Dr. Pepe’s Diploma Casebook: Case 91 – SOLVED!
Dear Friends,
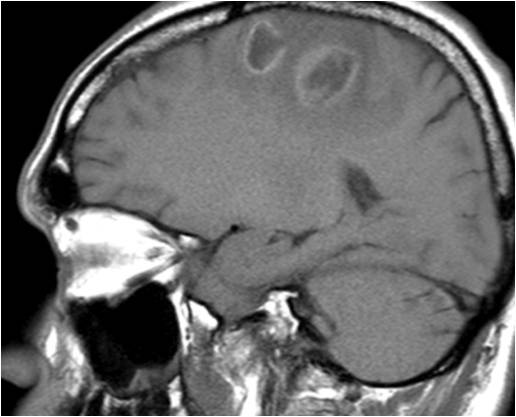
Today I am showing images of a 48-year-old man with two brain lesions and a pre-op chest radiograph. What would be your diagnosis regarding the chest?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
Diagnosis:
1. Carcinoma
2. Hydatid cyst
3. Pulmonary infarct
4. None of the above
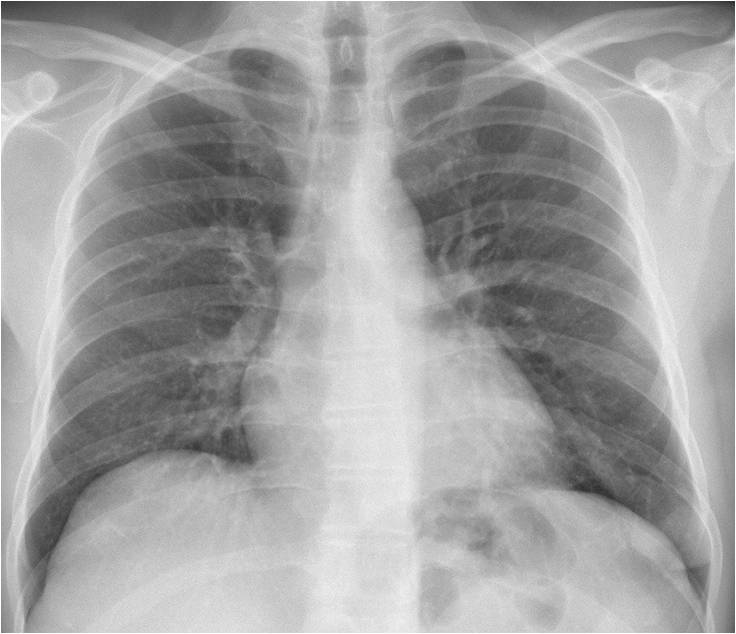
Findings: PA radiograph shows an ovoid lesion in the left costophrenic angle (A, arrow), with an oblique tubular shadow arising from the upper aspect (A, red arrow).
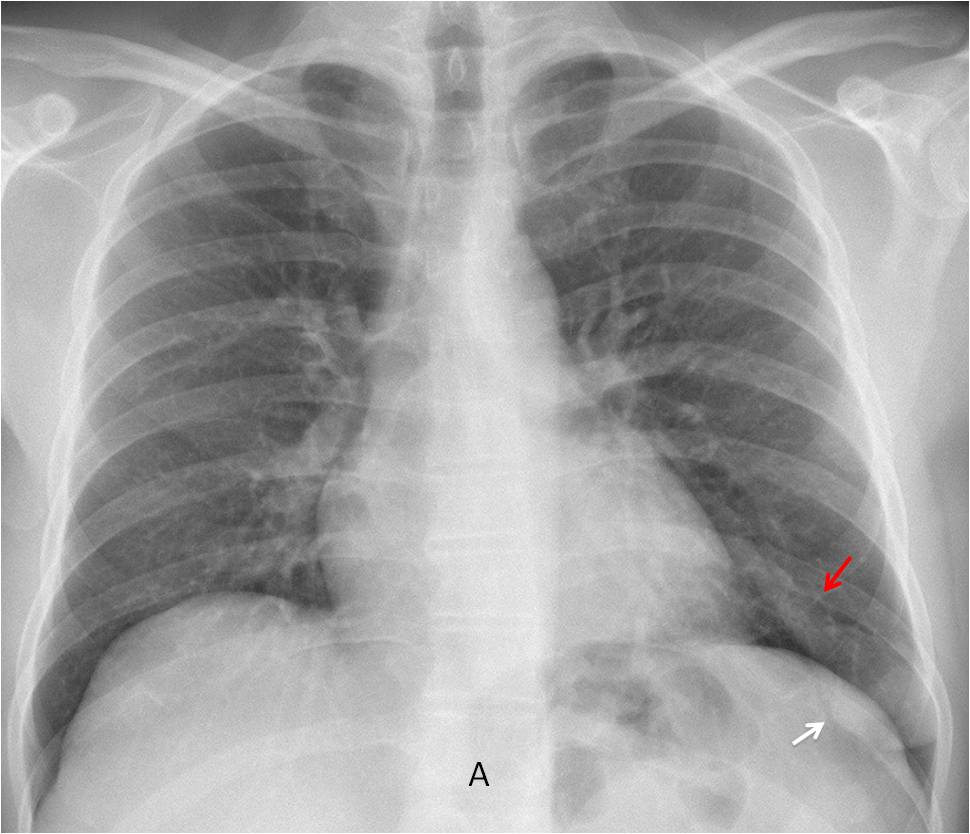
Enhanced axial CT demonstrates that the ovoid nodule and the aorta enhance at the same time (B, arrow). 3-D reconstruction shows an afferent and efferent vessel (C, arrows) arising from the nodule.
