Dr. Pepe’s Diploma Casebook: Case 87 – SOLVED!
Dear Friends,
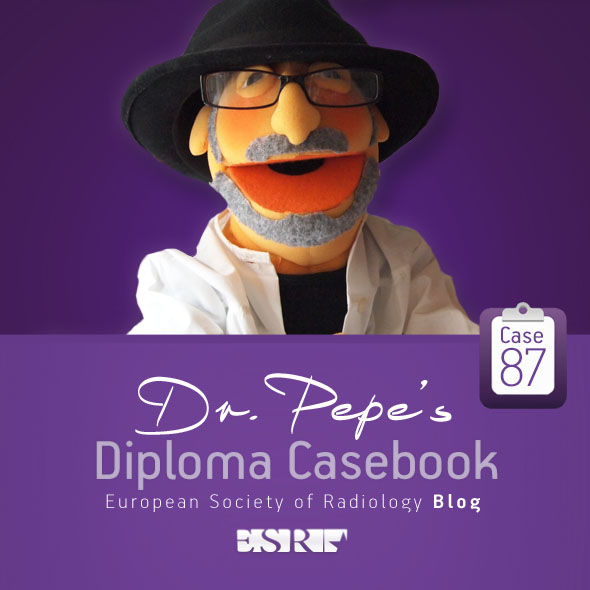
Today I am presenting radiographs of an 83-year-old woman who has had a cough and fever for the last four weeks.
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
Diagnosis:
1. Acute RML pneumonia
2. RML syndrome
3. RML neoplasm
4. Any of the above
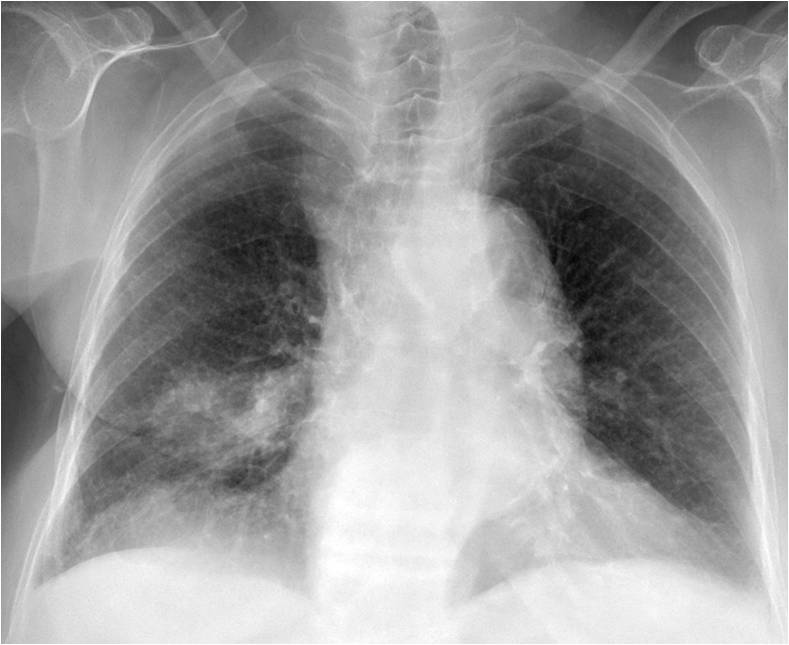

Findings: PA radiograph depicts air-space disease in the RML (A, arrow). The lateral view shows the typical triangular appearance of RML collapse (B, white arrows), with a widening of the proximal aspect (Golden’s sign) suggesting a central mass (B, red arrow). There are also multiple compression fractures of the spine.
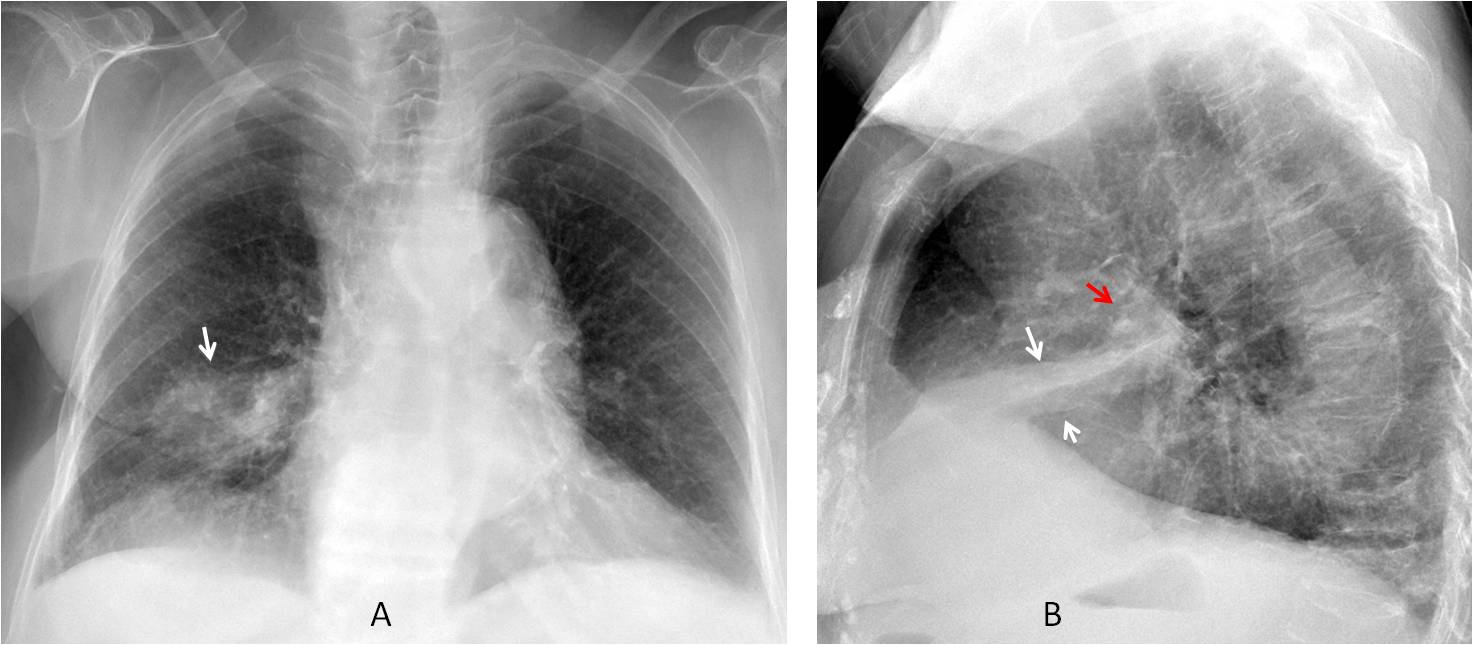
Golden’s sign was overlooked and the patient was treated for pneumonia. Five months later the proximal mass was larger (C, arrow). Unenhanced CT shows the mass (D, arrow), confirmed to be malignant at bronchoscopy.
