As keen followers of my career will know, the chest is my particular area of expertise, so that’s where we’re returning this week. This case is a 39 year-old woman with a cough.
1. Mediastinal lymph nodes
2. Endothoracic goiter
3. Esophageal diverticulum
4. None of the above
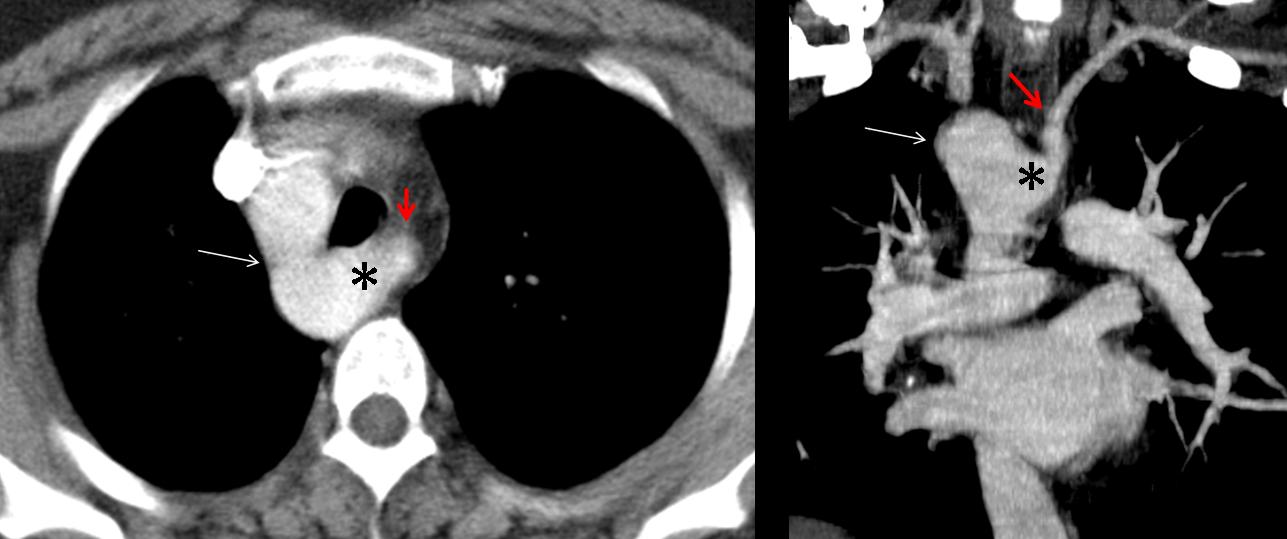
Given that the trachea is in a central position and the aortic arch cannot be seen on the left side, the most likely diagnosis is a vascular anomaly (
right aortic arch). CT confirms the right aortic arch (long arrow). The left subclavian artery (
red arrow) is seen to arise from a large Kommerell diverticulum (asterisk).
Final diagnosis: Right aortic arch with aberrant left subclavian artery
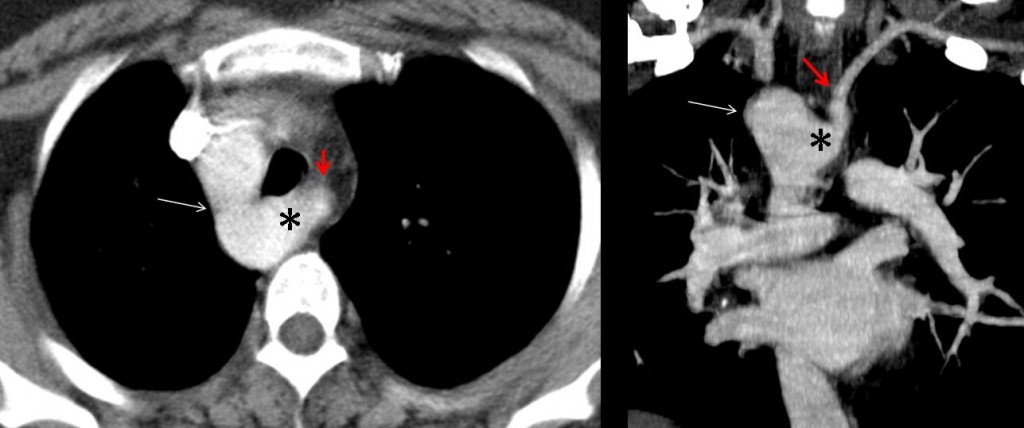
Fig. 2
Right aortic arch is one of the congenital aortic variants. Congenital aortic arch anomalies (CAAA) result from errors in the embryological development of the branchial arches, and include isolated aberrant right subclavian artery, right aortic arch, and double aortic arch. CAAA are often discovered as an incidental finding on chest plain films performed for other reasons.
