Dr. Pepe’s Diploma Casebook: Case 82 – SOLVED!
Dear Friends,
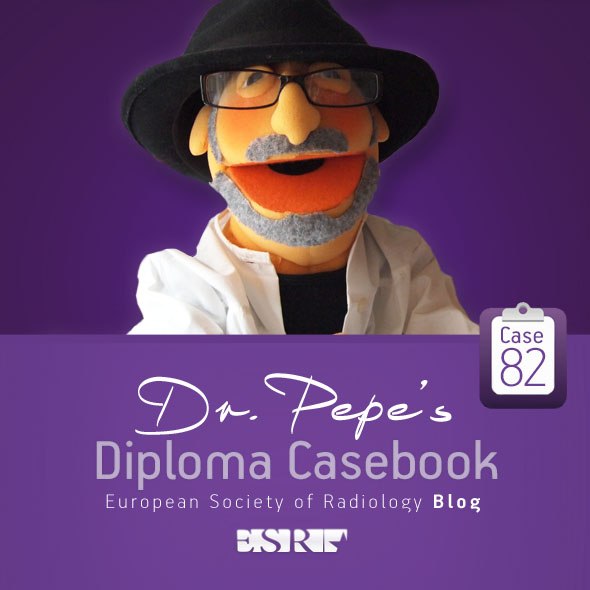
Today’s images belong to a 35-year-old man with chest pain. What do you see?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.

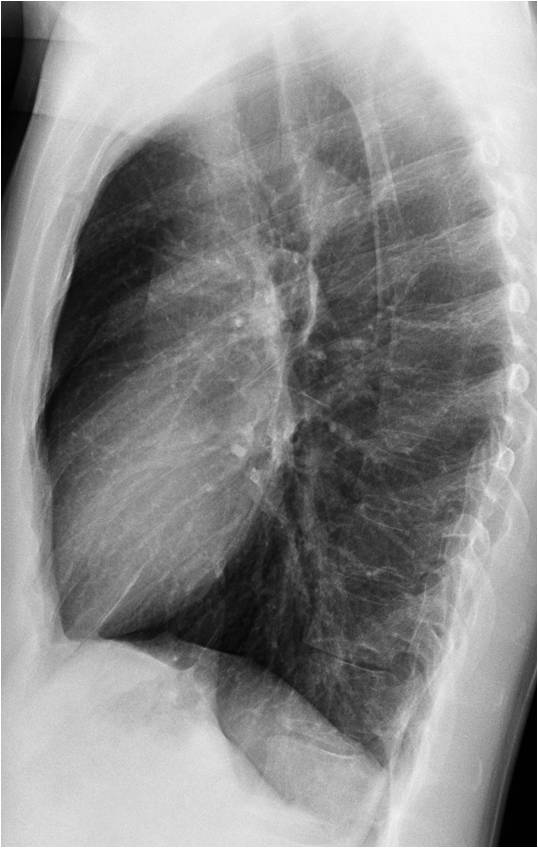
Findings: PA radiograph shows a horizontal line at the right costophrenic angle (A, arrow).
This line represents a small amount of pleural fluid and is very suggestive of an accompanying pneumothorax. Looking at the upper lung, a small pneumothorax is found in the apical region (B, arrows).
Final diagnosis: spontaneous right pneumothorax
Pneumothorax is a common problem that is usually easy to identify in the chest radiograph. However, sometimes its appearance is not easily recognised and an incorrect diagnosis is made. In the following discussion I will present common and uncommon manifestations of pneumothorax in the erect chest radiograph, as well as the most frequent causes of this condition.
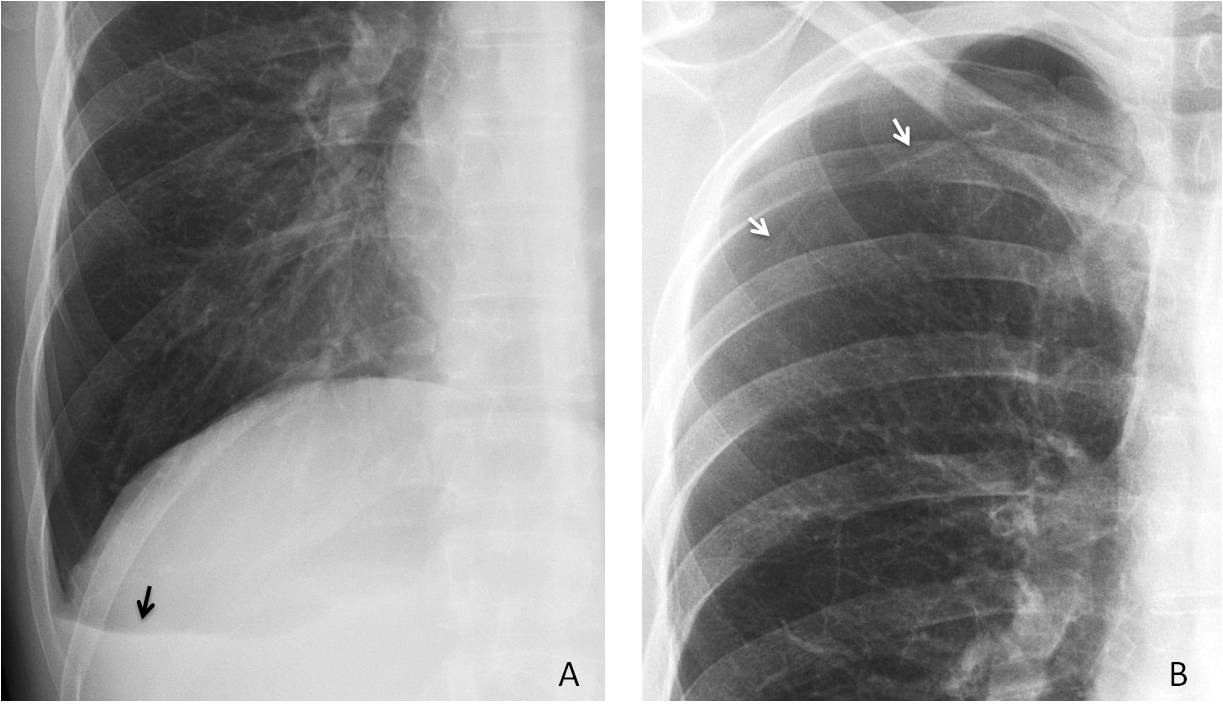
The erect PA radiograph is by far the best view to identify pneumothorax, which is seen as a thin curved line separating the lung from the darker avascular pleural space (Fig. 1 A). In case of doubt, an expiration film increases the dark pleural space, making the pneumothorax more obvious (Fig. 1 B).
