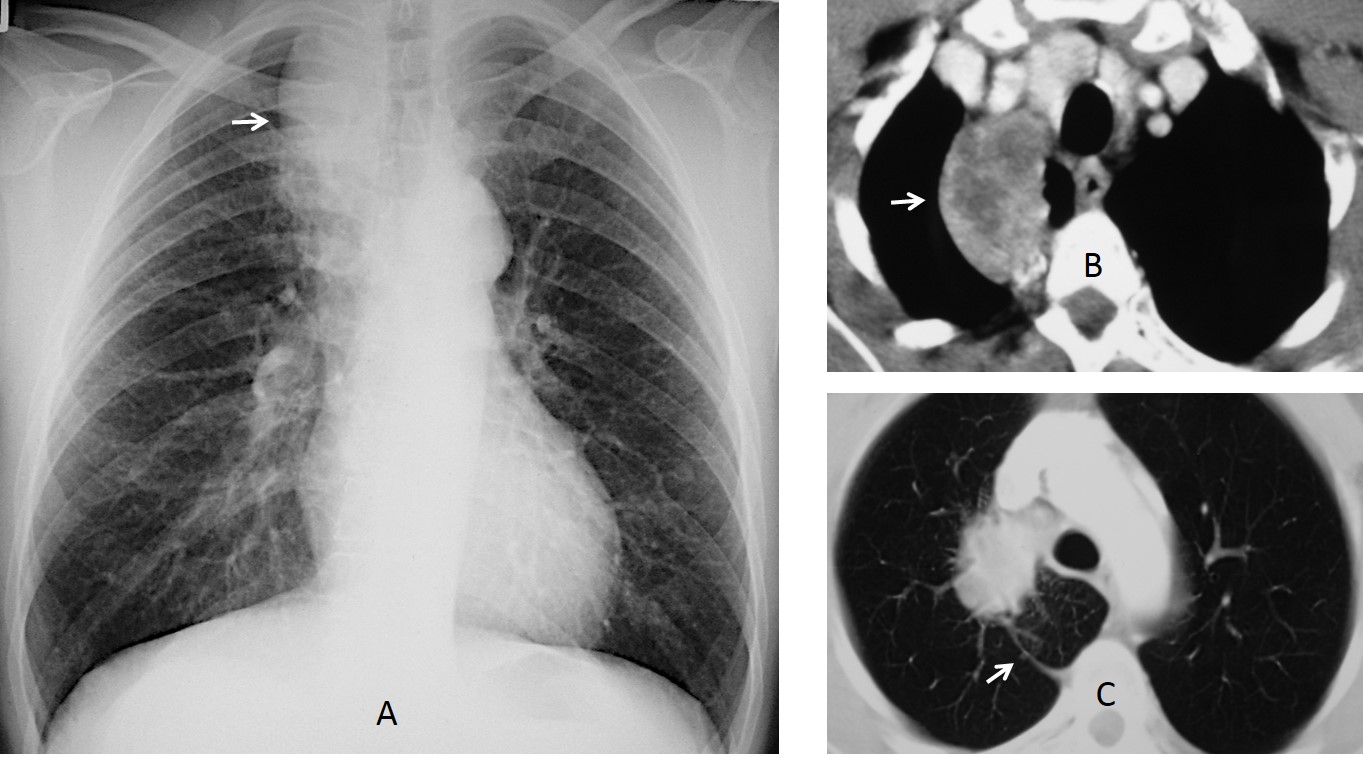
Final diagnosis: carcinoma of the lung within an azygos lobe.
The objective of this presentation is to discuss the azygos lobe, a normal variant that occurs when the azygos vein penetrates the lung, carrying along pleural layers that entrap a portion of the right upper lobe.
In about 0.4% of PA chest radiographs, the azygos lobe is seen as a fine convex line (azygos fissure) that crosses the apex of the right lung. The upper portion has a triangular shape (trigone) corresponding to areolar tissue between the pleural layers. The azygos vein appears as a pear-shaped shadow at the lowermost part of the fissure. On CT, the fissure is clearly visible as a convex line, and the vein is seen as a thicker structure following the same path (Fig. 1).
It is important to note that the enclosed lung is part of the RUL and not an independent segment.
