Dr. Pepe’s Diploma Casebook: Case 83 – SOLVED!
Dear Friends,
Today I am showing chest radiographs of a 59-year-old man with abdominal pain and pruritus.
What do you see?
Check the images below, give me your thoughts in the comments section, and come back for the answer on Friday.
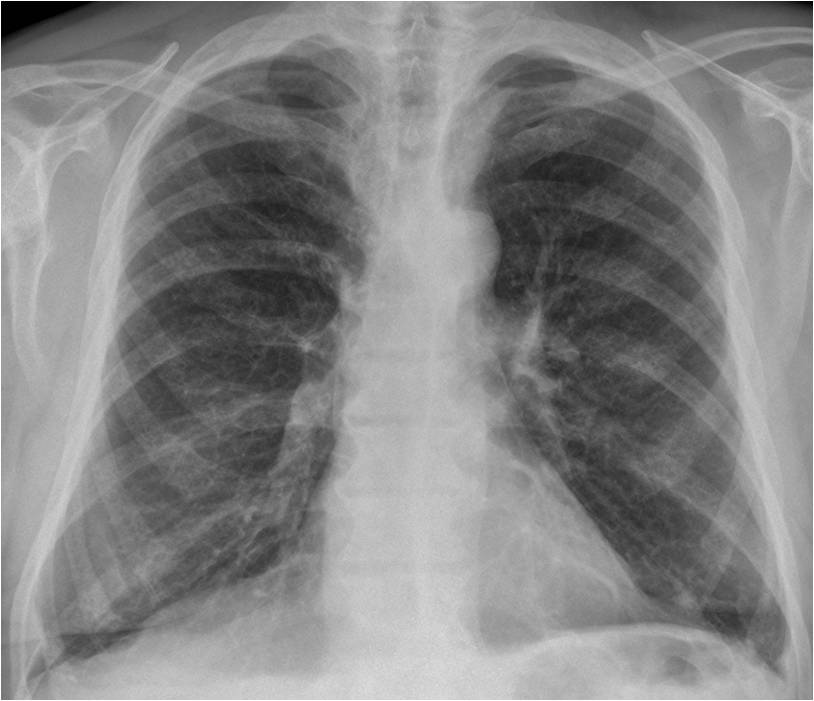
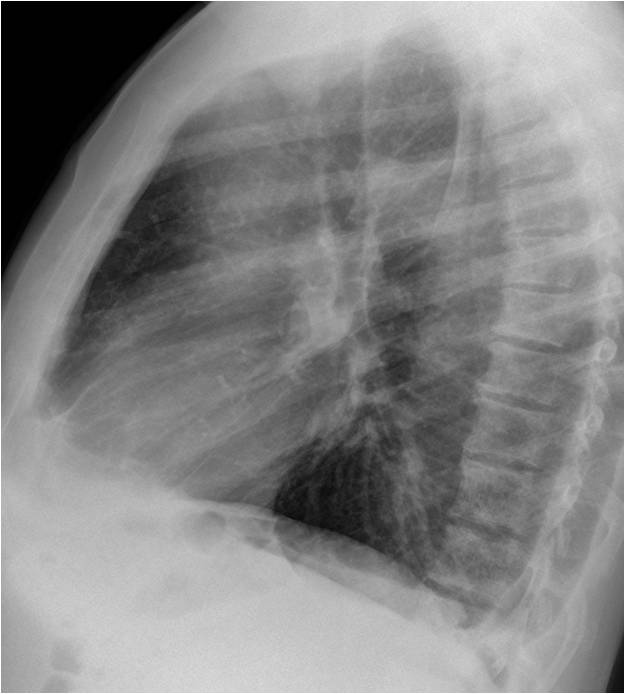
Findings: the most obvious finding is an overall increase in bone density. The sclerotic ribs simulate pulmonary infiltrates in the PA view (A). The increased bone density is more evident in the dorsal spine (B).
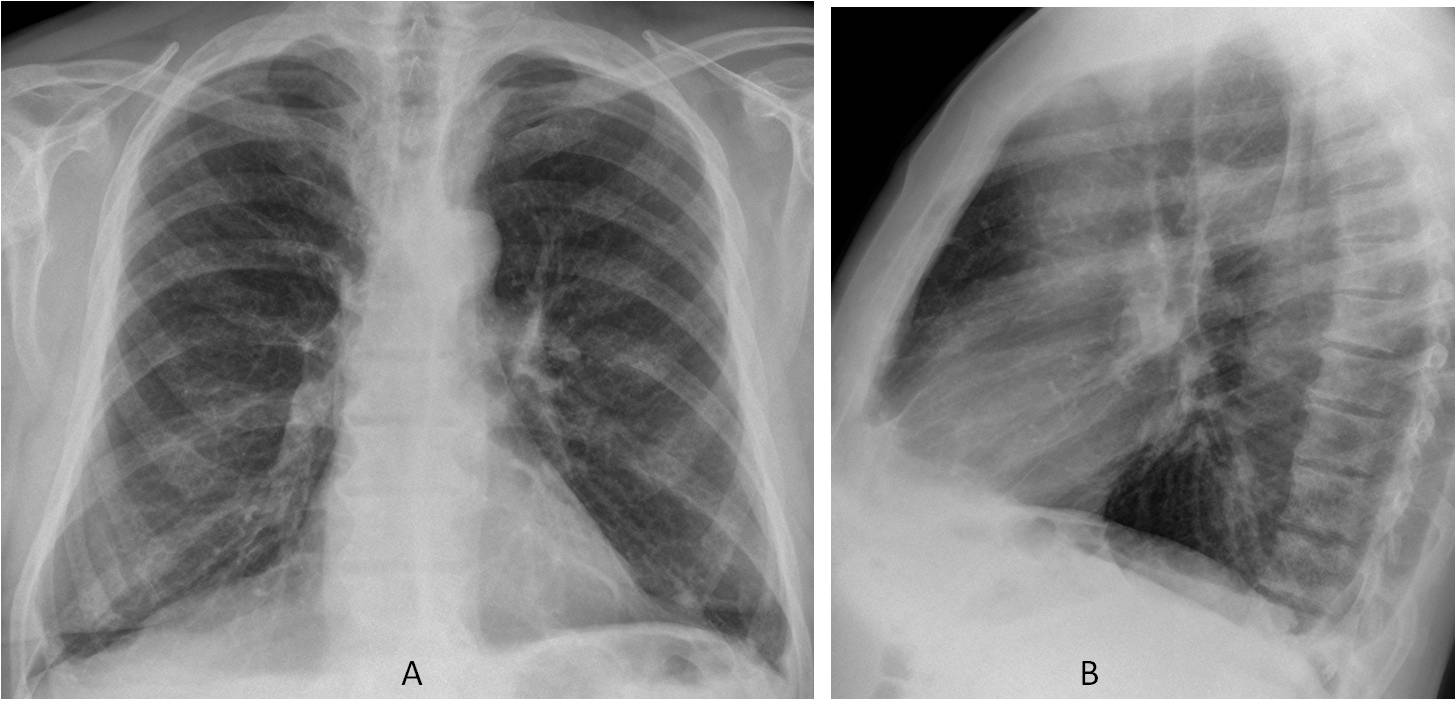
AP and lateral views of the lumbar spine (C and D) show marked sclerosis of the vertebral bodies and pelvic bones. The findings are indicative of a disease that increases the density of marrow-forming bones. Lymphoma and mastocytosis are good possibilities. Biopsy of a skin lesion demonstrated mastocytosis.