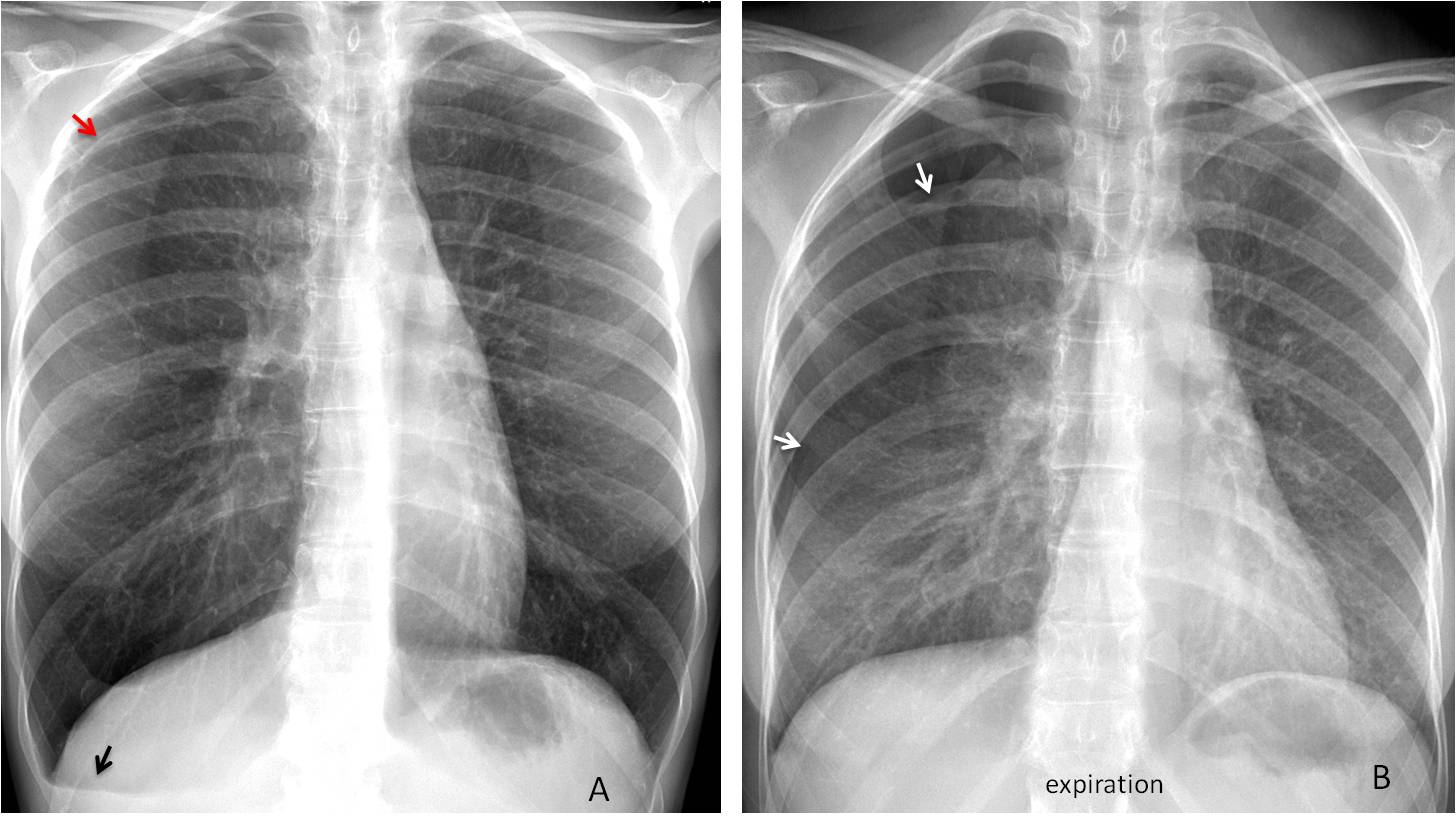
Fig. 1
Fig. 1: 43-year-old woman with recurrent catamenial pneumothorax. The PA radiograph shows the line of the pneumothorax in the right apex (A, red arrow). Note the small effusion at the right costophrenic angle (A, black arrow). The expiration film better demonstrates the lung-pleura interface (B, arrows).
About 20% of pneumothoraces are associated with a small amount of pleural fluid that appears as a double horizontal line (V line) or, more commonly, as a single line in the costophrenic angle (Fig. 2). This is a helpful clue to suspecting pneumothorax when the classic findings are not obvious (Fig. 3).
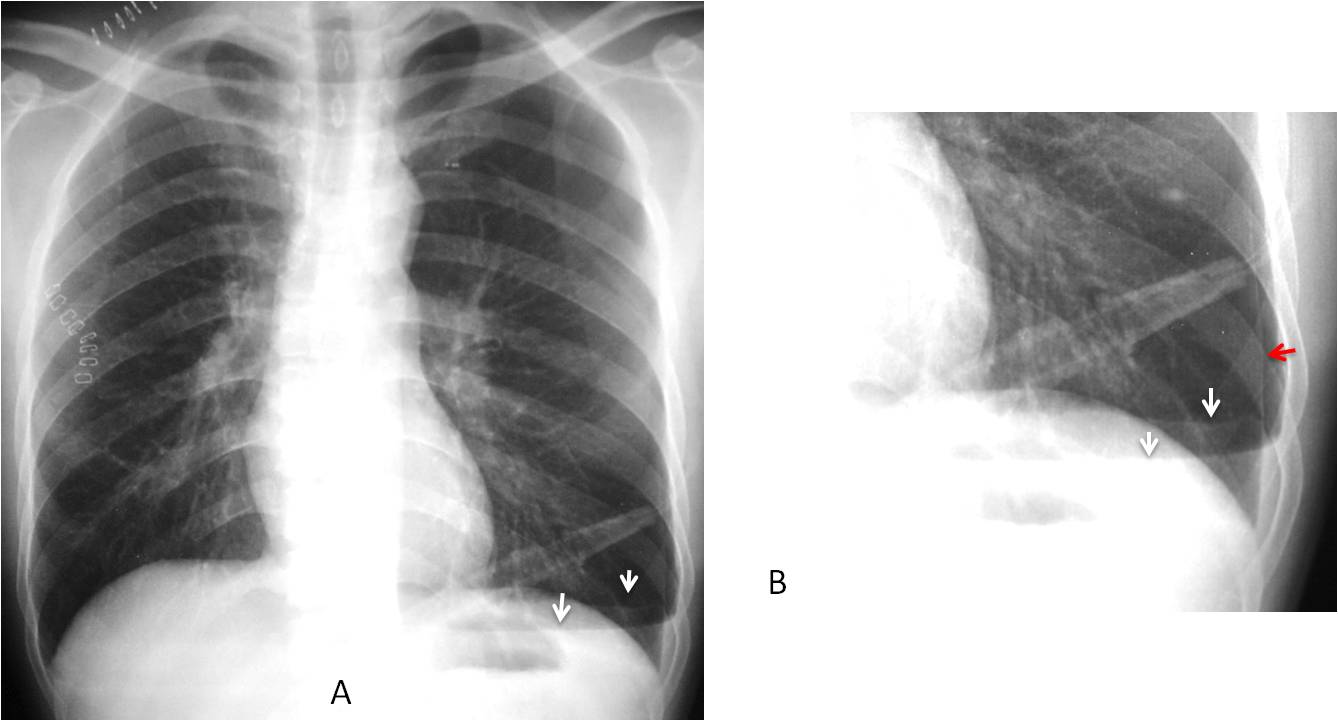
Fig. 2
Fig. 2: Postoperative pneumothorax. There is a V line at the left costophrenic angle (A, arrows), better seen in the cone down view (B, arrows), which also shows the lung-pleura interface (B, red arrow).