Right aortic arch can be divided into two groups. Those without an aberrant right subclavian artery (mirror image) are often symptomatic because they are associated with cardiac anomalies, whereas those with an aberrant right subclavian artery only sporadically show symptoms in adults (stridor, wheezing or dysphagia) due to tracheoesophageal compression.
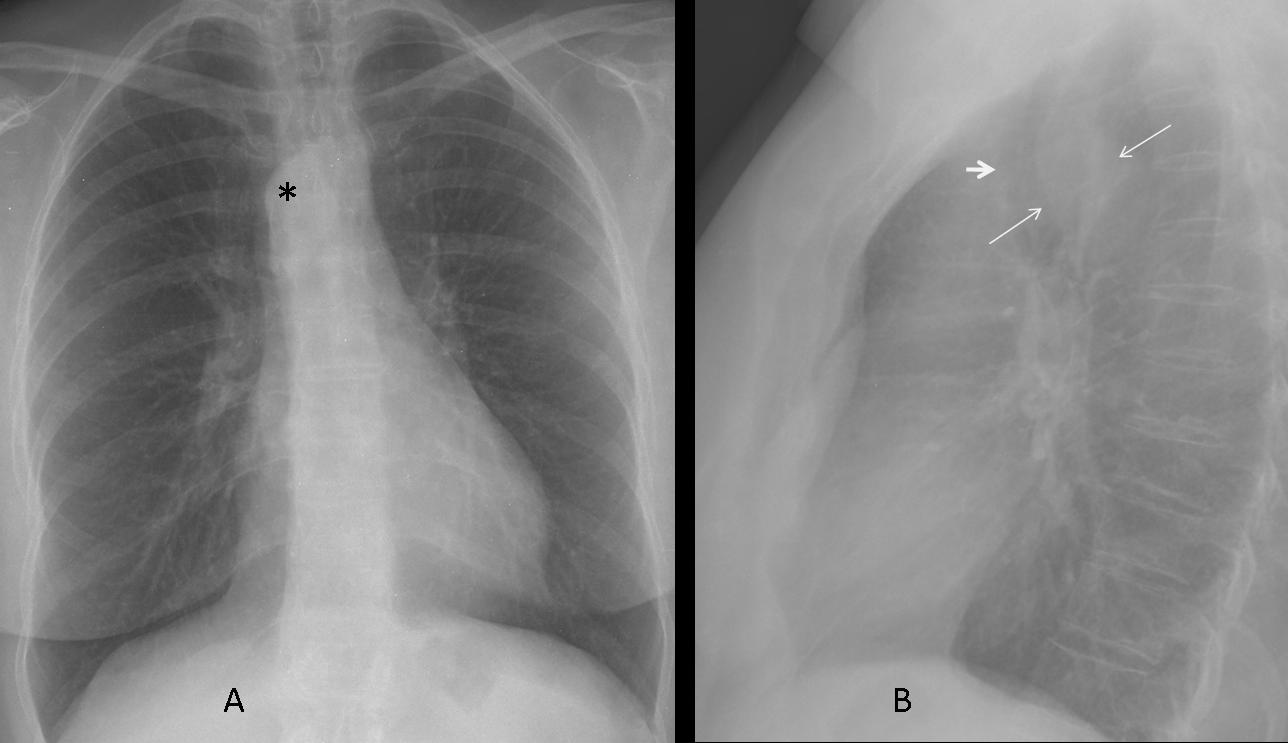
In patients with right aortic arch, the chest plain film shows the trachea in a central position or displaced to the left side, and the aortic arch cannot be identified on the left side. Sometimes a large aortic arch is seen on the right side of the trachea (asterisk in A). The lateral view (B) may show anterior displacement of the trachea (short arrow) with widening of the posterior tracheal line (long arrows).