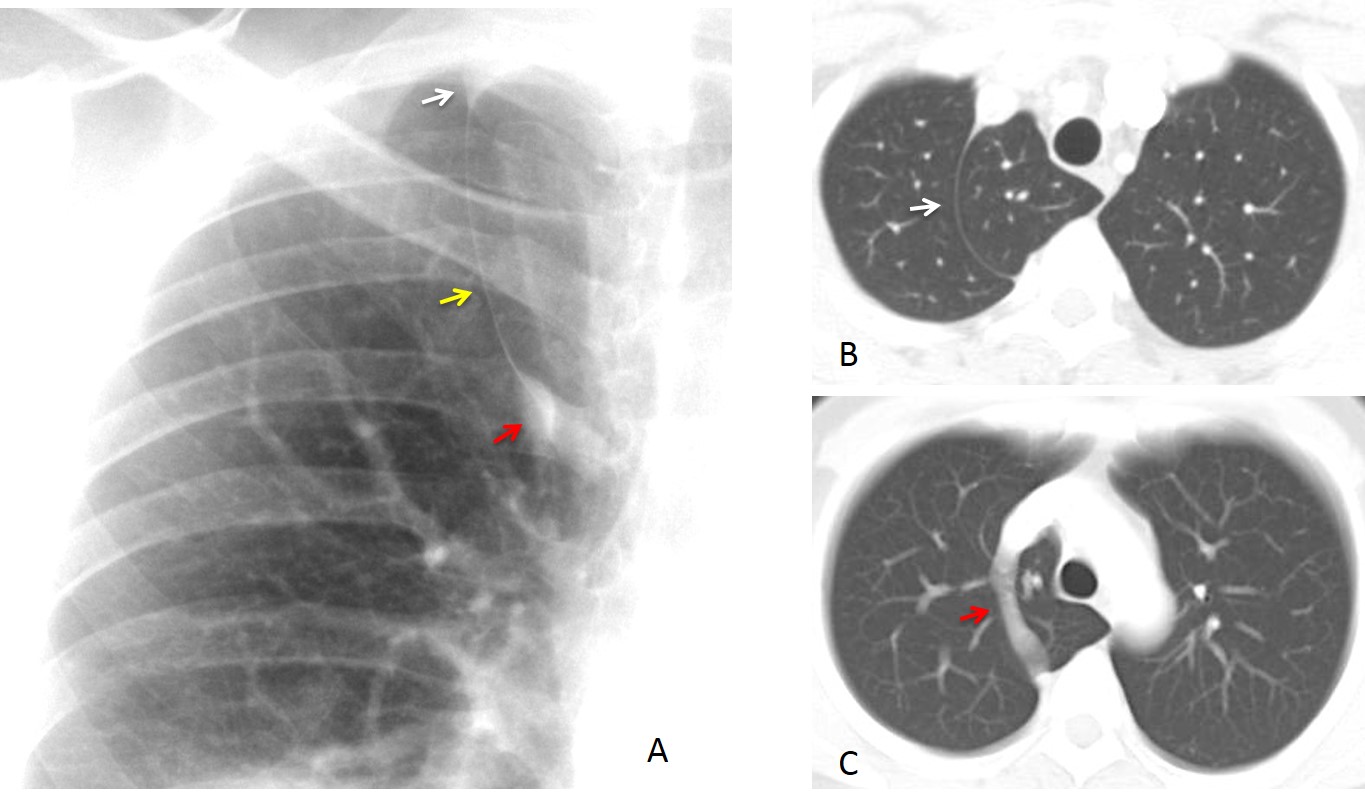
Fig. 1
Fig. 1: azygos lobe. PA radiograph shows the trigone (A, white arrow), the fissure (A, yellow arrow), and the vein (A, red arrow). Axial CT confirms the fissure (B, arrow), and a more caudal slice shows the vein as a thicker structure (C, arrow) draining into the SVC.
In most patients with this variant, the azygos lobe is detected as an incidental finding.
As in the remainder of the lung, the parenchyma within the azygos lobe may be affected by inflammatory or neoplastic disease. The azygos fissure acts as a barrier that can change the usual appearance of a pathology and make it simulate other conditions, as occurred in the case shown initially.
Pneumonia within an azygos lobe may be confused with RUL collapse because the azygos fissure mimics an elevated minor fissure (Fig. 2). The diagnosis is made by identifying the trigone and by noticing the lack of retraction of the right hilum.
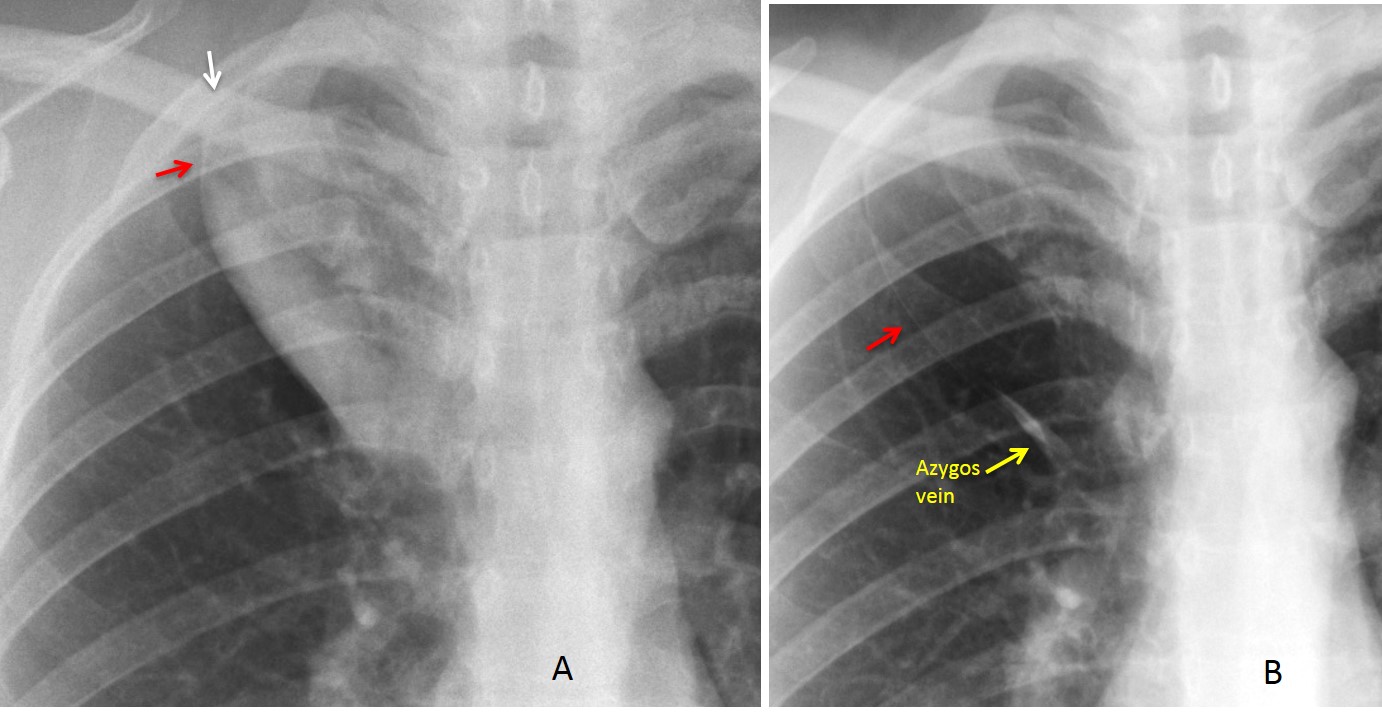
Fig. 2
Fig. 2: 28-year-old woman with pneumonia in an azygos lobe. The azygos fissure simulates an elevated, convex right middle fissure, leading to the erroneous diagnosis of RUL collapse. This mistake is avoided by recognising the trigone (A, arrow) and the superior portion of the fissure (A, red arrow). In addition, the trachea and right hilum are not retracted. The azygos lobe is clearly visible after healing has occurred (B, arrows).