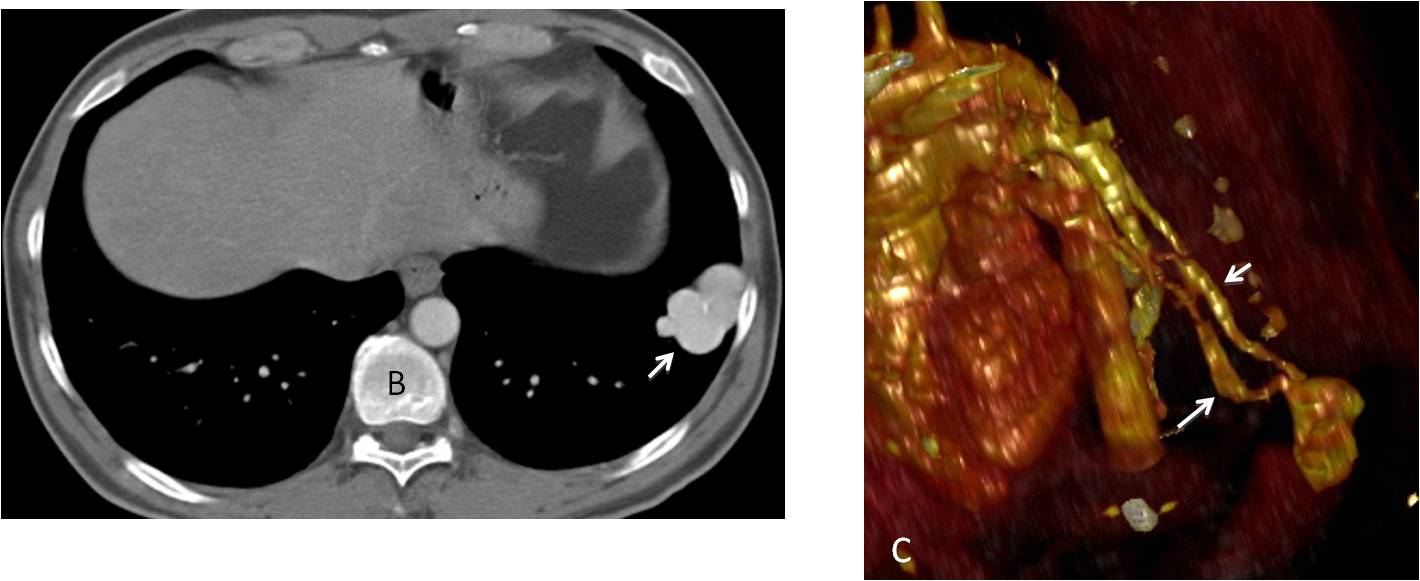
Final diagnosis: Arteriovenous malformation with embolic brain abscesses.
In Diploma Casebook case #89 I mentioned the upper corners of the PA film, depicting the shoulders. In this presentation I would like to comment on the lower corners, which correspond to the costophrenic angles (CA).
The CA is the aerated space between the chest wall and the diaphragm; it has a normal inclination of about 30º. The depth of the CA varies (Fig. 1 A and B), and it is flattened in patients with lung hyperexpansion (Fig. 1 C).
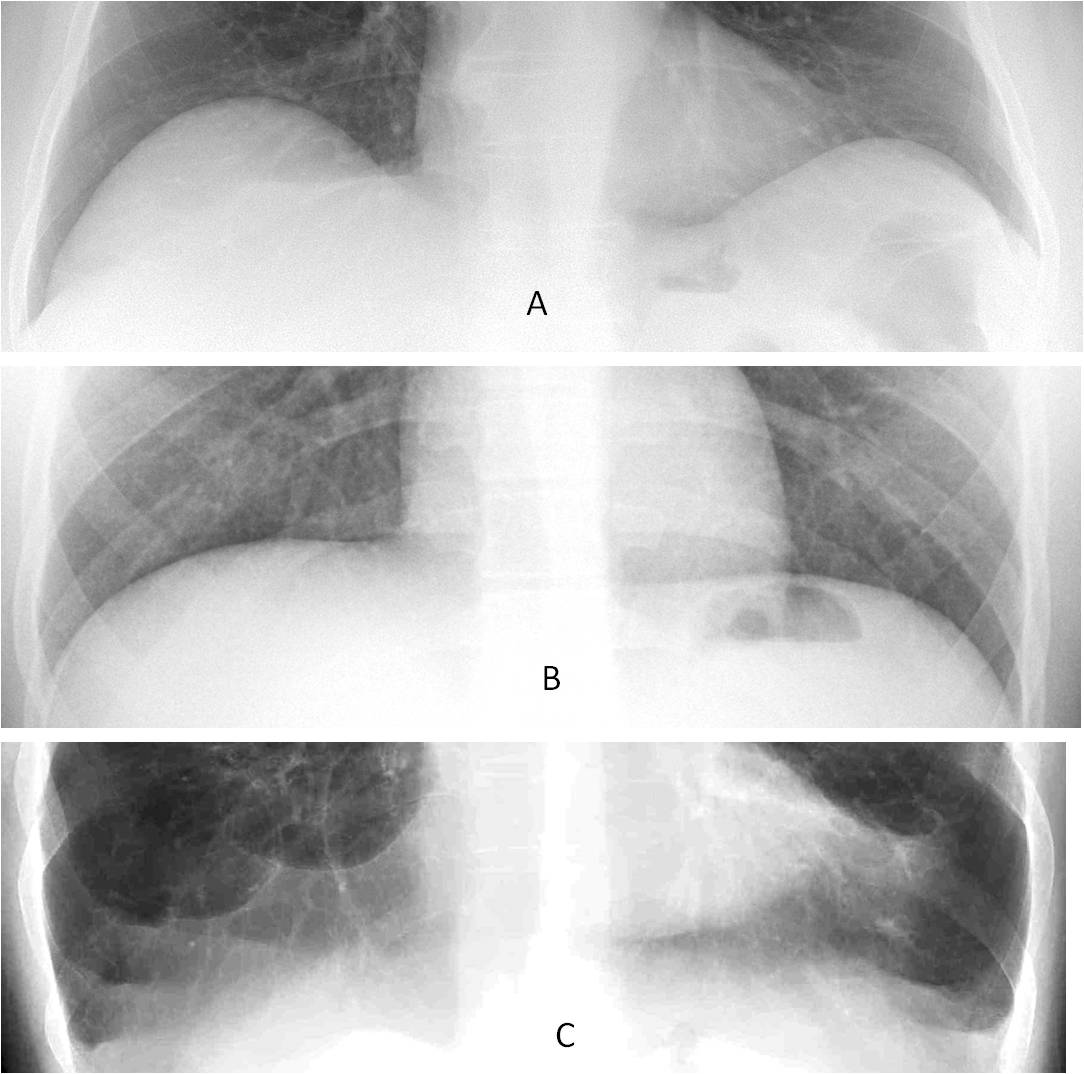
Fig. 1
Fig. 1: Two normal patients with different depths of the CA (A and B). Patient with emphysema and flattening of the CA (C).
A blunted CA should be considered abnormal, and sometimes it is the only visible abnormality in the PA radiograph. In this presentation I would like to discuss the differential diagnosis of blunted CA, based on the morphology of its upper border, which can be concave, straight, or convex .
A concave upper border of a blunted CA (meniscus sign) is a typical indication of free pleural effusion of any etiology (Fig. 2).