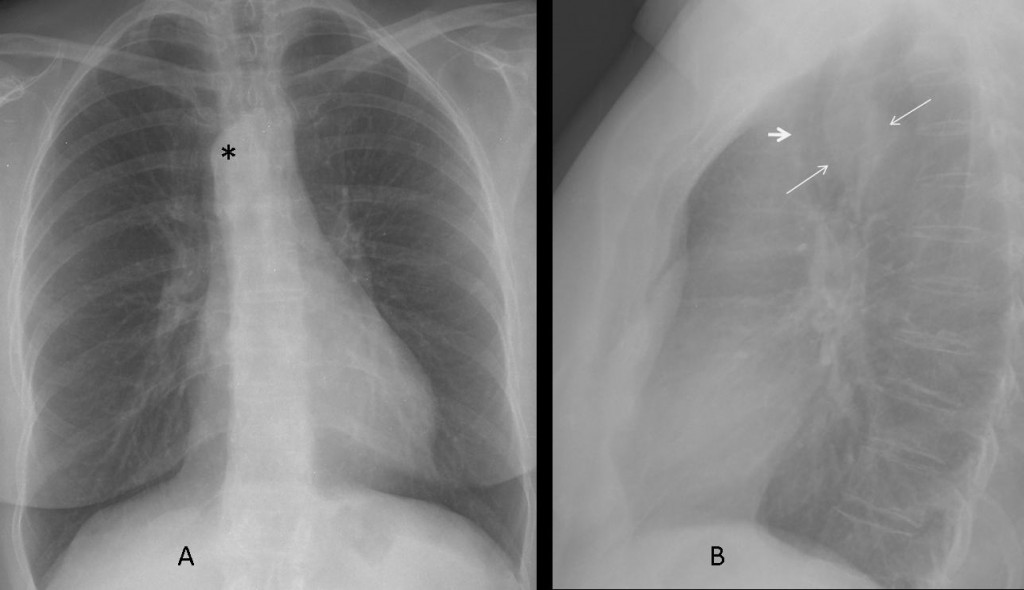
Fig. 3
CT and MRI are excellent tools to differentiate between congenital aortic arch anomalies, and are the main diagnostic techniques used in symptomatic patients:
49 year-old woman with asthma. The plain film (Fig. 4) shows the trachea in a central position and a right aortic arch (arrow).

Fig. 4
CT confirms the aortic anomaly and shows an incomplete double aortic arch (Fig. 5).
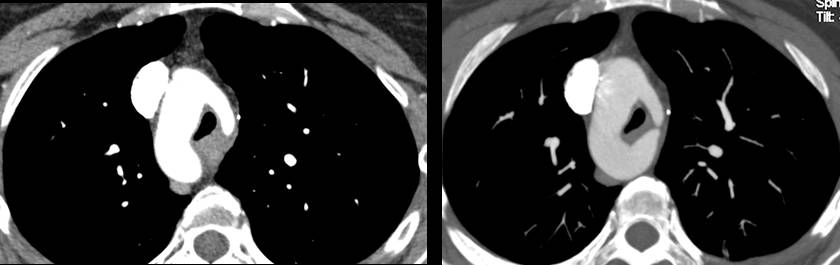
Fig. 5
This anomaly produces a vascular ring with narrowing of the trachea (Fig. 6a). The left subclavian and left common carotid arteries arise from the anterior portion of the incomplete left arch (Fig. 6b).
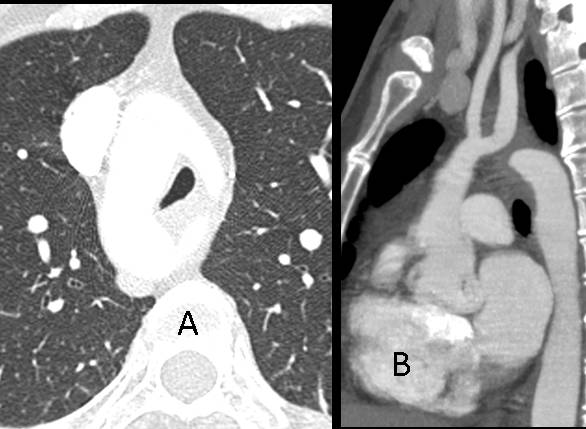
Fig. 6
The differential diagnosis includes enlargement of the thyroid gland (goiter) and paratracheal lymphadenopathy. The left aortic arch is usually visible on chest radiography and narrows down the diagnosis. When in doubt, CT can be used to differentiate between goiter, lymphadenopathy, and congenital aortic anomaly.
