Dr. Pepe’s Diploma Casebook: Case 90 – SOLVED!
Dear Friends,

I am back with a new case, provided by my good friends Paula García and Alberto Villanueva. Images belong to a 52-year-old man with a dry cough. Operated on for cutaneous melanoma ten years earlier. Check the images below, leave us your thoughts in the comments section and come back on Friday for the answer.
Diagnosis:
1. Tuberculosis
2. Metastases
3. Varicella pneumonia
4. Any of the above


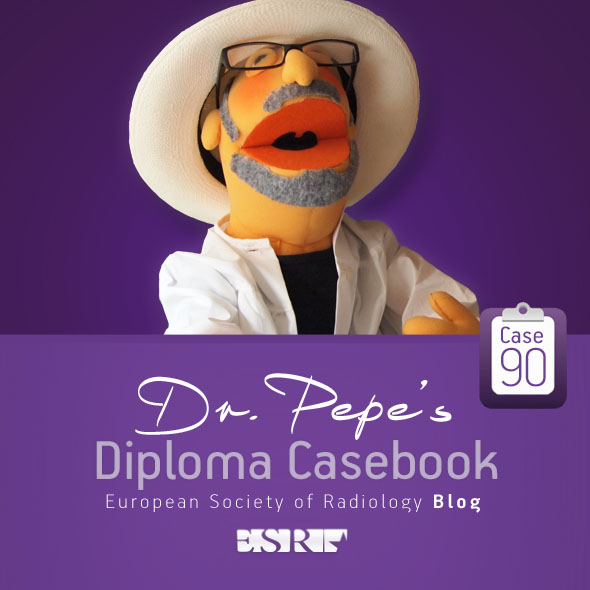
Findings: Chest radiographs show multiple miliary nodules in both lower lobes (A and B, circles). Scar lesions are also seen (A, arrows).
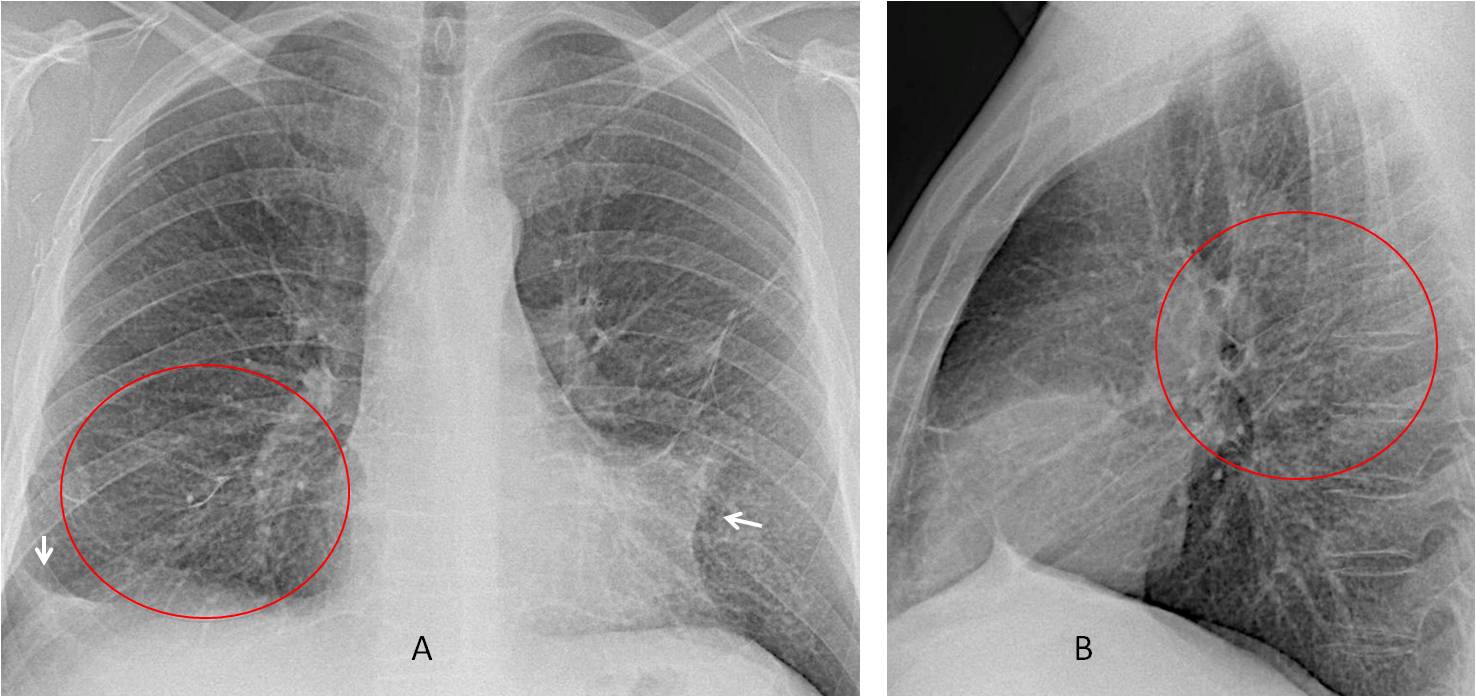
The miliary nodules are more obvious in the comparison with a previous film, taken one year earlier (C and D).
