Dr. Pepe’s Diploma Casebook: Case 89 – SOLVED!
Dear Friends,
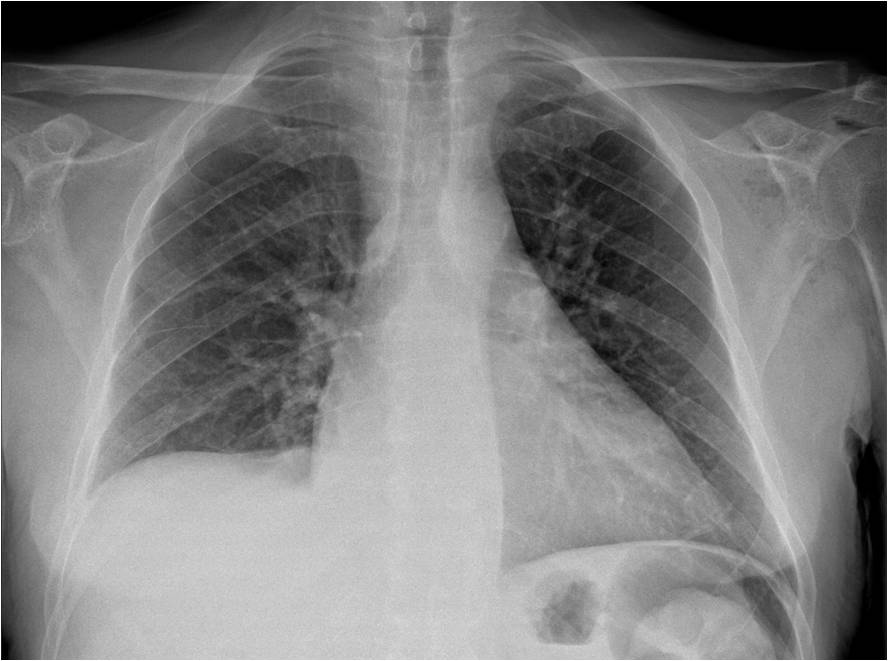
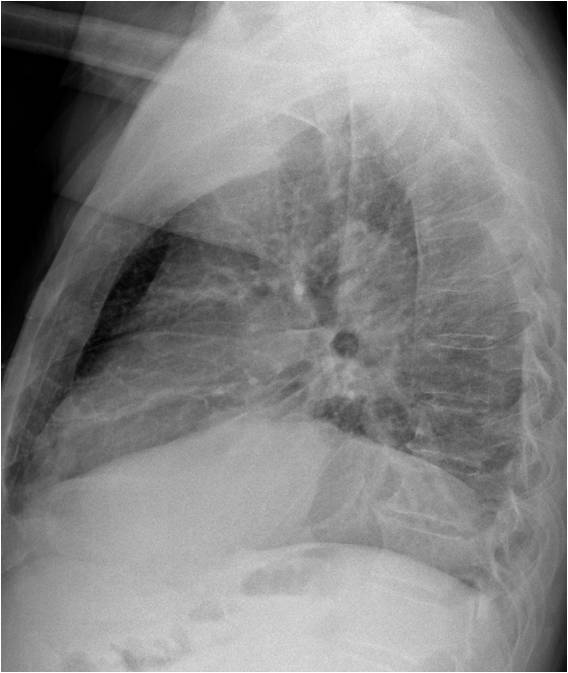
This week we are presenting radiographs of a 42-year-old diabetic man with chest pain and fever. What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
Findings: There are pockets of gas in the left shoulder (A, circle). Cone down view shows air within the shoulder joint (B, white arrows) and soft tissues of the arm (B, red arrows).
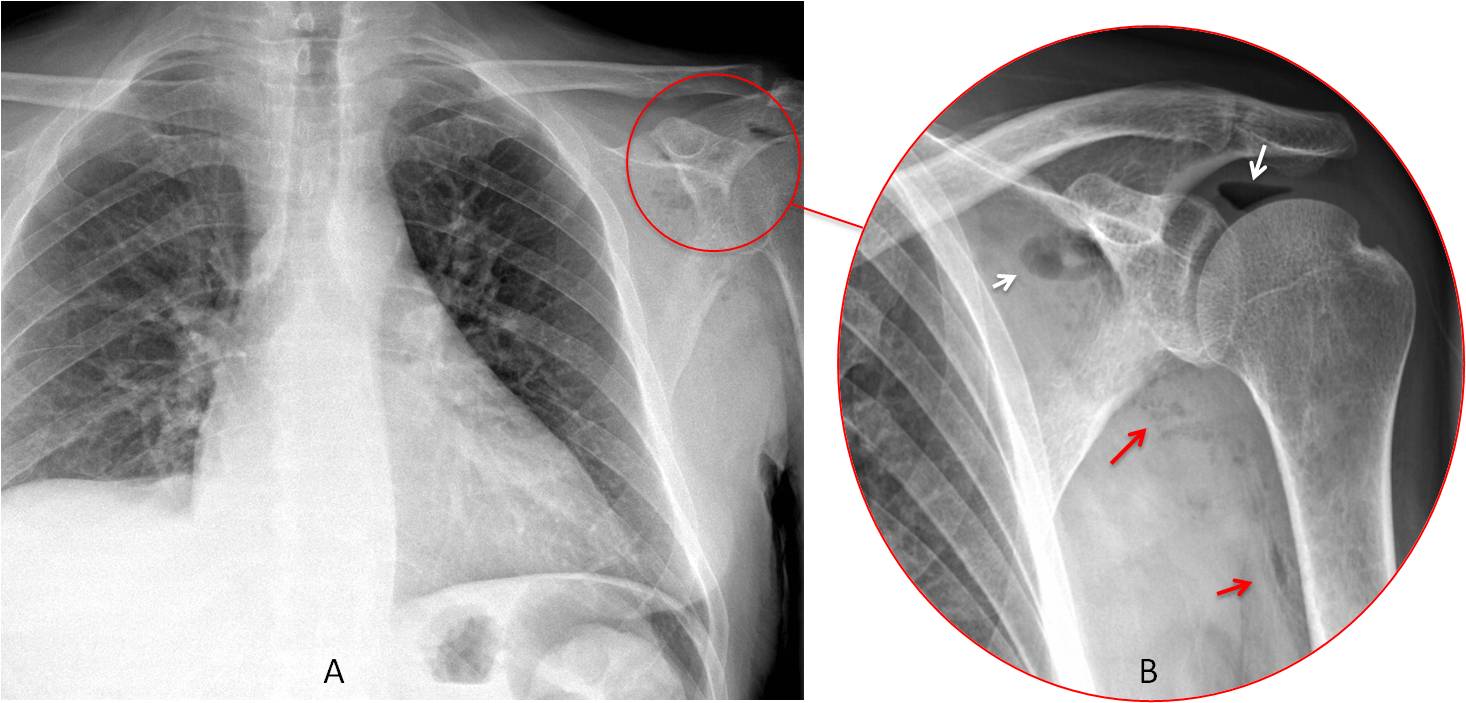
Final diagnosis: Septic arthritis of the left shoulder.