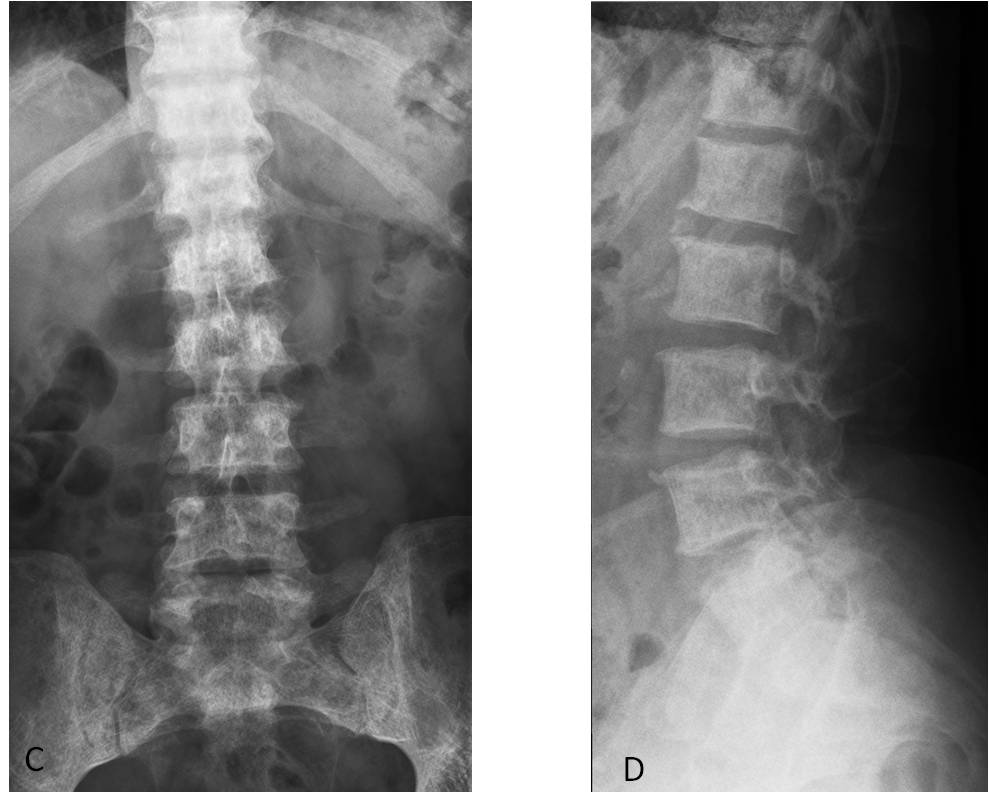
Final diagnosis: systemic mastocytosis
The thoracic spine is an important landmark in the chest radiograph. Hidden by the mediastinal structures in the PA view, it is clearly depicted in the lateral view. It is important to check this structure because it can offer information that may be overlooked or misinterpreted. The objective of this presentation is to review the basic semiology of the thoracic spine as seen in the lateral chest radiograph.
A simple classification divides spinal conditions into focal, affecting one or several vertebra, or diffuse, affecting the whole thoracic spine. Focal conditions may change the height or opacity of the vertebral bodies and the intervertebral disc. Diffuse conditions mainly affect the density of the vertebral column. Static changes (eg, kyphosis, scoliosis) will not be discussed here.
Among the focal processes, the most obvious finding is increased density of a vertebral body (ivory vertebra). The differential diagnosis includes osteoblastic metastasis, lymphoma, hemangioma, and Paget disease. By far, osteoblastic metastasis is the most common cause of dense vertebrae, usually arising from a prostate or breast neoplasm (Fig. 1).
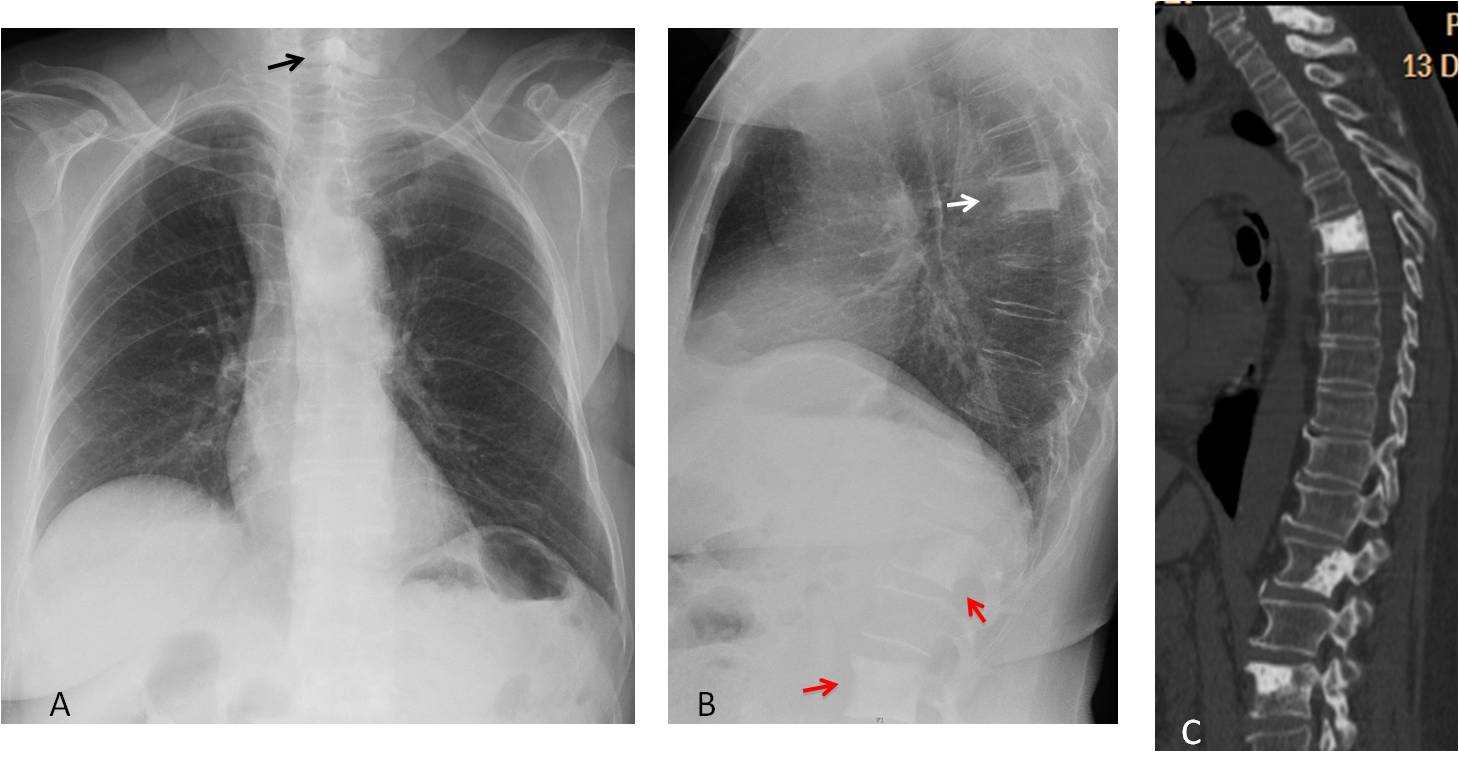
Fig. 1
Fig. 1: 58-year-old woman with left mastectomy for breast carcinoma. PA chest film shows a sclerotic lesion in C-6 (A, arrow). Lateral view shows a D-6 ivory vertebra (B, white arrow), and sclerotic foci in L-1 and L-3 (B, red arrows), confirmed with spinal CT (C). Osteoblastic metastases.