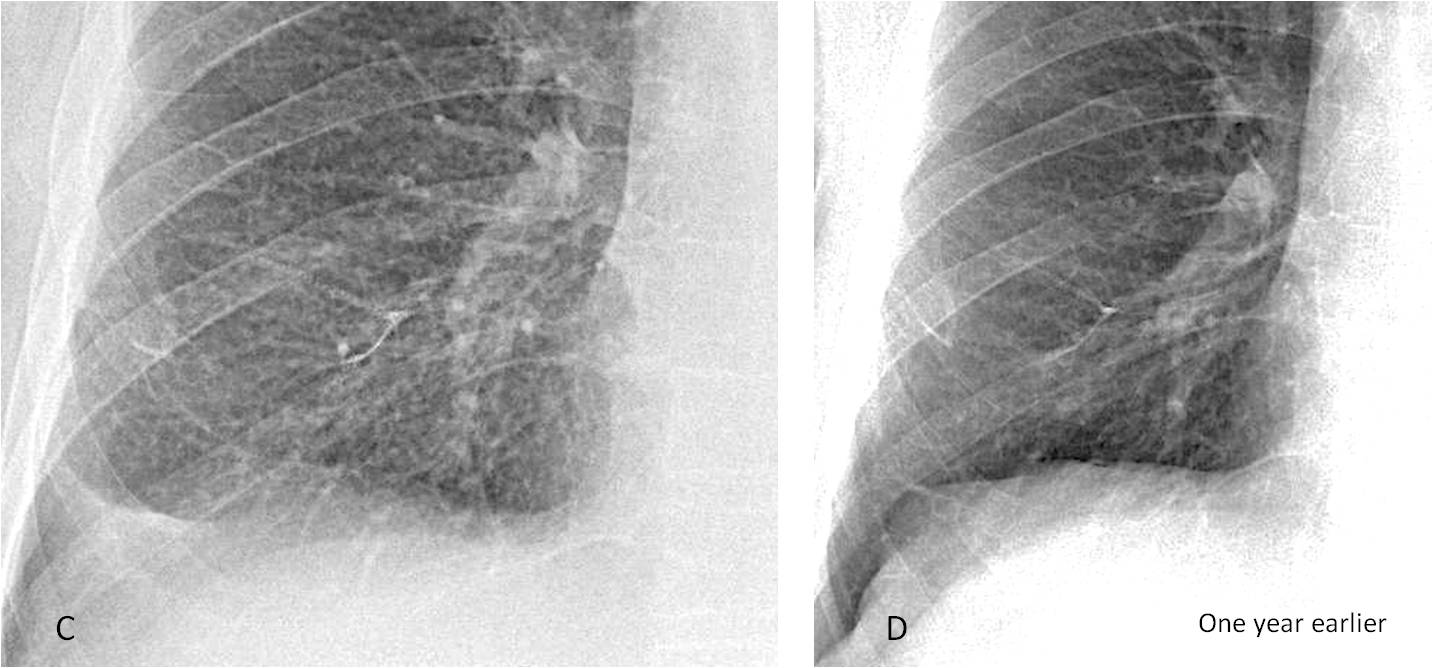
Axial and sagittal CT images confirm the presence of multiple miliary nodules predominantly located in the lower lobes (E and F, circles).
Final diagnosis: Miliary metastatases from melanoma.
I’m showing this case to discuss miliary nodules in the chest radiograph. The Fleischner Society defines the miliary pattern as a series of discrete rounded opacities, 3mm or less in size, distributed throughout the lungs. In CT images they are seen as randomly distributed micronodules.
Approximately 80 conditions can display this pattern and, as this case shows, miliary nodules may be difficult to see (this is the bad news). The good news is that, once the pattern is identified, there is an easy, practical approach to narrow down the possibilities. In my experience, the first step in approaching a miliary lesion is to decide whether it is acute or chronic. This decision is based on the clinical findings and comparison with recent films.
Infection is the most common cause of miliary nodules in acutely ill patients. The first consideration should be miliary TB, secondary to hematogenous dissemination. Usually the nodules show no predominant lung distribution (Fig. 1). About one-third of cases have associated findings (consolidation, cavitation, or lymphadenopathy).
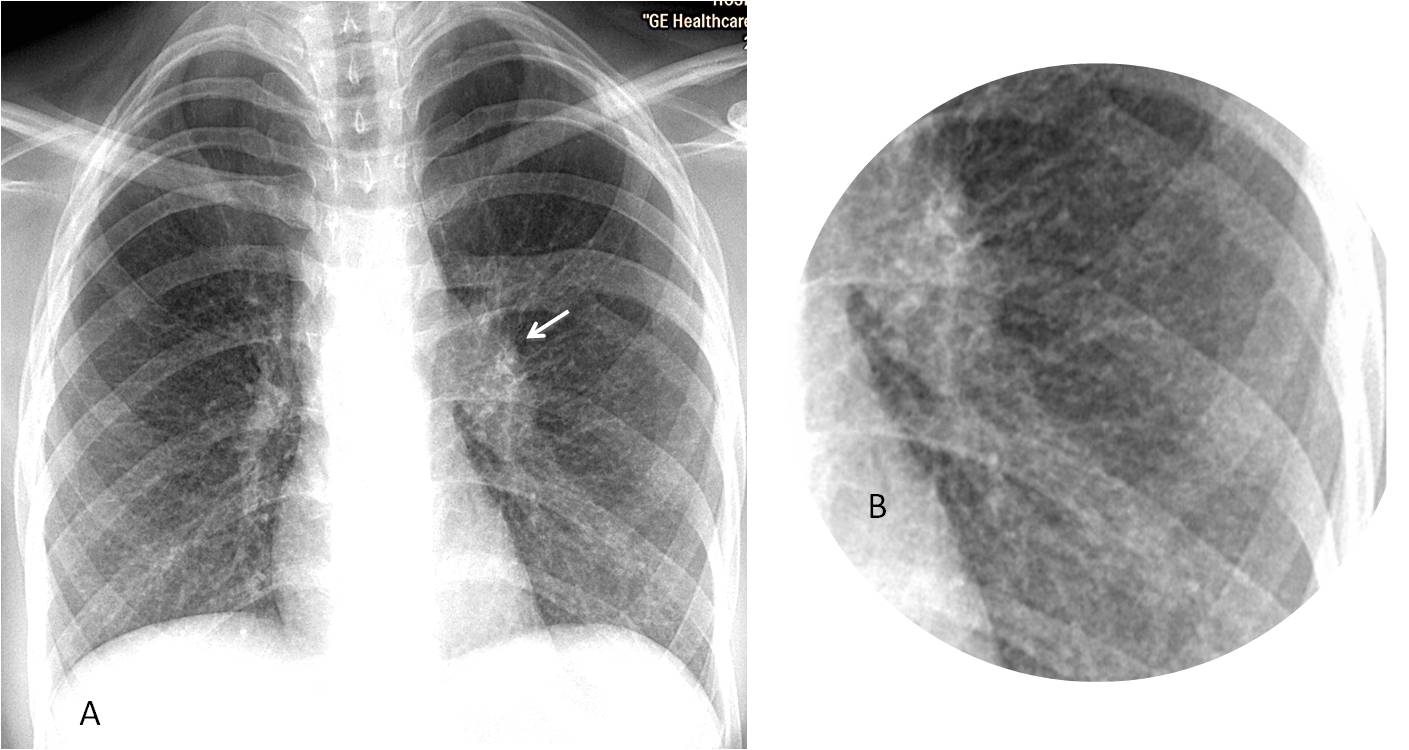
Fig. 1
Fig. 1: 27-year-old woman with fever and malaise. The chest radiograph (A) shows a widespread miliary pattern, better seen in the insert (B). The left hilum is enlarged (A, arrow). Associated lymphadenopathy is not uncommon in HIV patients. Diagnosis: Miliary TB.
