Dr. Pepe’s Diploma Casebook: Case 86 – SOLVED!
Dear Friends,
Today I am presenting radiographs of a 27-year-old male drug abuser who has had a fever for the last two weeks.
Check the images below, leave your thoughts in the comments section and come back for the answer on Friday.
Diagnosis:
1. Staph Pneumonia
2. TB
3. Pneumocystis
4. None of the above
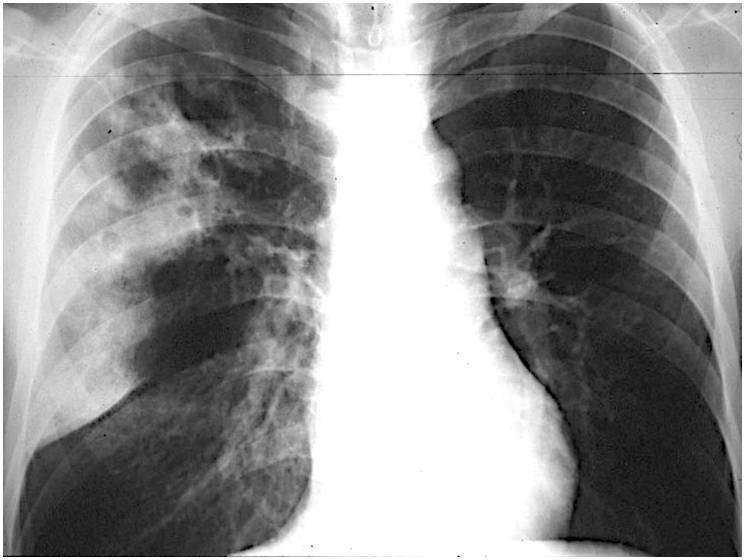
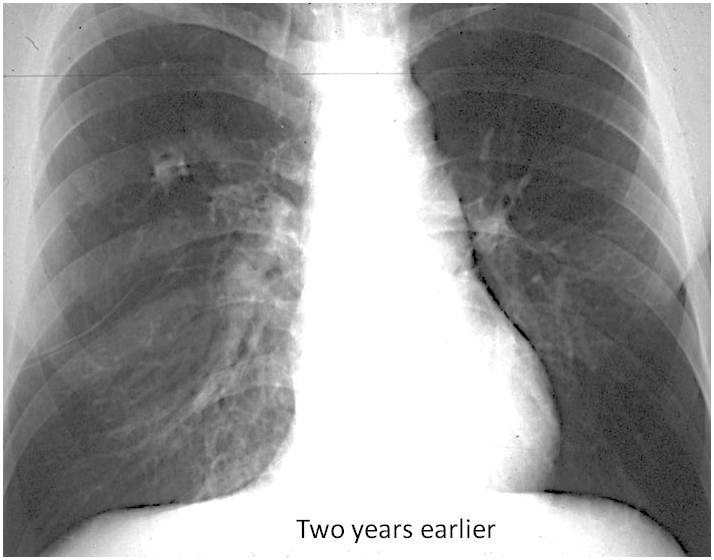
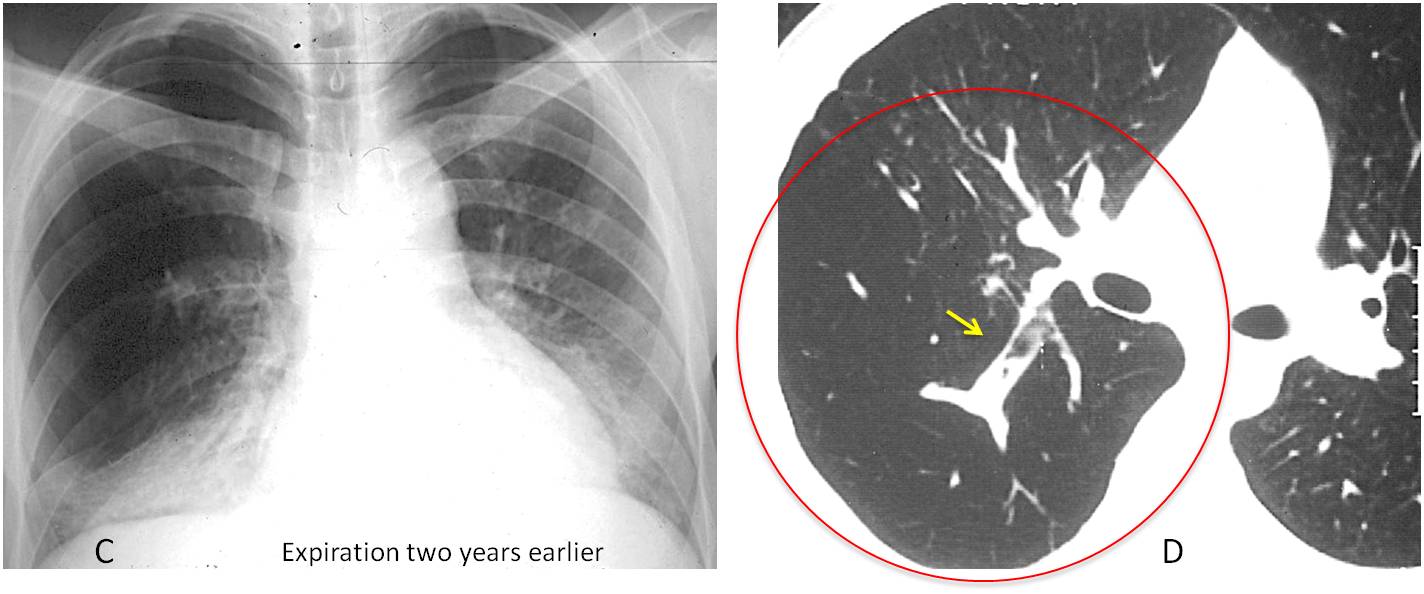
Findings: PA chest film shows RUL air-space disease with an apparent cavitation (A, red arrow). The infiltrate is limited inferiorly by a descended minor fissure (A, white arrow). Two years earlier the fissure was in the same position (B, white arrow) and a rounded opacity was visible in the RUL (B, yellow arrow).