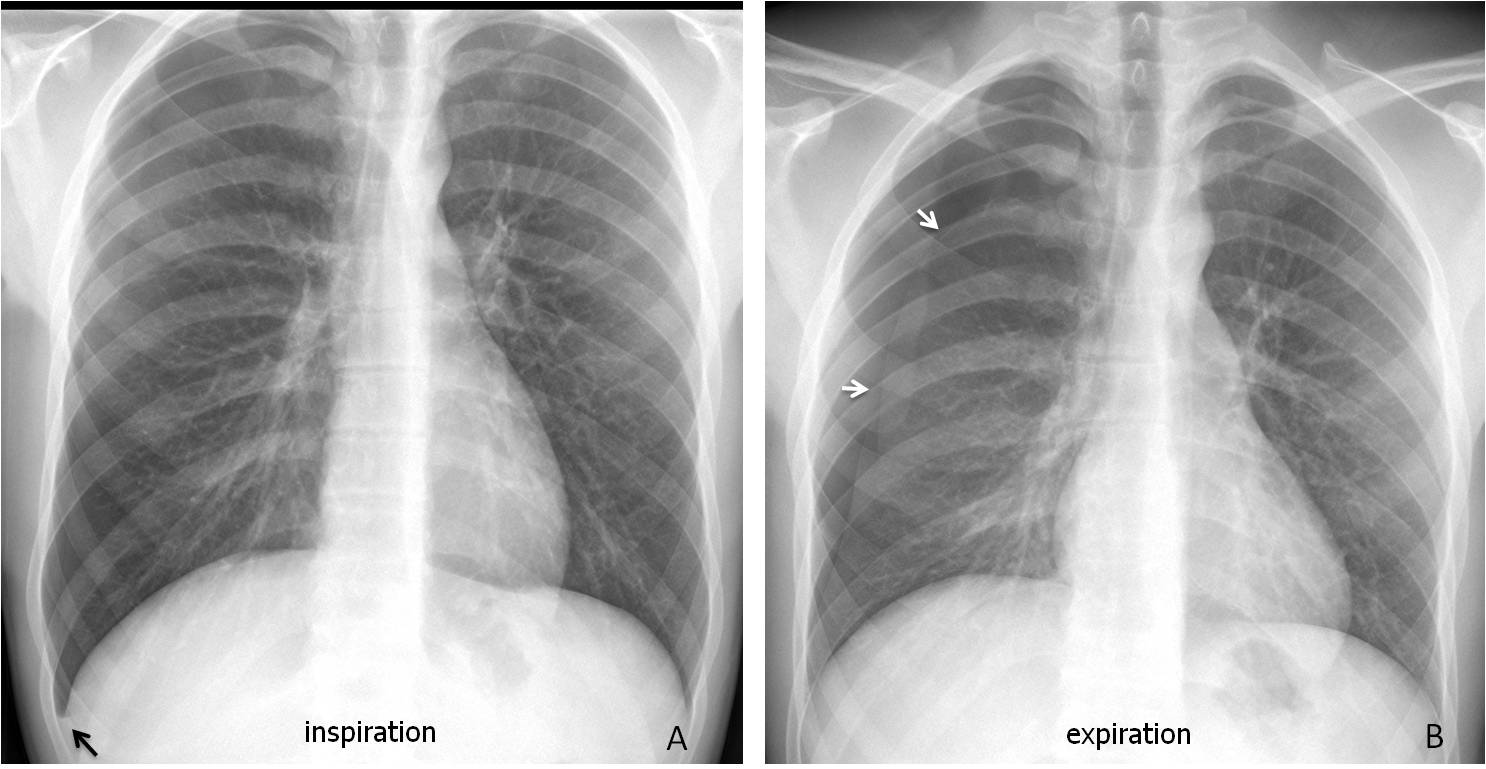
Fig. 3
Fig. 3: Young male with spontaneous pneumothorax. The inspiration film is not conclusive except for minimal blunting of the right costophrenic angle (A, arrow). The expiration film clearly demonstrates a pneumothorax (B, arrows). This is the smallest V line I have ever seen!
A large pneumothorax causes collapse of the whole lung. It is easy to recognise, unless you are a medical student who interprets the collapsed lung as a lung mass. Incidentally, in these cases the lateral view can be misleading (Fig. 4).
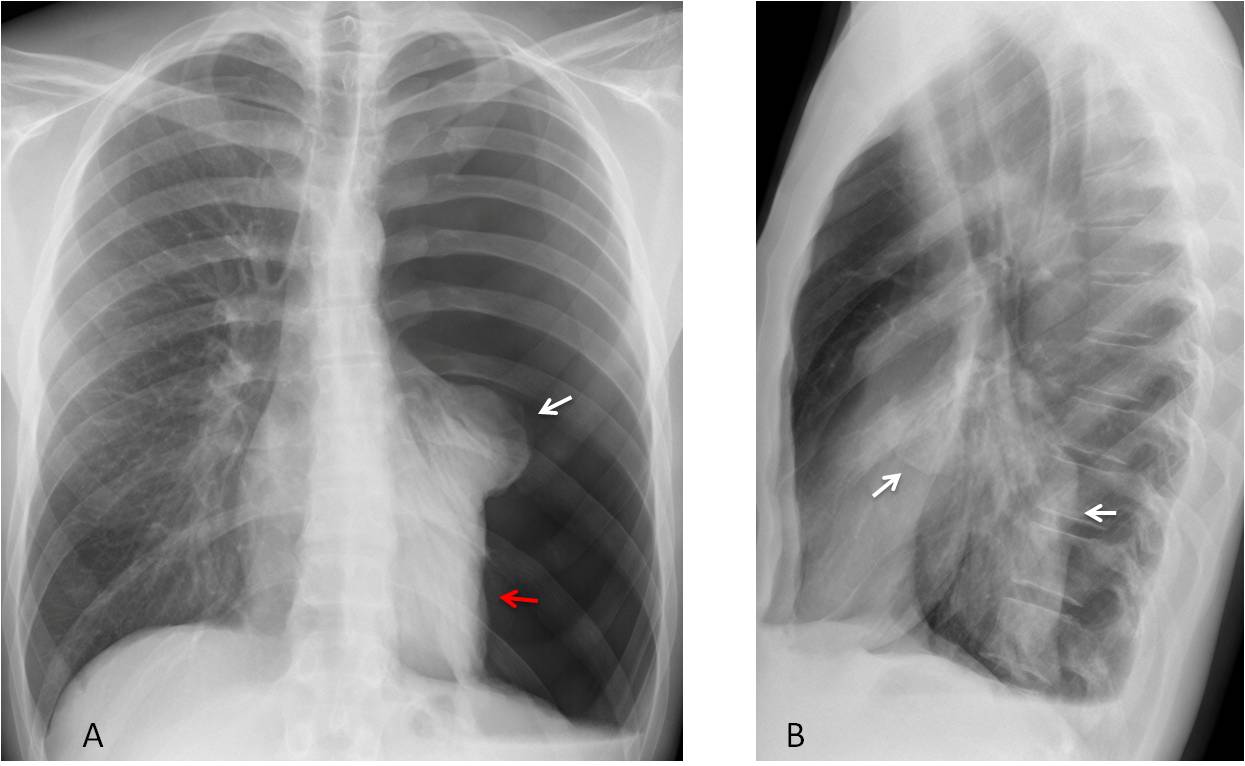
Fig. 4
Fig. 4: Total pneumothorax. The left upper lobe collapses downward (A, white arrow), whereas the lower lobe (A, red arrow) remains anchored to the mediastinum by the pulmonary ligament. The collapsed lobes present a bizarre appearance in the lateral view (B, arrows).