The azygos fissure is a part of the pleural space. Pleural fluid may collect within the fissure, giving a bizarre appearance that should not be confused with other conditions. The appearance reverts to normal after the fluid disappears (Fig. 3).
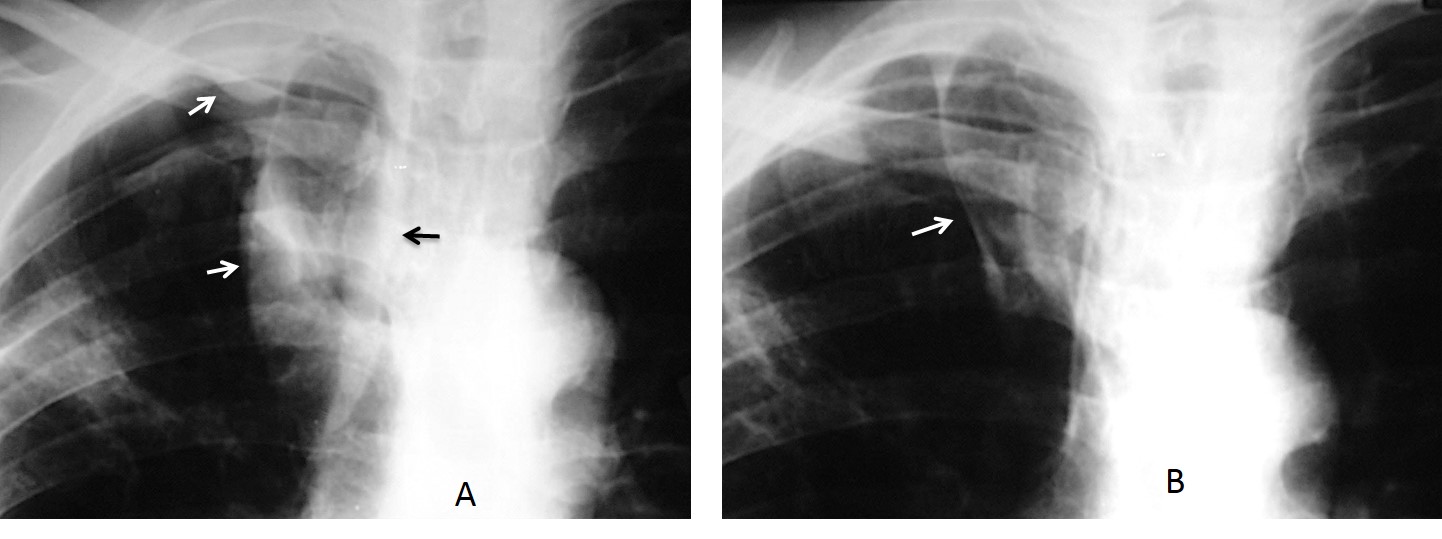
Fig. 3
Fig. 3: 56-year-old man with pneumonia and pleural effusion. In the initial film, the fluid has collected in the apex of the lung, azygos fissure, and paratracheal space (A, arrows). After treatment, the fluid has disappeared and the azygos lobe is now obvious (B, arrow).
An azygos lobe that is very large or very small may be mistaken for disease by the unaware (Fig. 4).