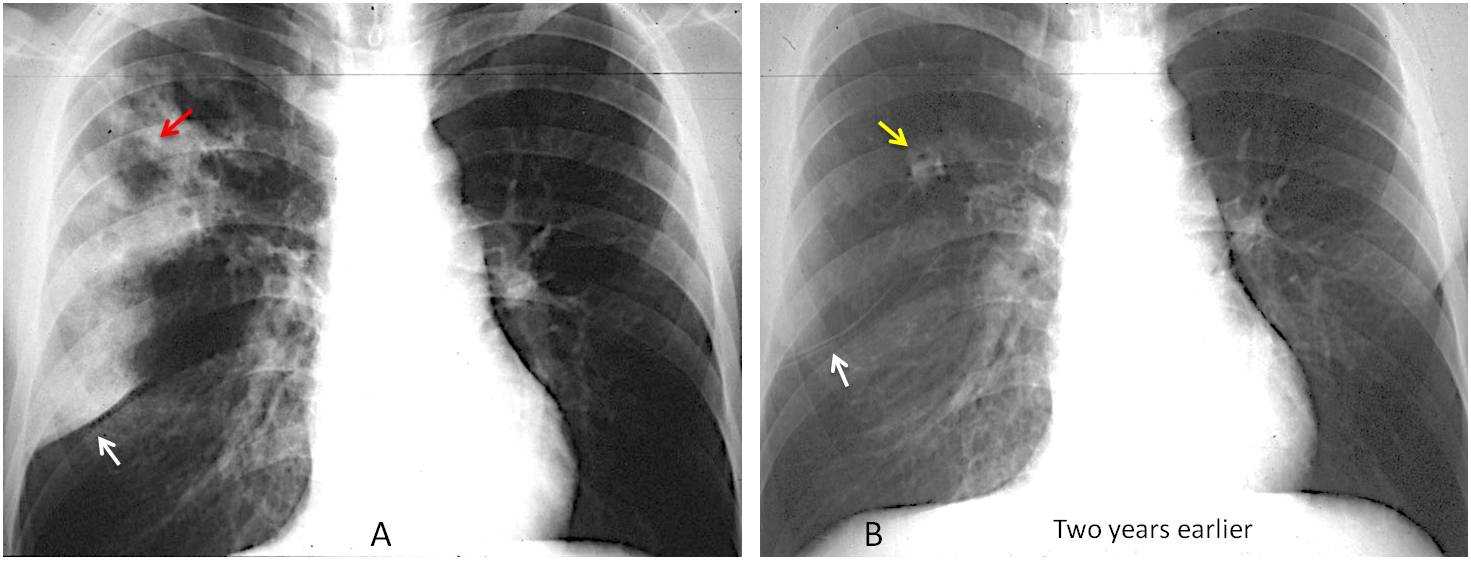
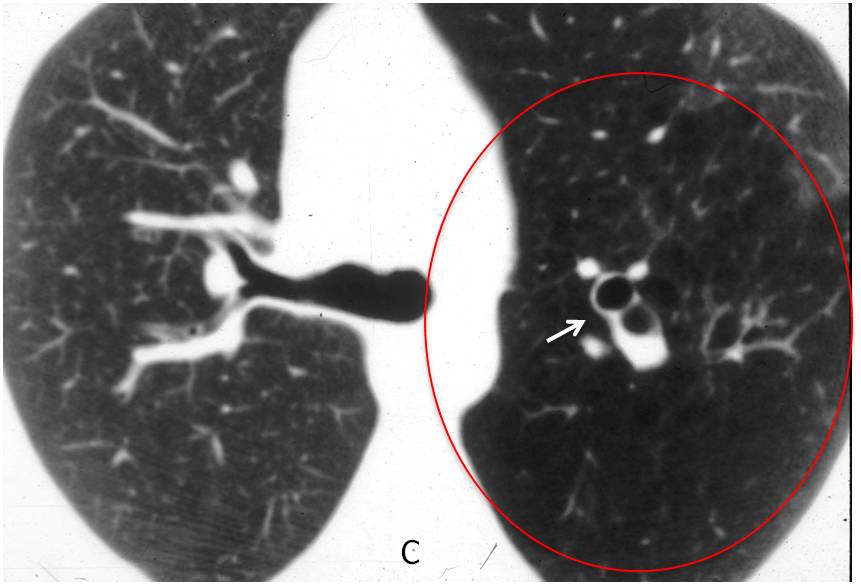
Expiratory film taken two years earlier depicted air-trapping in RUL (C). CT at that time showed increased lucency of the posterior segment of RUL (D, circle) with a large mucous impaction (D, arrow). This appearance is highly suggestive of congenital bronchial atresia.
Final diagnosis: pneumococcal pneumonia in a patient with congenital bronchial atresia
I am showing this case to discuss the subject of expiratory films. Standard chest radiographs are taken with the patient upright and in full inspiration. In certain circumstances, expiratory films may complement the information offered by the inspiratory film.
There are two main indications for acquiring an additional expiratory view:
When pneumothorax is suspected and the inspiratory film is not helpful
To confirm or exclude air-trapping of the lung
Here I’d like to discuss the diagnostic value of expiratory films.
The most common indication for an expiratory film is to confirm/exclude a suspected pneumothorax that is not seen in the inspiratory radiograph (Fig. 1). Negative findings on expiration are practically conclusive for ruling out pneumothorax (Fig. 2)
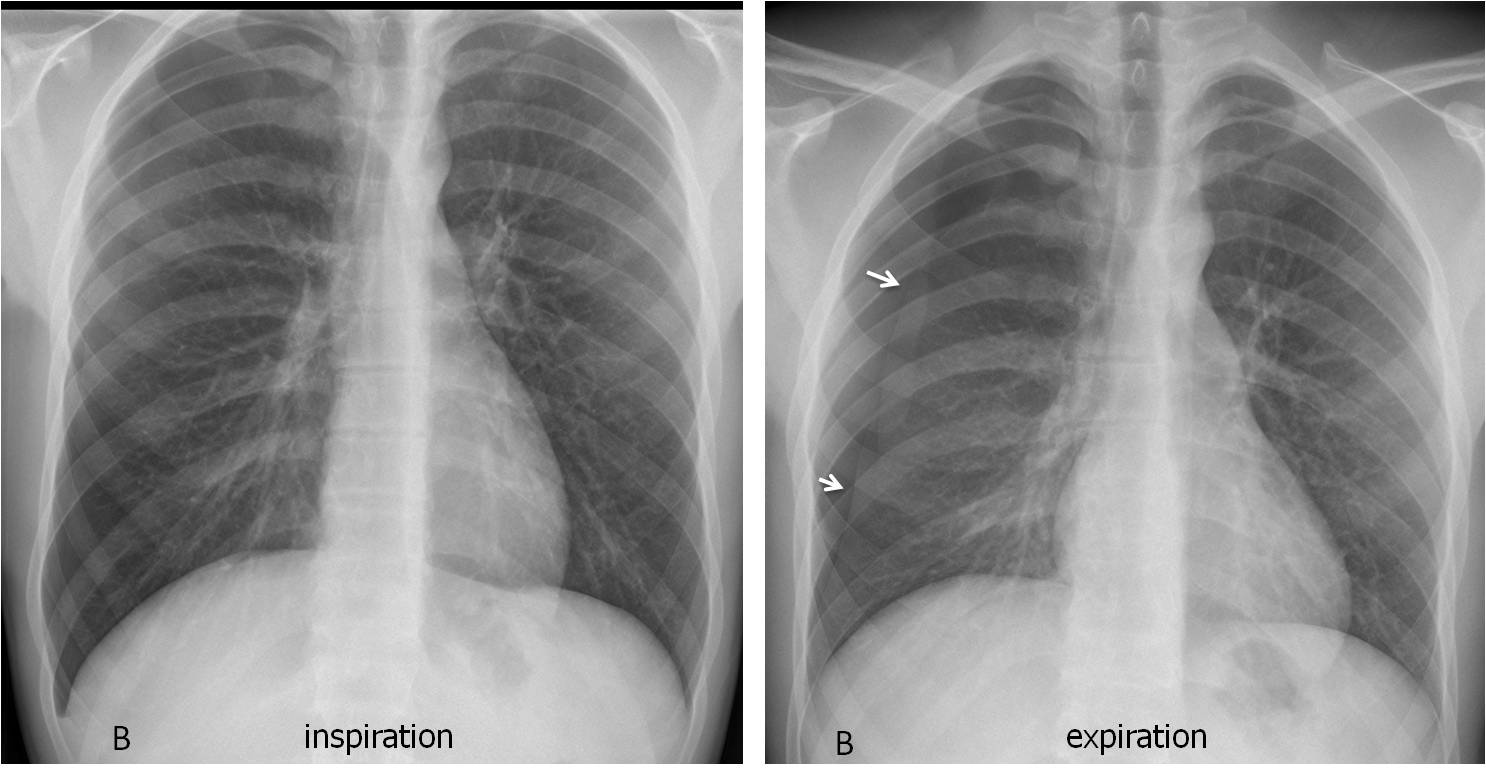
Fig. 1
Fig. 1: 24-year-old man with sudden chest pain suggestive of a pneumothorax. The inspiratory film (A) is inconclusive. The expiratory film clearly shows a right pneumothorax (B, arrows).