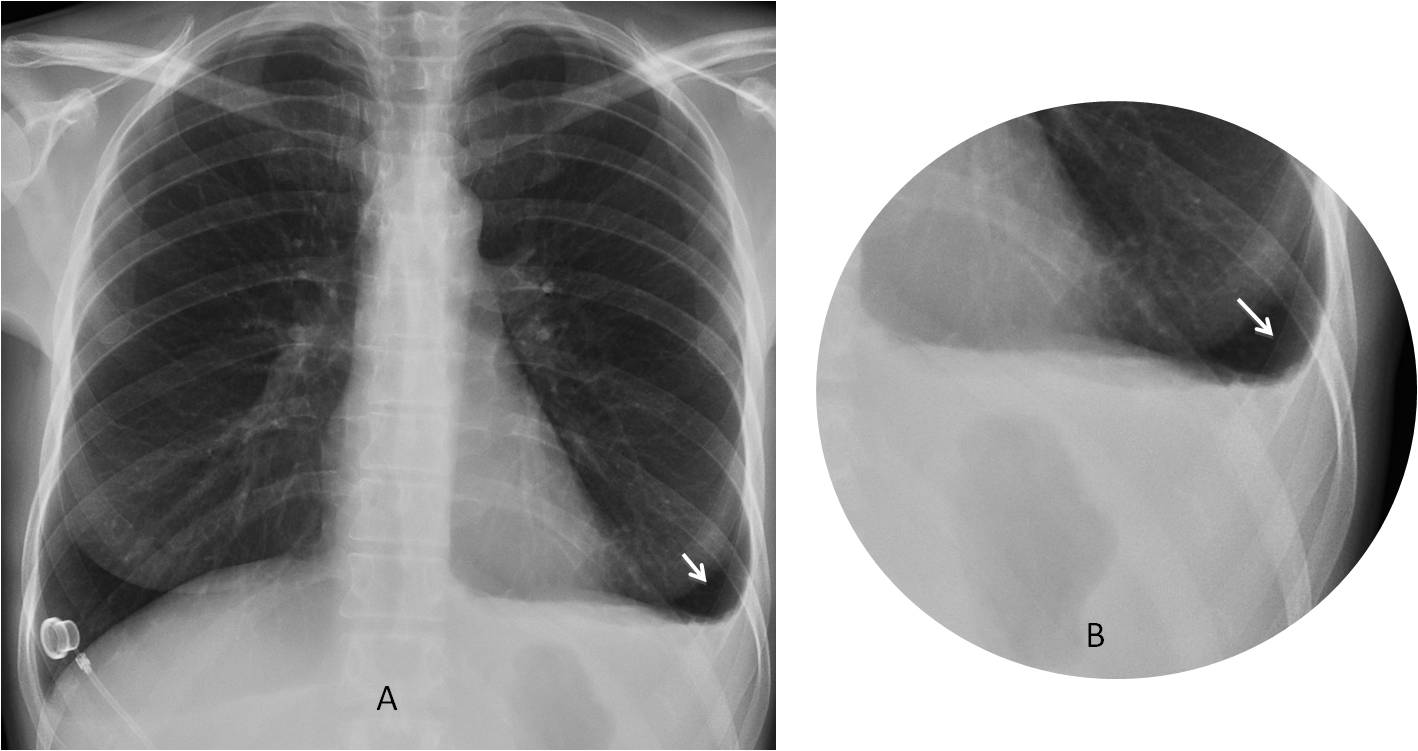
Fig. 2
Fig. 2: 47-year-old man with pancreatitis. The meniscus sign (A and B, arrows) indicates a small pleural effusion and is the only abnormality visible in the chest radiograph.
This typical meniscus is sometimes simulated by pleural thickening or loculated fluid (Fig. 3). To be certain, a decubitus view or US examination should be performed. Comparison with previous films is always useful.
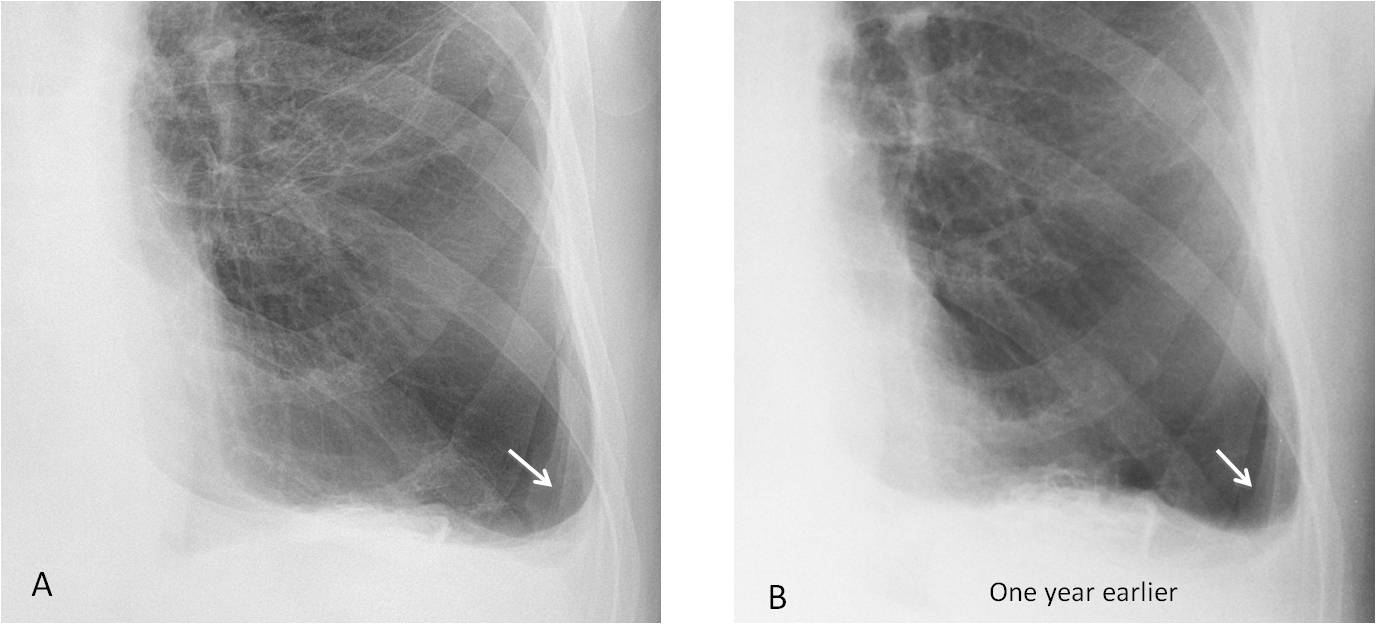
Fig. 3
Fig. 3: 56-year-old man with pleural thickening simulating free fluid (A, arrow). Radiograph taken one year earlier shows no change (B, arrow).
In my experience, a straight hemidiaphragm with a blunted CA suggests scarring from a previous condition (Fig. 4). Pulmonary infarct or previous surgery are the first to come to mind. Since I don’t have scientific data to support this, you have to trust your own judgement.