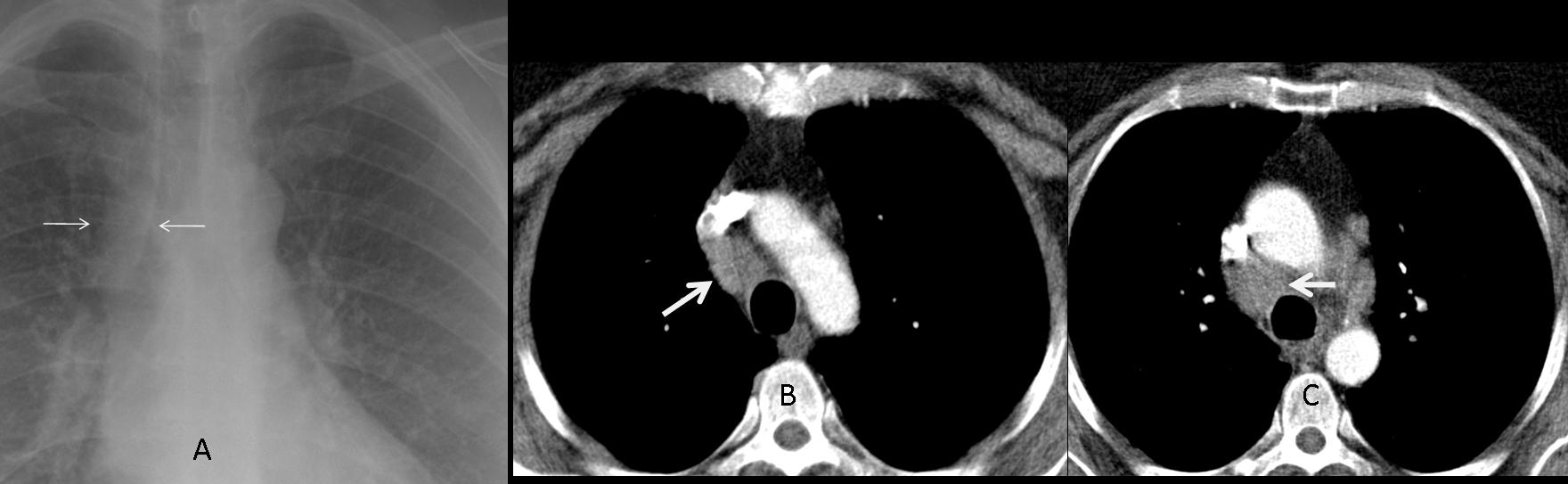
45 year-old woman with sarcoidosis. Plain film shows widening of the right paratracheal stripe (arrows, A). CT confirms lymphadenopathy in the right paratracheal region (arrows, B and C).
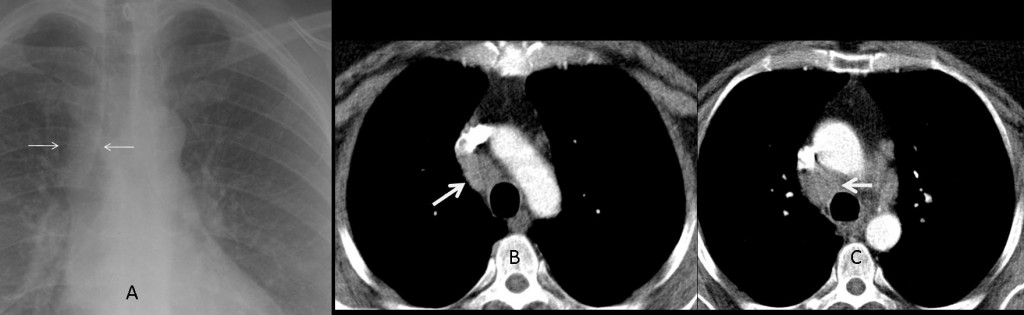
Fig. 7
52 year-old man with goiter. The plain film shows a cervical-thoracic mass (Fig. 8, asterisk) with tracheal displacement (arrows); the aortic arch is in the left position.