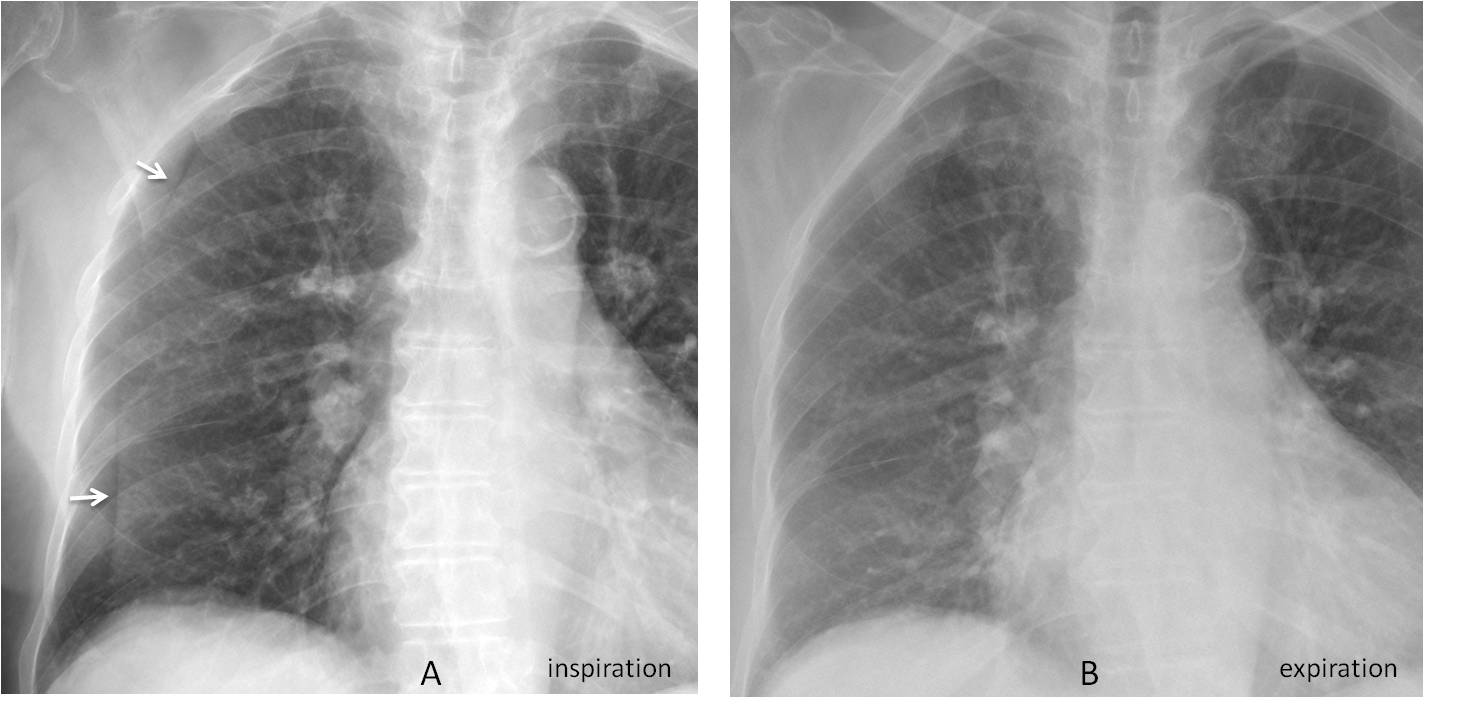
Fig. 2
Fig. 2: 79-year-old woman with a peripheral line that suggests a pneumothorax (A, arrows). The line disappears in the expiratory film (B), confirming that it is caused by a skin fold and pneumothorax is not present.
The second indication to obtain an expiratory film is to confirm/exclude air-trapping of the lung. Nowadays, CT on expiration is widely used to detect areas of small airway obstructive disease, but expiratory views are little used in conventional radiography. A pity, because they are a great source of information.
Remember that you cannot diagnose air trapping unless you have an inspiration/expiration pair.
Localised areas of air trapping within the lungs are easily demonstrated with expiratory films, and indicate further workup to establish an etiologic diagnosis (Fig. 3).
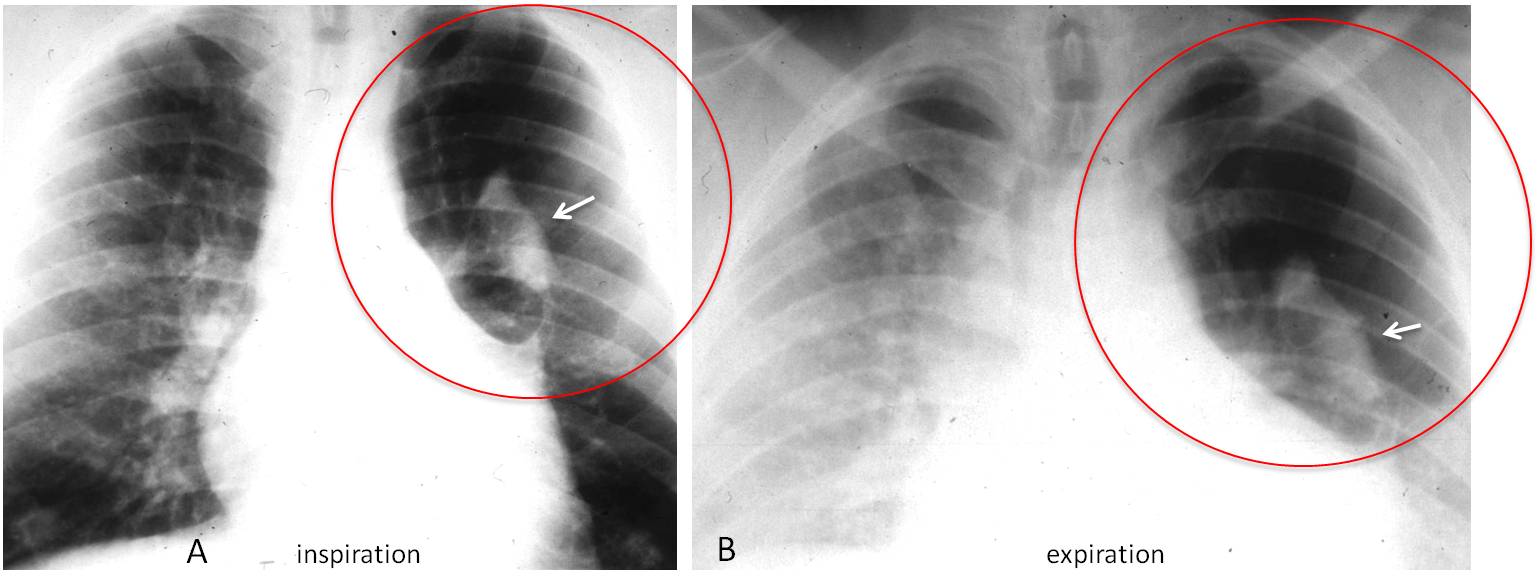
Fig. 3
Fig. 3: 45-year-old asymptomatic man. PA chest film shows increased lucency of the left upper lung (A, circle) and an ovoid shadow within it (A and B, arrows). The expiratory film depicts air-trapping in this area (B, circle).