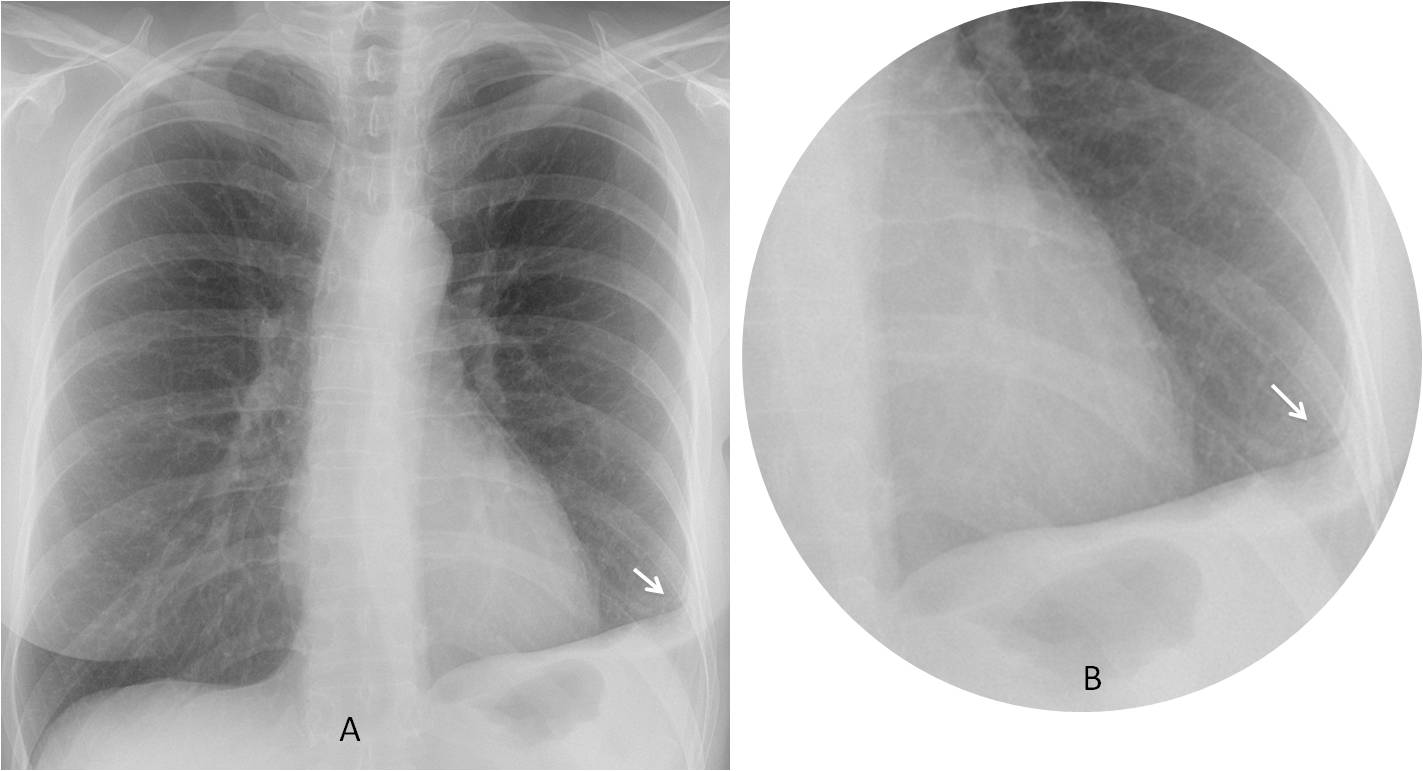
Fig. 4
Fig. 4: 49-year-old woman. The straight oblique diaphragm and the blunted angle suggest scarring (A-B, arrows). Previous history of pulmonary infarct.
A blunted CA can occur in some cases of collapse of the lower lobe (Fig. 5). Pay attention to the downward displacement of the hilum to avoid confusing pleural disease with lower lobe collapse (See Diploma case #79).
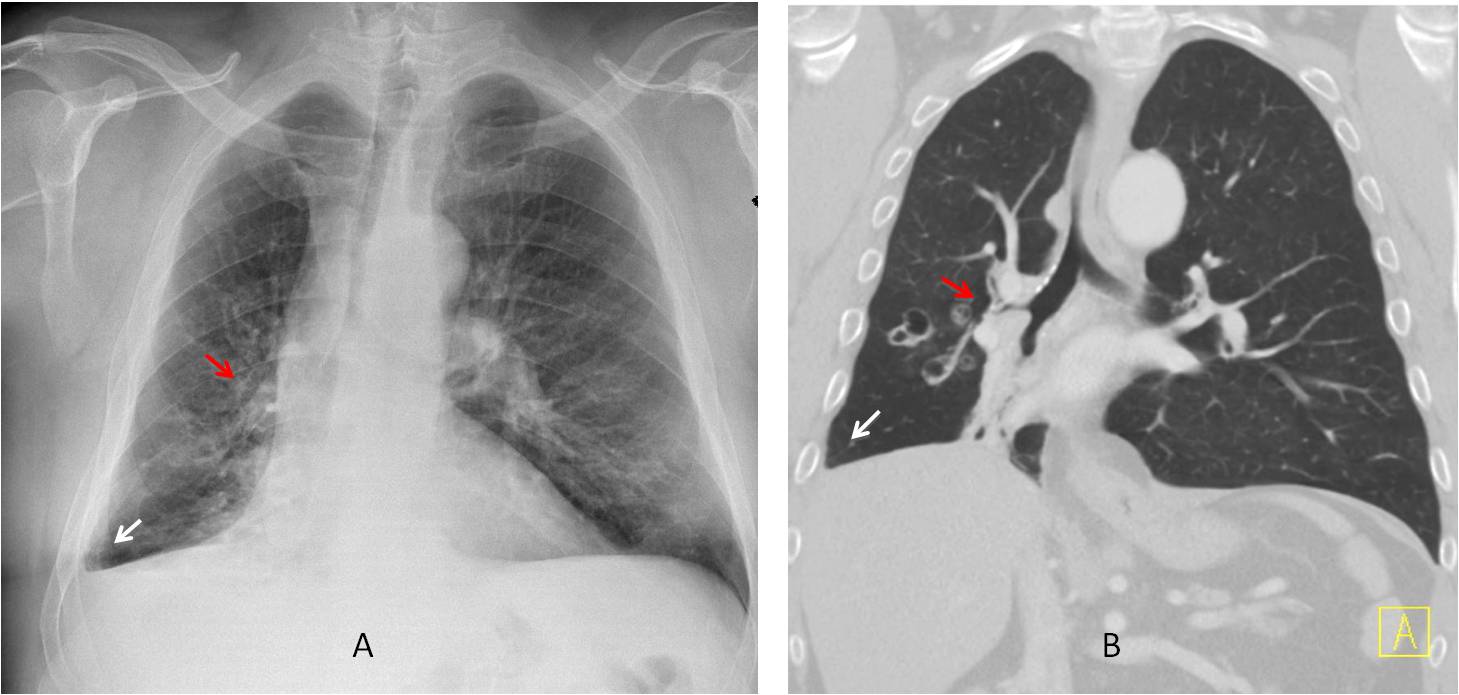
Fig. 5
Fig. 5: 69-year-old man with bronchiectasis and RLL collapse. Note the blunted right CA (A and B, arrows). On coronal CT no pleural fluid is seen. Note the descended right hilum secondary to lobar collapse (A and B, red arrows).