TIP: The complete lung collapse practically rules out any significant lung disease.
Tension pneumothorax occurs when a check-valve mechanism allows continuous influx of air into the pleural space. It should be suspected when there is mediastinal shift and depression of the hemidiaphragm (Fig. 5). It is important to recognise tension pneumothorax because it represents a medical emergency.
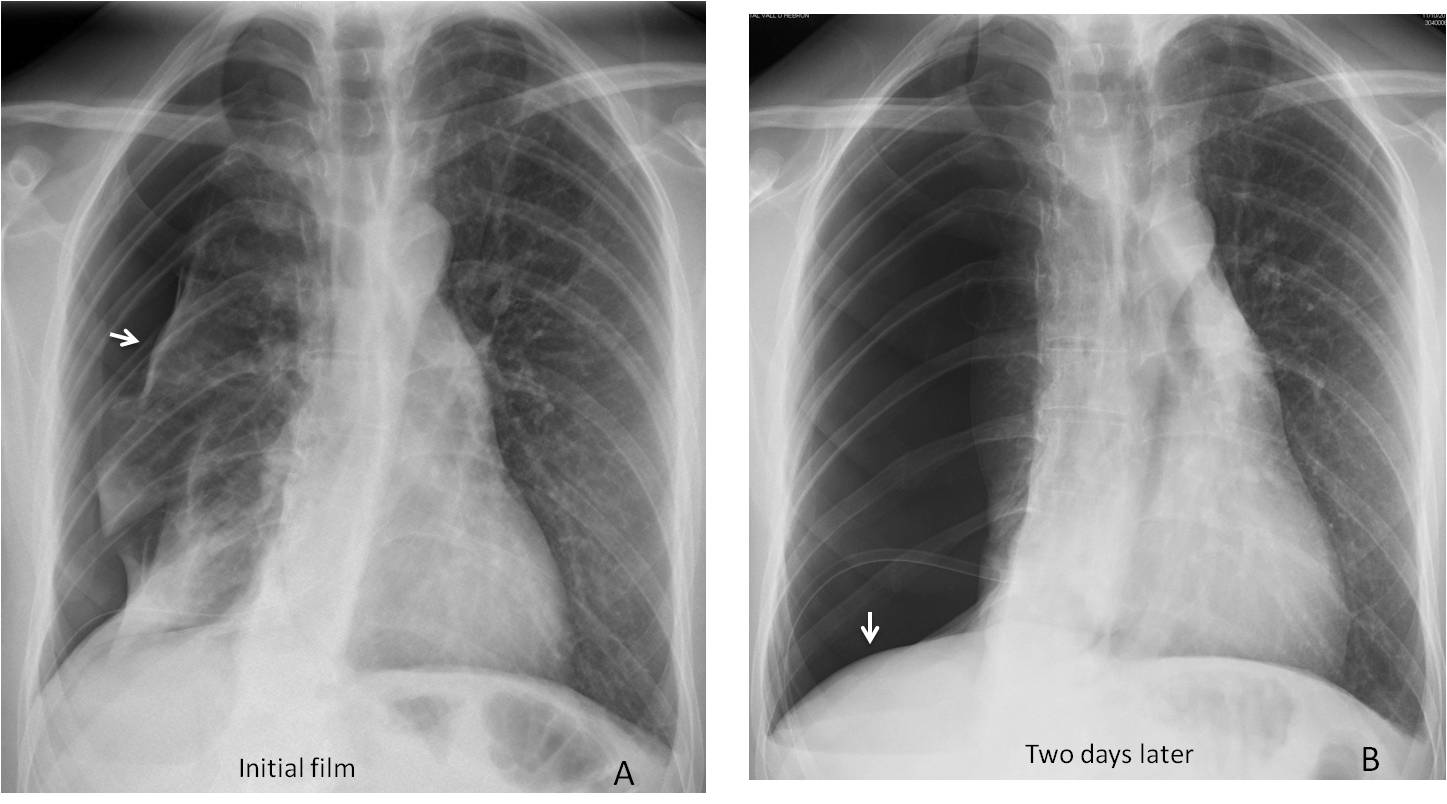
Fig. 5
Fig. 5: Tension pneumothorax after bronchoscopic biopsy. The initial film shows a moderate pneumothorax (A, arrow), which has increased two days later despite the chest tube. Note the mediastinal shift and depression of the hemidiaphragm (B, arrow).
Hydropneumothorax combines air and fluid in the pleural cavity, giving rise to an air-fluid level. The most common cause is iatrogenic, (drainage or surgery) (Fig. 6). If that’s not the case, postulate a connection with a mediastinal viscus (Fig. 7).
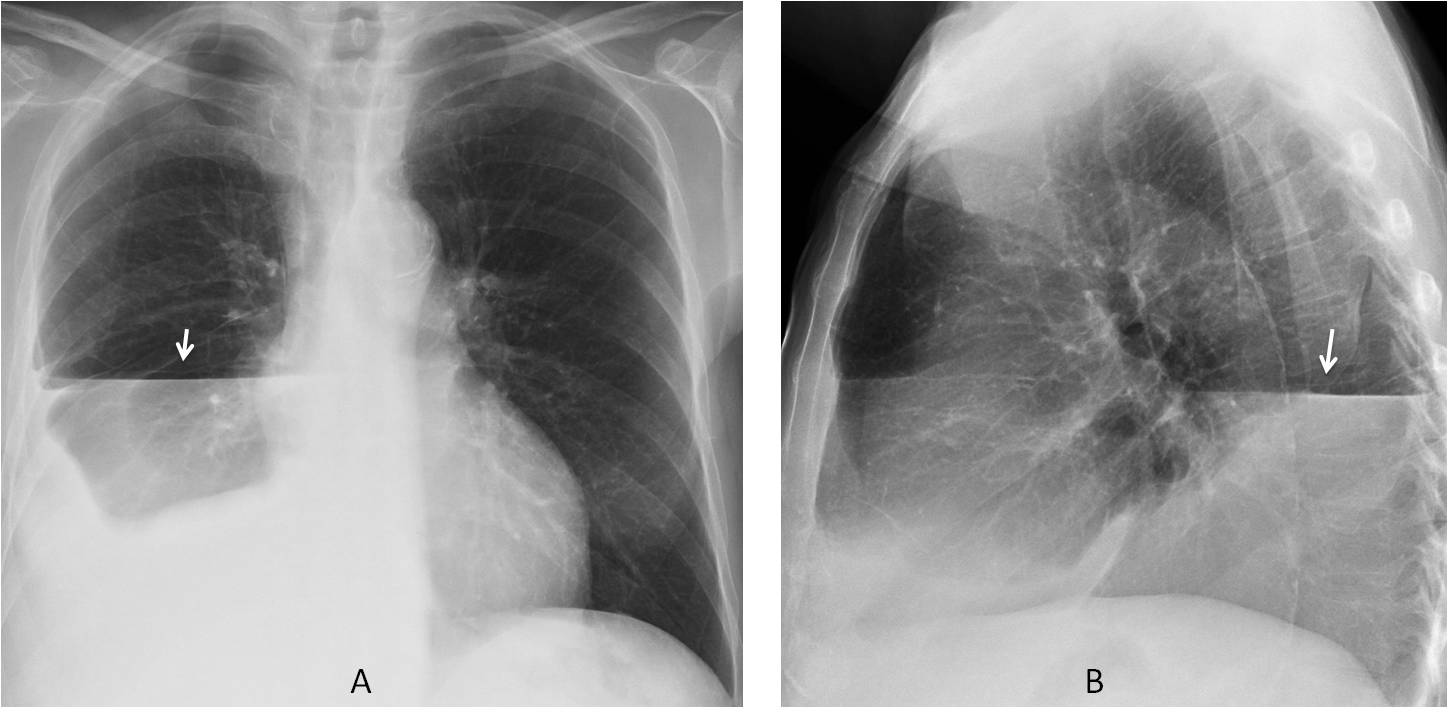
Fig. 6
Fig. 6: Hydropneumothorax after drainage of a large right pleural effusion. An obvious air-fluid level is visible in the PA and lateral films (A and B, arrows).