Final diagnosis: RML collapse secondary to endobronchial carcinoma.
The reason for presenting this case is to discuss RML collapse. Whereas the majority of lobar collapses are secondary to a malignant endobronchial tumor, in my experience RML collapse is most commonly due to non-malignant causes, usually inflammatory disease.
The small size of the lobe and the lack of permeability of the limiting fissures hinders collateral ventilation from the adjacent lobes, resulting in a loss of volume regardless of the patient’s disease. Because of this monotonous response to different conditions, I find it difficult to elaborate on RML collapse. For this reason, I am focusing this presentation on two main points:
1. Diagnosing RML collapse
2. Discussing the most common causes
RML collapse has a nondescript appearance in the PA view. Due to the lobe’s small size, collapse is not accompanied by secondary signs, other than fissure displacement.
The lateral view is needed to reveal the loss of volume, indicated by the close proximity of the minor and major fissure (Fig. 1). The necessary conclusion is that the lateral view is indispensable to diagnose RML collapse.
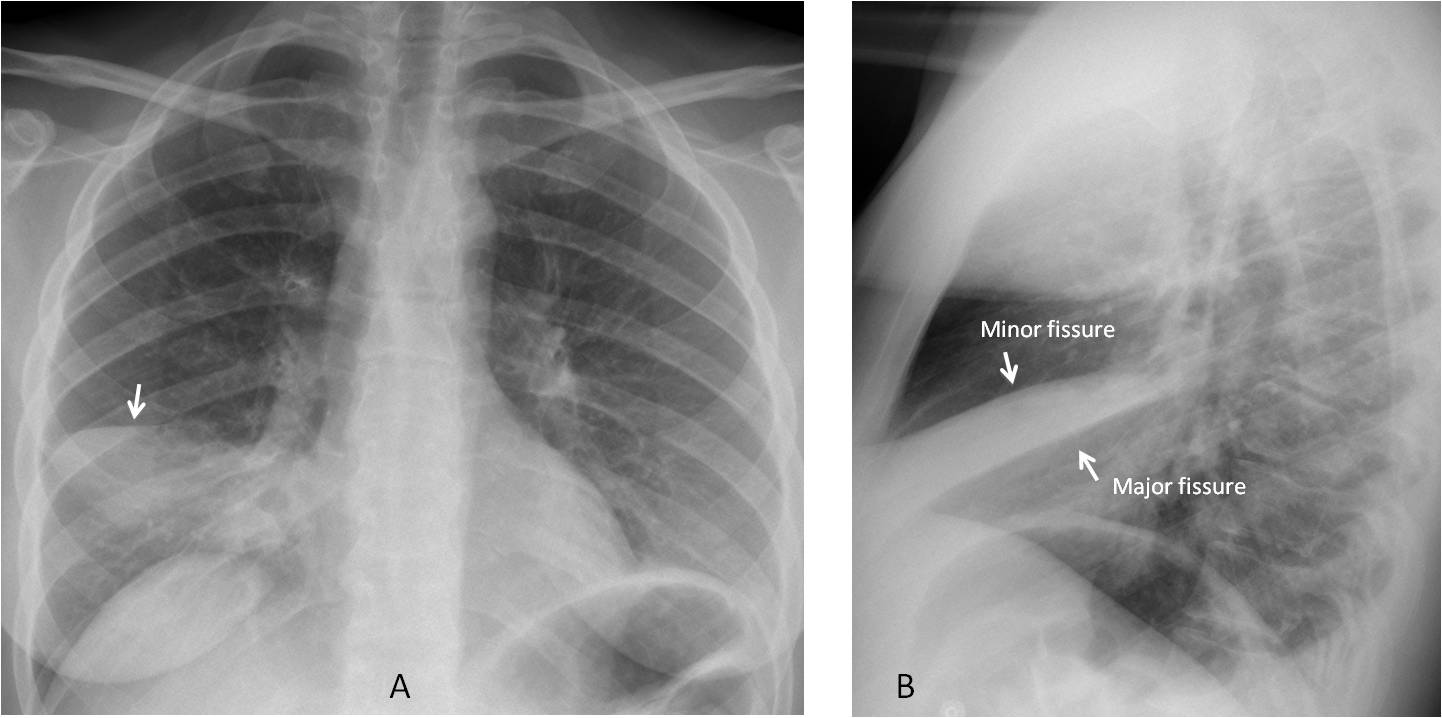
Fig. 1
Fig. 1: RML pneumonia seen as air-space disease in the PA view. The minor fissure is descended (A, arrow). The lateral view shows the typical triangular appearance of RML collapse (B).
The importance of the lateral view is emphasized by the fact that RML collapse can be nearly invisible in the PA view, only suspected because of some blurring of the right heart border (Figs. 2 and 4).