Convexity of the upper border of a blunted CA suggests a pulmonary condition affecting the area, especially if the border is poorly defined (Fig. 6). In the presence of a compatible clinical history, pulmonary infarction should be suspected, and enhanced CT should be performed.
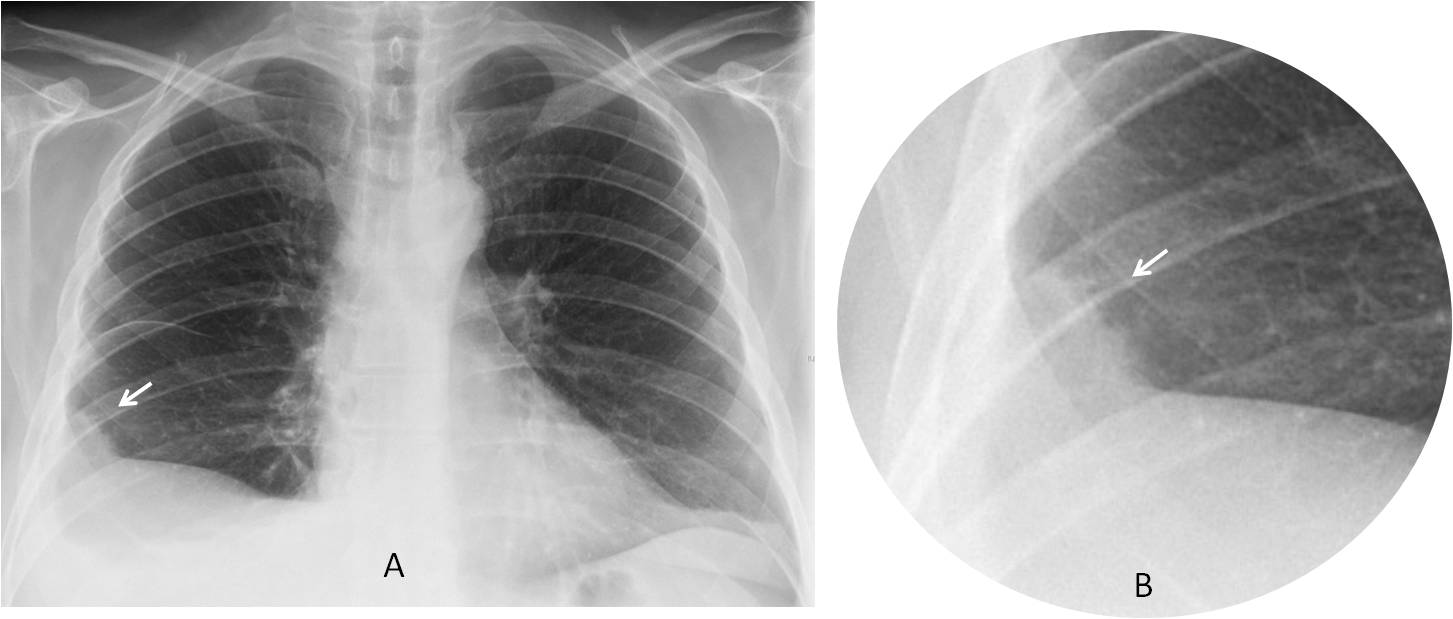
Fig. 6
Fig. 6: 54-year-old man admitted with chest pain. PA radiograph shows a blunted right CA with an indistinct convex border, a feature known as Hampton’s hump (A and B, arrows). There is a small amount of fluid in the minor fissure and plate-like atelectasis at the left lung base.
Enhanced axial and coronal CT shows pleural effusion and an embolus in the RLL artery (C and D, arrows). This study was done at 3:00 a.m. and the embolus was missed. The next day the person reading the chest radiograph discovered the Hampton’s hump, reviewed the CT, and confirmed the diagnosis of pulmonary infarct.
Fig, 6
In asymptomatic patients, another cause of a convex upper border of the CA is diaphragmatic hernia (Fig. 7). Remember that the diaphragm is a frontier organ and apparent chest lesions may arise from below.
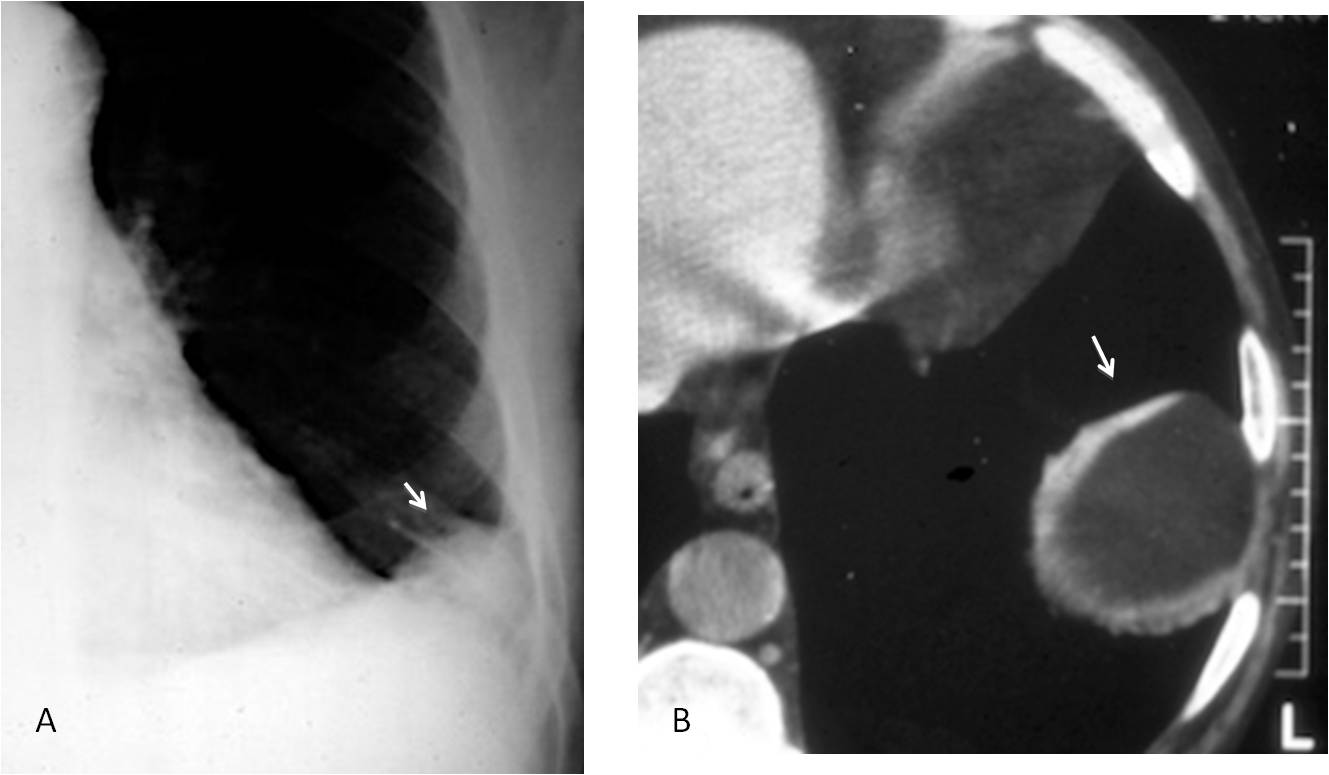
Fig. 7
Fig. 7: Blunting of the left CA in an asymptomatic patient, simulating a Hampton’s hump (A, arrow). Unenhanced CT shows herniated abdominal fat (B, arrow).