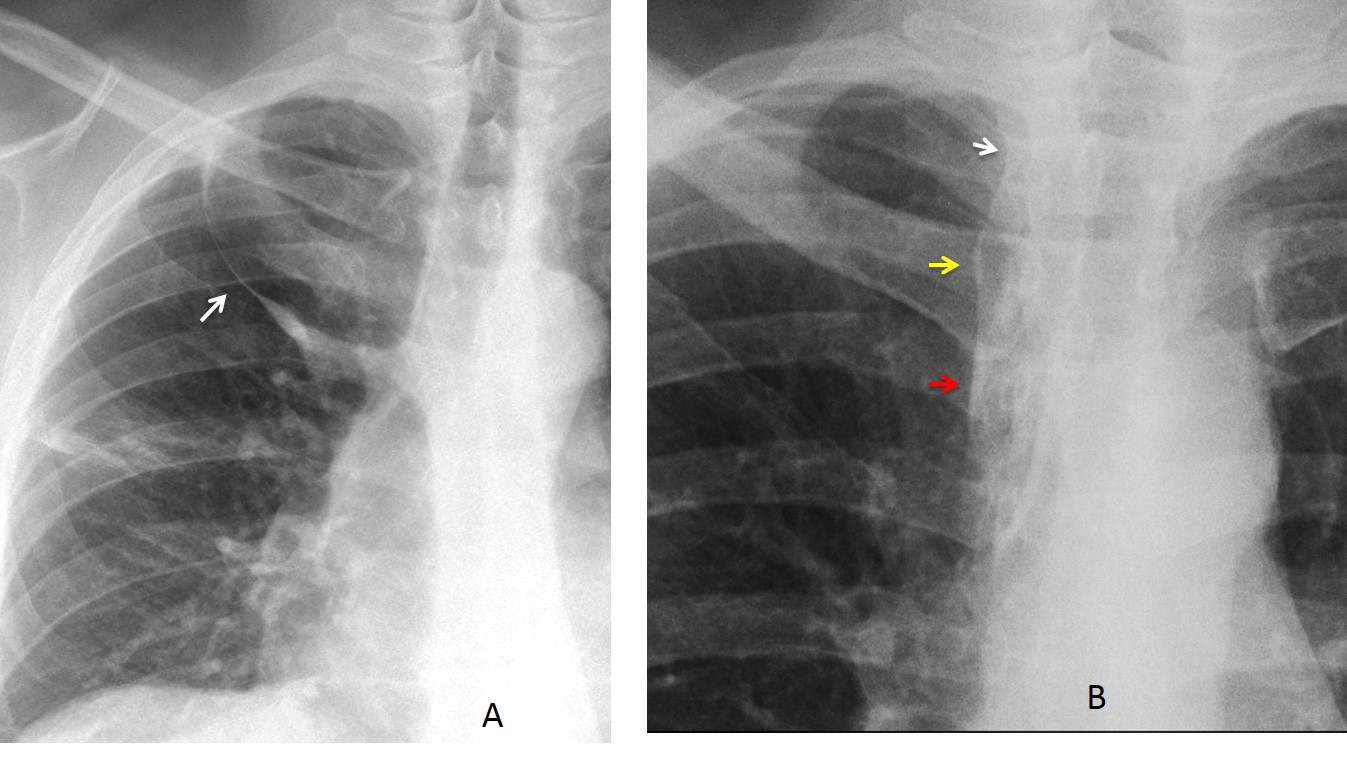
Fig. 4
Fig. 4: large azygos lobe that may be be confused with an upper lobe cavity (A, arrow). Small azygos lobe that can be identified as such by recognizing the trigone (B, white arrow), the fissure (B, yellow arrow) and the vein (B, red arrow).
A common variant known as opaque azygos lobe may simulate a mediastinal mass. It occurs in elderly persons and is caused by elongated supra-aortic vessels overlapping a shallow azygos lobe. The diagnosis is easy for those aware of this entity (Figs. 5 and 6).
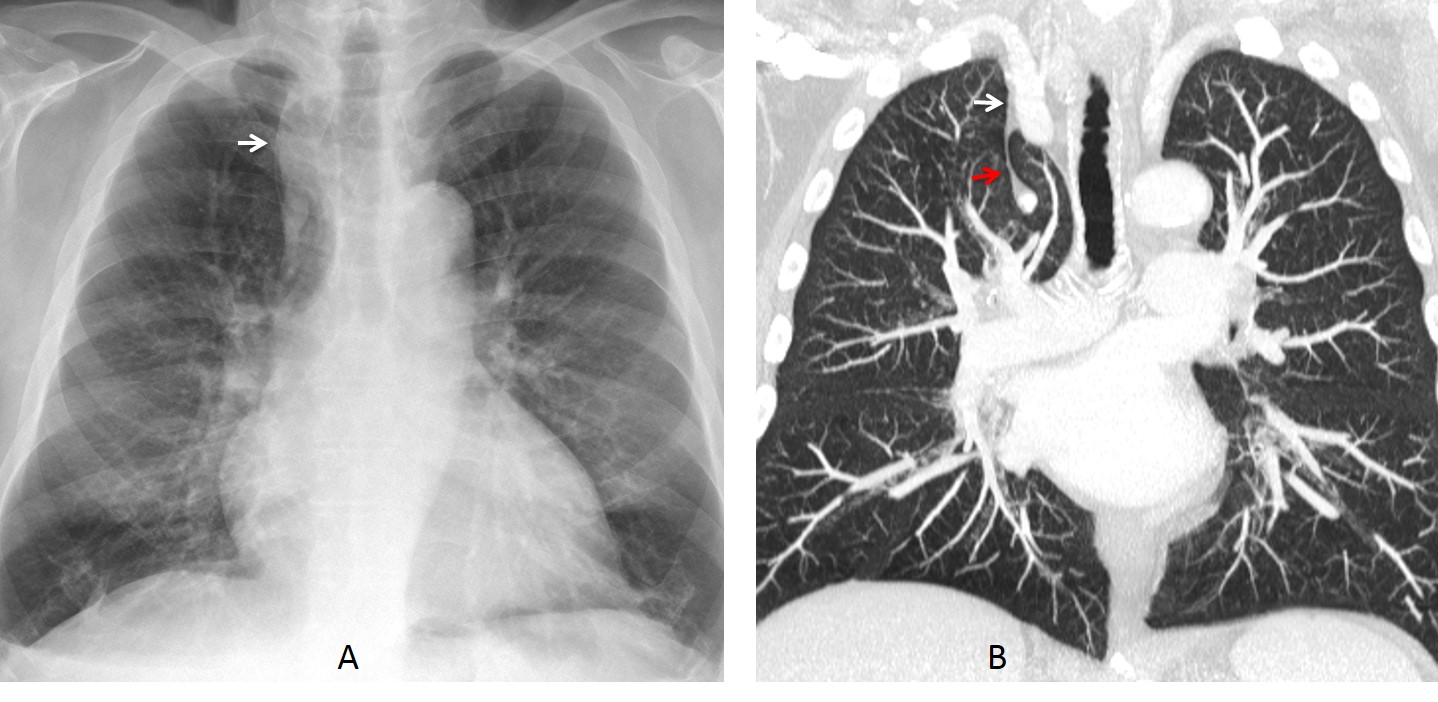
Fig. 5
Fig. 5. asymptomatic 67-year-old man with a suspected mediastinal mass on the PA radiograph (A, arrow). Coronal CT shows a small azygos lobe (A, red arrow) and dilated supra-aortic vessels (B, white arrow) as the origin of the opacity.