Another cause of ivory vertebra is the condition known as vertebral haemangioma. It is not properly a tumour, but more of a hamartomatous lesion. Vertebral haemangiomas are asymptomatic and an innocuous finding. They appear as a dense vertebra with vertical trabeculation. These features are practically pathognomonic of the condition (Fig. 2).
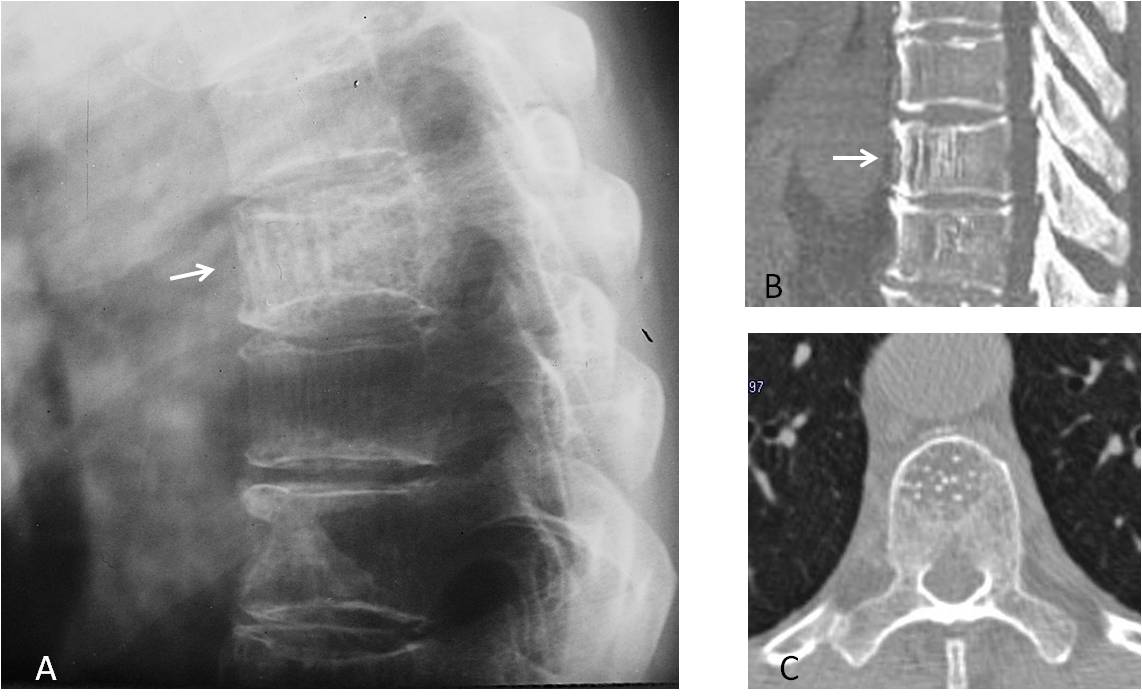
Fig. 2
Fig. 2: Typical hemangioma in a mid-thoracic vertebra (A, arrow). The vertical striation is confirmed with sagittal CT (B, arrow) and is seen as punctiform opacities in the axial view (C).
Paget disease is another cause of ivory vertebra. The size of the vertebral body is usually increased, a finding considered practically pathognomonic (Fig. 3). It should be pointed out that a normal-sized ivory vertebra does not exclude Paget disease .
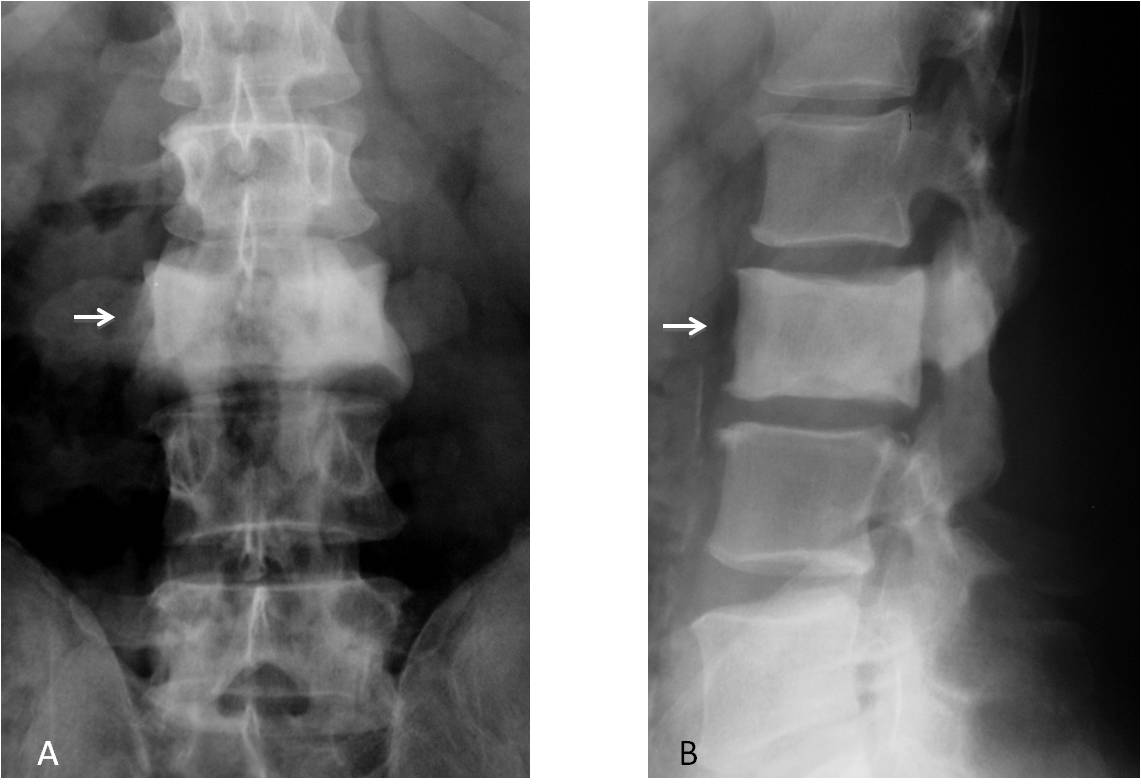
Fig. 3
Fig. 3: Ivory vertebra in Paget disease (A and B, arrows). Note the increased size compared to the vertebrae above and below. My apologies for showing a lumbar vertebra, but it’s such a nice example, I couldn’t resist.