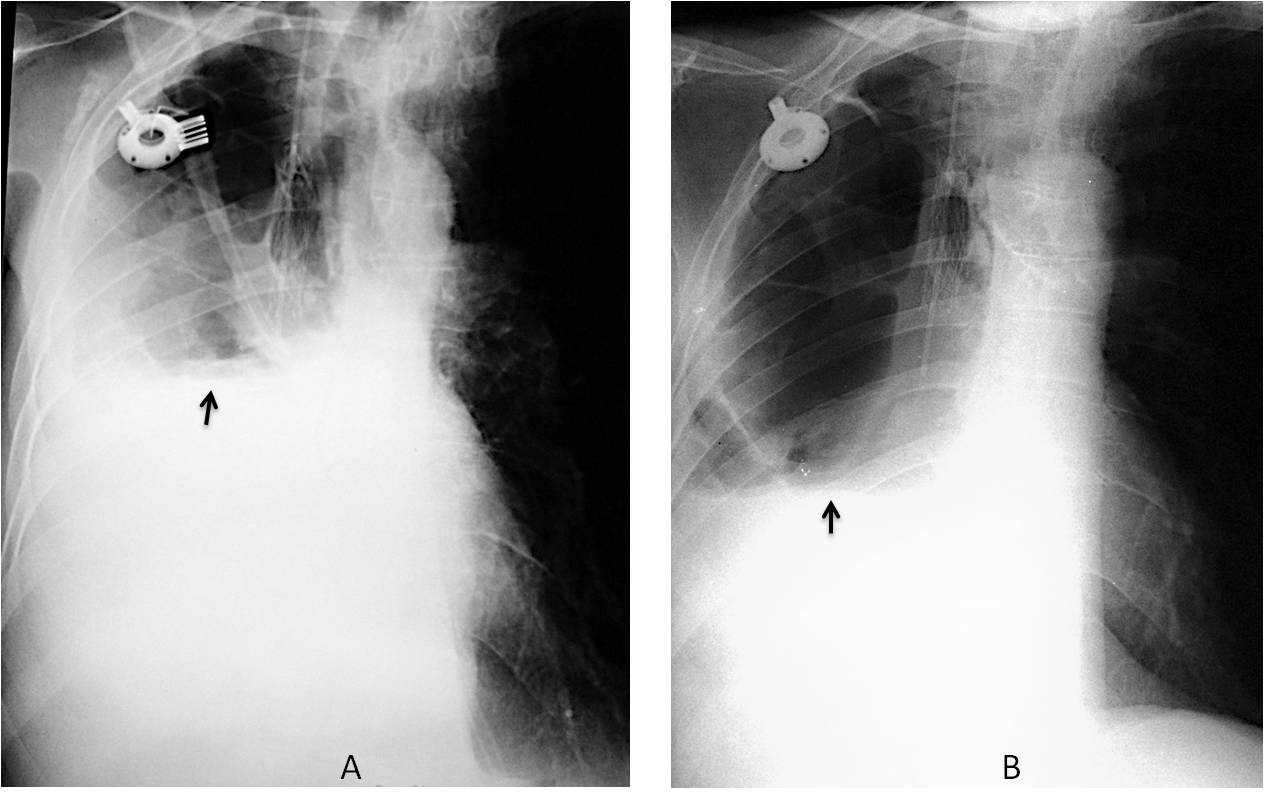
Fig. 7
Fig. 7. Hydropneumothorax after right upper lobe resection to treat carcinoma (A, arrow). One week later, the pleural air has increased and the air-fluid level has descended (B, arrow), indicating an air leak. The patient died and failure of the RUL stump ligature was found.
Pneumothorax can have an atypical appearance when there are pleural adhesions secondary to a previous infection or surgery. The adhesions change the typical appearance and should not be confused with pulmonary bullae or cysts (Fig. 8).

Fig. 8
Fig. 8: 54-year-old man with a pneumothorax after right lung transplantation. Pleural adhesions have modified the shape of the pneumothorax, simulating two cystic structures (A, arrows). The lung-pleura interface is evident in the lateral view (B, arrow).
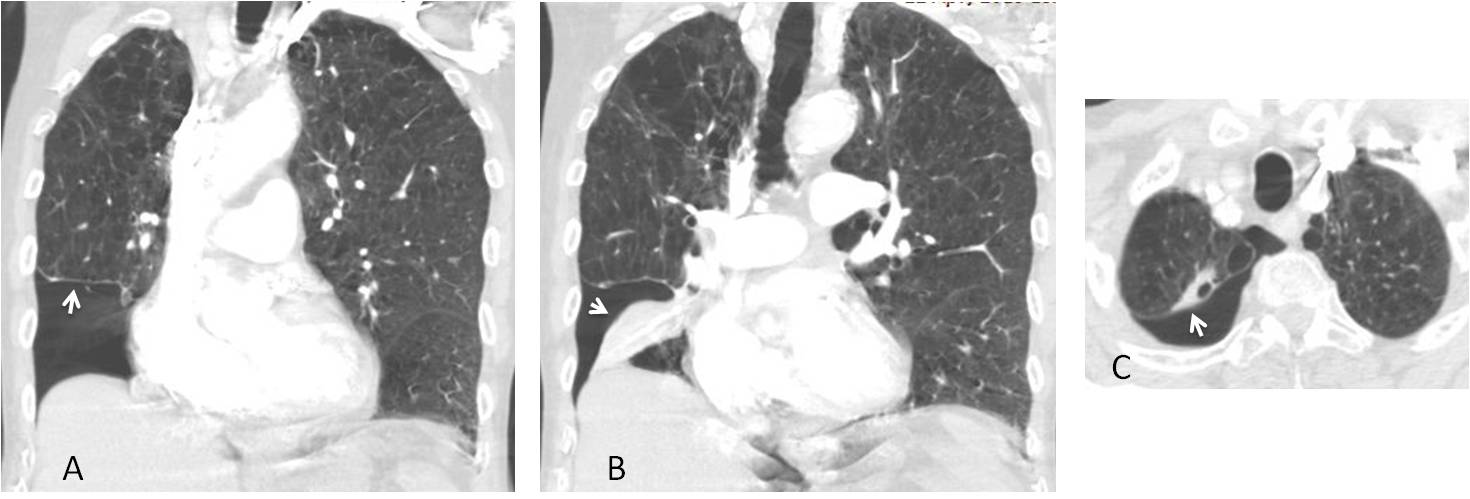
Lobar collapse causes a local increase of retraction forces, resulting in an atypical location of pleural air, when present (Fig. 9). When this occurs in the lower lung, it is called subpulmonary pneumothorax (Fig. 10).