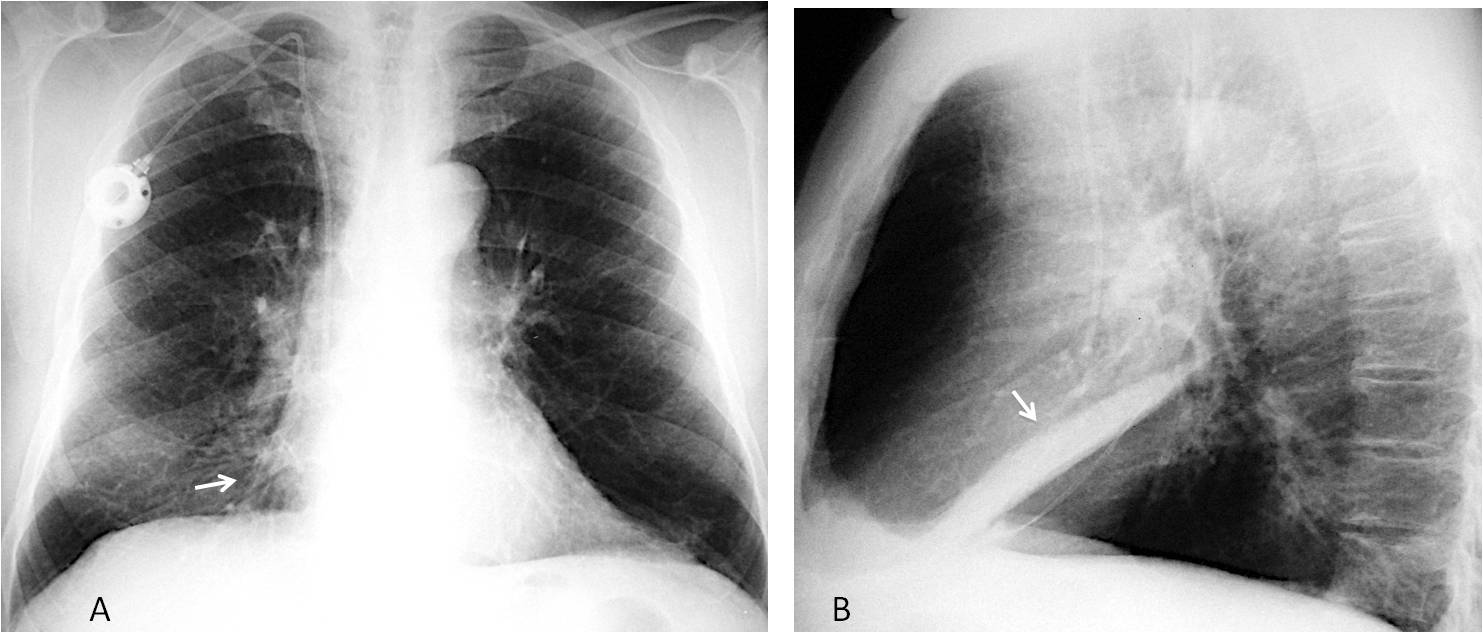
Fig. 2
Fig. 2: Chronic RML collapse is only visible in the PA view as slight blurring of the right heart border (A, arrow). The lateral view confirms RML collapse (B, arrow).
Determining the etiology of RML collapse is difficult on chest radiography. The three most common causes are
1. Acute pneumonia
2. Chronic inflammatory disease (RML syndrome)
3. Carcinoma
CT is helpful in chronic cases, but not always diagnostic. Bronchoscopy should be done when an endobronchial lesion is suspected.
Acute RML pneumonia may be patchy, but can affect the entire lobe, causing volume loss (Fig. 3). The clinical symptoms favor an acute condition. Clearing after adequate treatment confirms the diagnosis (Fig. 4).
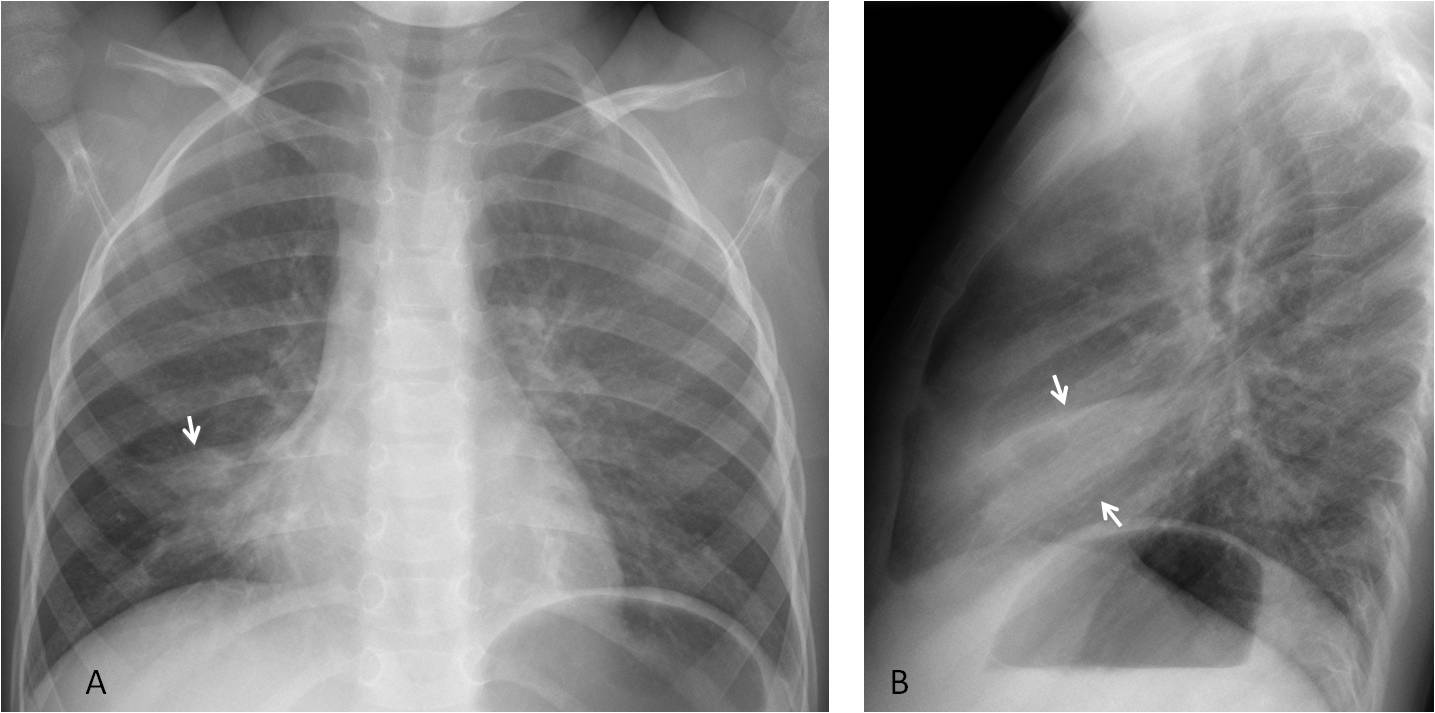
Fig. 3
Fig. 3: Five-year-old boy with acute pneumonia. Note the descended minor fissure in the PA view (A, arrow) and loss of volume of the lobe in the lateral view (B, arrows).