Axial CT depicts a large area of lucent lung in the apical-posterior segment of the LUL (C, circle) with a dilated bronchus filled with mucus and air in the center (C, arrow). Diagnosis: congenital bronchial atresia
When an entire lung traps air, the expiratory film confirms the diagnosis and identifies the affected lung as the one that fails to empty on expiration (Fig. 4).
It is important to emphasise that air trapping can only be confirmed with inspiration/expiration films, because a single inspiratory film can be deceptive (Fig. 5).
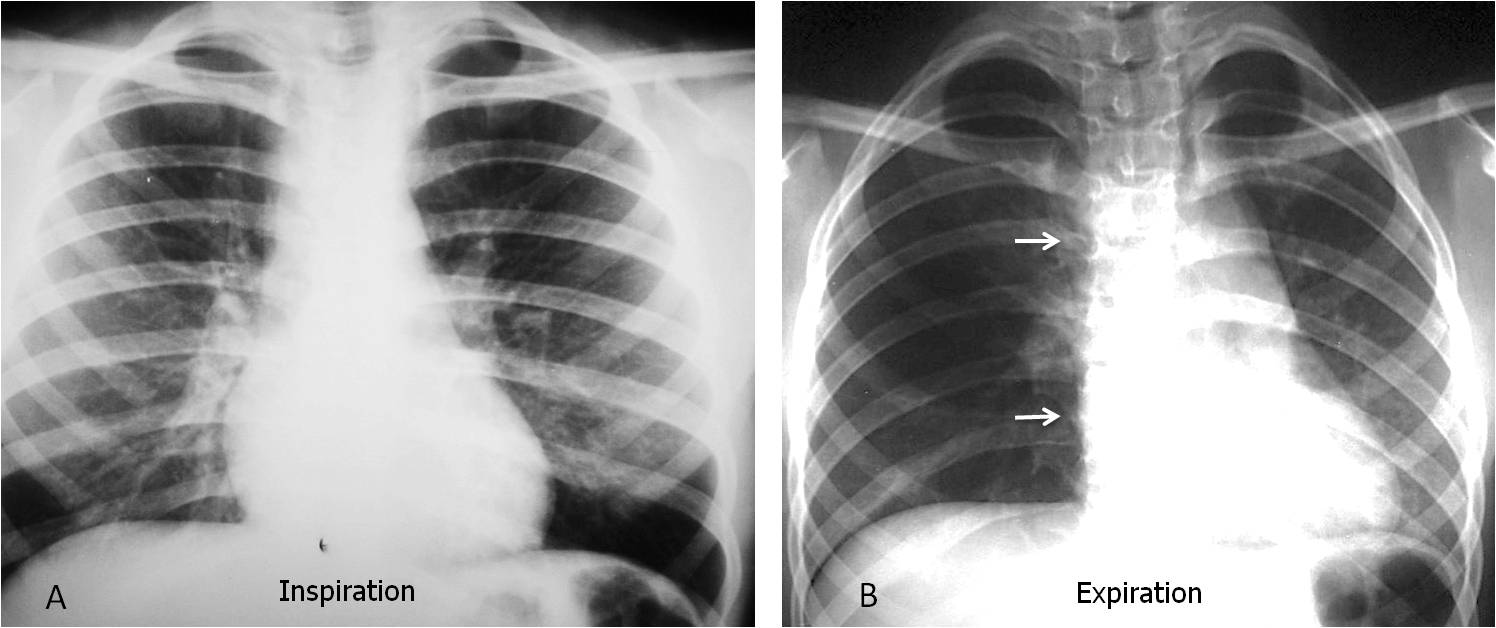
Fig. 4
Fig. 4: 3-year-old child with suspected foreign body aspiration. Inspiratory film (A) looks normal. Expiratory film shows air-trapping of the whole right lung with mediastinal deviation towards the left (B, arrows). A foreign body was retrieved from the right main bronchus.
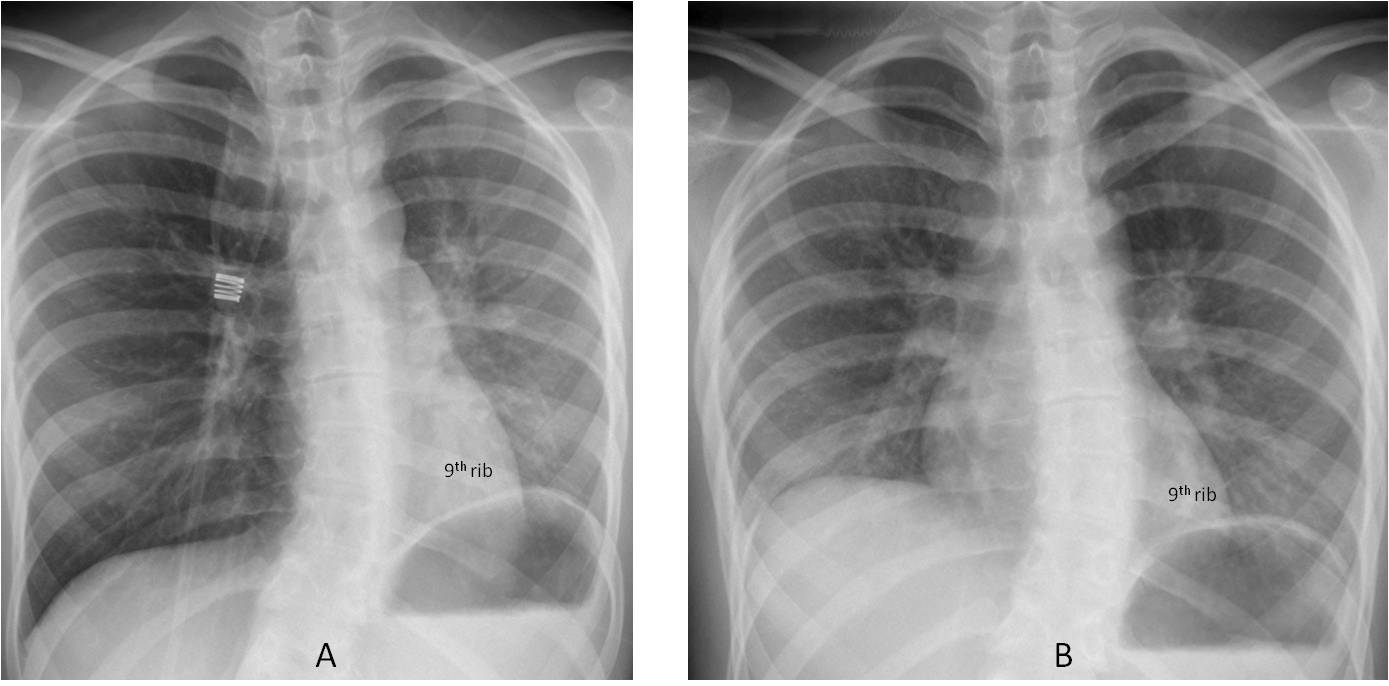
Fig. 5
Fig. 5: patient with extrinsic asthma. Inspiratory film (A) shows increased lucency of the right lung and a smaller left lung. On expiration (B), the right lung lucency disappears and the left lung remains the same. This appearance is typical of obstruction of the left main bronchus: on inspiration, air enters the right (normal) lung, which becomes more lucent. On expiration, the right lung empties.