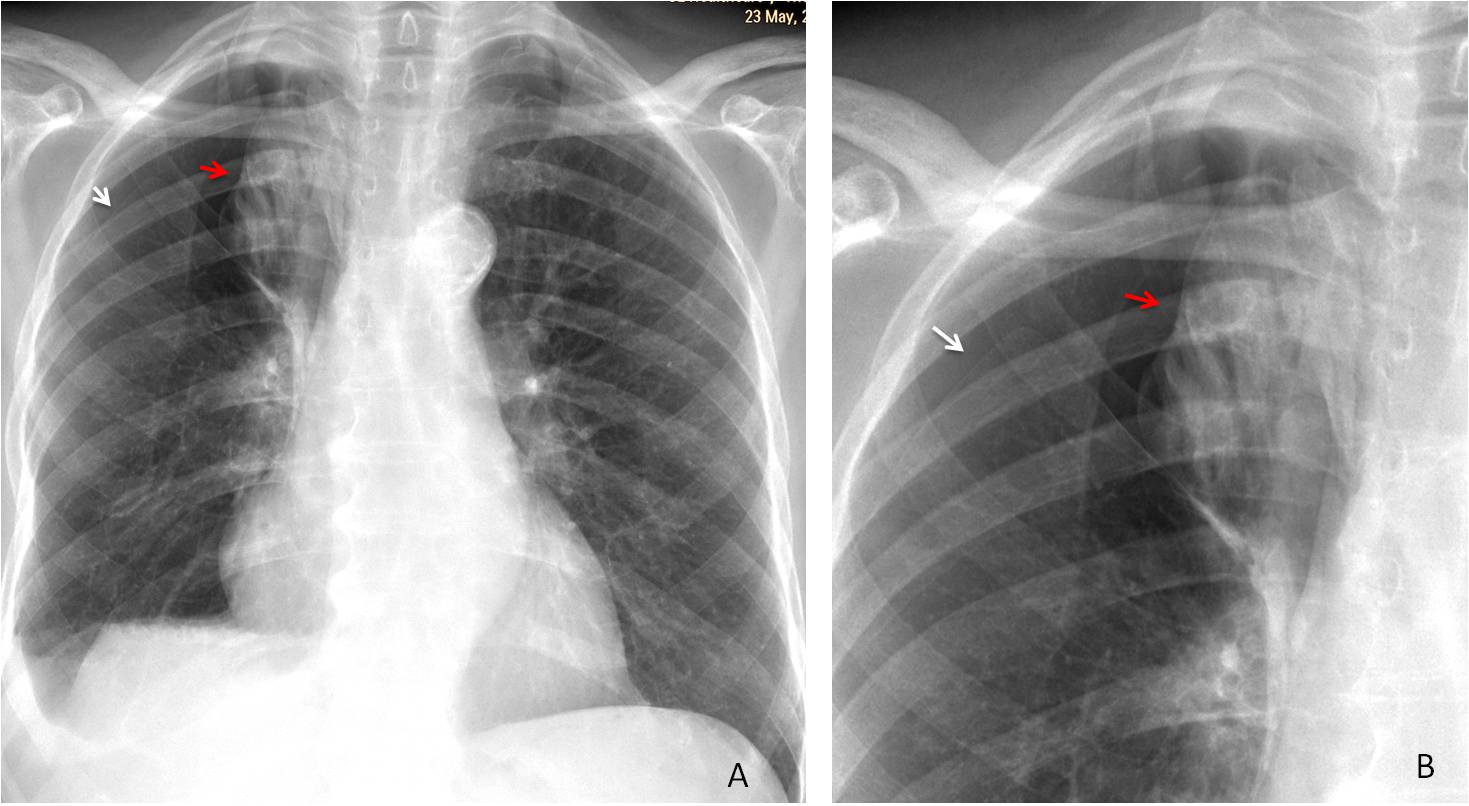
Fig. 9
Fig. 9: Carcinoma with RUL collapse (A and B, red arrows). Pneumothorax after percutaneous biopsy is confined to the upper region (A, white arrow) and is better seen in the cone down view (B, white arrow).
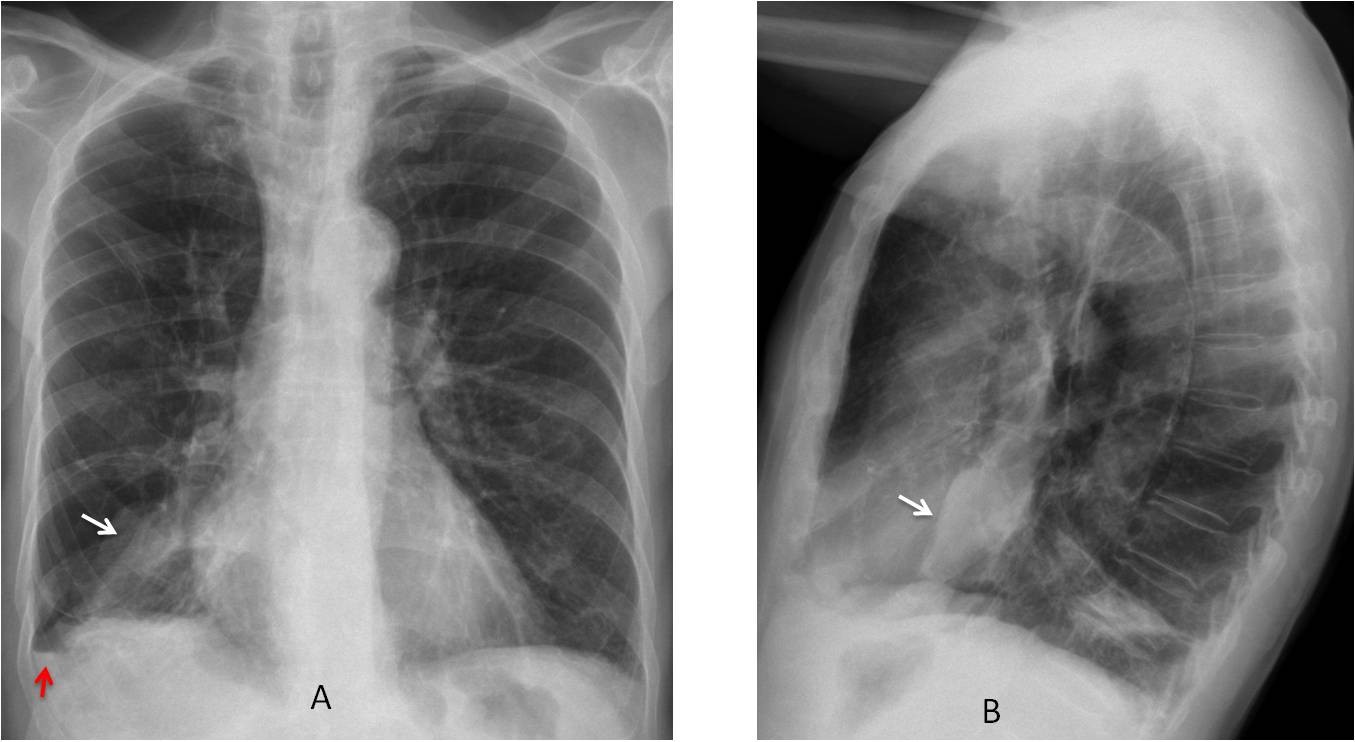
Fig. 10
Fig. 10: Partial RLL collapse and subpulmonary pneumothorax. PA view shows a triangular opacity at the right base (A, white arrow). A V line is visible (A, red arrow) with pleural air above. The lateral view shows a sharp anterior lung-pleura interface (B, arrow).