Our teachers always told us to “look at the corners of the film”. In this presentation I would like to talk about the upper corners, which include the shoulder structures. Significant disease may be overlooked by failing to examine these areas. In almost all cases, abnormalities in or around the shoulder are only visible in the PA film.
One or both shoulders are visible in most PA chest radiographs. The bone structures are well depicted: the articular ends of the AC joint should be aligned, with a maximum separation of 3mm. The glenohumeral joint usually appears distorted because of the oblique positioning of the arms. Most of the scapula is visible, as well as the surrounding soft tissues (Fig. 1).
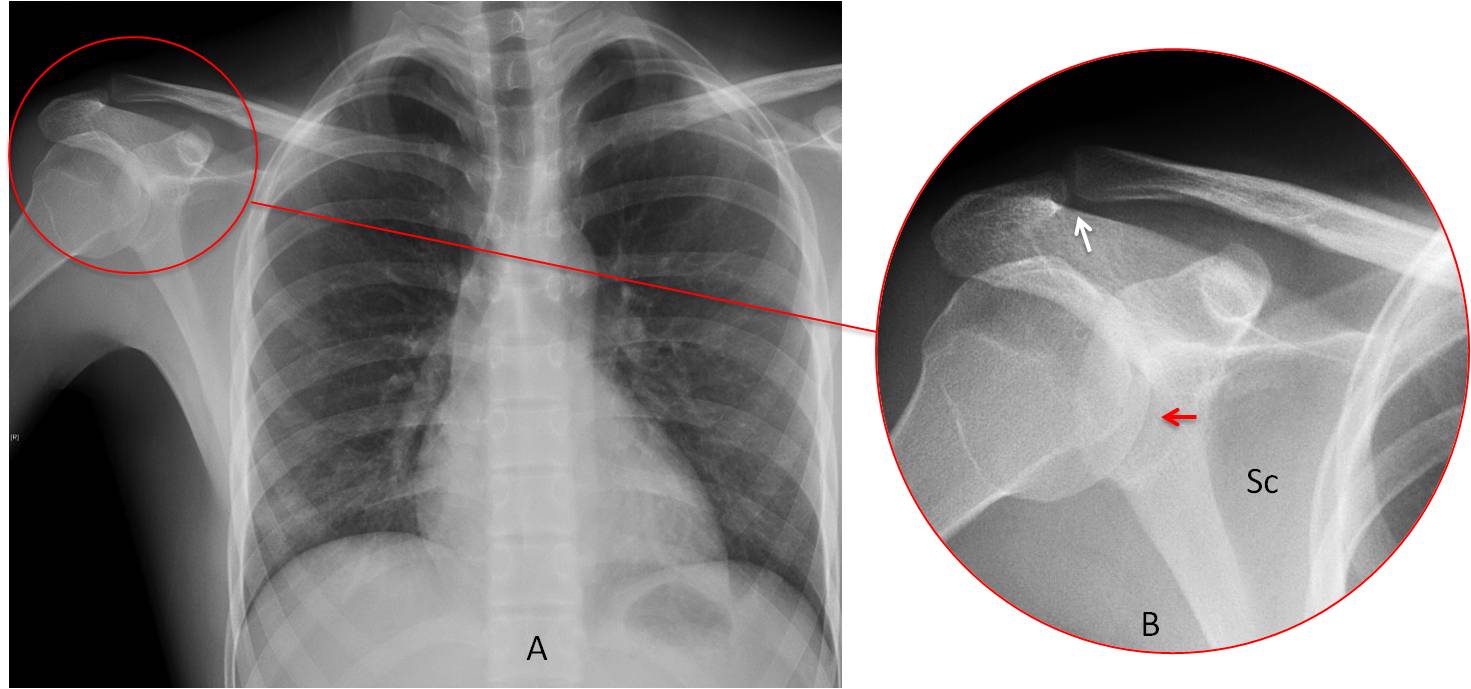
Fig. 1
Fig. 1. Normal shoulder, as seen in the PA chest radiograph (A, circle). The main bone structures are the AC joint (B, white arrow), the glenohumeral joint (B, red arrow) and part of the scapula (Sc).
Most conditions affecting the shoulder and visible in the chest radiograph are either degenerative or traumatic. They may be classified as:
1. Soft tissue calcifications
2. Post-traumatic findings
3. Miscellaneous conditions
Soft tissue calcification is a relatively frequent finding. The most common site is the supraspinatus tendon, detected at the upper border of the humeral head (Fig. 2). This calcification occurs mainly in middle age and can be very painful. Cone down views of the shoulder should be taken to verify the finding. A previous film may be all that is needed for confirmation (Fig. 3).
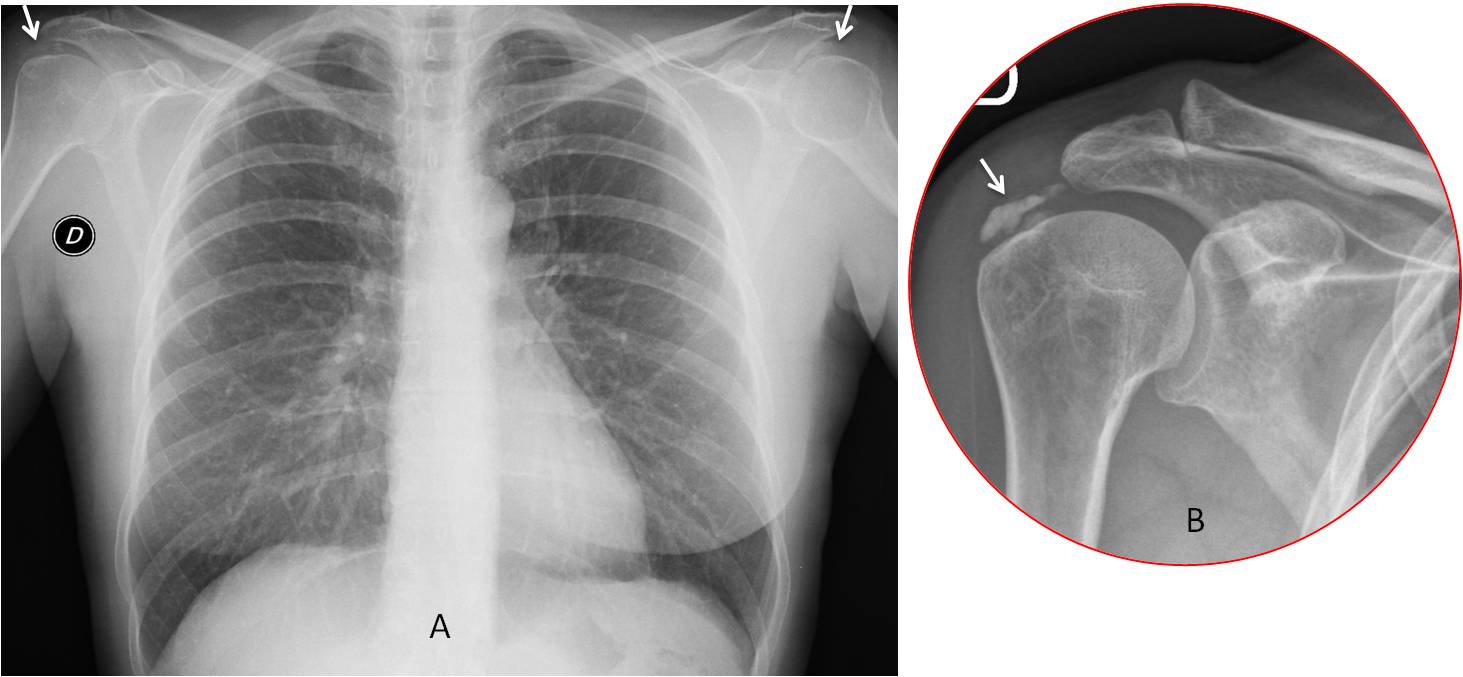
Fig. 2
Fig 2. Bilateral calcific tendinitis detected in the chest radiograph (A, arrows). Cone down view of the right shoulder clearly shows calcium in the rotator cuff (B, arrow).