CT is very helpful in patients showing inconclusive findings in the chest radiograph. The typical appearance is multiple well-defined nodules distributed in a random pattern (Fig. 2).
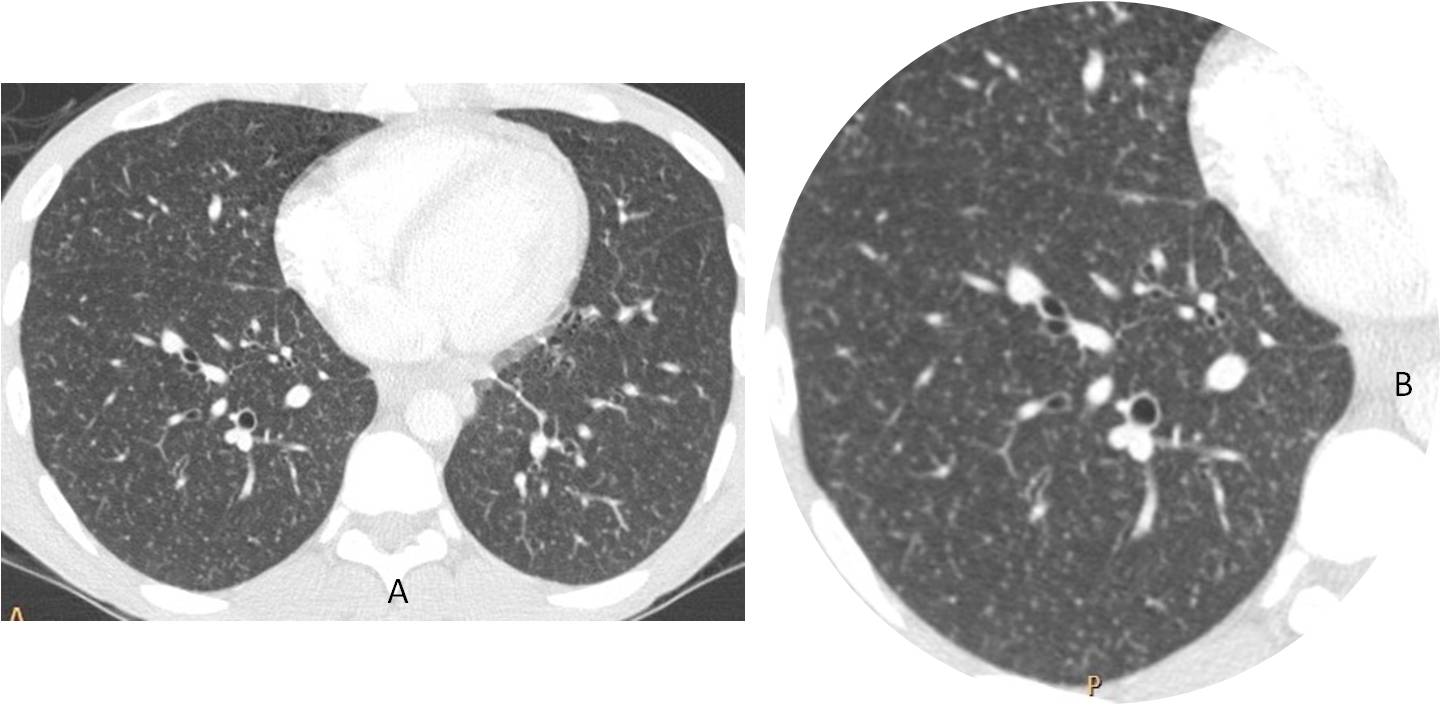
Fig. 2
Fig. 2: 38-year-old man with AIDS and a doubtful chest radiograph. Axial CT images (A and B) show multiple, small, well-defined nodules with a nonspecific distribution. Proven miliary TB.
Bronchogenic spread of TB may give an appearance similar to miliary TB. Cavitations are usually obvious and the nodules are coarser (Fig. 3).