Note that the left hemidiaphragm does not move (it is superimposed on the 9th rib in inspiration and expiration).
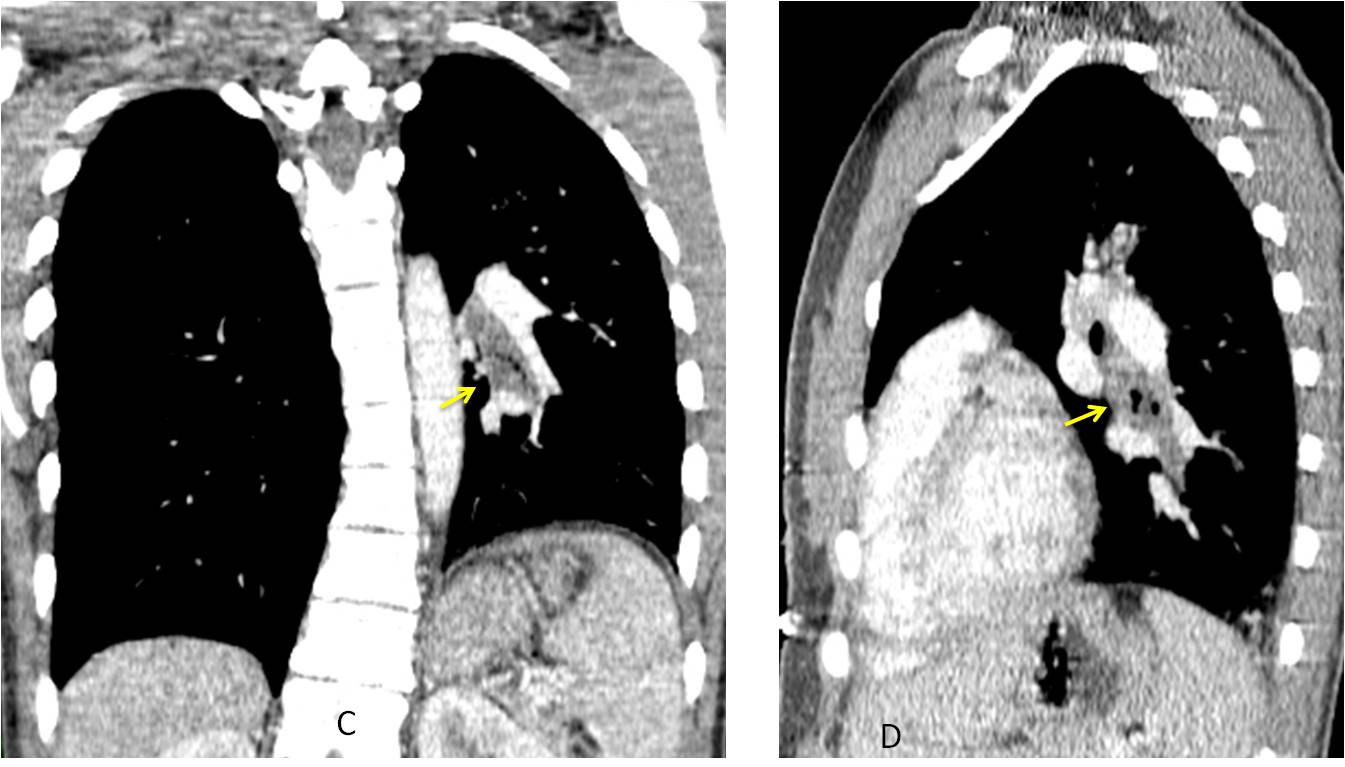
Fig. 5
Coronal and sagittal CT images show obstruction of the left bronchus by thick mucus (C and D, arrows). The patient was treated with mucolytics and bronchodilators, and the appearance of the chest returned to normal.
Broadly speaking, the two main causes of air-trapping are:
- Central bronchial obstruction, of any cause
- Peripheral obstructive disease of the small airways.
Figs. 4 and 5 are good examples of air-trapping due to a central obstruction. CT is diagnostic in these cases and is the technique of choice when a segmental bronchial lesion is suspected, but not visible on conventional radiography (Fig. 6).
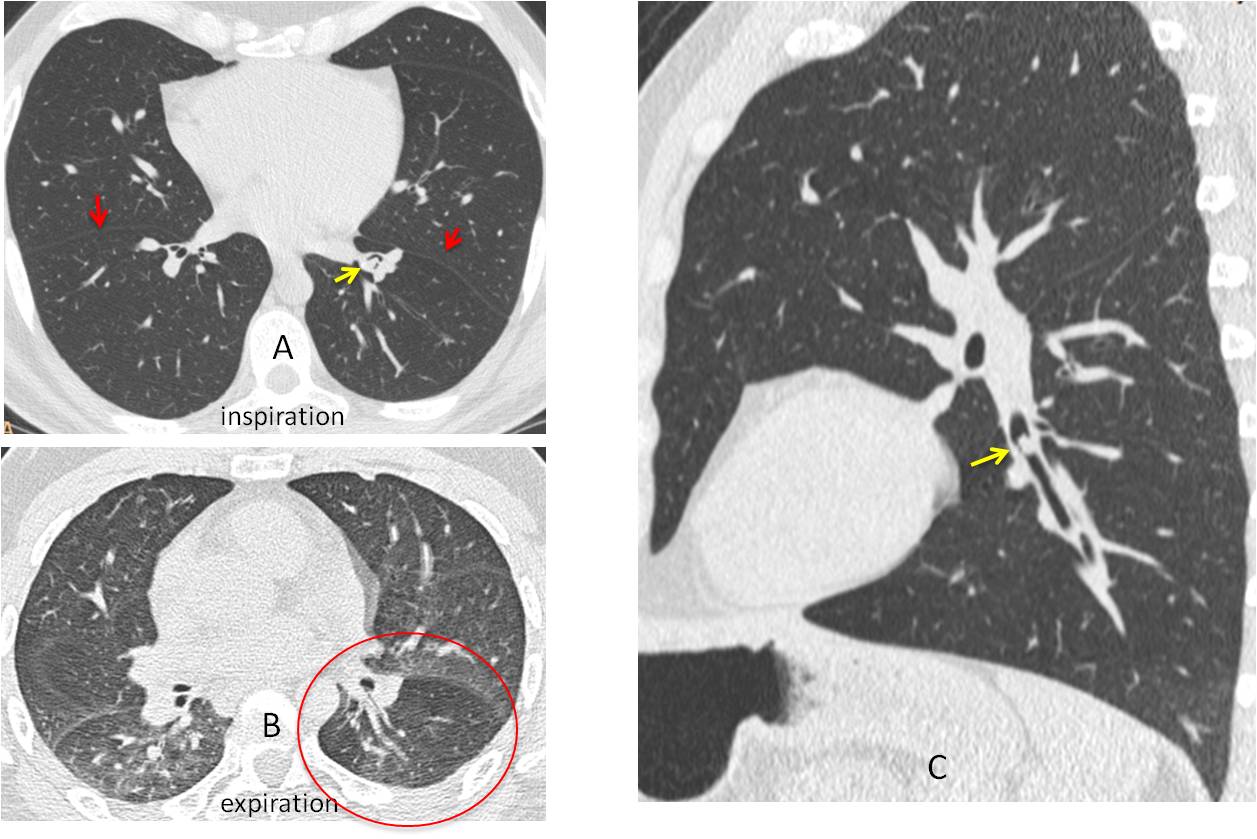
Fig. 6
Fig. 6: 42-year-old man with persistent cough. Inspiratory CT shows slight LLL volume loss (A, red arrows) with a suggestion of an endobronchial lesion (A, yellow arrow). The expiratory image shows LLL air-trapping (B, circle). Sagittal reconstruction confirms a small rounded lesion in the LLL bronchus (C, arrow). Diagnosis: carcinoid
Peripheral obstructive disease of distal bronchi may affect the entire lung or a part of it (Fig. 7), or be widespread, a sign of diffuse small airway disease (Fig. 8). Swyer-James/McLeod syndrome is a well-known cause of unilateral hyperlucent lung. In these patients, the main bronchi are permeable and the air-trapping is secondary to peripheral bronchiolitis following viral infection in childhood (Fig. 7).