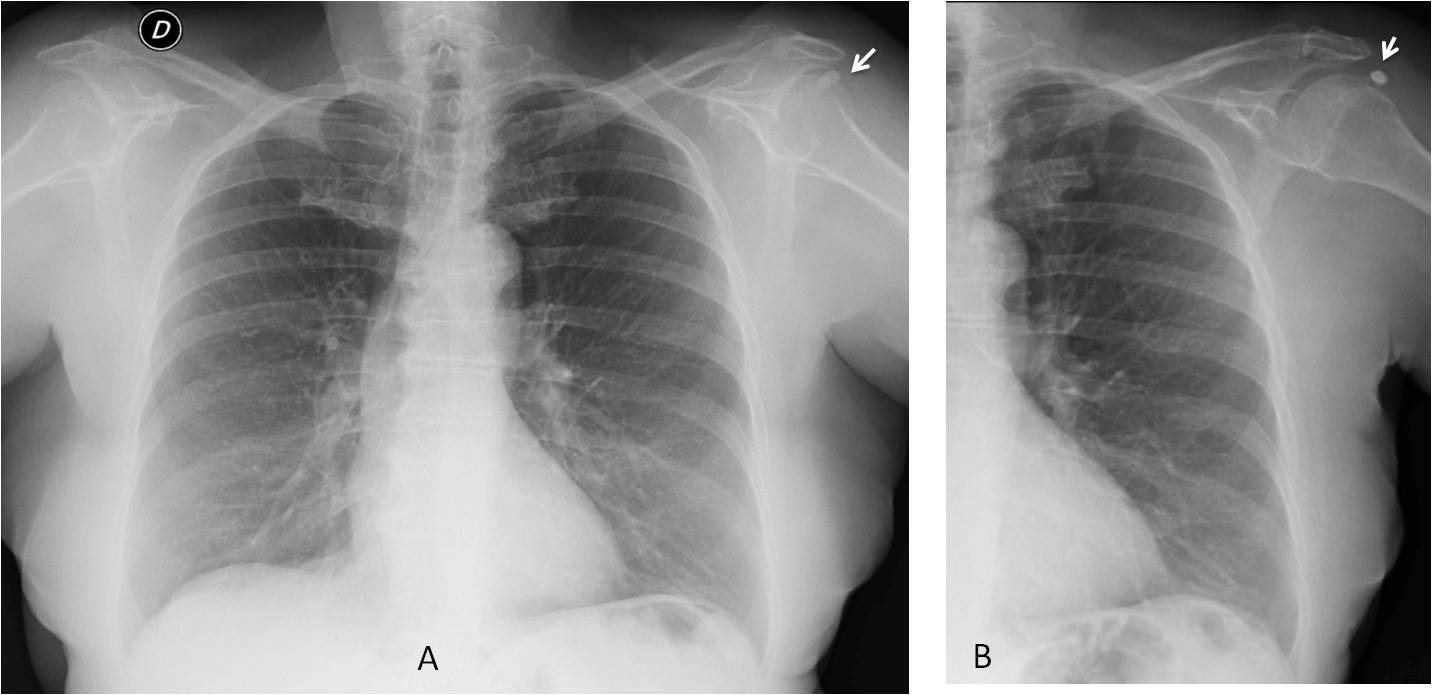
Fig. 3
Fig. 3. Calcific tendinitis of the left shoulder (A, arrow). A previous chest film confirms that the calcium is in the soft tissues (B, arrow).
Synovial chondromatosis is a benign condition characterized by multiple, loose, intra-articular bodies. When chondromatosis affects the shoulder, it appears as multiple rounded calcifications around the shoulder joint (Fig. 4).
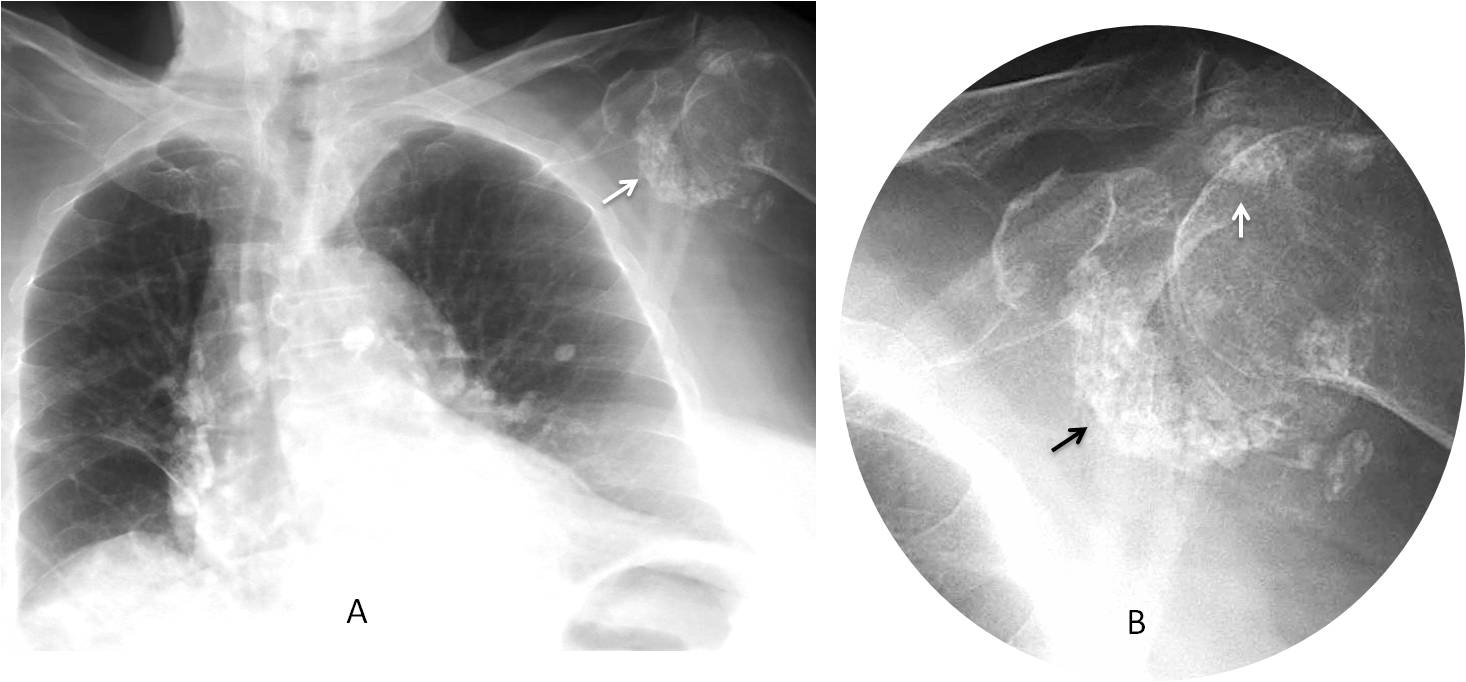
Fig. 4
Fig. 4: 85-year-old woman with synovial chondromatosis of the left shoulder (A, arrow). Cone down view shows the multiple loose bodies in the joint to better advantage (B, arrows).