Lytic areas in the vertebrae usually correspond to metastases, the most common tumoural lesions of the spine (Fig 4). The differential diagnosis includes primary tumours and rarely, infection.
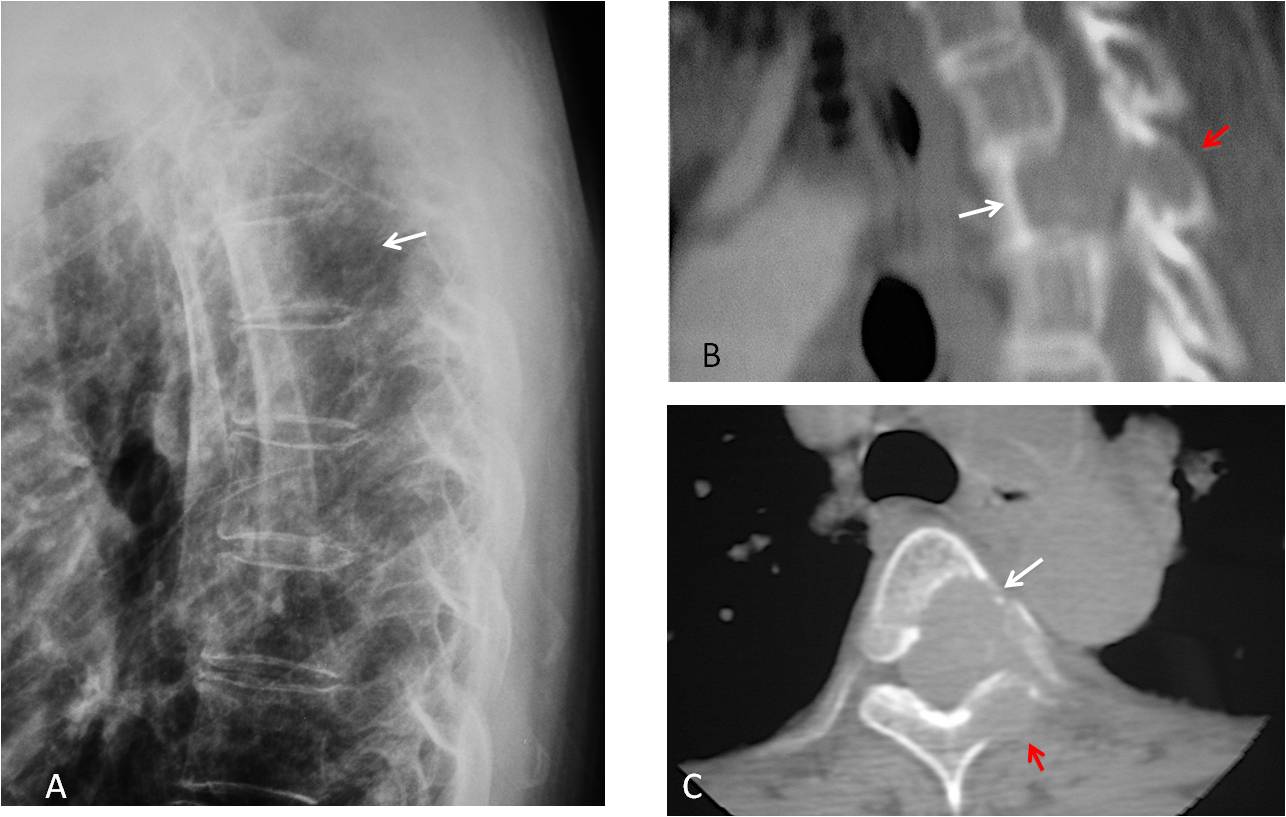
Fig. 4
Fig. 4: Cone-down view from a lateral chest radiograph showing a lytic area in T-4 (A, arrow). Sagittal and axial CT confirm the lesion (B and C, white arrows), which also affects the posterior elements and spinal canal (B and C, red arrows). Diagnosis: metastasis from lung carcinoma.
Loss of height of a vertebra is usually secondary to trauma (Fig. 5). It is less often due to a lytic lesion that has weakened the vertebral structure, resulting in collapse. The subdiaphragmatic region should always be checked to avoid missing fractures of the lower vertebrae (Fig. 6).
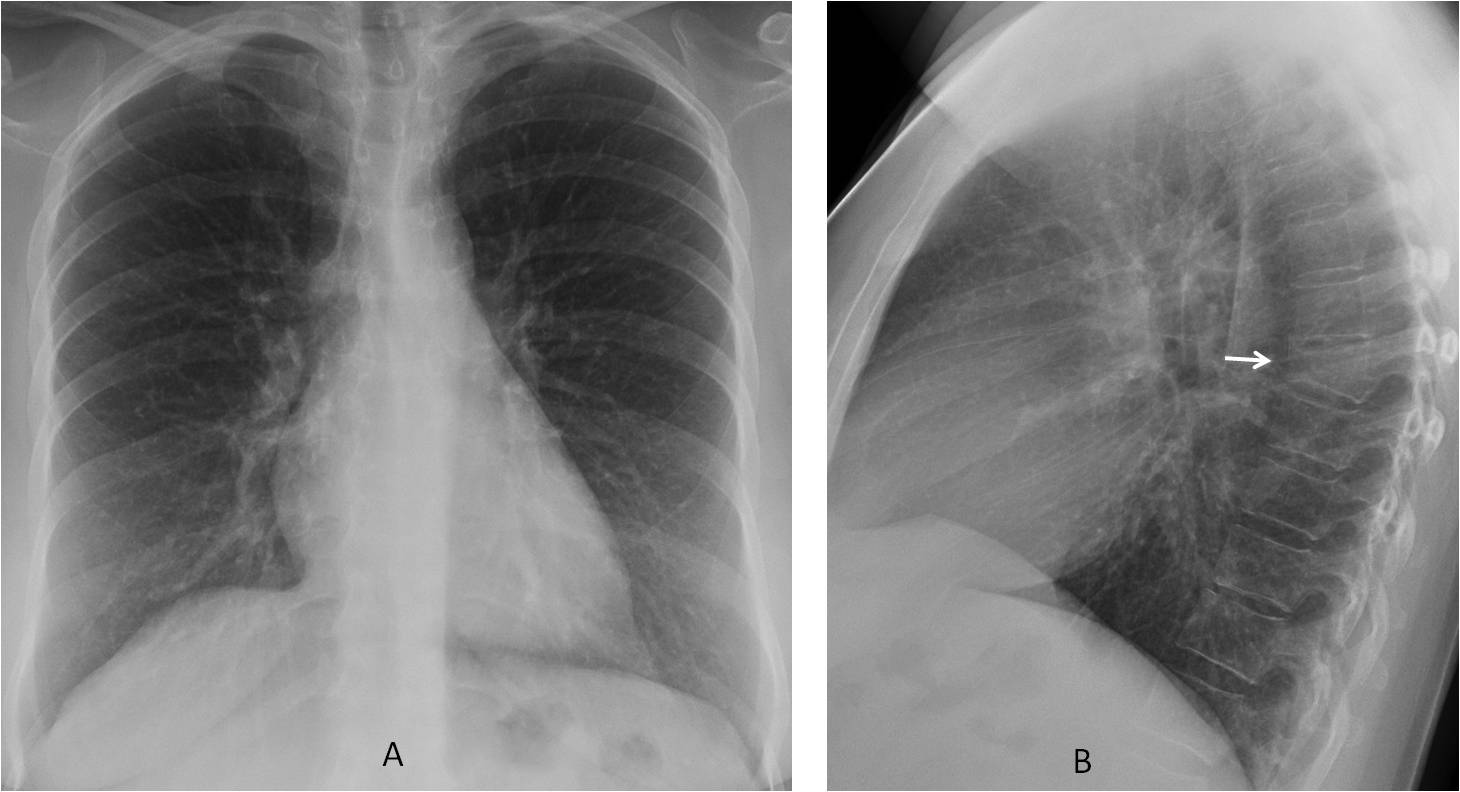
Fig. 5
Fig. 5: Wedged appearance of D-7, secondary to a car accident (B, arrow). The lesion is not visible in the PA view (A).