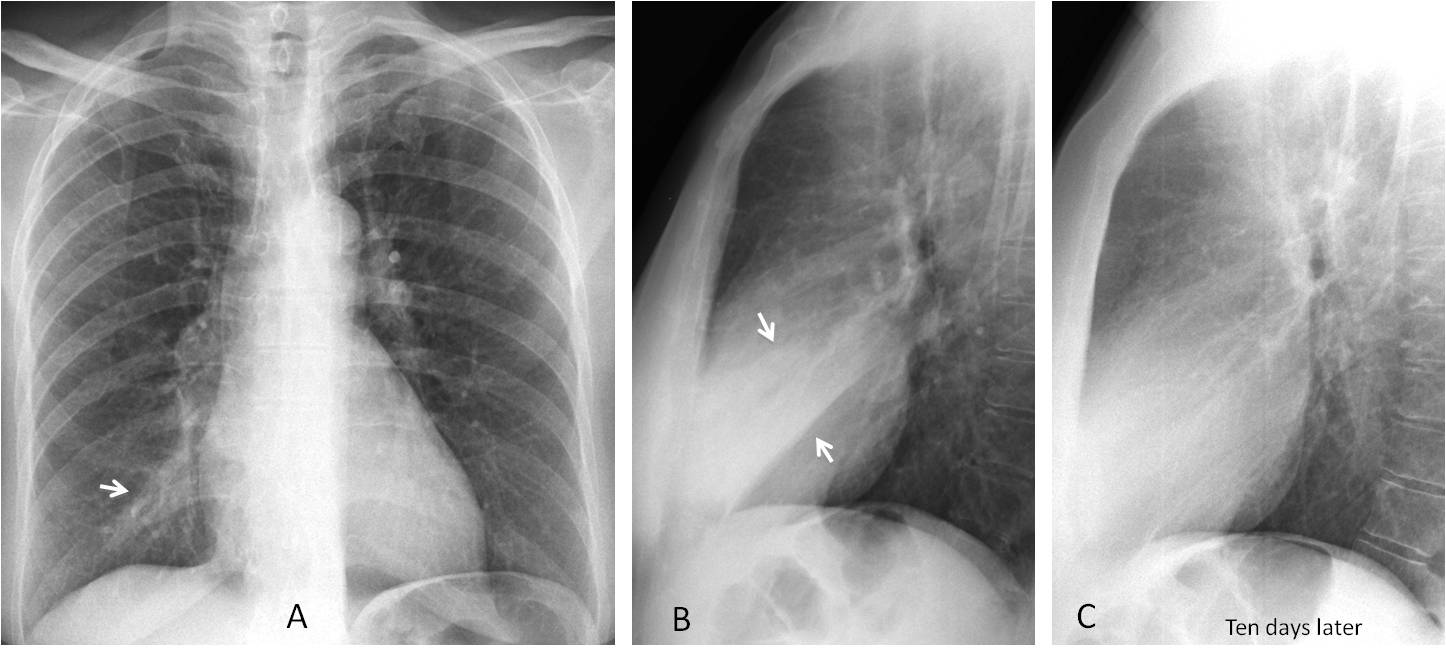
Fig. 4
Fig. 4: Acute pneumonia is barely visible in the PA view (A, arrow). The lateral view shows it clearly, with loss of volume of the RML lobe (B, arrows). Ten days later the pneumonia has cleared (C). This case proves that even large RML infiltrates may be overlooked in the PA radiograph.
Chronic RML collapse (RML syndrome) is usually caused by previous inflammatory disease aggravated by the poor drainage of the lobe. It results in bronchiectasis, easily seen on CT (Fig. 5). If an endobronchial lesion is suspected, bronchoscopy should be done (Fig. 7).
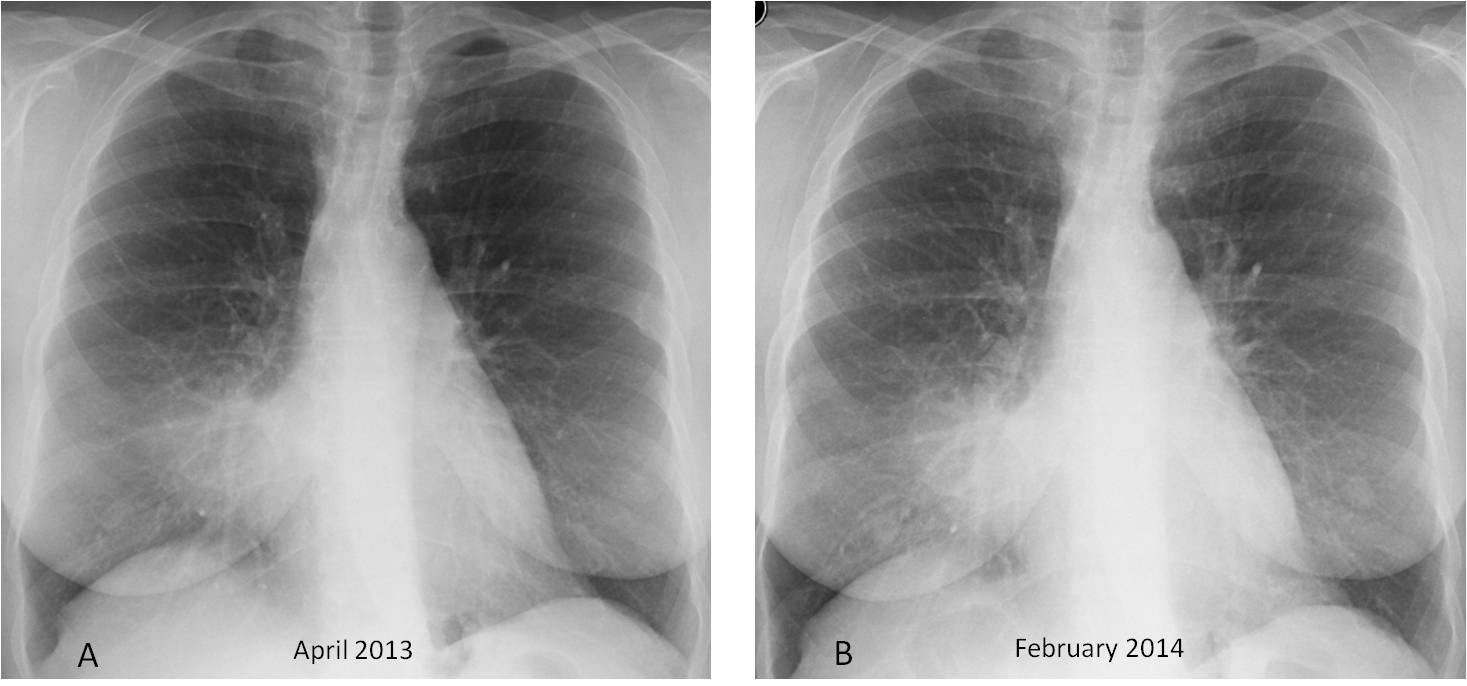
Fig. 5
Fig. 5: 59-year-old woman with RML syndrome. Radiographs taken 10 months apart show no change in the infiltrate (A and B, arrows).