Shoulder calcifications should not be confused with metal material used in surgical repair of shoulder instability. Recognising the obvious metal density is the clue to a correct diagnosis (Fig. 5).
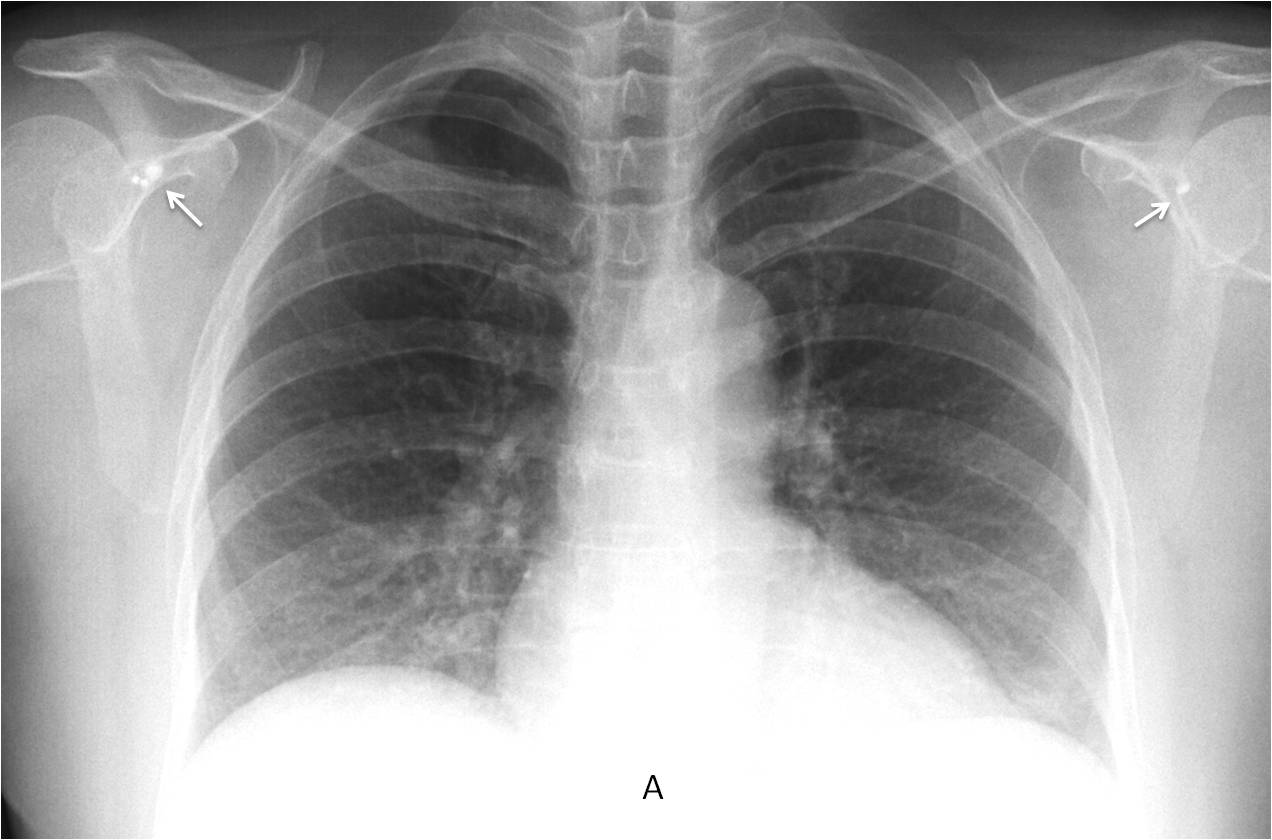
Fig. 5
Fig. 5: 43-year-old woman after surgical repair of shoulder instability. Note the metal devices in both shoulders (A, arrows).
The shoulder joint is prone to acute trauma, and the chest radiograph may detect associated fractures that are not suspected on clinical examination (Fig. 6).
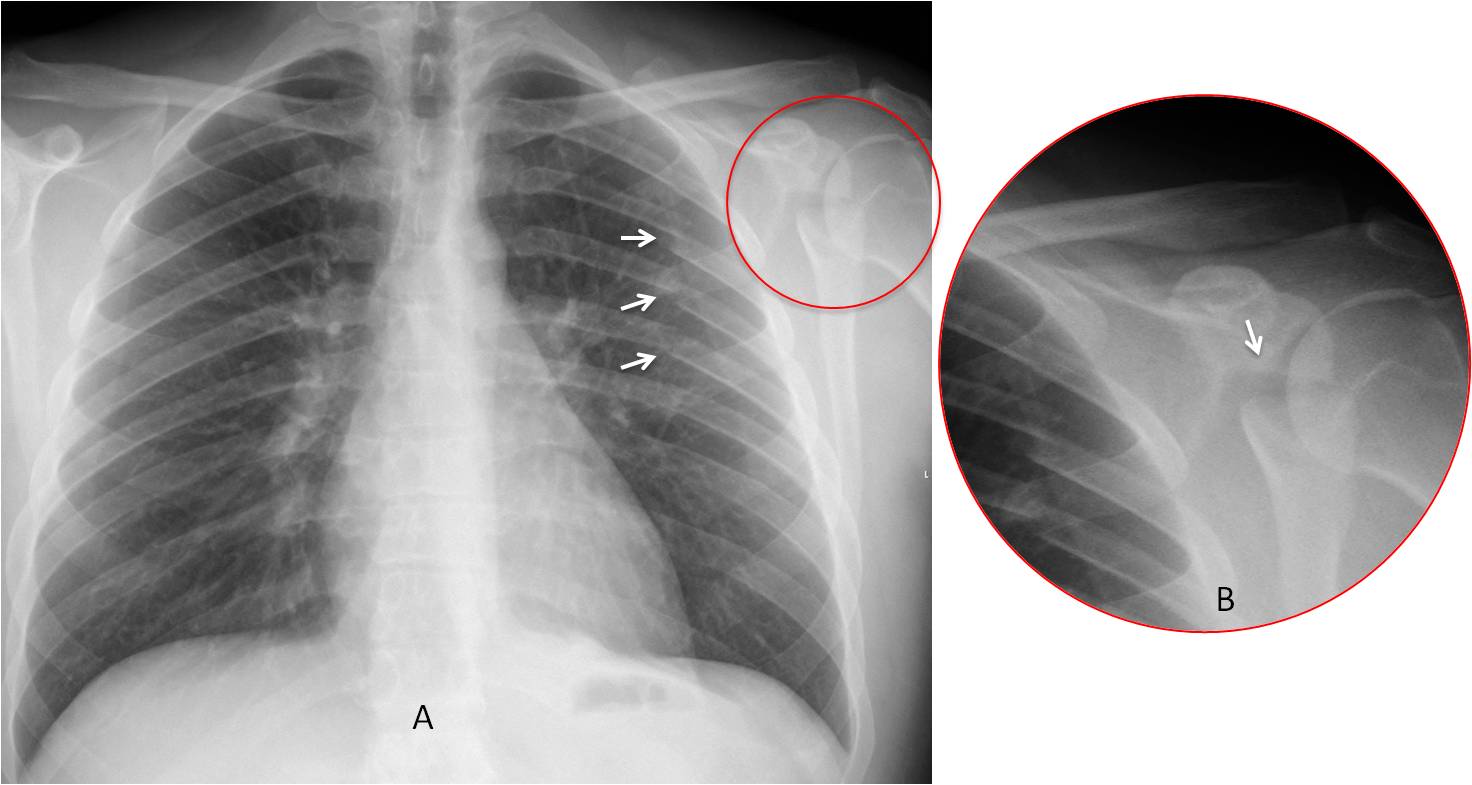
Fig. 6
Fig. 6: 38-year-old man after a car accident. PA radiograph shows several rib fractures (A, arrows) and a transverse scapular fracture (A, circle), better seen in the cone down view (B, arrow).
