Dear Friends,
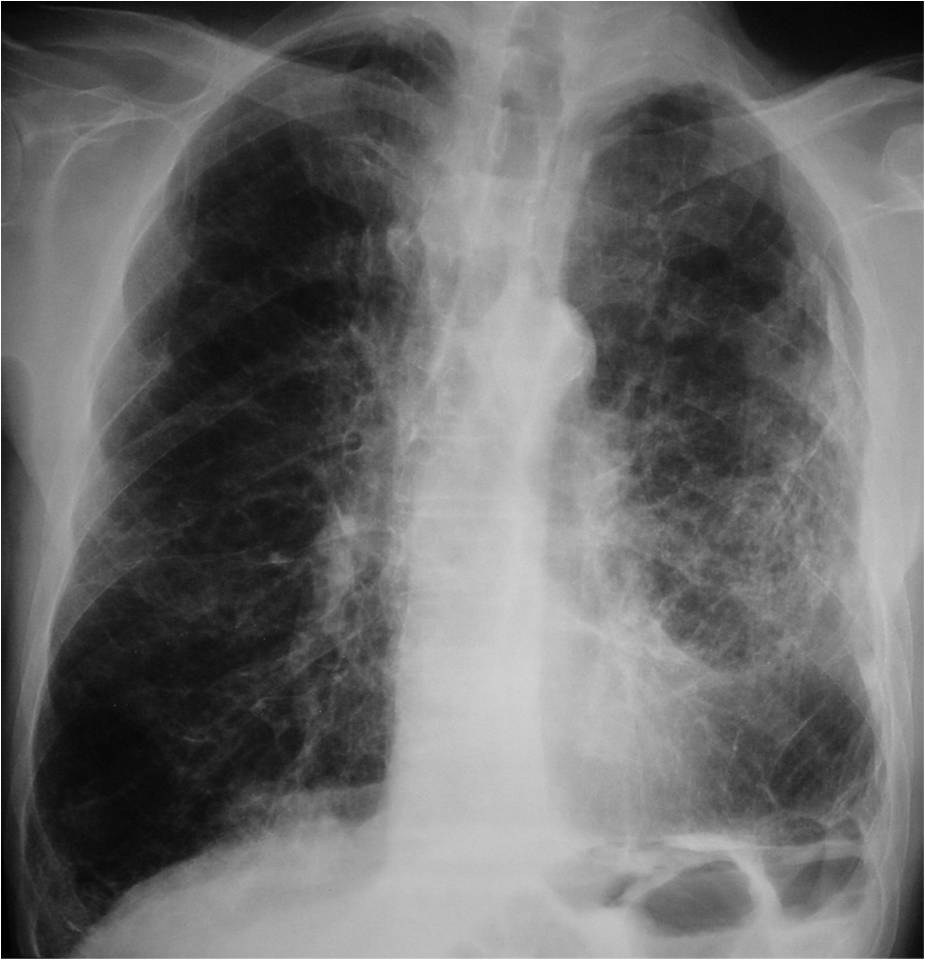
Today we are showing chest radiographs of a 75-year-old man with a cough and haemoptysis.
What do you see? Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.