CT confirms the basal pneumothorax (A, arrow), with segmental collapse of the right lower lobe (B, arrow). In the axial view, the pneumothorax extends to the lung apex (C, arrow). There are bullae throughout both lungs.
Pneumothorax has many causes. The three most common are iatrogenic (biopsy, surgery), traumatic (Fig. 11), and spontaneous (secondary to rupture of an apical bleb).
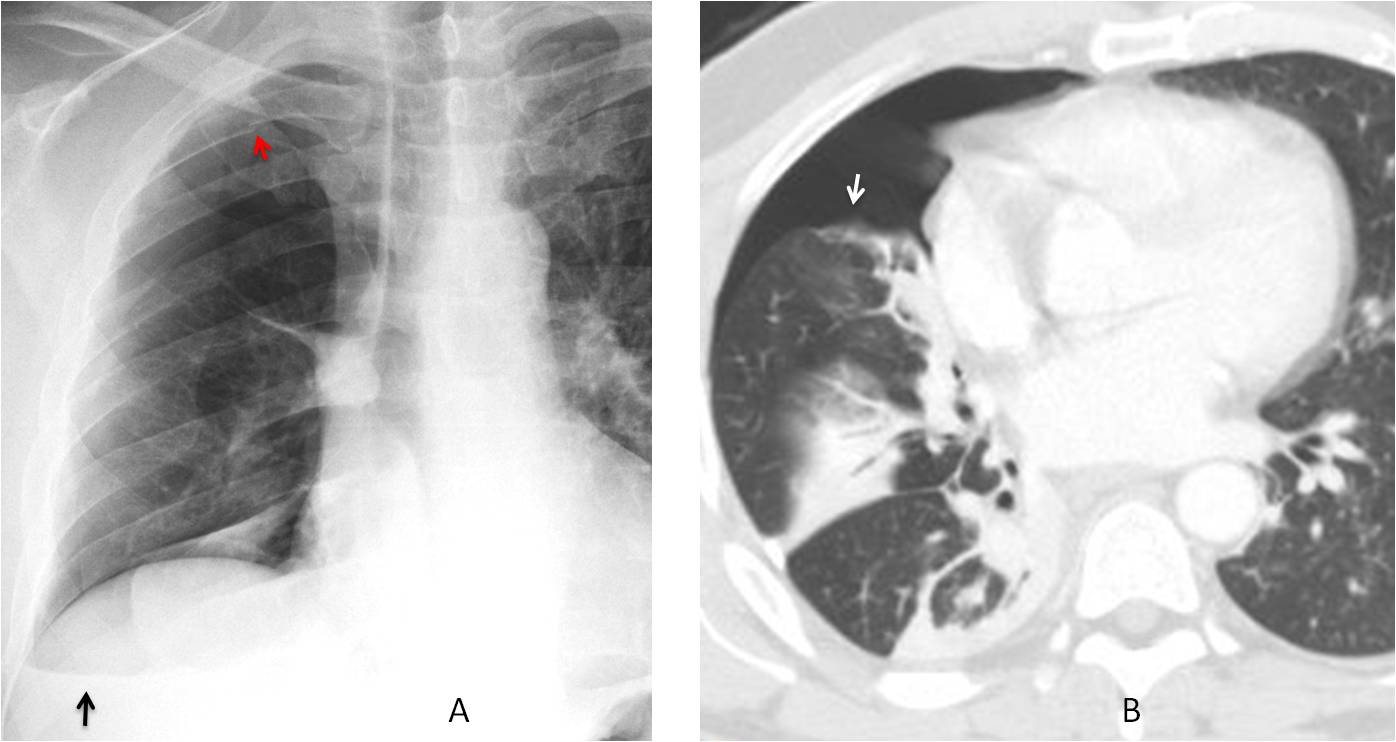
Fig. 11
Fig. 11. Pneumothorax secondary to trauma from a car accident. PA chest film depicts nondescript opacities in the right lower lung. A V line is visible (A, black arrow). There is a fracture of the third rib (A, red arrow). CT shows pulmonary opacities indicative of lung contusion and a pneumothorax (B, arrow).
Just for show, I want to end with striking images of an uncommon cause of pneumothorax: cavitated pulmonary metastases breaking into the pleura and causing air leakage (Fig. 12).