The chest radiograph may also detect chronic post-traumatic lesions such as non-united fractures or recurrent dislocation (Fig. 7).
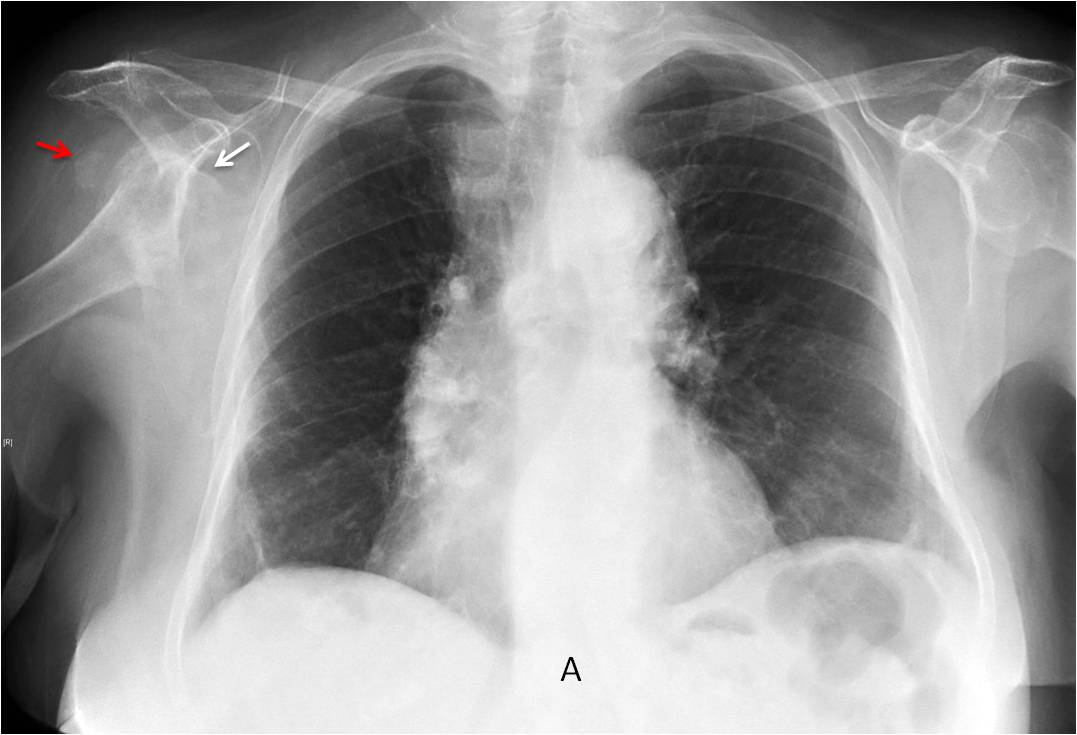
Fig. 7
Fig. 7: 76-year-old woman with recurrent anterior shoulder dislocation after trauma. PA view shows the dislocated shoulder (A, white arrow) and a loose body in the joint (A, red arrow).
AC dislocation is a common post-traumatic sequela, often overlooked in the acute phase if other more serious fractures are present. It can be asymptomatic and detected in subsequent chest radiographs (Fig. 8). Remember that a significant number of these dislocations are associated with rotator cuff injury.
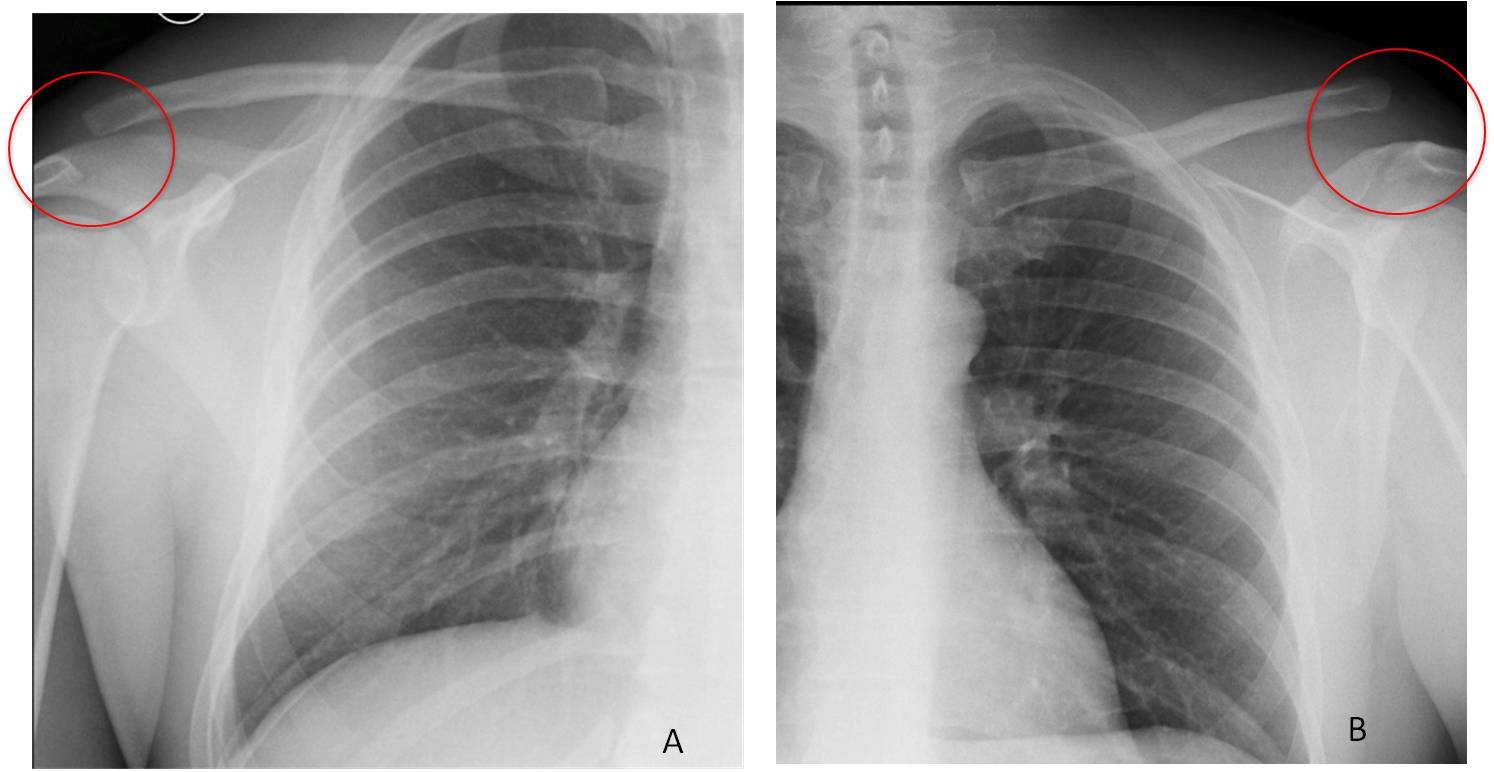
Fig. 8
Fig. 8. Two patients with AC dislocation discovered in the chest film. There is a lack of alignment of the AC joint and upward elevation of the distal clavicle (A and B, circles).