I have seen several cases of right traumatic diaphragmatic hernia in which the liver rotates and the gallbladder occupies the area of the CA (Fig. 8). I don’t know if this has been reported, but in the old days, when I saw a gallbladder in that position, I suspected traumatic hernia. And occasionally I was right.
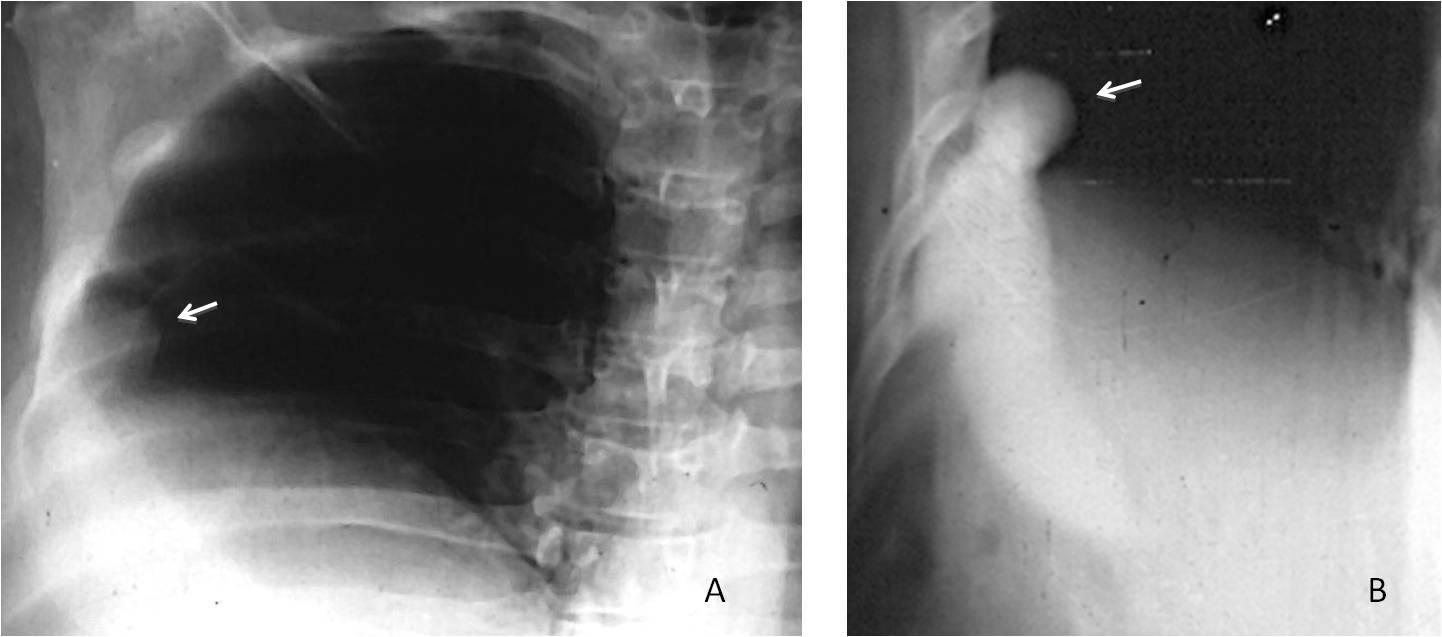
Fig. 8
Fig. 8: This is a VOC (very old case). The right CA has a convex shape (A, arrow). An oral cholecystogram (look it up in the history books) demonstrated herniation of the gallbladder causing the abnormal shadow (B, arrow). Surgical diagnosis: traumatic hernia.
The presence of one or two horizontal lines overlapping the CA (V line) is a useful indicator of pneumothorax (Fig. 9), which may be overlooked when small. The V line may be the only visible sign. If necessary, an expiration film should be performed (see Diploma case #35).
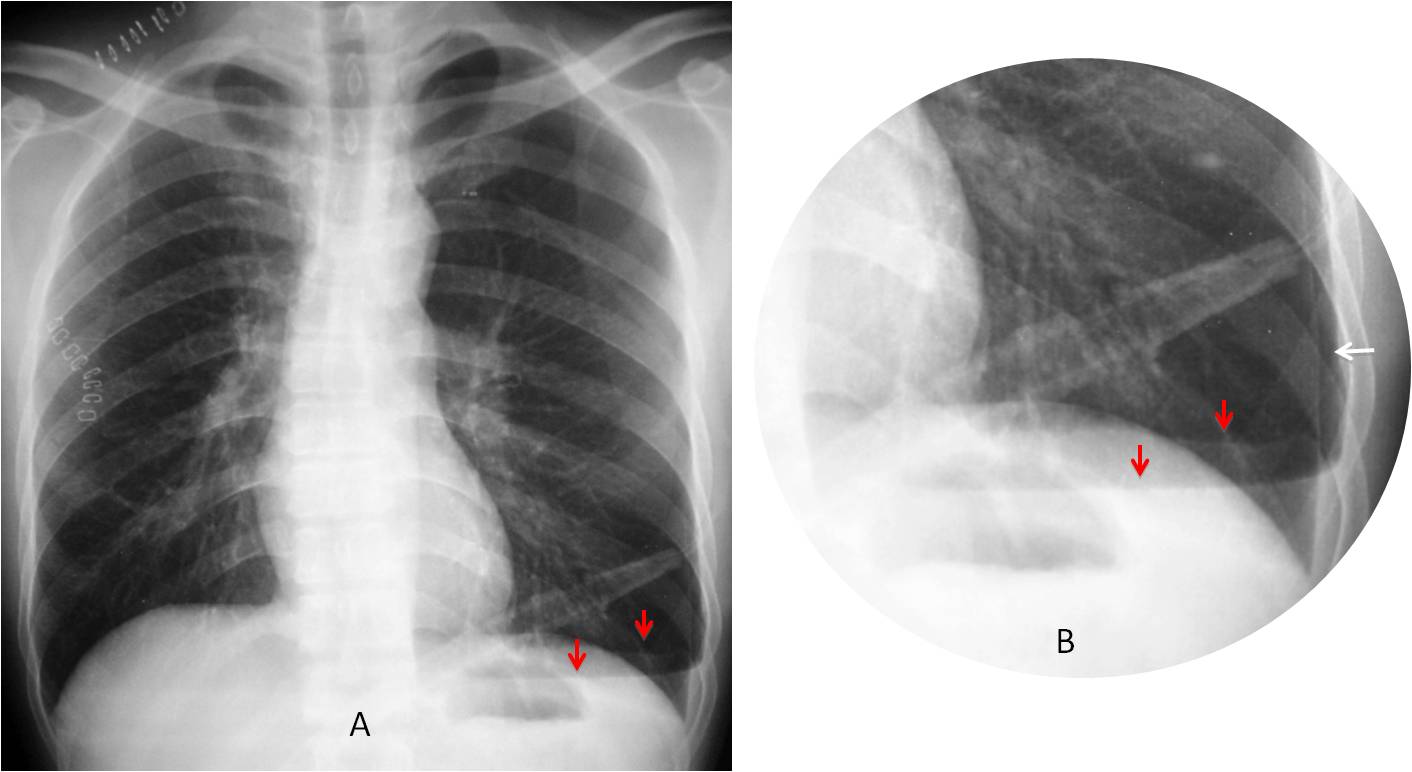
Fig. 9
Fig. 9: Typical V line. Note the two branches of the V, better seen in the cone down view (A and B, red arrows), where the pneumothorax is more evident (B, white arrow).