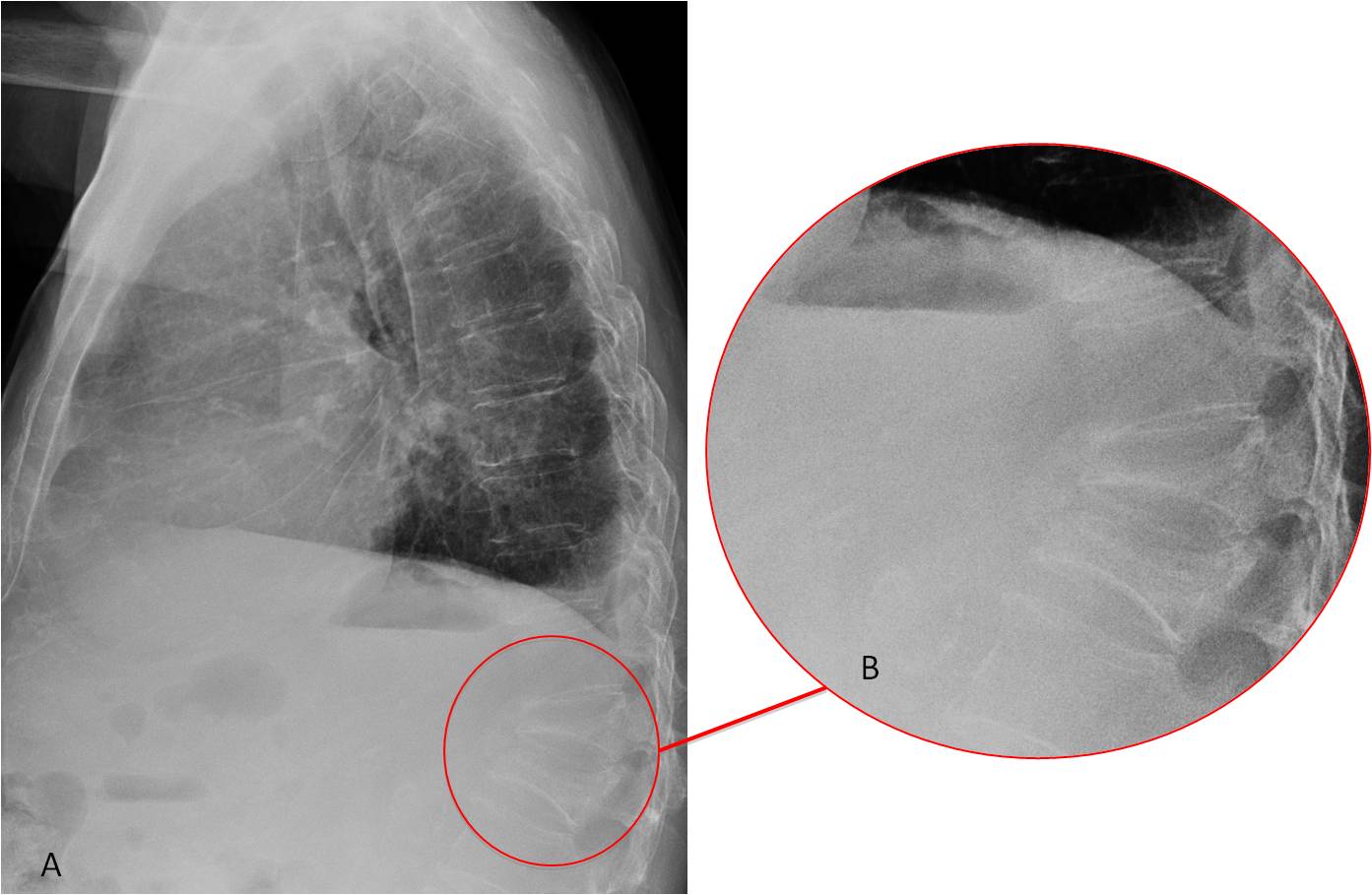
Fig. 6
Fig. 6: L-1 and L-2 compression fractures secondary to a car accident (A, circle). The fractures are better seen in the cone-down view (B).
Narrowing of the intervertebral space is the hallmark of disk disease. The most common cause is degenerative disk disease, in which the narrowing is accompanied by sclerotic borders of the vertebral end-plates. Calcification of the disk is an associated finding that increases with age. It has no clinical significance (Fig. 7).
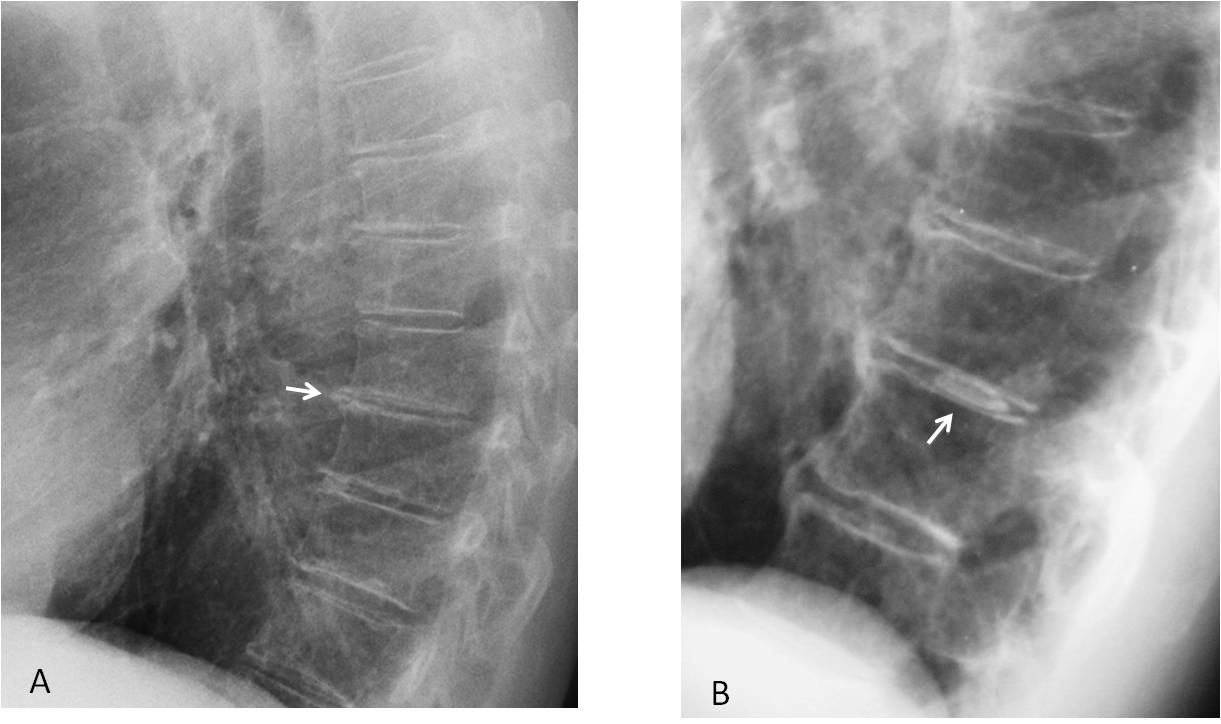
Fig. 7
Fig. 7: Degenerative narrowing of the disk at D7-D8. Note the sclerotic vertebral endplates (A, arrow). In another patient, the narrowed disk is associated with calcification of the nucleus pulposus (B, arrow), which is more prevalent in the lower thoracic spine.