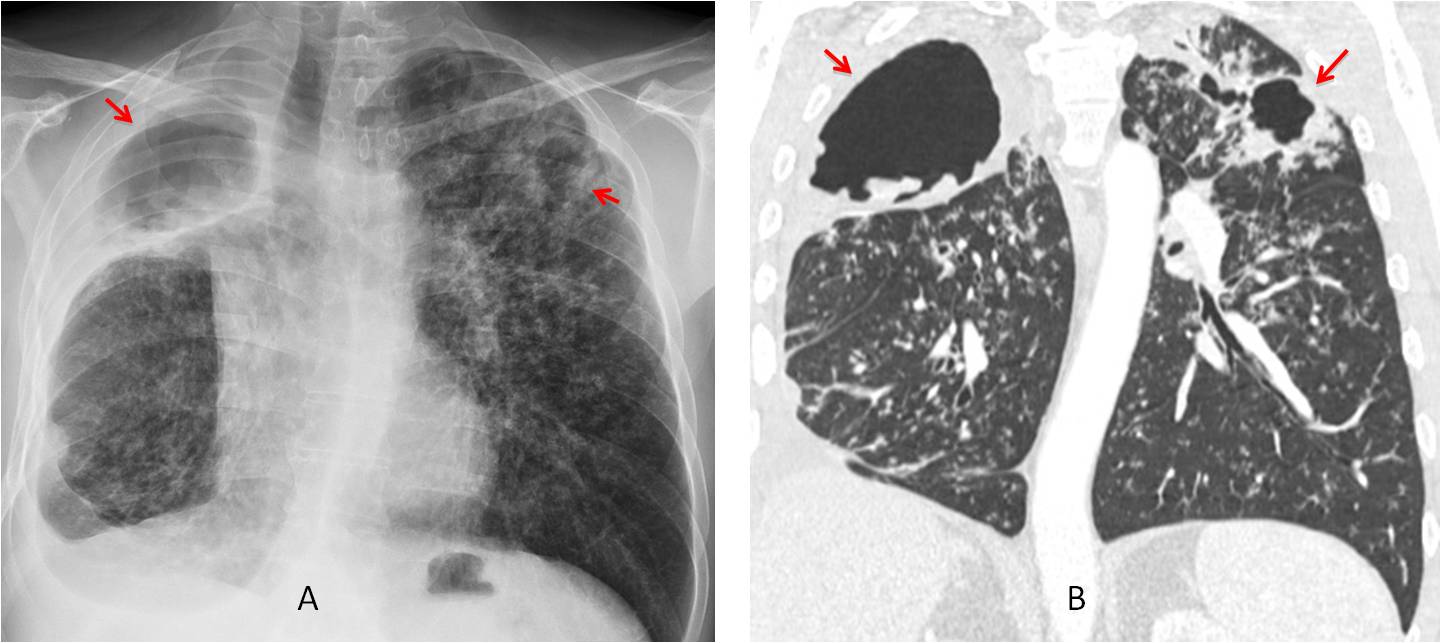
Fig. 3
Fig. 3: 47-year-old man with active TB and bronchogenic spread. There are cavities in both upper lobes (A and B, red arrows) and numerous nodules in both lungs. A right pleural effusion is also evident.
Viral infections may produce a miliary pattern. Usually the nodules are larger and suggestive or air-space disease rather than interstitial nodules (Fig. 4). The most common is varicella pneumonia, easy to suspect by the typical skin lesions visible in the great majority of patients.
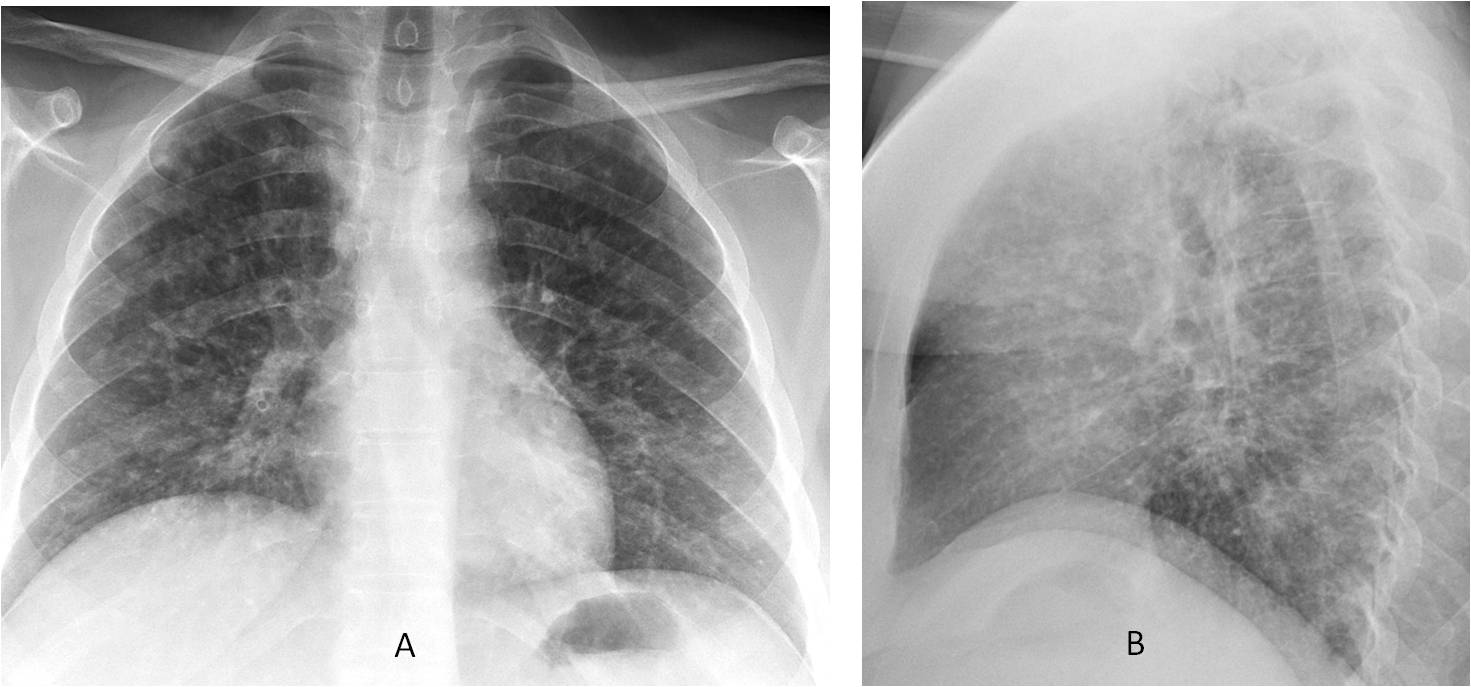
Fig. 4
Fig. 4: 29-year-old woman with acute fever and skin lesions. Chest radiographs (A and B) show a diffuse coarse miliary pattern (compare with Fig. 1). Diagnosis: varicella pneumonia.