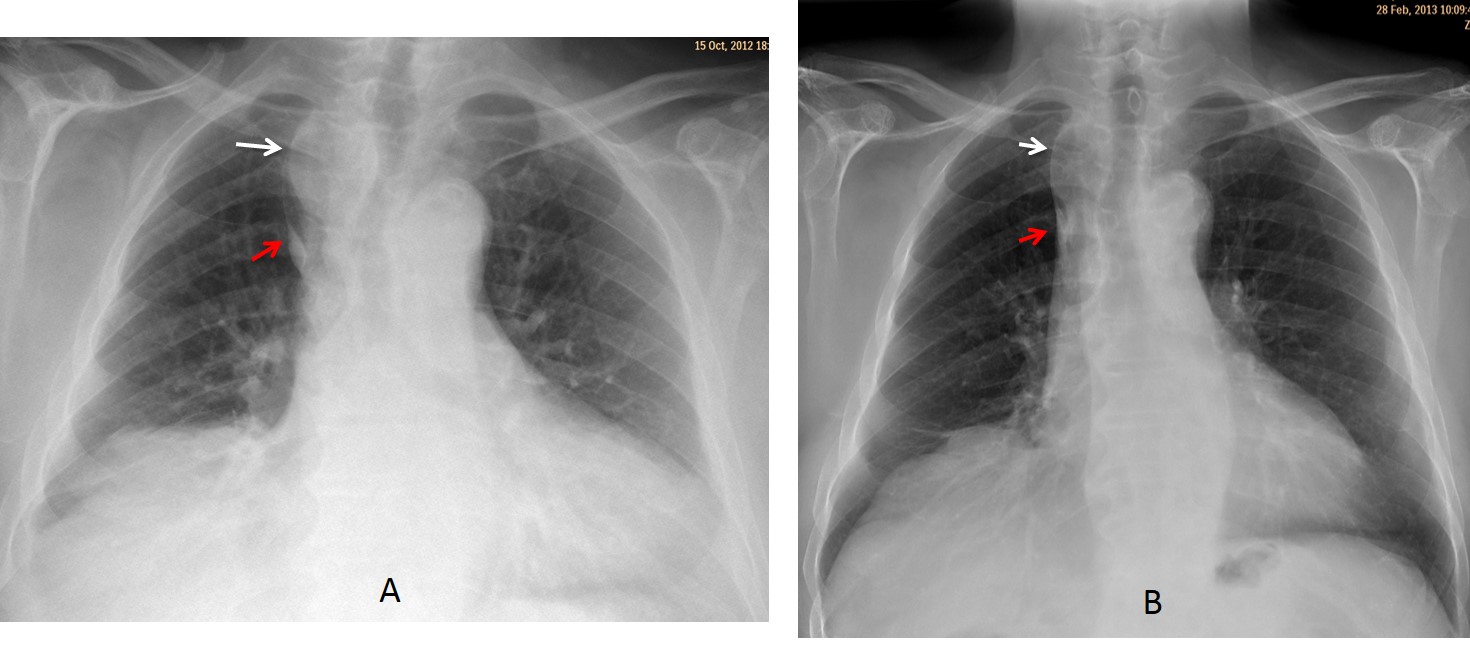
Fig. 6
Fig. 6: asymptomatic 72-year-old man with an azygos lobe (A, red arrow) and elongated vessels (A, white arrow), simulating a mediastinal mass. CT study was not deemed necessary. Six months later, the apparent mass has decreased in size and the appearance is more typical of an opaque azygos lobe (B, arrows).
Azygos continuation is a congenital anomaly in which the supra-renal portion of the IVC is missing and the blood drains into the azygos system. When this anomaly coincides with an azygos lobe, the dilated vein produces a bizarre appearance on chest radiography that should not be misinterpreted (Fig. 7).
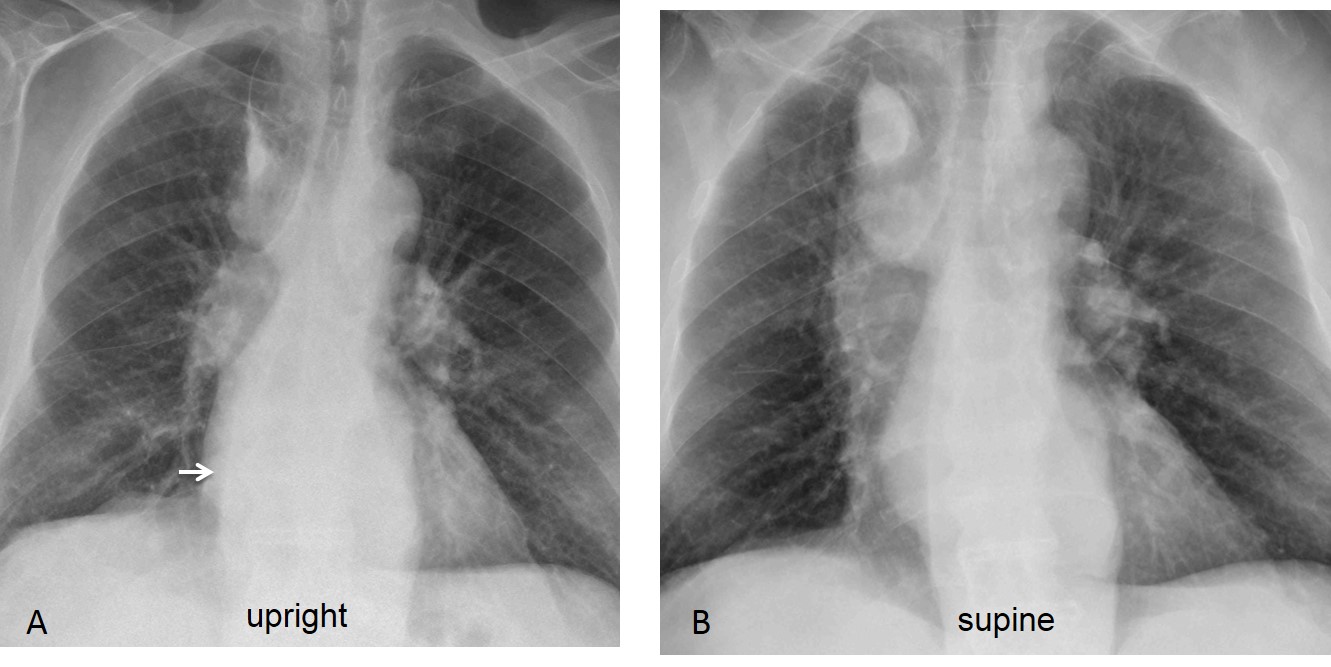
Fig. 7
Fig. 7: patient with liver cirrhosis, and azygos continuation of IVC plus azygos lobe. The upright chest film shows tortuous paraspinal lines (A, white arrows) and a large azygos vein (A, red arrow). The azygos vein markedly is increased in size in the supine view (B, red arrow).