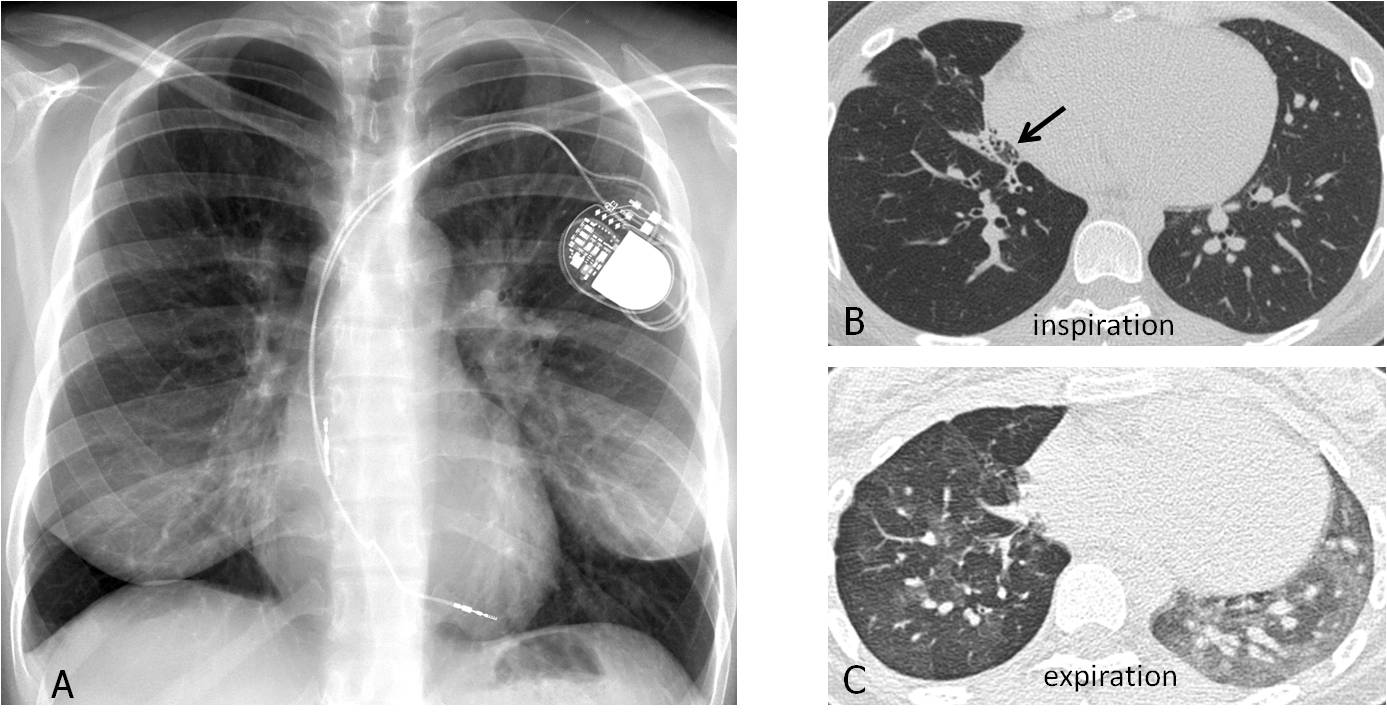
Fig. 7
Fig. 7: 47-year-old woman with MacLeod syndrome. PA film shows a hyperlucent right lung with decreased vascularity (A). Inspiratory CT shows decreased vascularisation and bronchiectasis (B, arrow). Expiratory CT confirms right air-trapping (C).
Expiratory CT is now widely used to detect small airway obstructive disease, characterised by the typical mosaic attenuation and air-trapping (Fig. 8).
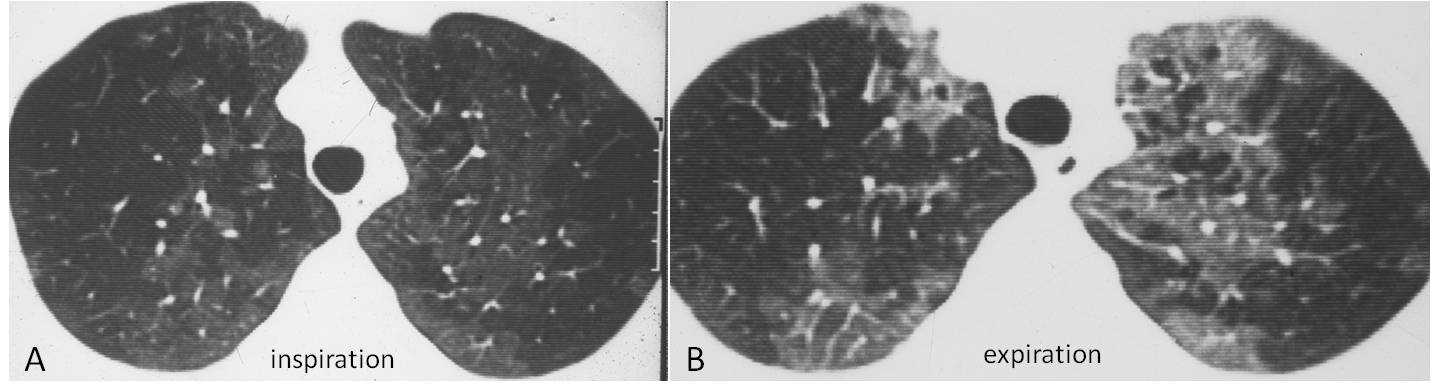
Fig. 8
Fig. 8: patient with diffuse bronchiolitis showing areas of mosaic attenuation on inspiration (A) and air-trapping on expiration (B). This study was done to prove to a skeptical colleague that the white areas on inspiration were normal and the dark areas abnormal. It dates from 1984, which makes me feel like a pioneer.