Among the chronic conditions showing a miliary pattern, uncomplicated silicosis is the most common one (Fig. 5). The nodules have an upper lobe predominance. About 3% of silicotic nodules calcify (Fig. 6A). Eliciting a history of exposure confirms the diagnosis.
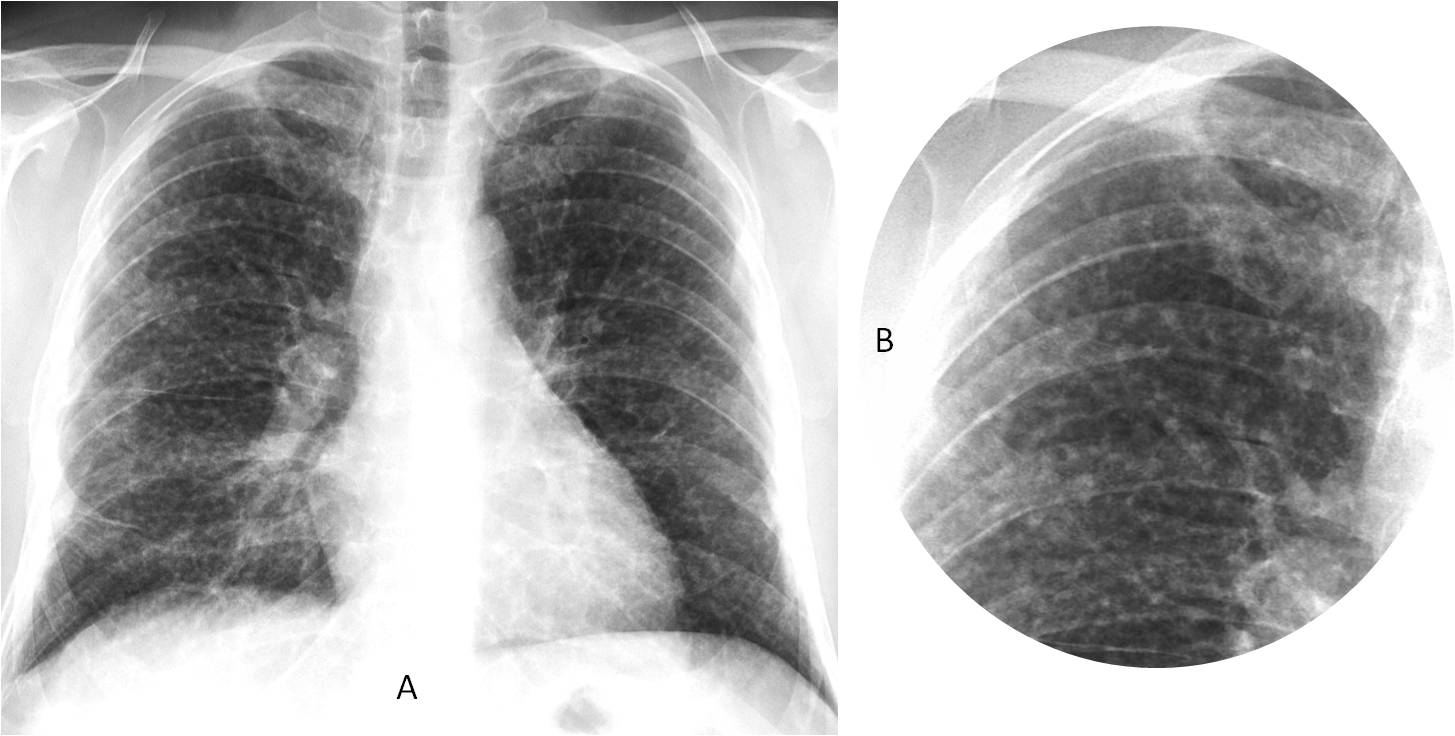
Fig. 5
Fig. 5: 55-year-old man with a mild cough and chronic miliary pattern (A and B). Interrogation confirmed a long history of dust exposure. Diagnosis: Uncomplicated silicosis.
About 5% of patients with silicosis show egg-shell calcifications in the mediastinal lymph nodes. The association of miliary nodules with egg-shell calcification is highly suspicious of silicosis (Fig. 6B).
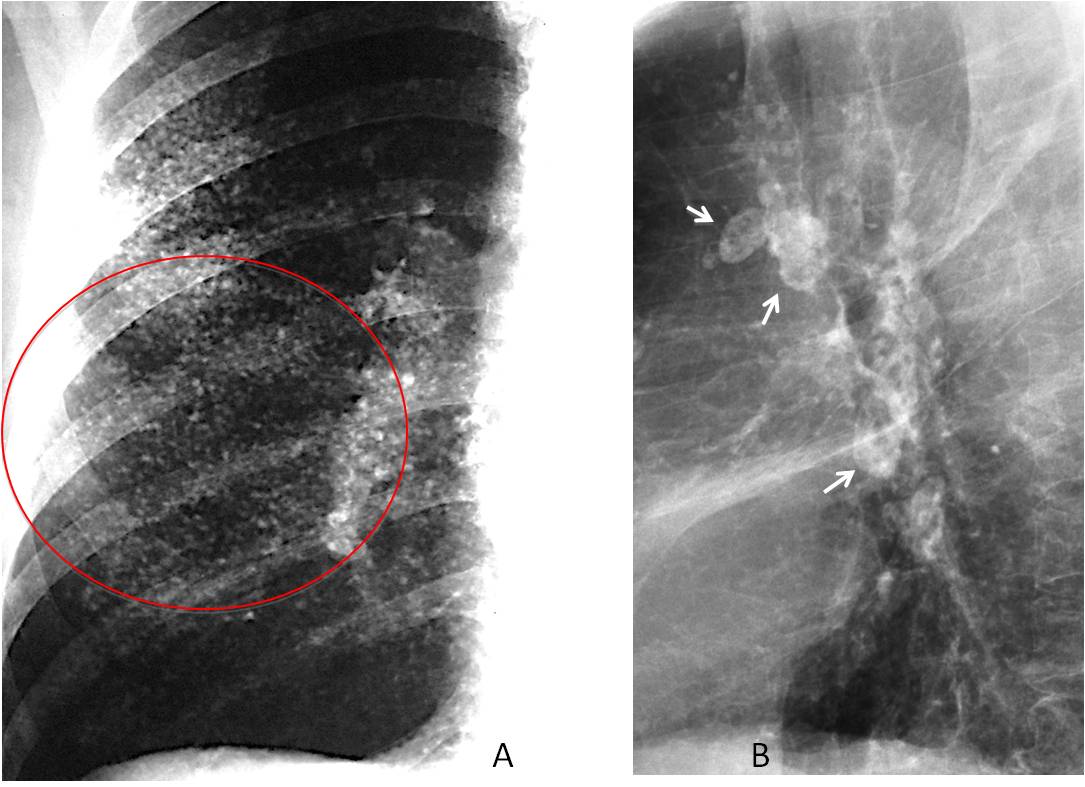
Fig. 6
Fig. 6: Long-standing silicosis with calcified nodules (A, circle). Lateral film in another patient shows typical egg-shell calcification of lymph nodes (B, arrows).