Click here for the answer to case #152
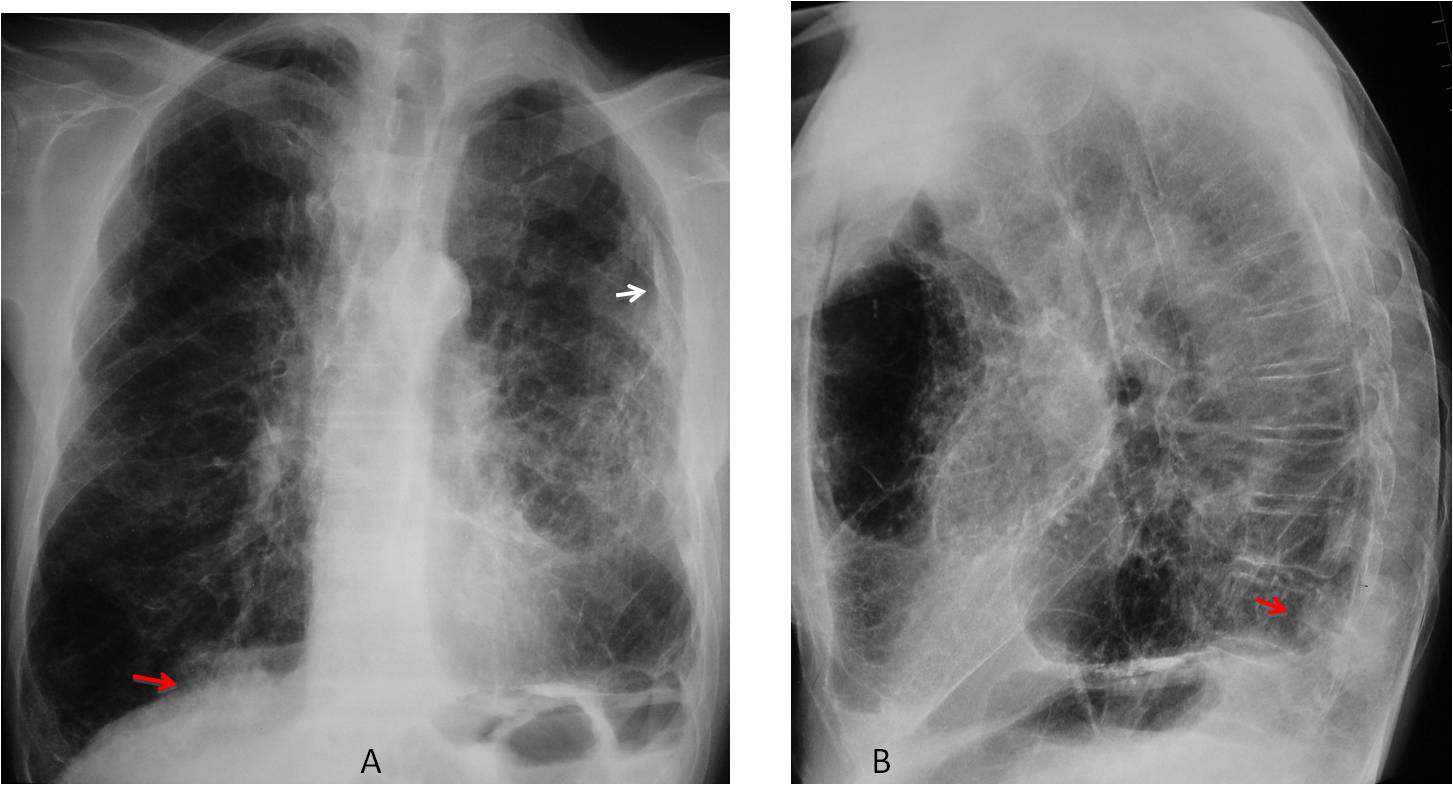
Findings: PA view shows emphysematous lungs with chronic fibrotic changes on the left and pleural calcification (A, arrow). The most important finding is a hidden mass in the RLL, barely visible in the PA radiograph (A, red arrow) and well seen in the lateral view in the posterior costophrenic angle (B, red arrow).
Coronal and sagittal CT confirms the presence of the mass (C-D, red arrows).
Percutaneous biopsy confirmed malignancy.