Lung hernias are uncommon. They may not be visible in inspiratory films, but can manifest in expiratory views. Lung hernia is secondary to weakening of the chest wall and is usually related to previous surgery. It can occur in the apex of the lung (Fig. 9), but most (80%) are intercostal (Fig. 10).
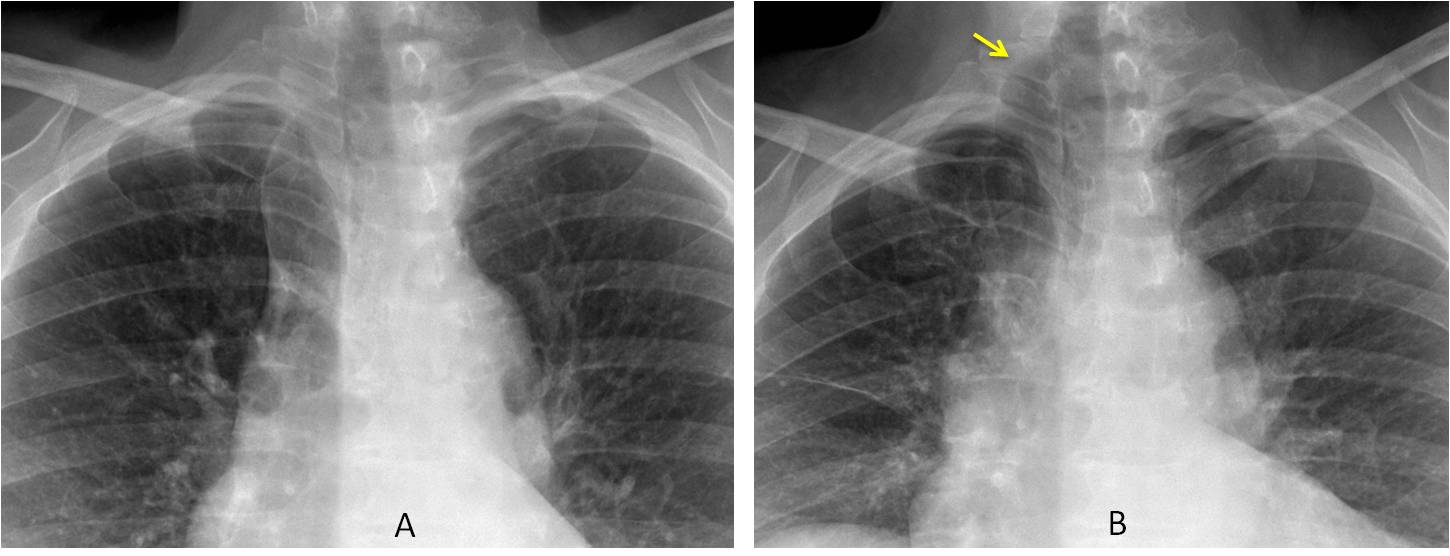
Fig. 9
Fig. 9: 49-year-old asymptomatic woman. The upper lungs appear normal on inspiration (A). Expiratory film shows apical herniation of the right lung (B, arrow). Incidental azygos lobe.
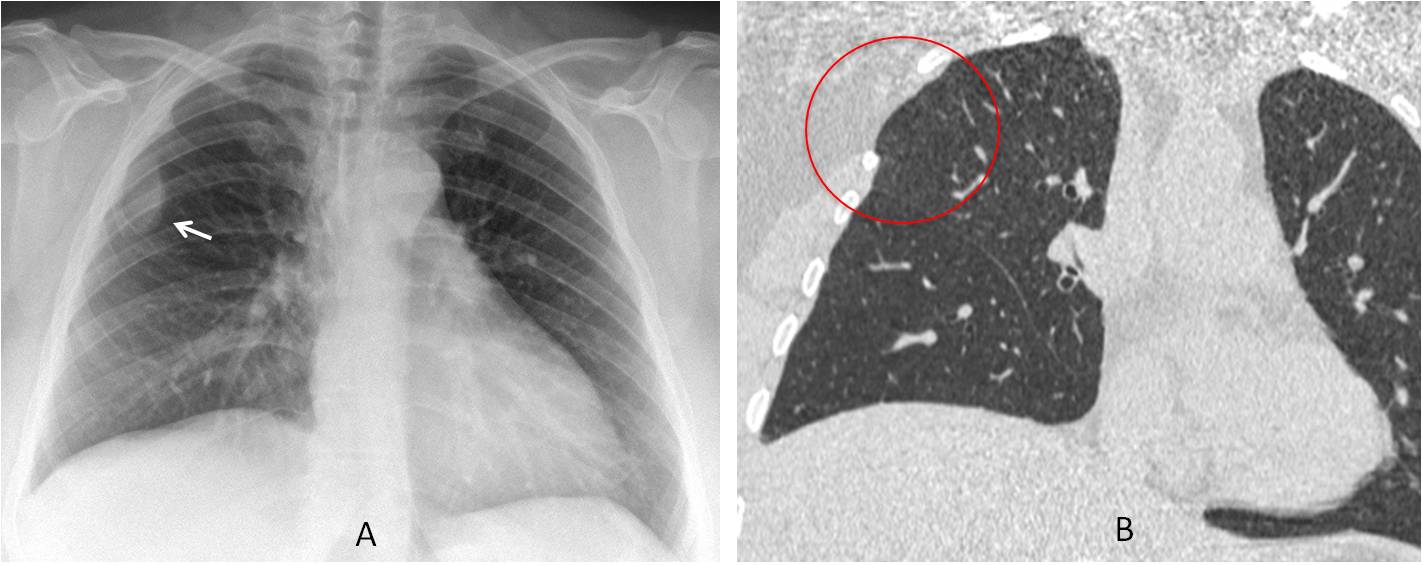
Fig. 10
Fig. 10: 41-year-old woman who underwent chest surgery in childhood. PA chest film shows a right extrapulmonary opacity (A, arrow). The corresponding intercostal space is widened. Coronal CT confirms the widened intercostal space and atrophy of the intercostal muscles (B, circle). The extrapulmonary opacity is not visible.
The patient was placed in the left decubitus position, and fat herniation was confirmed (C, arrow). Expiratory CT showed lung herniation at the same weak spot (D, red circle).