Chest radiography may also detect post-traumatic changes of the AC joint and osteolysis of the distal clavicle, not uncommon in weightlifters (Fig. 9).
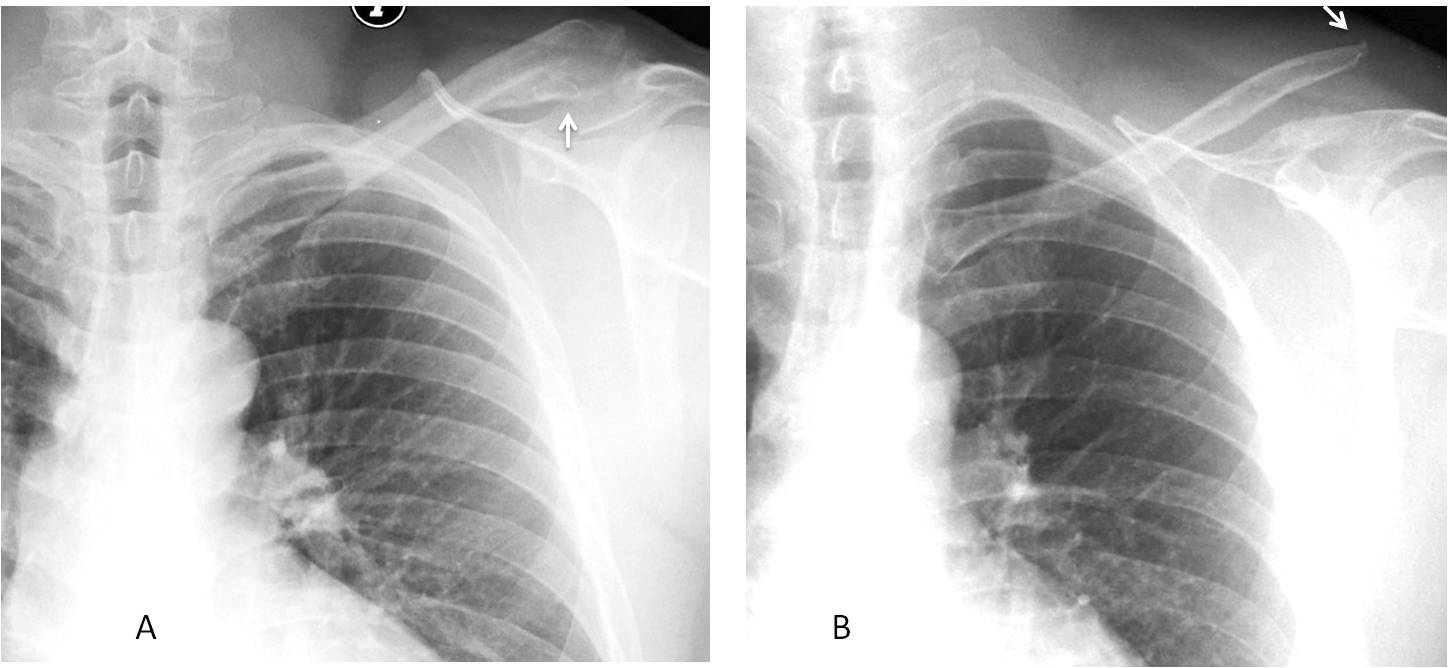
Fig. 9
Fig. 9: 34-year-old man with chronic post-traumatic AC dislocation and an exuberant soft tissue calcification (A, arrow). Another patient with AC dislocation and osteolysis of the distal clavicle (B, arrow).
Miscellaneous conditions include degenerative disease of the shoulder and AC joint. Systemic diseases (Fig. 10) or tumours (Figs. 11 and 12) can affect the shoulder bones and be detected in the chest radiograph, leading to further investigation to establish the definite diagnosis.
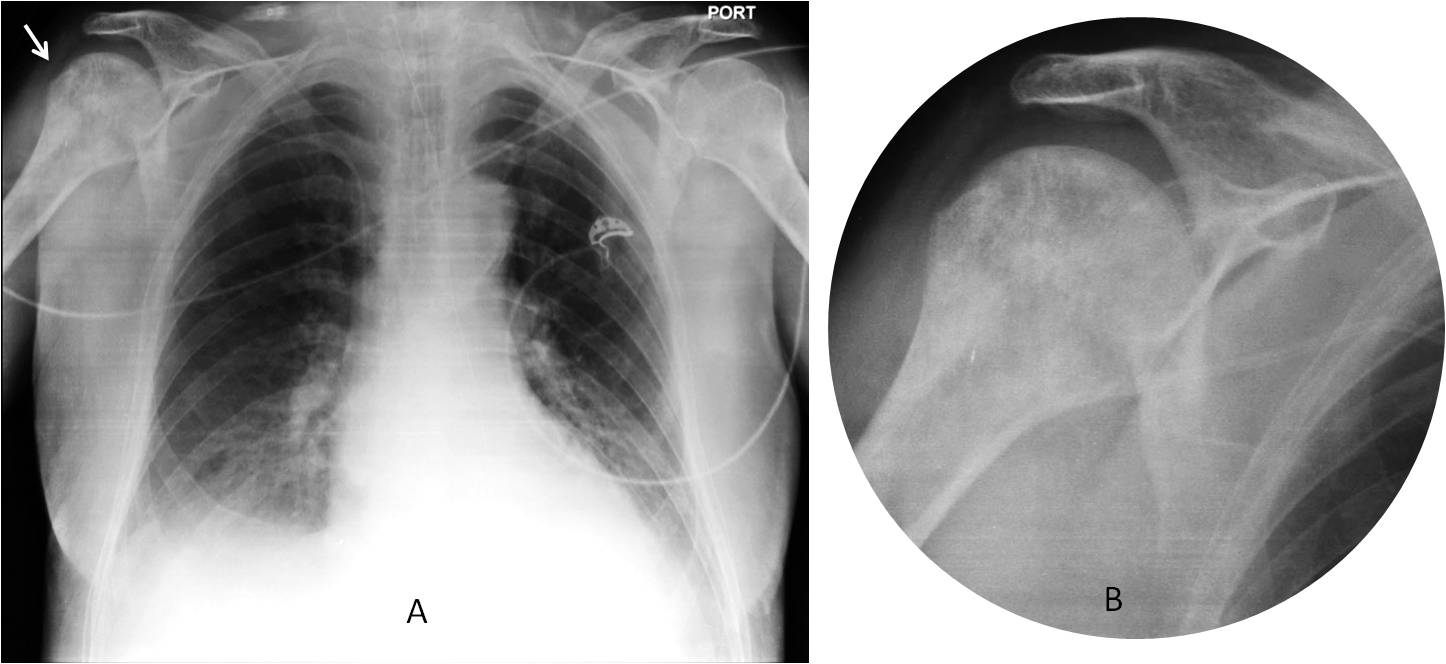
Fig. 10
Fig. 10: 76-year-old man with Paget’s disease of the left humerus, detected in the chest radiograph (A, arrow). Cone down view shows the typical features of Paget’s disease of the humeral head (B).