Unenhanced coronal and sagittal CT images show marked dilatation of the azygos and hemiazygos veins (C and D, white arrows), as well as an enlarged azygos arch (C and D, red arrows).
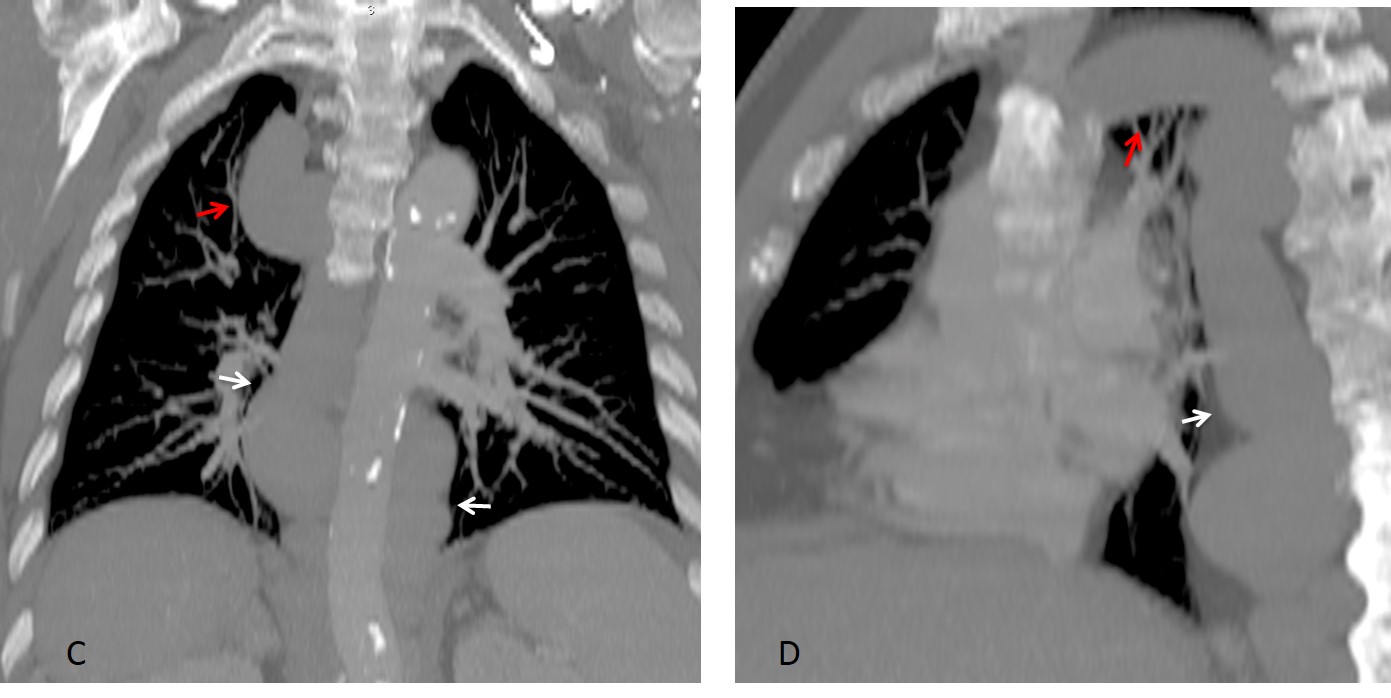
Fig. 7
Enhanced axial CT shows the enlarged azygos vein within the fissure (E, arrow). Coronal view of the abdomen demonstrates the IVC interruption at the level of the renal veins (F, arrow).