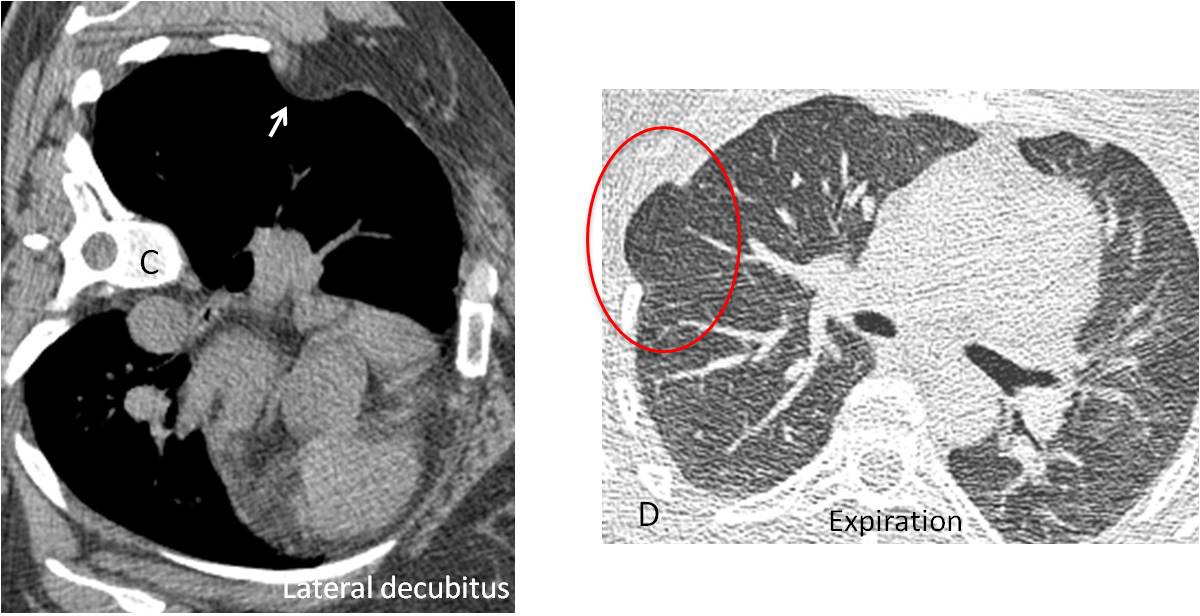
Fig. 10

Follow Dr.Pepe’s Advice:
1. The most common use of expiratory films is to demonstrate a doubtful pneumothorax.
2. Expiratory films are necessary to confirm/rule out air-trapping.
3. The main causes of air-trapping are central bronchial obstruction and peripheral small airway disease.


None of the above. Klebsiella pneumonia with cavitation and bulging fissure sign.
Why did the fissure was in the same location two years earlier?
Pneumocystis
Tb
TB
Bulging fissure and cavitations suggest Klebsiella.
However, two year-old lesion flaring up sounds more like TB!
Tuberculosis – old cavity is the source, lobar spread speaks against staph. Pneumocystis would have more spectacular anamnesis.
….pazza idea…..BOOP, da tossicità polmonare all’abuso di farmaci….
First – it is important to persue the right lateral radiograph to see the type and precise localisation of pathology spread.
On two year chest radiograph:
1. there is no evidence of pulmonary vessel system pathology in both lungs
2. in the lungs there is the evidence of peribronchovascular component, better vizualised in the right lung, especially in medioinferior lung fields, where also is seen the approaching of all the main components of architectonics, what could be the hypoventilation of right medius and/or inferior lung lobus.
Besides on the level of 2-3 anterior intercostal space there is local shadow of peribronchovascular homogeneous component with partly good and ill-defined margins. There is no evidence of nodulal opacities in both lungs.
3. The right hila shows the initial sign of deformation due to peribronchovascular component. There is no evidence of bronchopulmonary lymphadenopathy.
4. From the level of anterior part of 3 rib in prehilar zone to the level of 6 rib layerally, mostly near the lateral chest wall there is thin line probably the shadow of interlobar pleura, which should be seen on the level of 3 rib – in this case it is lower (it could be because of hyperventilation of right lobus superior because of hypoventilation of middle/inferior lobus or on the contrary).
Both costophrenic angles and both lung apex are not seen and couldn’t be analised. There is no evidence of soft tissue pathology.
New chest radiograph:
In addition to previous features, there is inhomogeneous lung parenchyma shadow on the level from anterior parts of 1 to 5 ribs, mainly in lateral zone and partly in prehilar. the superior part of this shadow is more inhomogeneous and the lower part shows lung consolidaion. On the level of 1st rib there is suspicion of cavitation. And it is not seen the right hilar shift due to TB process. There is no evidence of left lung involvement (nodular pattern, consolidation, cavitation etc).
Staph Pneumonia usually involves lower lobes.
According to patients anamnesis – drug abuser – it should be HIV/AIDS suspicion.
If supposing HIV possitive, the chest pathology could be TB, but it do not look like typical TB in such patients (though – for TB it is typical right-sided, and there should be a little signs of transbronchial spread of TB in the left lung due to big lesion in the right lung).
It should be make differential diagnosis also with Pneumocystis pneumonia – but this could be excluded – it has typicall bilateral spread and it could be Legionella Pneumonia – patchy, peripheral, nonsegmental consolidation initially unilateral and confined to one lobe, but there is no unformation of transplantant operation.
If HIV-negative – TB
Dear Olena, I am impressed by your thoroughness.You deserve some help. Imagine that you are looking only at the previous film. What would you think?
Thank You!
Ok. First af all, I’m not sure that the normal possition of the patient while performing radiograph was hold, because I didn’t see the trachea gap in the middle, and there is additional gap (like trachea) but in paramediastinal right side on that level. And I didn’t see normal anatomical airways division in the right hila because of mentioned earlier peribronchovascular component.
Remarkable is the right lung parenchyma, which shows poor peripheral vascularity throughout the lung area and decreased lung vascularity in the right lobus superior and paramediastinally over the diaphragm – “Parallel” or “divergent” patterns of vascular reorientation – the evidence of right lobus inferior atelectasis and due to this mentioned shift down of minor fissure.
The both lung apex can not be analised, what is important, because there could be signs of old inflammation process.
The most problem is that shadow on the level of anterior part of 2 rib – it seems that there is some nodular pattern or it is the aggregation of smaller nodulus in secondary pulmonary lobule, because it seems that there is a gap of bronchi in the middle of that pattern and some vessel shadows peripherally this nodul.
It is solitary lesion and differential diagnosis is wide – tuberculoma, mts, sarcoidosis, Wegener’s granulomatosis, peripheral cancer, fungi lesion, aspergilosis – the two last are also typical for drug abusers.
It looks like this process is chronic/long lasting in this patient.
That is what I think.
and also I think that there could be pleural reaction on inflammation in right lobus superior
Tb
i think its none of the above.
===if v c the two yrs old xray it is just showing small cavitating lesion in right mid lung zone which has increased in number in new xray—-considering its multiplicity and the H/O IV drug abuser these favor the septic emboli.
===Regarding opacifiction of the right upper and mid zones it seems to be superadded consolidation which can be any organism which IV abusers are prone to.But not specifically klebsiella or staph because the fissure which seems to be bulging by consolidation is in actual at the same position as was 2 years ago. And this bulging position of fissure 2 years ago seems to be due to emphysematous changes in the lung which IV abusers are also prone to develop.
Also consider that drug abusers may have processes unrelated to their addition.
Ya differentials include. TB and staph
I would say that there is underlying bronhihal atresia which was complicated later on.
Good for you! I declare you the winner!