Occasionally, pulmonary nodules hide in the CA and may be overlooked. They are difficult to identify unless we specifically examine the CA, searching for occult disease (Fig. 10).
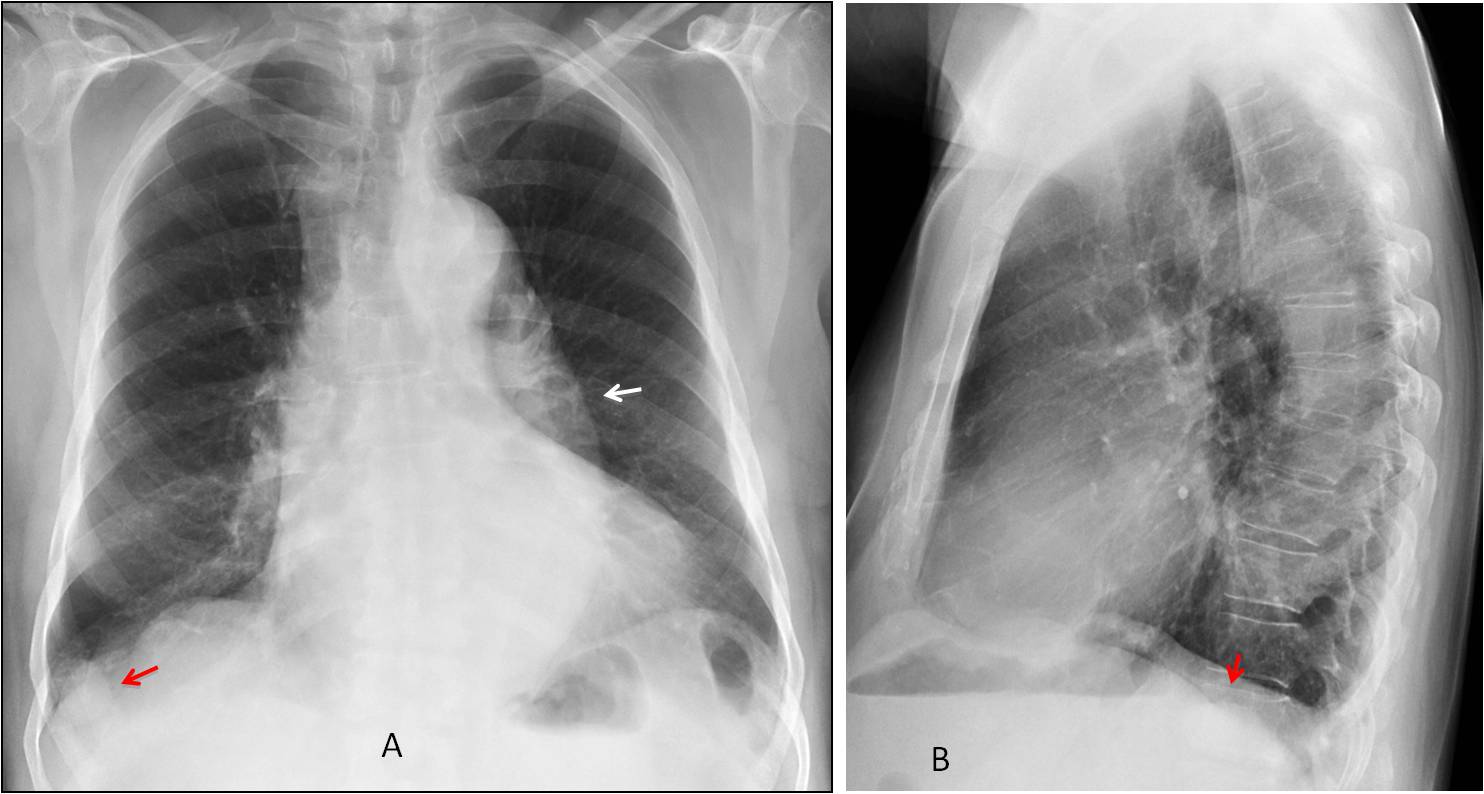
Fig. 10
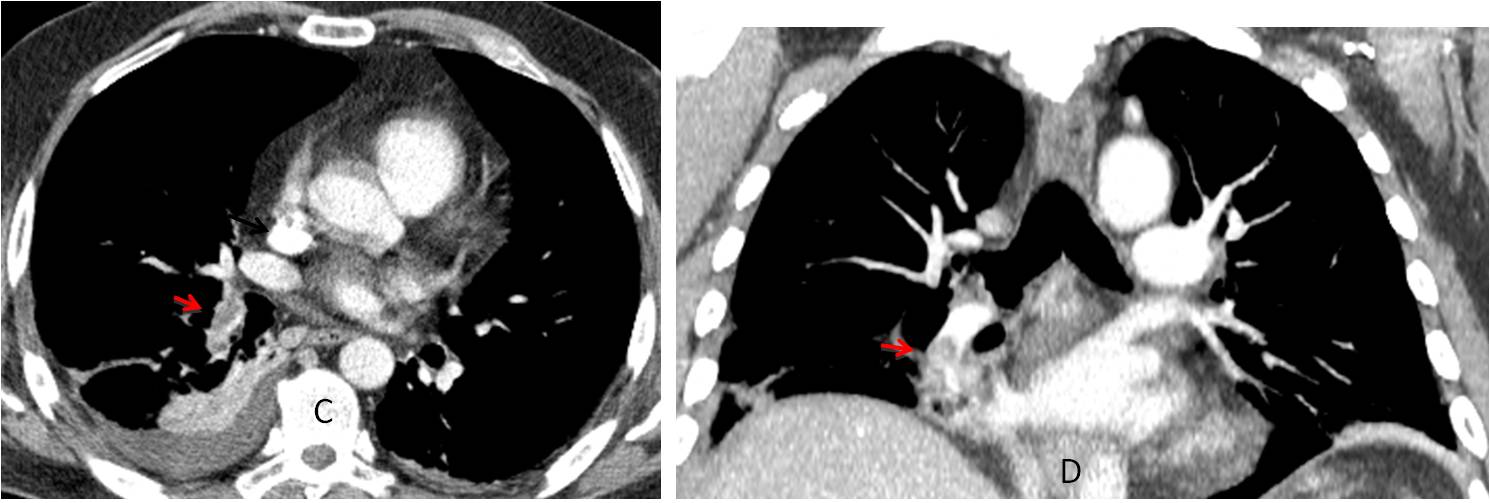
Fig. 10: 73-year-old patient with suspected aortic dissection. Note the prominent descending aorta (A, arrow). A nodule located in the right CA was overlooked (A and B, red arrow).