Fig. 8
CT confirms the presence of an enlarged thyroid (Fig. 9, arrow) with calcifications.

Fig. 9

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- Congenital aortic anomalies can be recognized in the chest radiograph by the position of the trachea and the aortic arch.
- CT and MRI should be used to differentiate between congenital aortic anomalies.
Ref. Embriology and imaging review of aortic arch anomalies. JTI 2012; 27:73-84
Case prepared by JM Mata




İn lateral view,there is slight dilatation of the eosaphagus.in PA graphy,there is a radiocontrast in Middle part of the oesaphagus.the answer should be Diverticulum.
The pulmonary hilus and the vessels are at the normal size.the trachea is at the midline.
What other sources that we can study for the examination?
I THINK ABOUT OESOPHAGUS STUDIED WITH MDC.
If you think of a diverticulum, the appropiate study is a barium swallow.
non of the above
IT COULD BR SOLUTION, BUT NOE LITTLE DISLCATIO ON DX PLEURIC SCISSUE , IN ANTERIOR AT LEVEL OVF UPPER DX LOBE.
INITIAL OBSTRUTION =
An elongated soft tissue shadow pushing the trachea anteriorly.
This lesion is extending from above—Neck.
I will go for Endothoracic goiter.
none of the above
endothoracic goiter
On the right anterior mediastinal border there is a slight curve which could be produced by an esophageal diverticulum.
None of the above.
Right aortic arch!
Good. You were first of many.
In AP dell’rx-torace, si osserva un lievissimo svasamento del profilo mediastinico alto a dx, con l’immagine tracheale che sembra mediana anzichè normalmente spostata a dx.In LL si osserva una impronta sulla superficie posteriore della trachea che sembra lievemente spostata in avanti.Inoltre lo spazio chiaro retrosternale non è chiaramente visibile.Non sono ben visibili le due arterie polmonarie lo spazio chiaro della finestra aorto-polmonare.Penso allora ad un ingombro adenopatico del mediastino medio.,.
Right aortic arch with aberrant left subclavian artery.
Aortic arch is on the right.
On the lateral film, the trachea is bowed toward. I think is by the presence of an aberrant left subclavian artery which passes behind it.
4. None of the above
I would suggest a right sided aortic arch (vs double aortic arch).
Then would be necessary to complete with a CT to confirm the diagnosis and rule out other associated vascular anomalies and possible complications.
I don’t see the aortic arch at the left, instead I see a upper right paramediastinic image that looks like a right aortic arch.
Right aortic arch
4. none of the above .
Right aortic arch with aberrant left subclavian artery
aortic knob is on the right and the trachea is slightly displaced toward the left instead of the right, as in normals. On the lateral film,the trachea is bowed toward by the aberrant left subclavian artery which passes behind it
endothoracique goiter at the left side
I will go with mestiastinal mass (maybe a endothoracic goiter)
Should be pulmoary sling .The radioopacity at the lateral view is obtained by the right aortic arc ,not a goiter .The most common abnormality seen in vascular patology is double aortic arc but there is not evidence of this .Then should considered the right aortic arc with left aberran subclavian .but the interrruption may be a least diagnosis in the vascular anomalies of the cardiac .
Good. I am glad the cavalry came to the rescue!
.Remember that in every mediastinal mass it is imperative to rule out a vascular origin
Findings include:
– widening of the right paratracheal stripe with focal mediastinal bulging (PA)
– the aortic knob is not adequately visualised (AP)
– minimum rotation of the film (AP)
– loss of the retrosternal lucency (L)
– anterior displacement of the trachea (L)
– widening of the posterior paratracheal stripe (L)
The pathology must be in the retrotracheal triangle (middle mediastinum).
The intrathoracic goiter creates lateral displacement of the trachea.
Lymphnode involvement extents laterally usually in the AP film.
Esophageal pathology fits with the imaging findings and cough (due to eg aspiration) but a diverticulum might have an air-fluid level.
Another diagnostic possibility is a vascular anomaly such as right aortic arch with aberrant left subclavian artery (though the right mediastinal bulging is somewhat higher than expected for an aortic arch and cough is not expected)
So the correct answer should be 3 (with a consideration regarding the vascular structures)
Endothoracic goiter