Infectious spondylodiscitis also narrows the disk space and produces irregularity of the endplates of one or both vertebrae. The findings may be subtle, and a high index of suspicion is needed to discover them in an early stage (see case 121 Caceres’ corner). TB is the most common cause worldwide, followed by S. aureus and Brucella infection in endemic areas (Figs. 8 and 9).
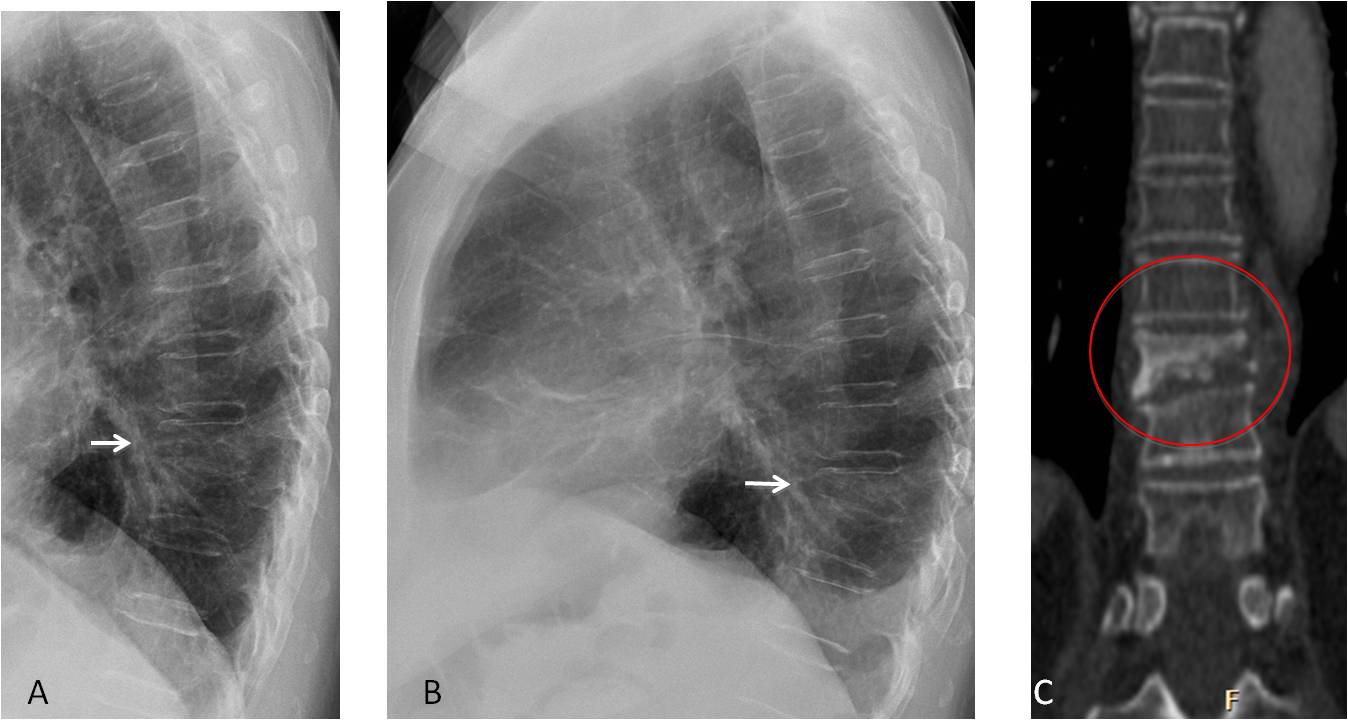
Fig. 8
Fig. 8: 57-year-old man with spinal pain. Initial film shows D9 height loss that was overlooked (A, arrow). Three months later there is obvious collapse of D9 (B, arrow). CT confirms the collapsed vertebra and irregularity of the D10 upper plate (C, circle). Diagnosis: tuberculosis.
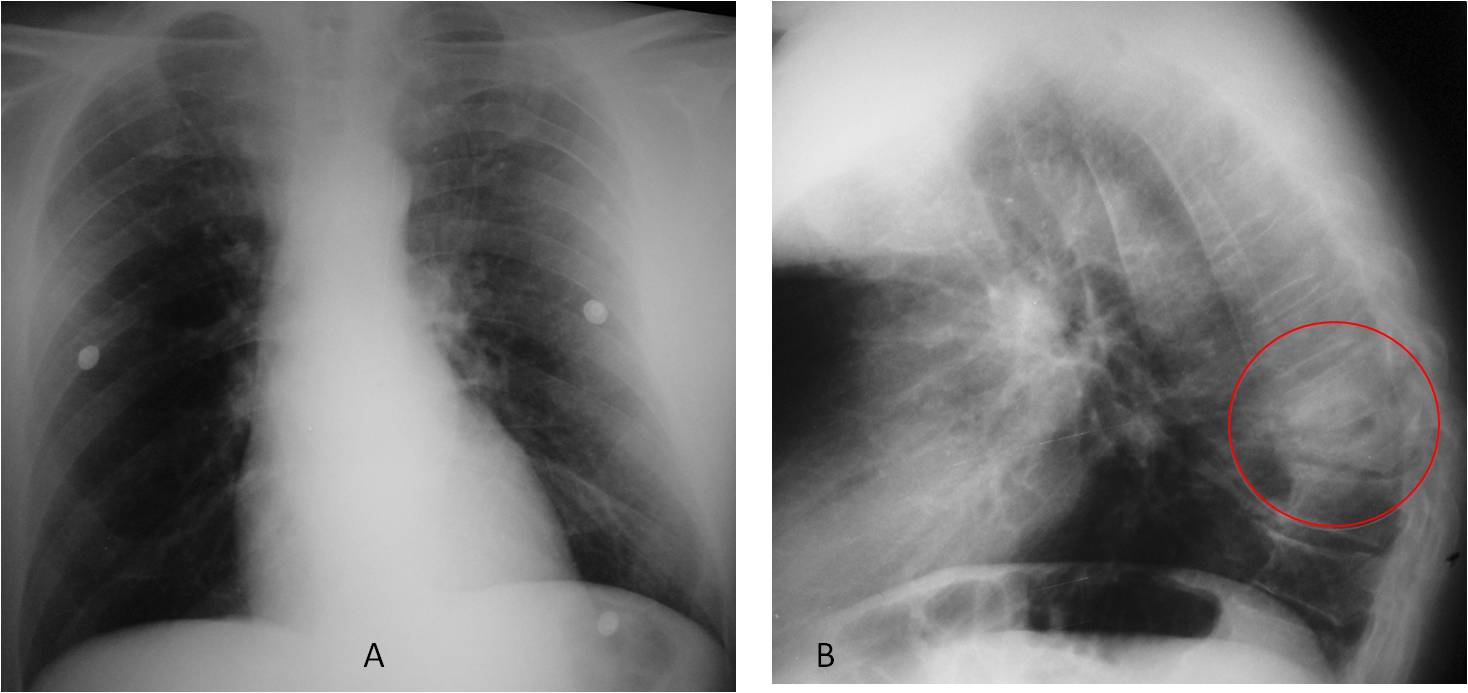
Fig. 9
Fig. 9: 54-year-old indigent admitted with severe back pain. PA view (A) is unremarkable. Lateral view shows sclerosis and marked destruction of D8-D9 and the intervening disk (B, circle).