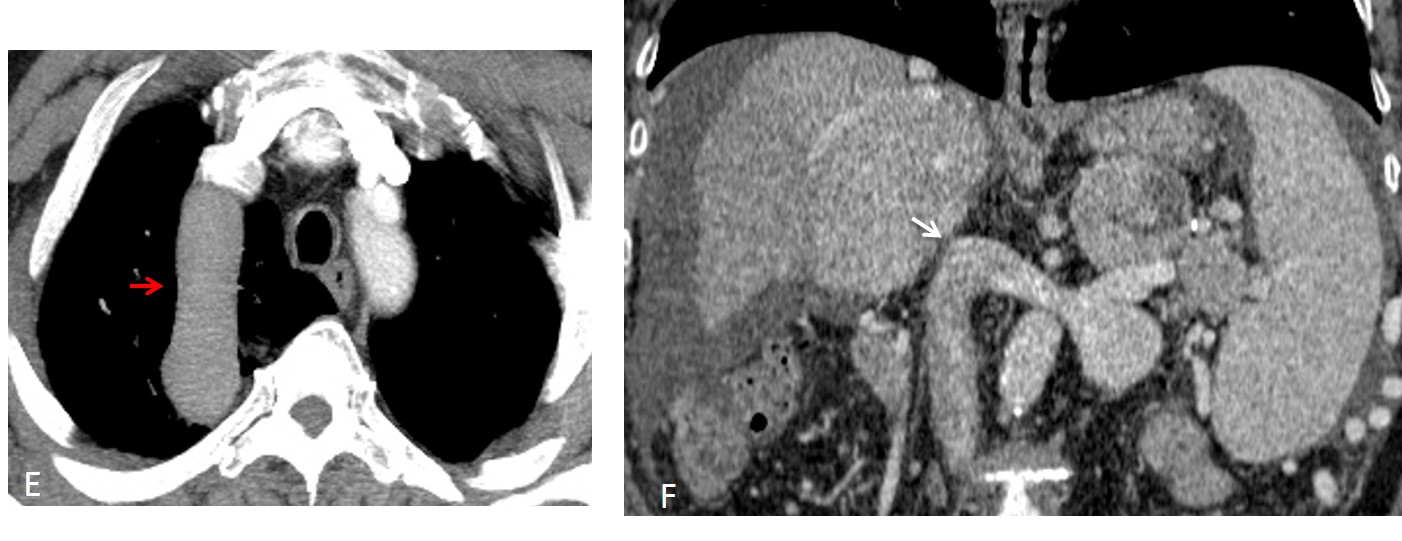
Fig. 7
Jumping azygos vein occurs when the vein formerly located in the fissure “jumps” and migrates to a paramediastinal location. The displacement is likely the result of a combination of factors: a shallow lobe, a previous pneumothorax that loosened the vein within the fissure, and episodes of cough and/or vomiting that pop the vein out like a watermelon seed squeezed between the fingers (Figs. 8 and 9).
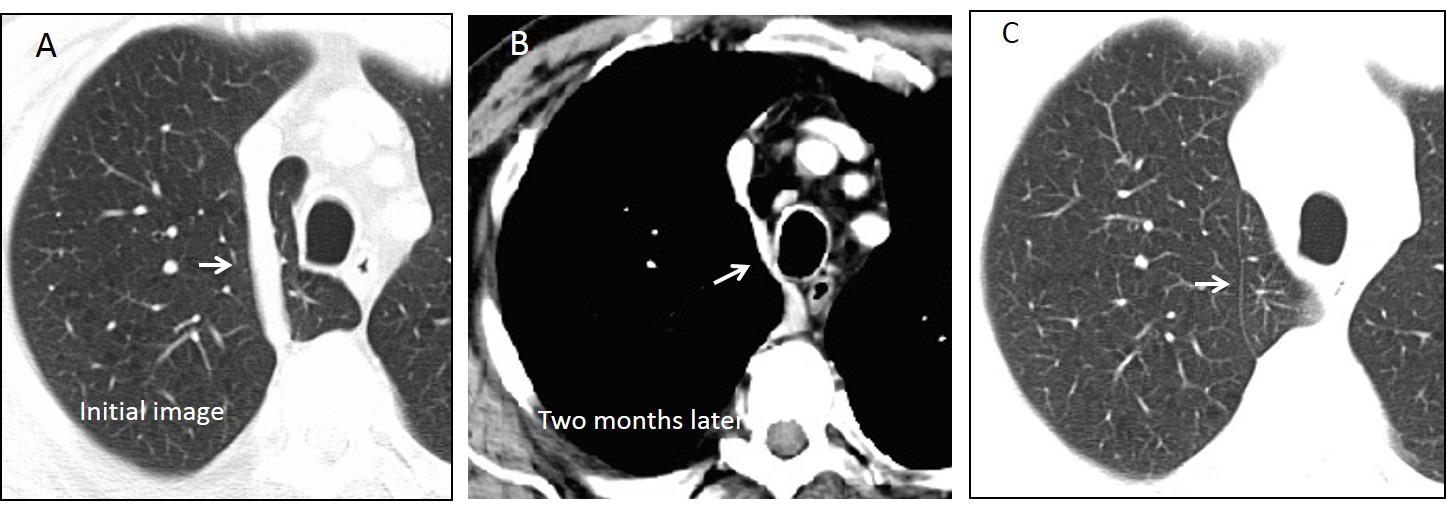
Fig. 8
Fig. 8: Good example of jumping azygos vein. Initial axial CT shows the vein within the azygos lobe (A, arrow). Two months later, the vein occupies a paramediastinal location (B, arrow) and the azygos fissure remains (C, arrow). The patient had a previous pneumothorax and had experienced episodes of forceful vomiting in the interval.