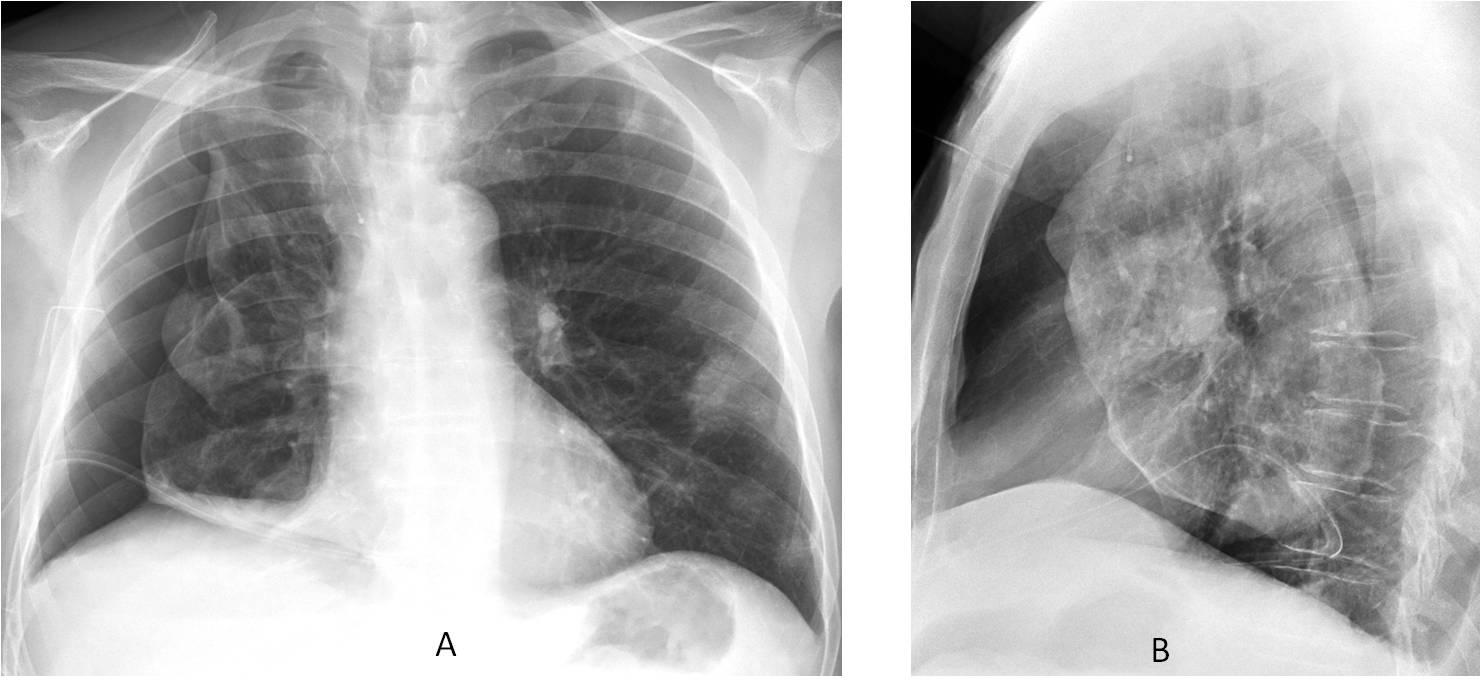
Fig. 12
Fig. 12: 45-year-old man with a right pneumothorax and multiple nodules in the left lung.
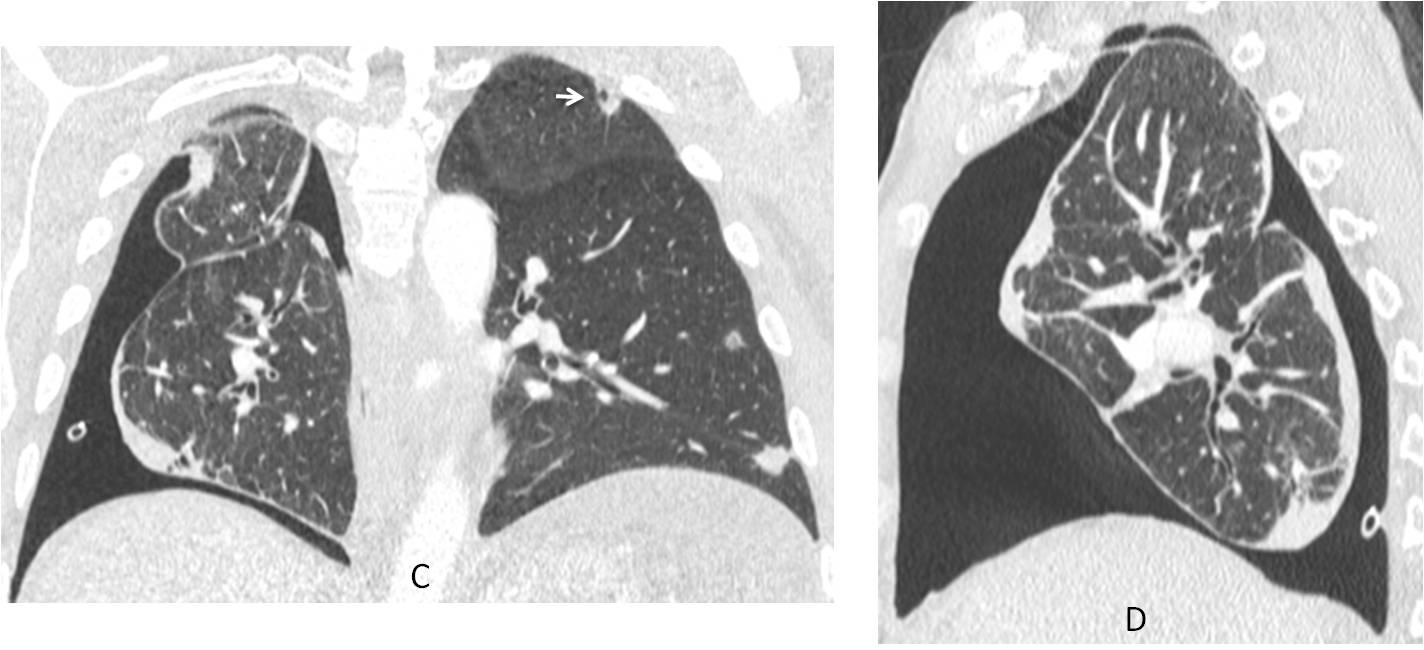
Fig. 12
Coronal and sagittal CT images show the pneumothorax and peripheral nodules in the left lung, one of them cavitated (C, arrow). Diagnosis: osteosarcoma with metastases.
Follow Dr.Pepe’s Advice:
1. The V sign helps to detect unsuspected pneumothorax.
2. Tension pneumothorax is characterised by mediastinal shift and diaphragmatic depression.
3. Lobar collapse causes an atypical location of pneumothorax.
4. Most common causes of pneumothorax are iatrogenic, traumatic, and spontaneous.


Right sided pneumothorax.
-pulmonary hilum narrowing
-round opacity in left cardiophrenic angle.(ivc?)
-hepatomegaly.
sorry right cardiophrenic
Right hydropneumothorax.
…penso che l’AP del torace sia in posizione supina….abnorme raccolta aerea si proietta contro la cupola diaframmatica dx, con profilo diaframmatico anomalo posteriormente in LL…sottile immagine rx-opaca curvilinea a livello dell’incrocio clavicola e 1 costa nonchè tra la 10 ed 11 costa in basso…. sulcus sign….il tutto come da pntorace….sufficiente completare con radiogramma in espirazione….
Right basal emphysematous bulla with right sided small pneumothorax.
A small air-fluid level at the right costophrenic angle – V line and Right sided pneumothorax.
After the heart (overlaps on the spine) there are viewing a line of transparent – maybe there is a pneumothorax loculated retrosternally.
Right sided pneumothorax
There is right sided air fluid level. Left hilum is slightly depressed in my opinion (same level with right hilum). Left lower lobe collapse with right hydrothorax? In lateral view i saw a vague triangular opacity at lung base.
Ryan
Right upper lobe pneumothorax
Right ap ica pneumothorax…
Rib metastasis (es)…
No rib metastases. Sorry.
Right hydropneumothorax
Congratulations to all of you. Final diagnosis is pneumothorax with V line.
Special mention to Mark, who was the first to suggest the diagnosis.
More information tomorrow
The vessels in the right lower zone are not reaching the periphery.
A lucency appears superimposed pushing the posterior part of the right diaphragm down.
Segmental emphysema?
right side pneumothorax