The lateral view demonstrates the RML volume loss (C, arrows). Enhanced sagittal and axial CT images show dilated bronchi filled with air and mucus (D and E arrows). Bronchoscopy showed RML bronchomalacia.
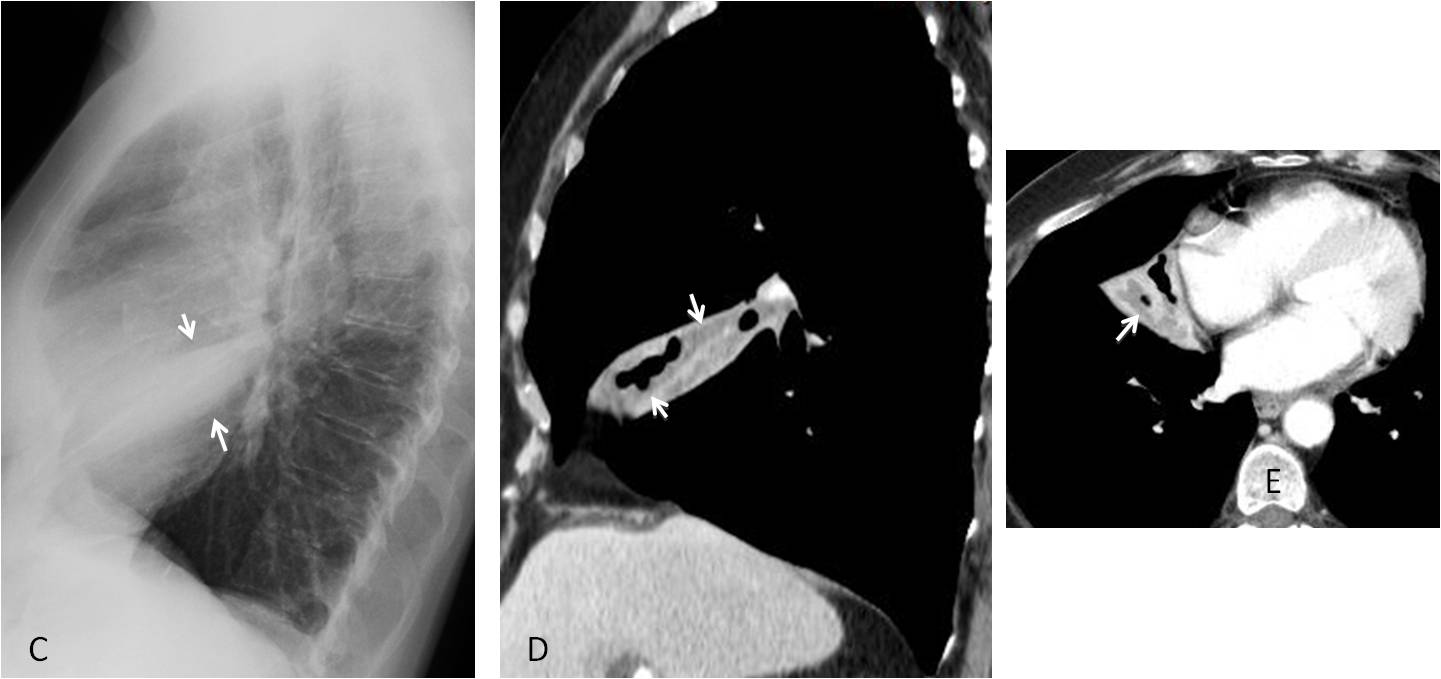
Fig. 5
Occasionally, RML syndrome may be due to foreign bodies lodged in the RML bronchus causing chronic collapse. Low-density foreign bodies may go unrecognized on CT images, and bronchoscopy is necessary to establish the diagnosis (Fig. 6).