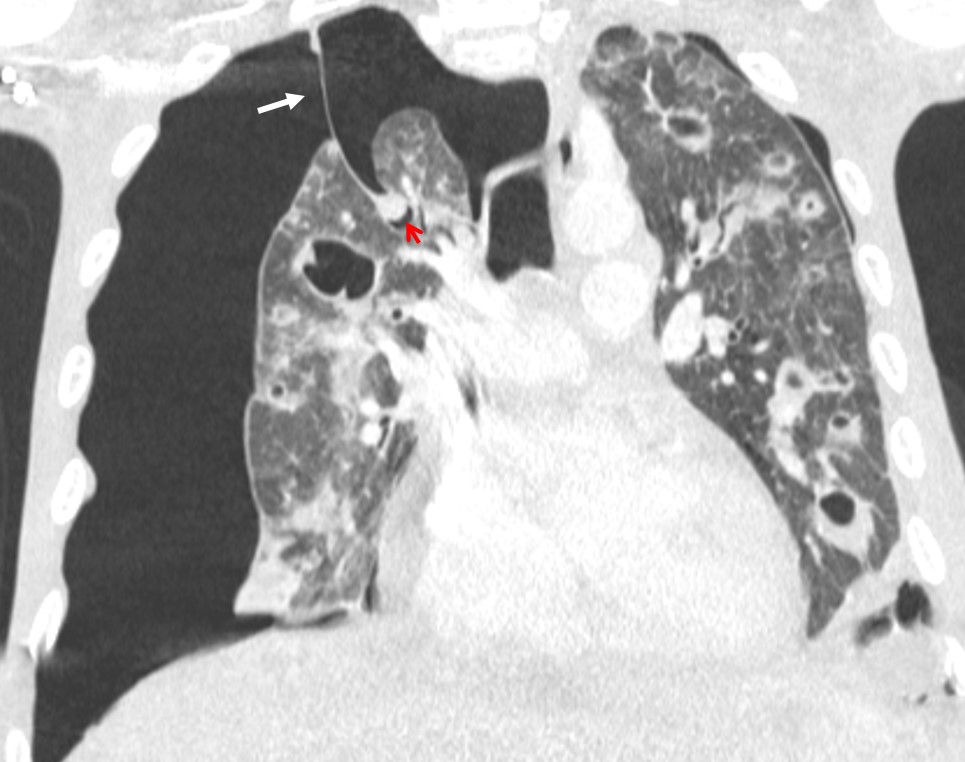
Fig. 9
Fig. 9: 35-year-old man with septic emboli and a pneumothorax. Coronal CT shows the azygos fissure (white arrow) and the azygos vein (red arrow) floating within the pleural space. It is easy to see how an episode of cough or vomiting could dislodge the vein and place it in the mediastinum.
Follow Dr.Pepe’s Advice:
1. Imaging manifestations of lung conditions may be distorted when they occur within an azygos lobe.
2. An opaque azygos lobe should not be confused with mediastinal pathology.
3. A jumping azygos may occur when a pneumothorax and forceful vomiting coexist.


A right paramediastinal soft tissue shadow extends above the superior clavicle, positive cervicothoracic sign (lung tissue comes between the mass and the neck).
It is mostly a mass in the posterior mediastinum.
1
…la massa può essere di pertinenza sia del segmento apicale lobo superiore sia del mediastino(risposta è 2 )….nello specifico essa dimostra dislocazione a sx della colonna tracheale nonchè sembra estendersi sul cappuccio aortico….diagnosi finale più probabile linfoma….Saluti da Bari….
…prego corrige: la risposta , in base a quanto dscritto è 3….entrambe(apice polmonare-mediastino)
Hello,
I think lesion is mediastinal. There is pregnancy sign – surface is smooth, one angle is obtuse, second isn’t but it’s localise in apex.
Moreover as was mentioned there is positive cervico-thoracic sign so we could precise location to posterior compartment of mediastinum. Trachea isn’t impacted what also confirms that sugestion.
Posterior mediastinal mass
A right mediastinal soft tissue density is mostly homogenous, but below 1st rib it looks a little inhomogenous. So I think there is two lesions- both pulmonary and mediastinal…
Chest X-ray of a 49 year old man presenting with couch of unknown duration shows a nearly elliptical non-calcific homogenous opacity along the right tracheal border at the thoracic inlet. Lower neck is not photographed and therefore it’s uncertain if it continues with the root of the neck. The lesion forms obtuse angle with the right lung apex and it’s therefore an extrapulmonary lesion. Trachea is neither deformed nor displaced and no convicing evidence of remodelling of adjacent ribs. The lesion most likely originates from the superior mediastinum with nerve sheet tumour( shcwannoma) a major differential. Intrathoracic goitre is also a consideration if the lesion continues with the root of the neck.
Opaque azigos lobe.
Bibliography:
Increased density of the azygos lobe on frontal chest radiographs simulating disease: CT findings in seven patients.
J Cáceres, J M Mata, X Alegret, J Palmer, and T Franquet
American Journal of Roentgenology 1993 160:2, 245-248
You did your research! But remember that the opaque azygos lobe occurs in older people because it is caused by elongation of supra-aortic vessels.
Still, I believe congratulations are in order.
1. Mediastinal mass
What about lungs changes? Are there any small nodules with random distribution in both lungs? . This kind of changes are present in hematogenous metastases, tbc, in some cases of sarcoidosis.
Tbc with paravertebral abscess? Too far from KISS rule?
A little too far. And the KISS rule would specify bilateral widening in a vertebral abscess
I would say 2
It seems to me inside the opacity in the right upper zone there are some tubular branching lucencies that could be readed as bronchogram so lesion would be a lung lesion. The outer sharp outline could be explained by an azygous fissure. A consolidation inside an azygous lobe would fit with this image.
A well-reasoned answer. But Dr Pedro was ahead of you by 24 h.
Right upper mediastinal mass.
Is there an opacity just below the medial end of the left clavicle?
CT didn’t show any opacity under the medial end of left clavicle.
4. Can´t tell
Probably, an opacified azygos lobe
Dear friends this is the last case of the first semester, Will see you again in September.
Explanation of the findings tomorrow. Congratulations to Dr. Pedro, who was the first to post the correct answer.
Have a nice summer!
Thanks/Hvala! 🙂
Ste dobrodošli!
c both
1. Mediastinal lesion