Coronal and sagittal CT confirm the severe bone destruction, as well as an accompanying soft-tissue mass (C, arrows). Diagnosis: advanced pyogenic infection.
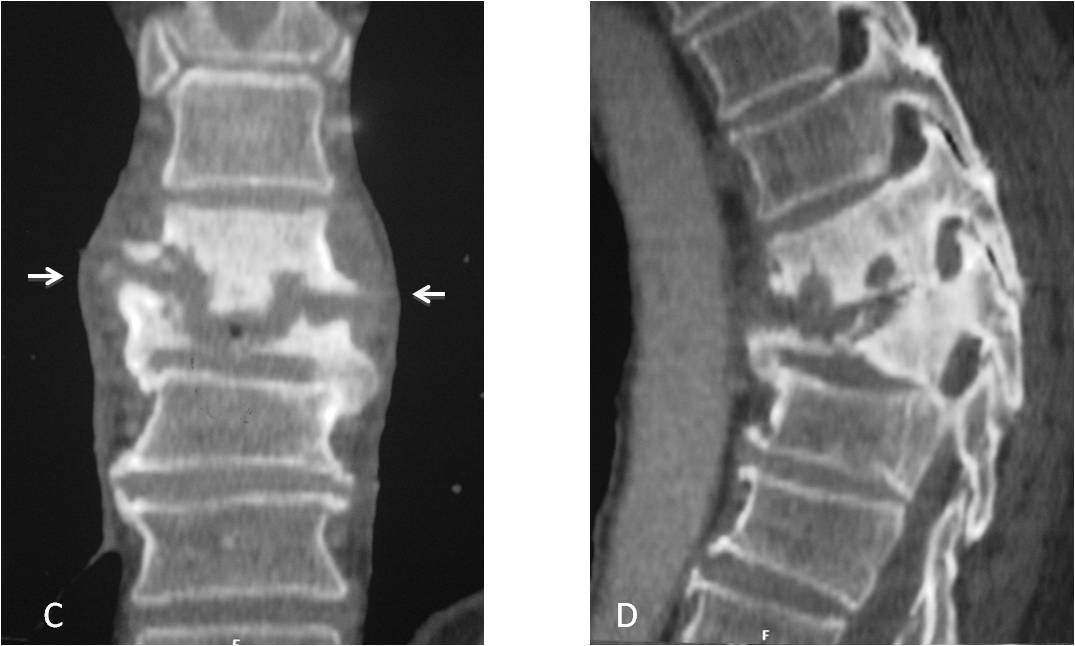
Fig. 9
Diffuse processes may increase or decrease the opacity of the thoracic spine. Overall increased opacity has many etiologies (e.g. osteoblastic metastasis, fluorosis) that should be investigated clinically. Renal failure causes the typical “rugger-jersey” appearance.
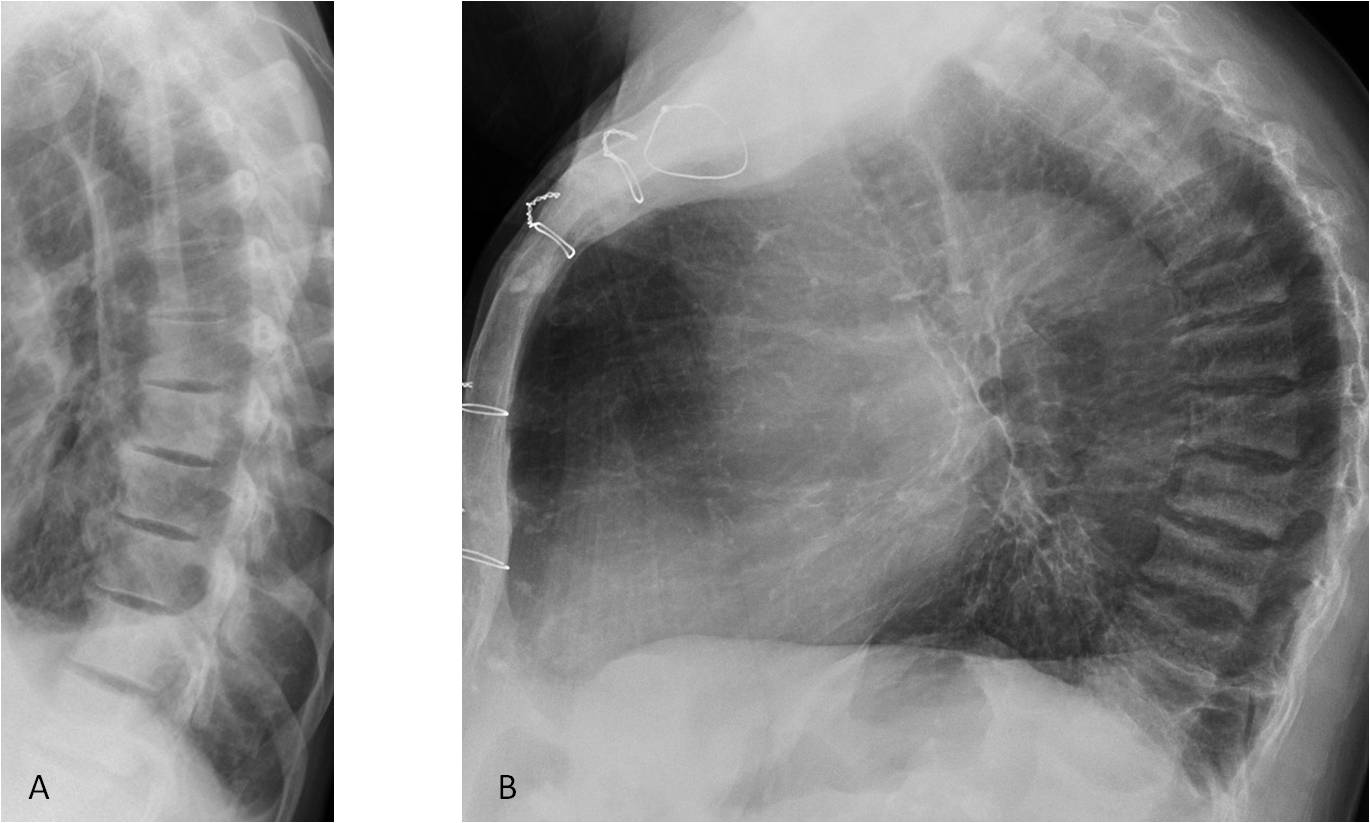
Fig. 10
Fig. 10. Osteoblastic metastases in adenoid cystic carcinoma (A). The increased bone density may be difficult to see by the untrained eye. B. Rugger-jersey spine in a patient with chronic renal failure.