Miliary calcifications can also be seen in healed infectious diseases. The most common are varicella pneumonia, TB, and fungal infection. Unlike fungal infection and TB, mediastinal lymph nodes do not calcify in varicella pneumonia. Due to the small size of the nodules, calcium may go unrecognized by the untrained eye. In case of doubt, CT will clarify the findings (Fig. 7).
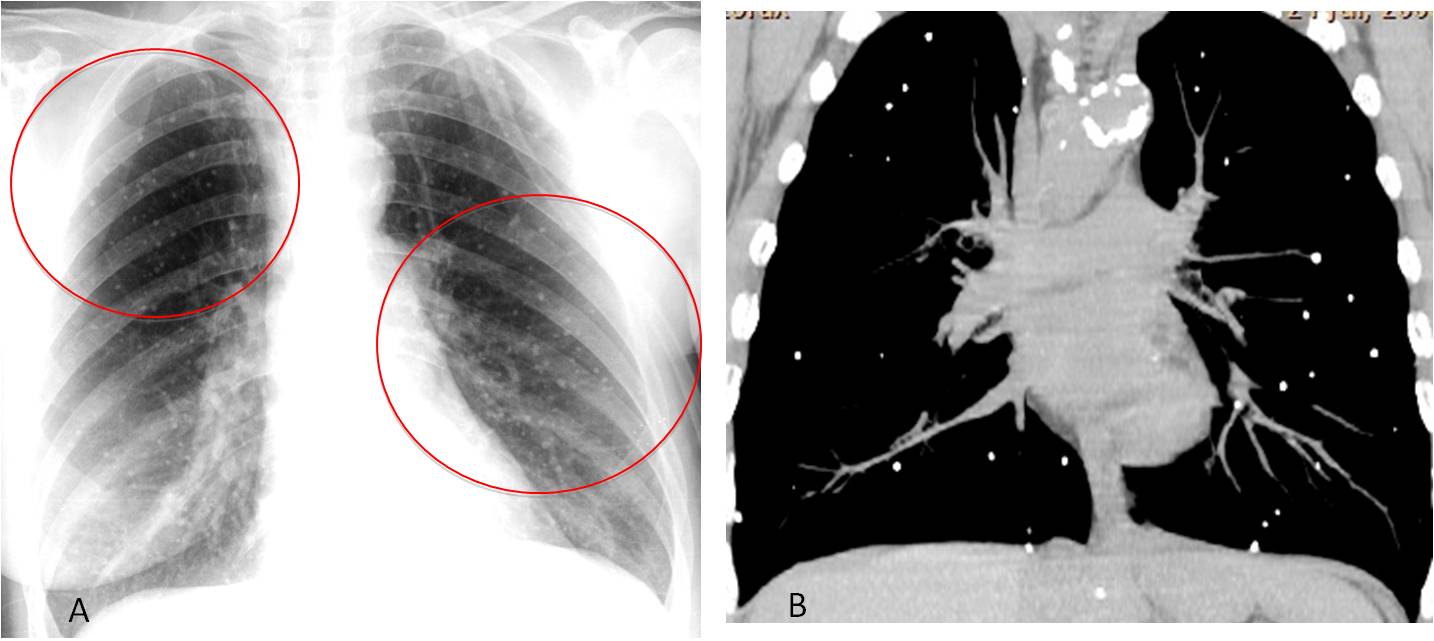
Fig. 7
Fig. 7: 52-year-old woman with a history of varicella pneumonia at the age of 11 years. Supine chest film shows probable miliary lung calcifications (A, circles) that are confirmed in the coronal CT image (B).
Miliary nodules are an uncommon manifestation of hematogenous metastasis. The most common primary tumors are thyroid, renal cell carcinoma, melanoma, and lung adenocarcinoma (Fig. 8). A helpful finding in suggesting metastases is the difference in size of some of the nodules, due to the seeding occurring at different intervals.