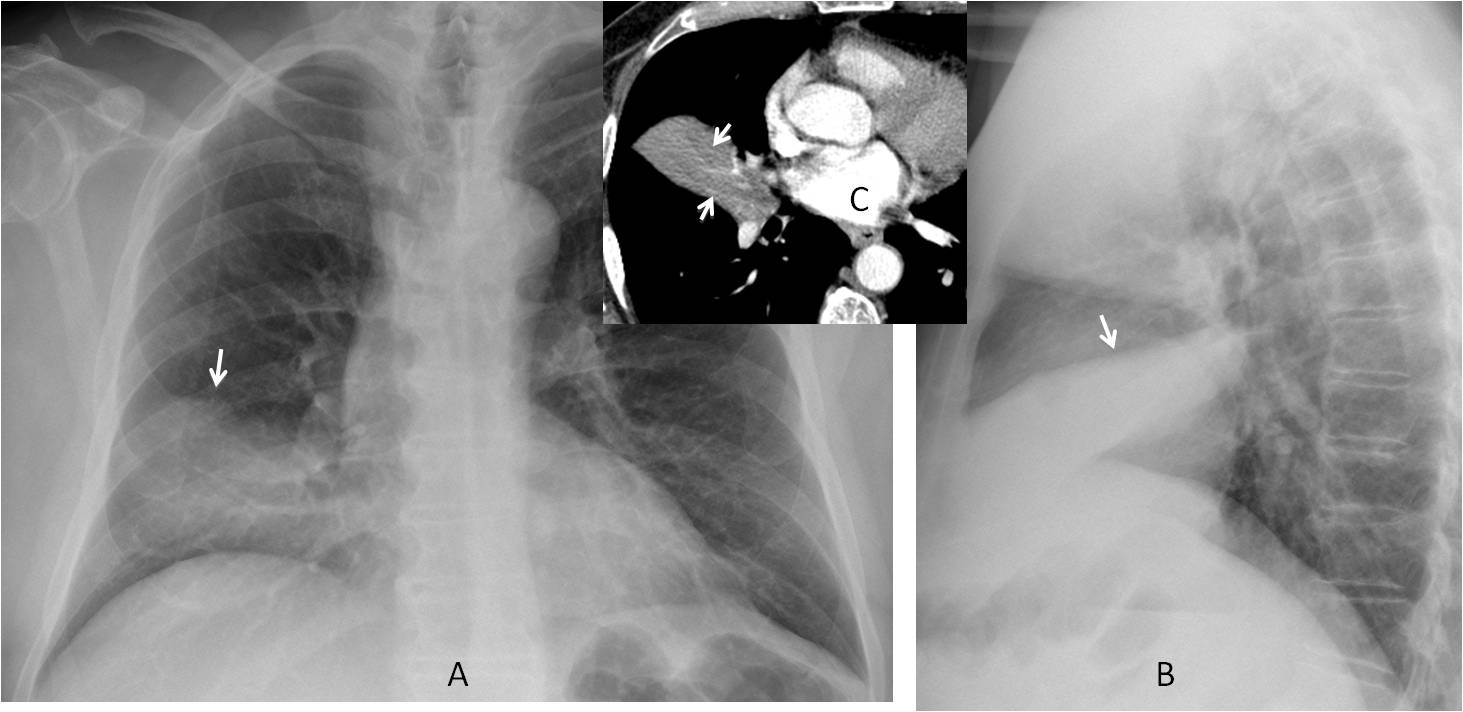
Fig. 6
Fig. 6: 71-year-old man with chronic RML disease. Chest radiographs show moderate RML collapse A and B, arrows) . Enhanced axial CT demonstrates a collapsed lobe with a mucus bronchogram (C, arrows). At bronchoscopy, a pea was found in the RML bronchus.
Broncholithiasis, a rare cause of RML syndrome, is easily identified on CT and sometimes visible in the plain film (Fig. 7). Broncholiths occur in patients living in areas where granulomatous disease of the lymph nodes is prevalent (TB, fungal infection, silicosis).
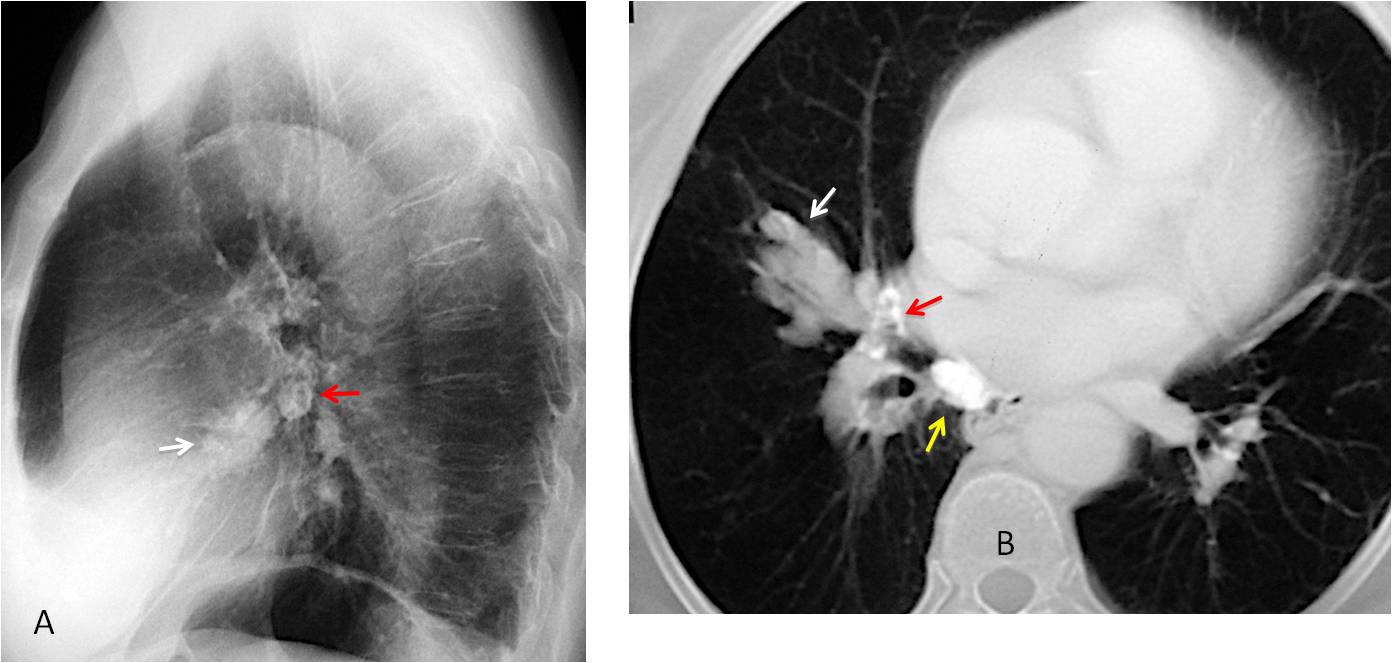
Fig. 7
Fig. 7. 72 y.o. man with a history of TB and chronic RML disease. Lateral chest film shows a nodular shadow in the RML (A, white arrow) and calcified lymph nodes in the hilum (A, red arrow). Axial CT depicts a RML mucous impaction (B, white arrow), with proximal calcifications (B, red arrow) and a calcified mediastinal lymph node (B, yellow arrow). Broncholithiasis was confirmed at bronchoscopy.
In my experience, carcinoma is less common than inflammation as a cause of RML collapse. Carcinoma should be suspected when the disease progresses (Fig. 8). CT and bronchoscopy are confirmatory. As was seen in the initial case of this presentation, discovery of a central mass (Golden’s sign) is highly suspicious for malignancy (Fig. 9).