Enhanced axial CT confirms the dissection (C, arrow). The nodule is visible in the right CA (C, red arrow) and does not enhance after contrast injection. It measured 14 HU in the unenhanced axial CT (D, red arrow). The nodule did not change at one-year follow-up.
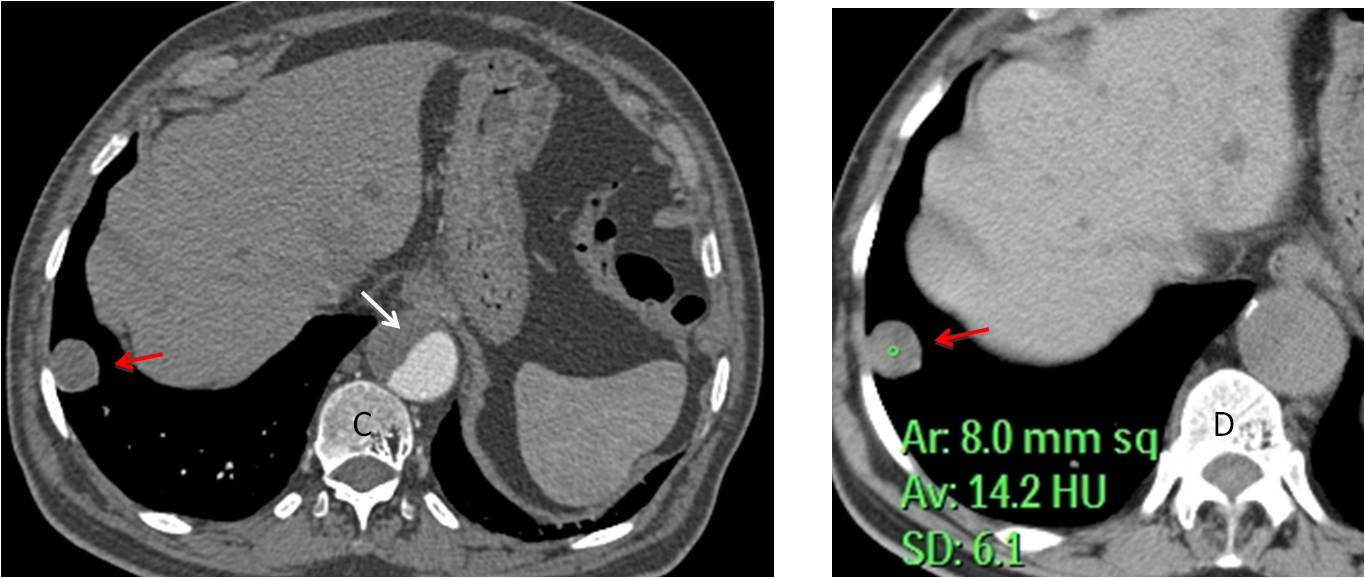
Fig. 10

Follow Dr.Pepe’s Advice:
1. The most common cause of a concave meniscus in the CA is free pleural fluid.
2. A convex shape of the CA in a symptomatic patient suggests pulmonary infarct.
3. A convex shape in a asymptomatic patient suggests diaphragmatic hernia.
4. The V line is highly suggestive of pneumothorax.


on PA view the increased vascularity in hilar and prehilar zones in both lungs and oligemia on the peripheral zones (Westermark sign), but more seen in left lung
On the left on the level of anterior part of 7-8 ribs above the costo-diaphragmal sinus there is opacity with smooth well-defined medial and lower contours, which adjacent to the chest wall laterally, in the middle of the shadow of this opacity suggesting calcification within it?
There is suggesting of enlarged vessel on the left (Fleischner sign)
Considering the asymptomatic case
suggesting – 3.Pulmonary infarction
According MRI – there are to lesions that show the contrast media enhance incomplete ring-like shape with a huge perifocal edema
suggesting demyelination (but the presence of edema could exclude it)or
Intracranial haemorrhage due to the changes in lung parenchyma because of venous thrombosis
Brain abscess and mts can not be excluded
there is broad based soft tissue opacity in left CP angle making obtuse angle with no obvious aggressive features–extrapulmonary likely pleural based.–can be pleural fibroma
Right axillary region faint rim calcified lesion–can be lymph node.
rest of chest seems to be fine.
regarding brain lesions they are showing incomplete ring enhancement favoring demyelinations.
Brain abscesses associated with vascular anomaly in a lung?
Rendu Osler Weber, pulmonary complications of shunting and brain abscess
Brain MRI: Two round lesions in cortex with ring enhancement and surrounding edema.
CXR: Round opacity with smooth margin left base, ?anterior as dome unaffected.
Another soft opacity with smooth margin in the right paratracheal region.
Ans: None of the above.
Does the response ‘carcinoma’ cover secondaries?
In yes, then ans could be carcinoma.
yes, carcinoma cover secondaries. But it is not a carcinoma. Sorry 😉
Rounded soft tissue opacity in the left lung base with calcific focus in centre, suggestive of calcified granuloma due to healed tuberculous infection.
Ring enhancing lesions in the parietal lobe with surrounding edema, suggestive of tuberculomas.
Overall conclusion is that of intracranial tuberculomas from reactivated pulmonary tuberculosis.
….la risposta dovrebbe essere la 4: nessuno dei precedenti….in base all’rx torace, si può escludere il CR ed il tubercoloma….ma anche la cisti idatidea polmonare perchè la formazione sembra di pertinenza pleurica….le due formazioni all’rm presentano cararatteristiche di natura infettiva, “matura”, come da ascessi e-o granulomi infettivi….come è il profilo immunologico del paziente ?…..CAMPEONES!!!!Felice per il Barca….noi a Bari stiamo soffrendo…..andiamo ai play-off….
Dear friend, look at the answer tomorrow. Força Bari!
Late in the day, giving credit to Uli, who made the correct diagnosis.
Images and final answer tomorrow
PAVM
PAVM with brain abscess