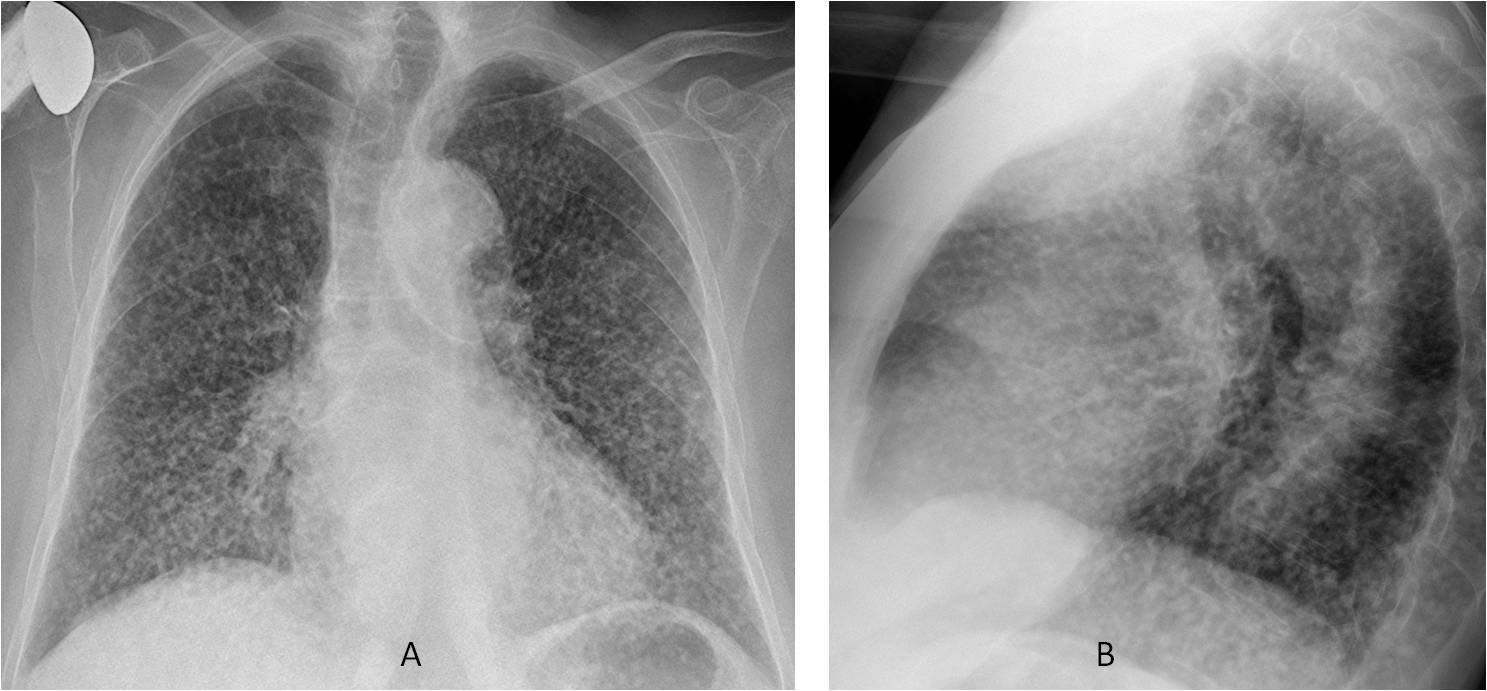
Fig. 8
Fig. 8: 78-year-old woman with dyspnea. No fever. Chest radiographs show a widespread miliary pattern in both lungs (A and B).
Axial and coronal CT confirms the presence of multiple miliary nodules in both lungs (C and D). Note that the nodules are not uniform in size. A macronodule in visible in the apical segment of the RLL (D, arrow). Final diagnosis: Adenocarcinoma of lung with miliary metastases.
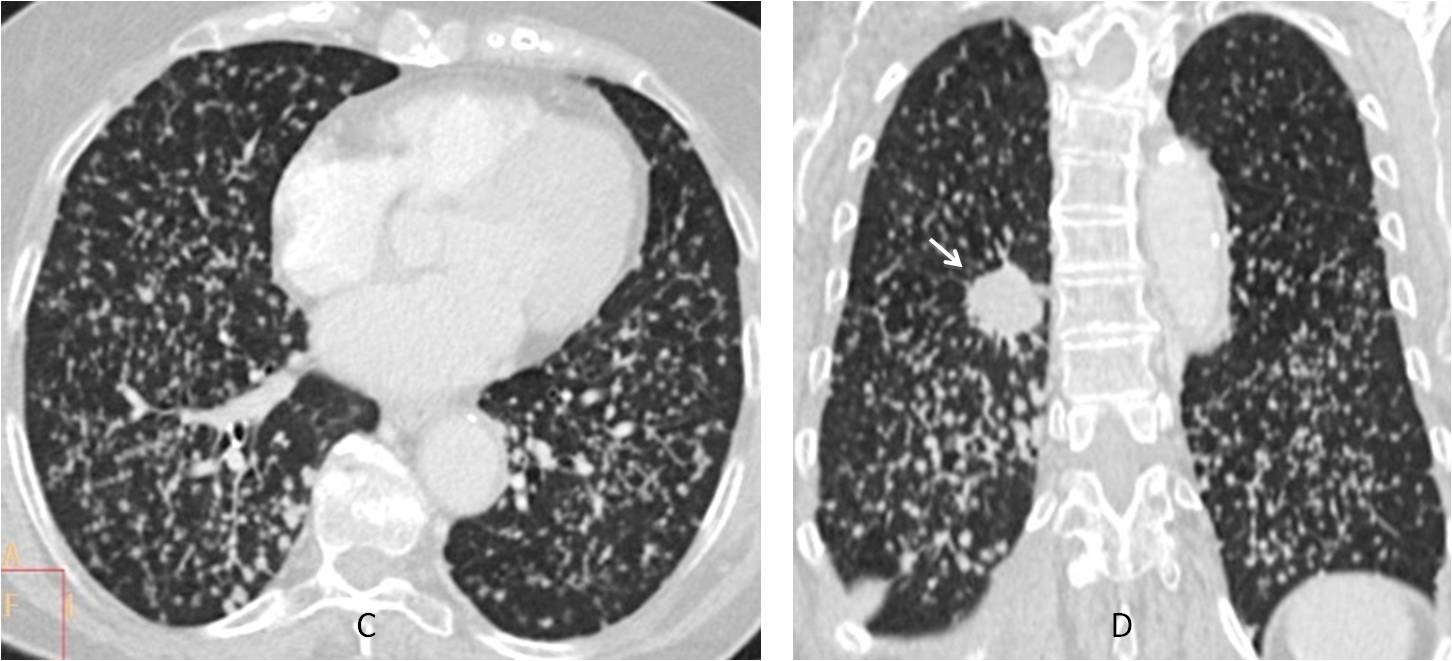
Fig. 8
Occasionally, systemic diseases may present with miliary nodules. The most common is widespread sarcoidosis, although the nodules are of a mixed type. Enlarged lymph nodes are usually present (Fig. 9).