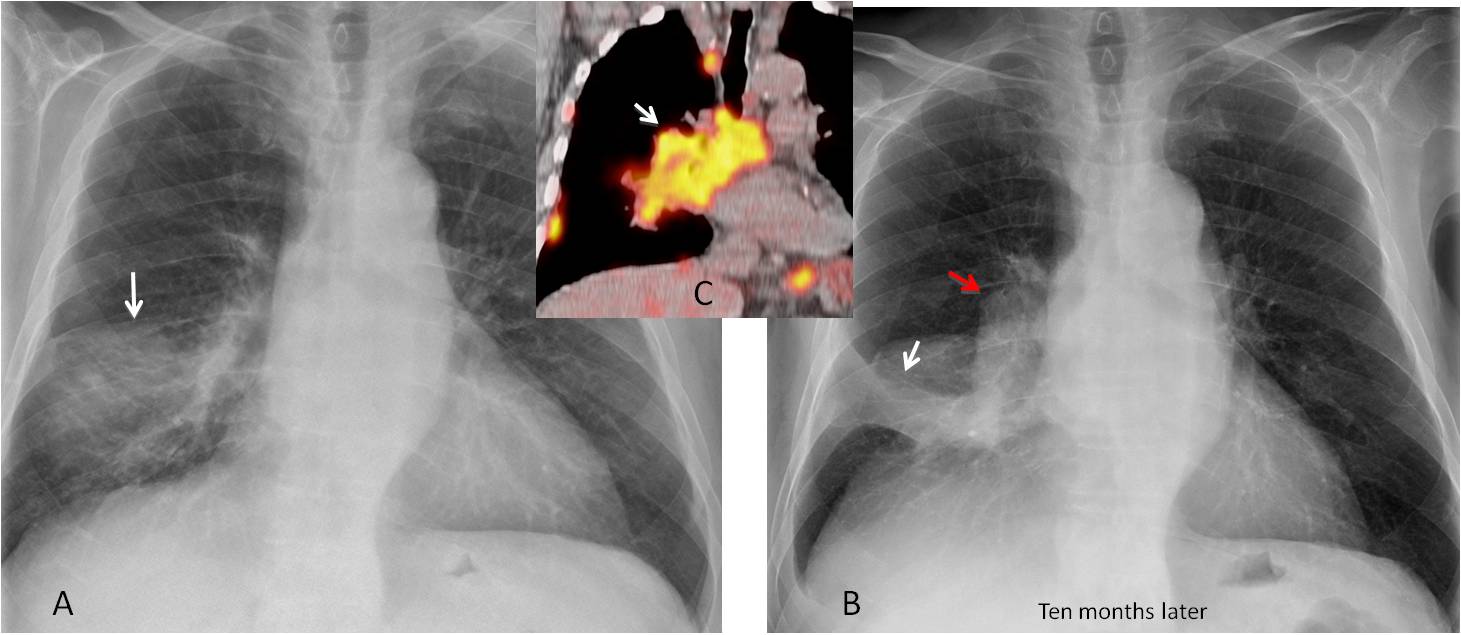
Fig. 8
Fig. 8: 81-year-old man with RML disease (A, arrow). Ten months later the lobe is collapsed (B, white arrow) and there is a mass in the right hilum (B, red arrow). PET-CT shows a large hilar and mediastinal mass (C, arrow). Diagnosis: carcinoma.
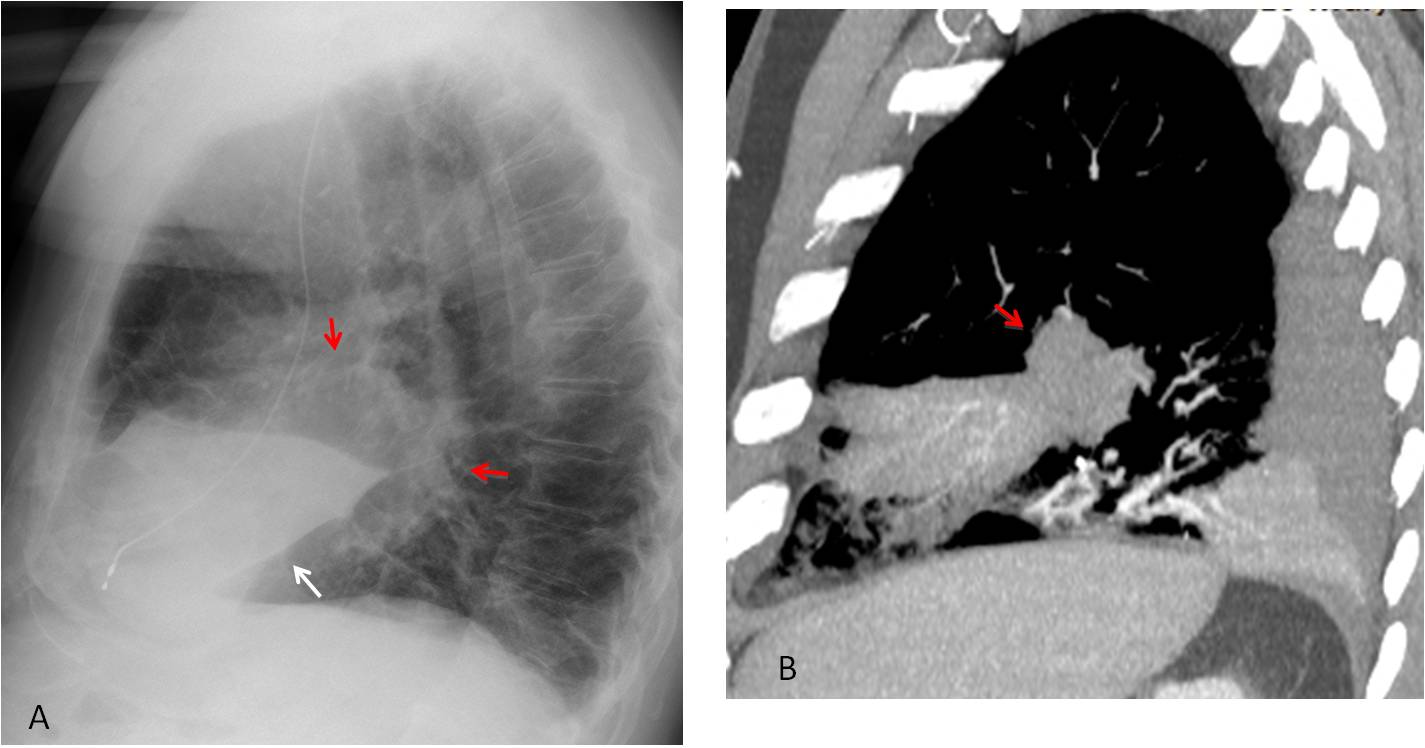
Fig. 9
Fig. 9: Golden’s sign in carcinoma. Lateral view shows moderate RML collapse (A, white arrow) and a large mass at the apex (A, red arrows). Enhanced sagittal CT confirms the presence of a mass at the origin of the RML (B, arrow).