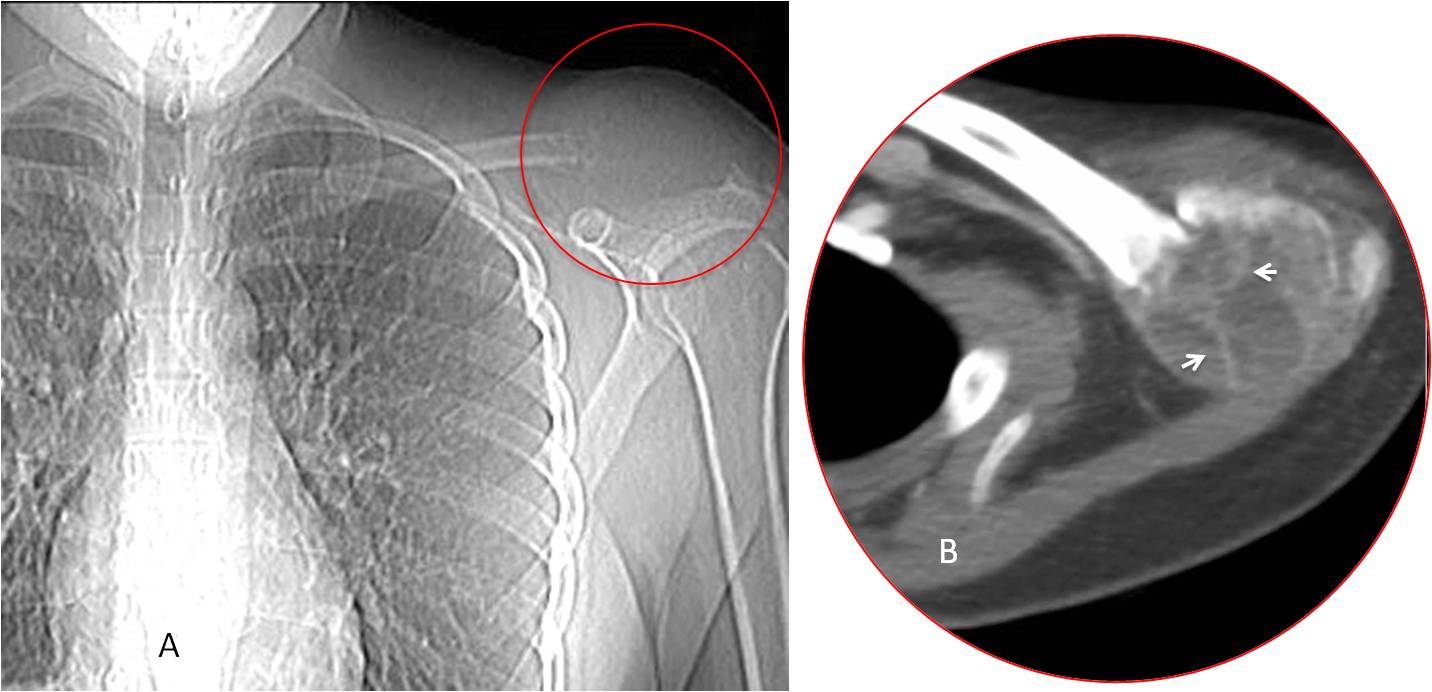
Fig. 11
Fig. 11: 22-year-old woman with a shoulder mass. Scout film shows an expansive lesion at the end of the clavicle (A, circle). CT confirms an expansive lesion with multiple bone ridges (B, arrows). Diagnosis: aneurysmal bone cyst.
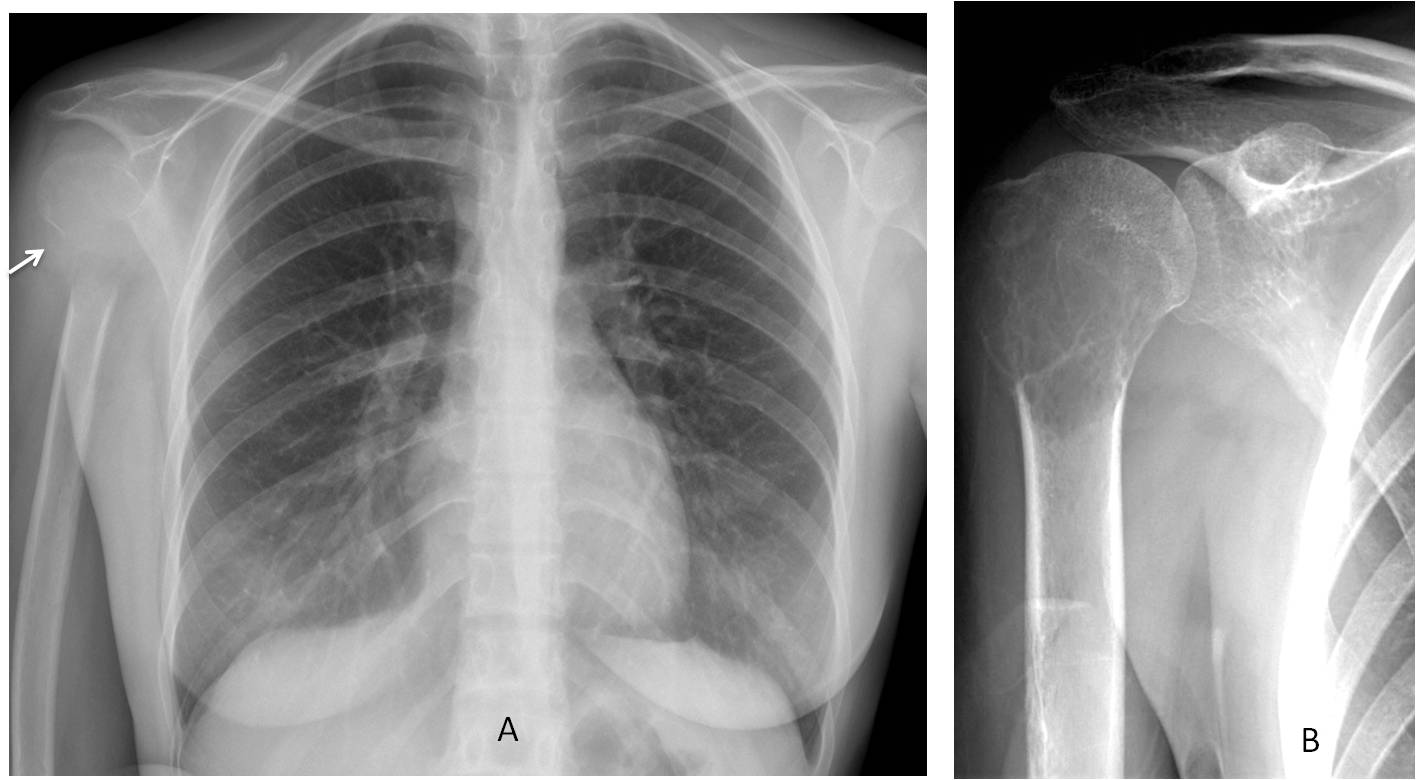
Fig. 12
Fig. 12: 28-year-old woman with a lytic lesion in the right humeral head (A, arrow). Cone down view of the shoulder confirms an expansive lesion with multiple septa. Diagnosis: giant-cell tumour.