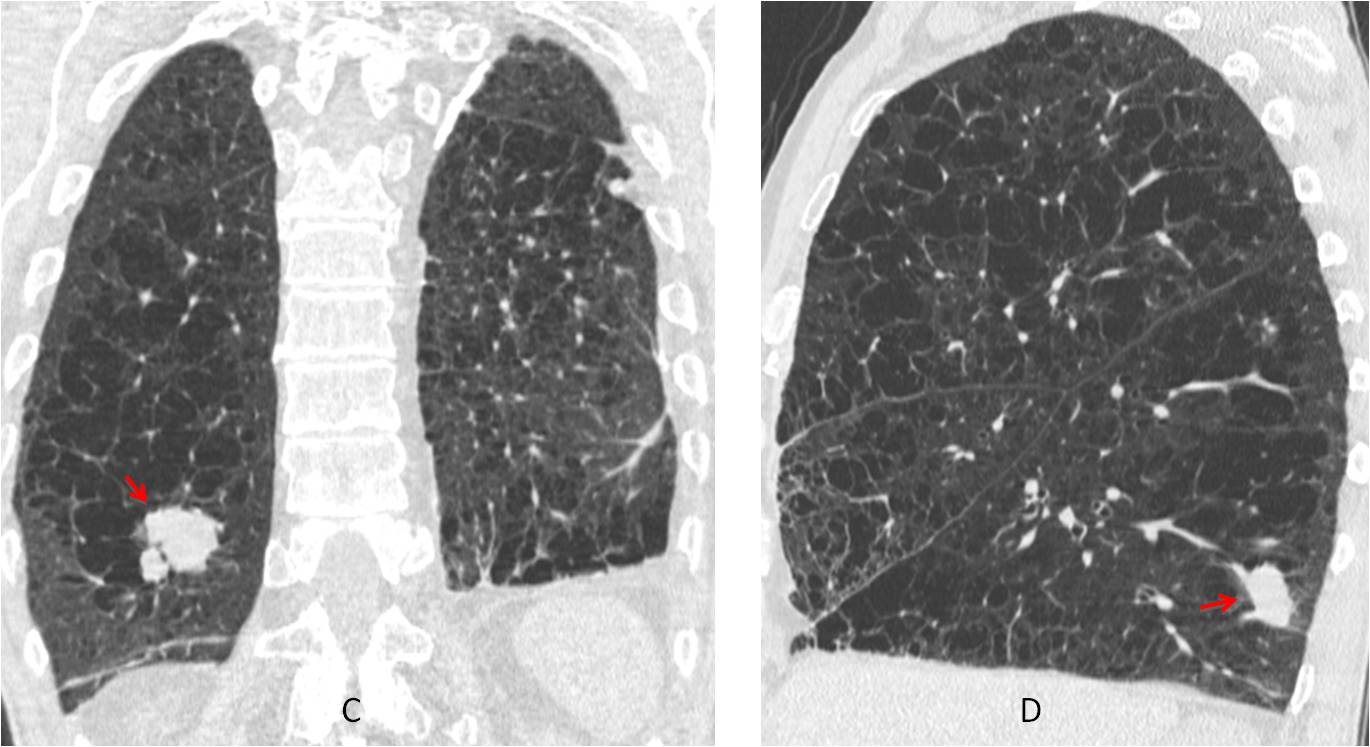
Final diagnosis: partially hidden adenocarcinoma of lung
Congratulations to Mahmoud, who was the first to see the carcinoma
Teaching point: remember the basics. Using checklists helps to find pathology that will be overlooked otherwise.


Emphysematous thorax with flatened of both hemidiaphgrams. There is loss of volume of the left hemithorax, with multiple tracts and intersticial thickening. Cardiac sillhoute sign is present. An intersticial pathology (pneumoconiosis, TBC…) can be suggested.
we think there is a nodular opacity with air adjacent to the left hilum, what can represent crescent air sign (aspergiloma?).
Not real. Try again 😉
fibrosing lung disease with superimposed infection on the left mid pulmonary field and ipsilater pleural effusion. It seems to me.
There is unilateral calcified pleural plaques along left hemidiaphragm and left lateral chest wall, findings that suggest previous TB, other DD: previous empyema or hemothorax.
also there is small volume of left lung with dense reticular opacities denoting fibrosis.
Also there is left upper mediastinal opacity, along with small volume of left lung and elevated left hilum, it suggests tight left upper lobe collapse.
Only four answers and none right. I feel in a “to be or not be” state (hope you know the movie).
Review the basics and try again!
There is a large opacity projected on lower dorsal spine in lateral view
In frontal view, it’s seen in left retrocardiac position with its lateral border parallel to the outline of descending aorta, likely represent posterior lung mass, lung cancer.
I hope I’m now “to be”.
Yes, you are
Thank you prof
alla base polmonare “dx” , in laterale sovrapposta alla colonna vertebrale…..opacità di massa…
Hi!lung mass on the ground of chronic pneumoconiosis or TB
(because of pleural calcification and fibrous elements)with unilateral localised lymphagitic carcinomatosis?!