Loss of opacity is very difficult to detect unless it is accompanied by multiple collapsed vertebra having a biconcave appearance (“fish” vertebrae). Most common causes are: osteoporosis, myeloma, or iatrogenic (Fig. 11)
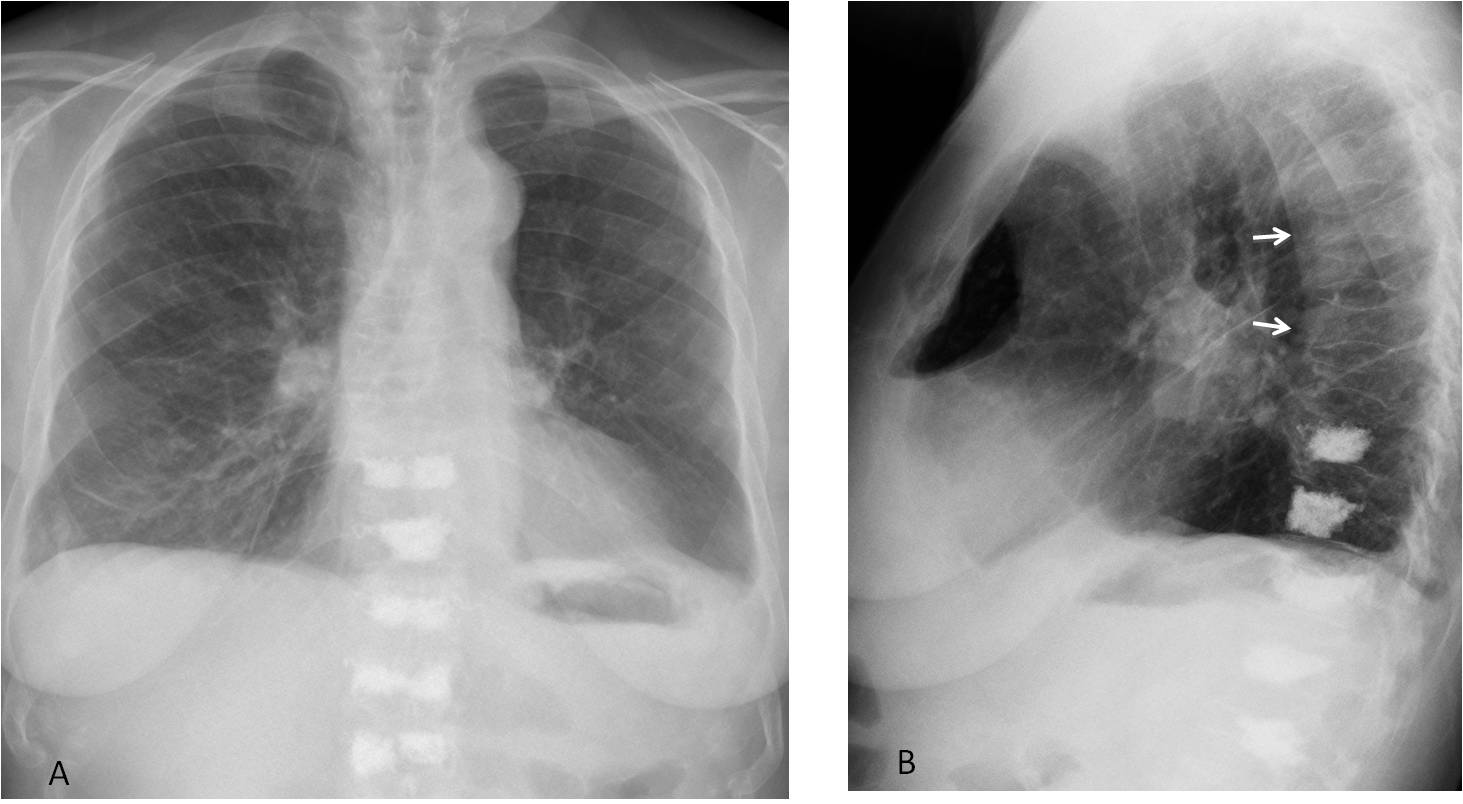
Fig. 11
Fig. 11. Marked spinal osteoporosis after lung transplantation. Note the multiple collapsed fish vertebrae (B, arrows). Vertebroplasty has been done in the lower thoracic and upper lumbar vertebrae.
Follow Dr.Pepe’s Advice:
1. Most common cause of ivory vertebra is metastasis from breast or prostate.
2. Metastatic disease is the most frequent cause of lytic defects in the vertebrae.
3. Infection is characterised by narrowing of the disk and vertebral plate erosion.
4. Diffuse loss of spinal density cannot be recognised unless it is accompanied by vertebral fractures.


Diffuse bony sclerosis
Mastocytosis
With the hint from aloria I think mastocytosis.
i too take hint from above! – mastocytosis
Also
flattened right dome.
anterior (and posterior?) cardiophrenic angle blunted.
Others gave a hint, so I remembered that there was a case of mastocytosis earlier. After a brief search, it found that indeed it was in Caceres Corner case 103, and radiographs belong to the same patient.
I imagine the case is either too easy or too difficult, because there are only four brave doctors answering.
…carissimo Professore …..oppure il caso lo hai già presentato un’altra volta….non ricordi?????
You are right: case 103 of Caceres’ corner. Considering my advanced age, it is a miracle that after presenting over 200 cases, I have repeated only one!
Still, this case is an excuse to discuss the thoracic spine in the chest radiograph, to be seen on Friday.
…grandissimo Prof: ….l’avevo capito e per questo motivo non ho partecipato alla discussione…..il mio Bari è 2° in classifica e vede profumo di serie A !!!!
Wait for the case next week. Is is a surprise to commemorate the 125th. presentation.
And congratulations for Bari’s classification!
hello everybody.
good job.
how can i follow the daily / weekly posts by Dr Pepe??
how can i regularly participate in this quiz??
thx
Just bookmark this page.
Dr. Pepe’s cases are posted on a Monday, usually every two weeks (with occasional exceptions). You can also follow the ESR on Facebook, as new cases are posted on our page: facebook.com/myESR