A common pitfall is pseudotumor of the humeral head (Fig. 13), a false lytic image secondary to internal rotation of the humerus. Do not confuse it with a true lesion. It disappears on external rotation.
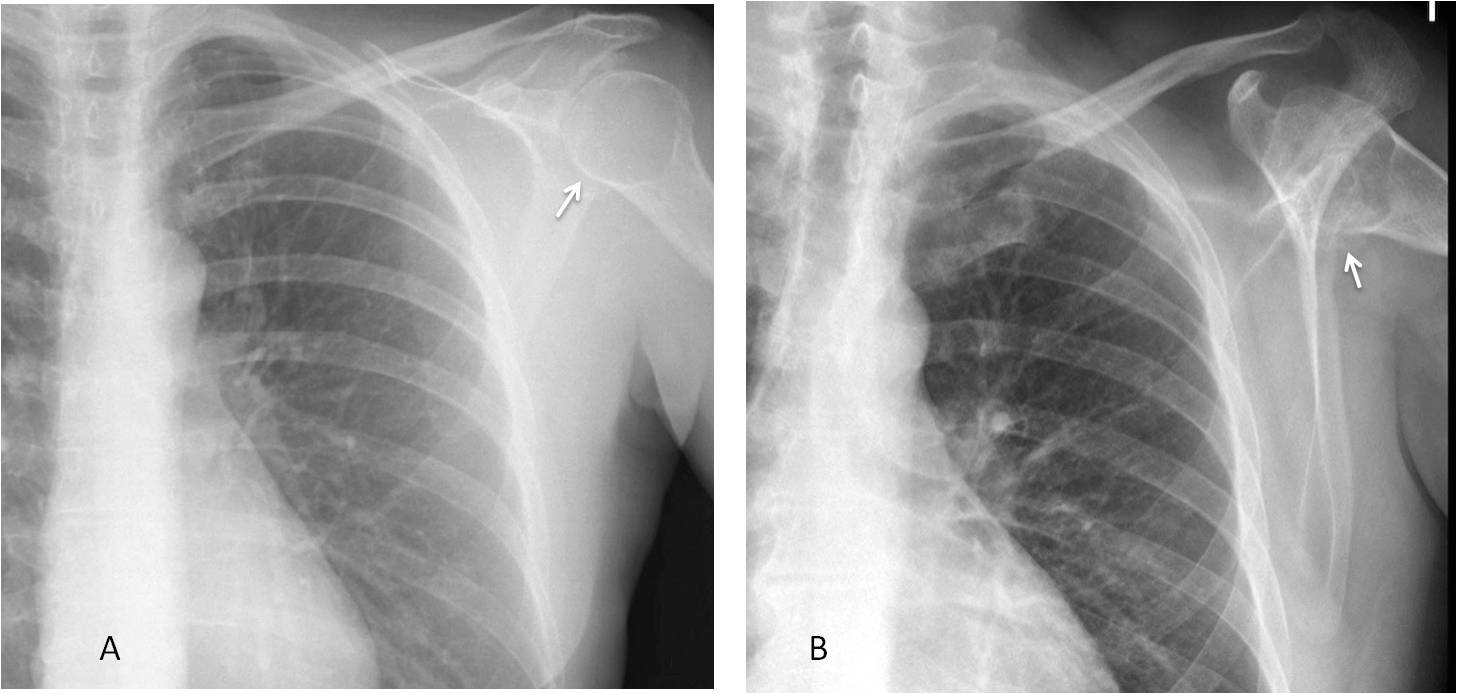
Fig. 13
Fig. 13. Two patients with pseudotumours of the humeral head (A and B, arrows).

Follow Dr.Pepe’s Advice:
1. Always look at the shoulders in the PA view.
2. Look for calcific tendinitis at the upper border of the humeral head.
3. Always look for AC joint dislocation.
4. Occasionally, systemic diseases are discovered by PA radiograph findings.


Trachea and main bronchi without visible abnormalities.
Following aortic contour without abnormalities.
Lungs: the right lung is decreased in volume, there are increased vessel shadows and linear pattern due to peribronchovascular infiltration, on the level of the 3d rib there is shadow of horizontal fissure.
in the left lung there is decreased lung attenuation mostly in upper and mid zones
Right hila shows abnormal bronchial and vessels division
There is mediastinum shadow enlargment suggesting hypertrophy of left ventricle, with smooth contours.
There is elevation of right hemidiaphragm on the level of anterior part of 4/5 ribs
On the lateral view – the darkening of the anterior mediastinum.
Suggestion of right lower lobe hypoplasia
Hello,
Obvious abnormality on this exam is elevation of right diaphragm. Minor fissure is in normal position. Where exactly is that pain?
You don’t need to know where the pain is to make the diagnosis. Allow me to withold the information
Beside above mentioned there is suspicious air collection underneath left hemidiaphragm.
Is there some hyperlucency of the soft tissues near the left shoulder joint? Might there be some emphysema / abscess / septic arthritis?
Oops I thought that was digital artifact!
Oops!
Is there a round soft opacity at the hilum?
No, to my knowledge
….vi è un allargamento del profilo mediastinico, sopratutto nella linea paraspinale sx, con occupazione delle spazio chiaro retrosternale….di natura adenopatica….linfoma?
At the left arm projection and subscapular,some areas of air density like subcutaneus emphysema.
P.S.
Very sorry,my english is little
Your English is adequate and your interpretation is excellent
At this time of the week I would like to congratulate Berti (Gold medal) and Bujar (Silver medal), as the two persons who saw the air over the shoulder. Last week’s case was similar and emphasized that we always should look at the corners of the film.
More information tomorrow. Happy weekend!