Since this presentation is not very glamorous, I want to end with a bonus case: An unusual peripheral adenocarcinoma that grew into the RML, ending up as a swollen lobe (Fig. 10).
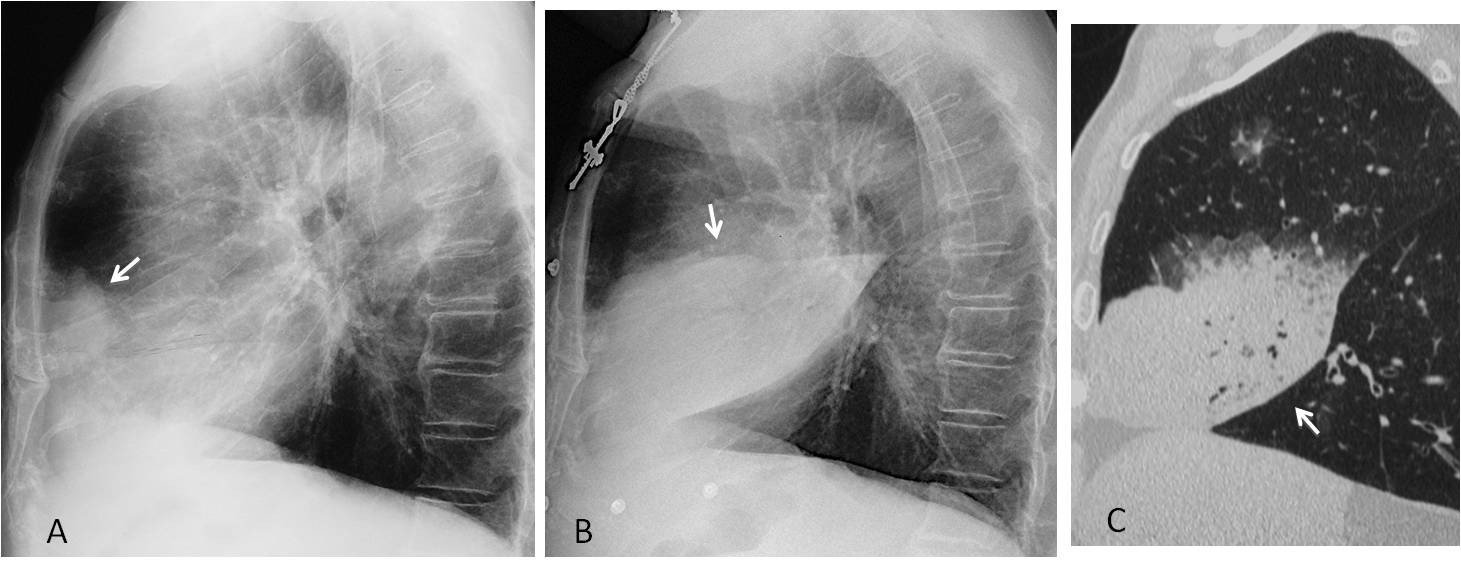
Fig. 10
Fig. 10: Peripheral RML adenocarcinoma that was overlooked initially (A, arrow). One year later the tumour has grown and infiltrated the whole RML (B and C, arrows).

Follow Dr.Pepe’s Advice:
1. The lateral view is indispensable to diagnose RML collapse.
2. The three main causes of RML collapse are acute pneumonia, RML syndrome, and carcinoma.
3. In RML syndrome, bronchoscopy is needed to exclude an endobronchial lesion.


2
1
Suspected pneumonia
2
2
Laconic, all of you!
RML syndrome + RLL pneumonia + aortic aneurism
There are age changes in the lung parenchyma – diffuse sclerosis, and also peribronchovascular component due to inflammation, or lymphogenous spread of neoplasma – canceromatosis ? Aorta deviation in arcus aortae, aorta thoracica and aterosclerotic changes in aorta, the increased volume of heart ventriculus/atrium left (?). Trachea deformation.
On the right in the right hila projection, more laterally, – increased lung attenuation – lung parenchyma consolidaiton, but according to lateral view – it seeems right middle lobe syndrome (infiltration, atelectasis). Besides, on lateral view suspicion on pleural inflammation reaction with probable start of pleural effusion. Or it could be also pleural fibrosis due to old pleuritis.
According to that that this is woman – there is no usual both mammae visualization – it could be normal due to age involution, and the shadow of both mammae is beyond FOV or there could be some technical reasons while performing this chestXray (the position of mammae), but it seems like there is no left mammae – maybe, mastectomy ?. If yes, the changes in lung could be neoplastic – mts? with postobstruction pneumonia.
There is additional shadow on the right chest wall above lateral sinus – it looks like soft tissue mass in chest wall – mesothelioma? which explains probable pleuritis. But the shadow of soft tissue which starts on lung field and follows beyond the chest wall is questionable – it could be right mammae partly resection – the likely shadow could not be seen symmetrically on the left. But on lateral view there is the shadow of mammae so this confuse.
There are fish-like vertabrae defformation, on the lateral view, especially the one opposite the hila projection – age degenerative distrophic bone changes.
It seems like there is combination of these three proposed options – because the right middle syndrome could be the result of RML neoplasm with postobsrtuctive pneumonia with lung canceromatosis.
4
Rationale:
Opacity right base obscuring right heart border = RML penumonia
Opacity right perihilar region with irregular margin, ? narrowing right bronchus intermed
Atelectasis pulling right dome upwards anteriorly
Vertebral collapse at multiple levels.
Right sided subpulmonic effusion?
…ci sono due patologie distinte……una è l’atelettasia del lobo medio, visibile in LL….l’altra è la patologia visibile in AP in cui non vi è il segno della silhouette ma patologia della porzione posteriore del polmone….si associano fratture vertebrali, da osteoporosi….
I think that the silhouette sign is missing because the RML collapse is severe.
Vertebral fractures were due to ospeoporosis.
if the vertebral compressions are all degenerative, then 2, if the cystic structures are bronchiectasis.
but margin of right perihilar opacity too irregular to exclude ca
CT?
4