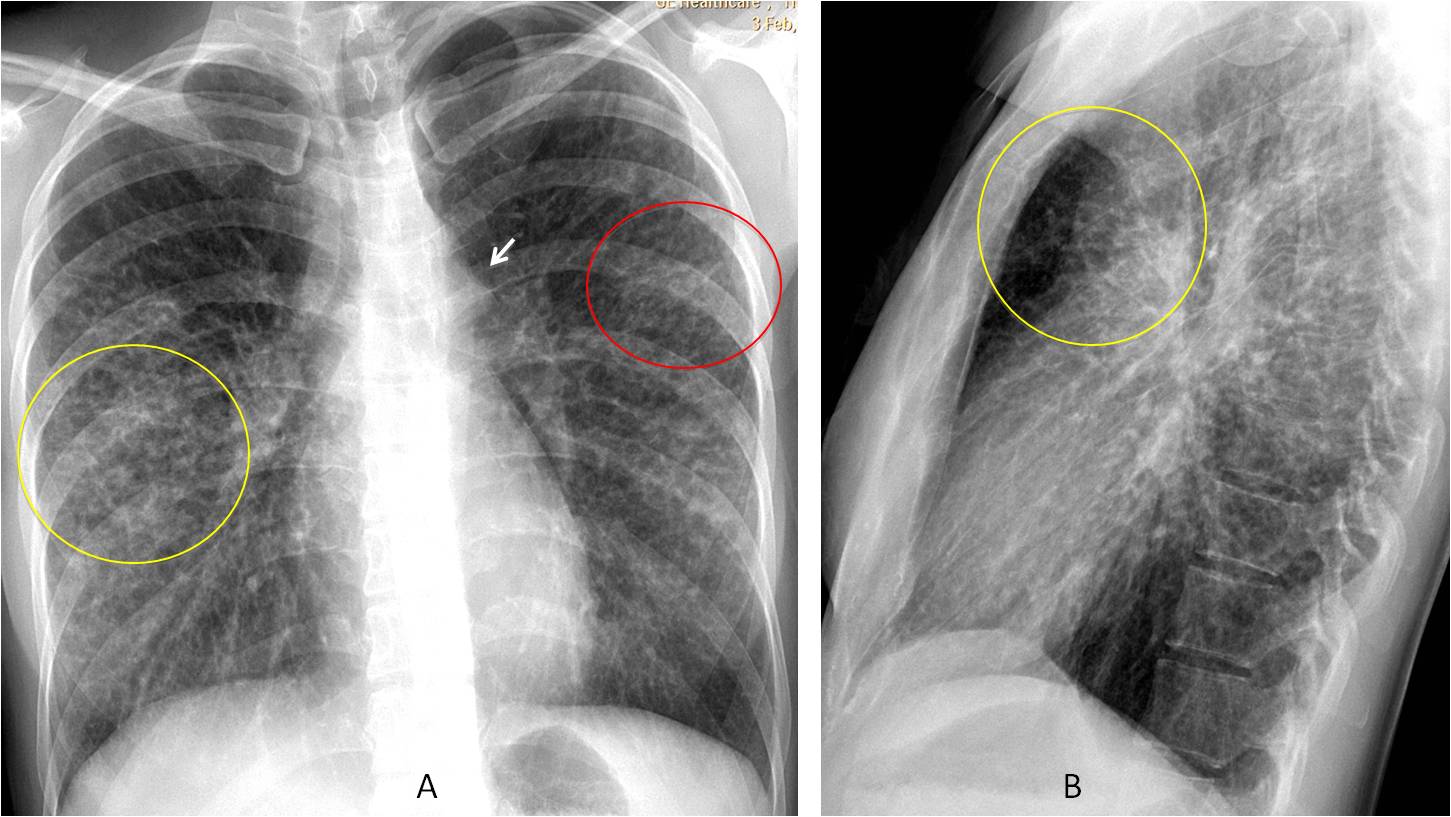
Fig. 9
Fig. 9: 33-year-old woman with sarcoidosis. There are areas of miliary nodules (A, red circle), intermixed with areas of larger nodules and linear shadows (A and B, yellow circles). Note the enlarged lymph node in the aorto-pulmonary window (A, arrow).

Follow Dr.Pepe’s Advice:
1. When acute miliary disease is discovered, always rule out miliary TB.
2. The most common cause of a chronic miliary pattern is silicosis.
3. Chronic miliary nodules and egg-shell calcification are highly suggestive of silicosis.
4. When a chronic miliary pattern with nodules of different sizes is discovered, think of metastases.


Hello,
There is diffuse reticular interstitial opacification. With pasy history I suppose lymphangitis carcinomatosis.
So answer 2.
In right axillary region are some vessel clips after surgery lymph node resection?
Yes, the surgical clips are from a previous resection
I hope that not only this part of my answer is true:)
My lips are sealed 😉
There is air space opacity in left mid lung zone silhouetting part of left heart border,likely representing consolidation/ collapse in lingula lobe, it is also surrounded by focal area of reticulonodular pattern ,so from choices above,tuberculosis is most likely.
Lymphangitis Carcinomatosa
If a single answer was required it would be lymphangitis carcinometosa.
However, the pleural tags, diaphragm tenting, ?fibrosis left mid zone make TB a probability.
Miliary is possible in varicella, as well as initerstitial features.
So I will have to go with any of the above.
…non tbc….non esiti di polmonite varicellosa( anamnesi positiva per pregressa varicella?)….KISS regola: linfangite carcinomatosa….
I feel proud of the five brave radiologists that answered this case. The patient has a miliary pattern, that can be caused by TB, metastases and varicella. Therefore, the correct answer is 4. Any of the above. First prize goes to sht, who agrees with me.
If you think this case is difficult, wait for the next one!
.,.,grazie grande PROF.