Welcome to the sixth season of Cáceres’ Corner. I will present cases during the month of September because Dr. Pepe is vacationing in Menorca with Miss Piggy and will not start the Diploma cases until October.
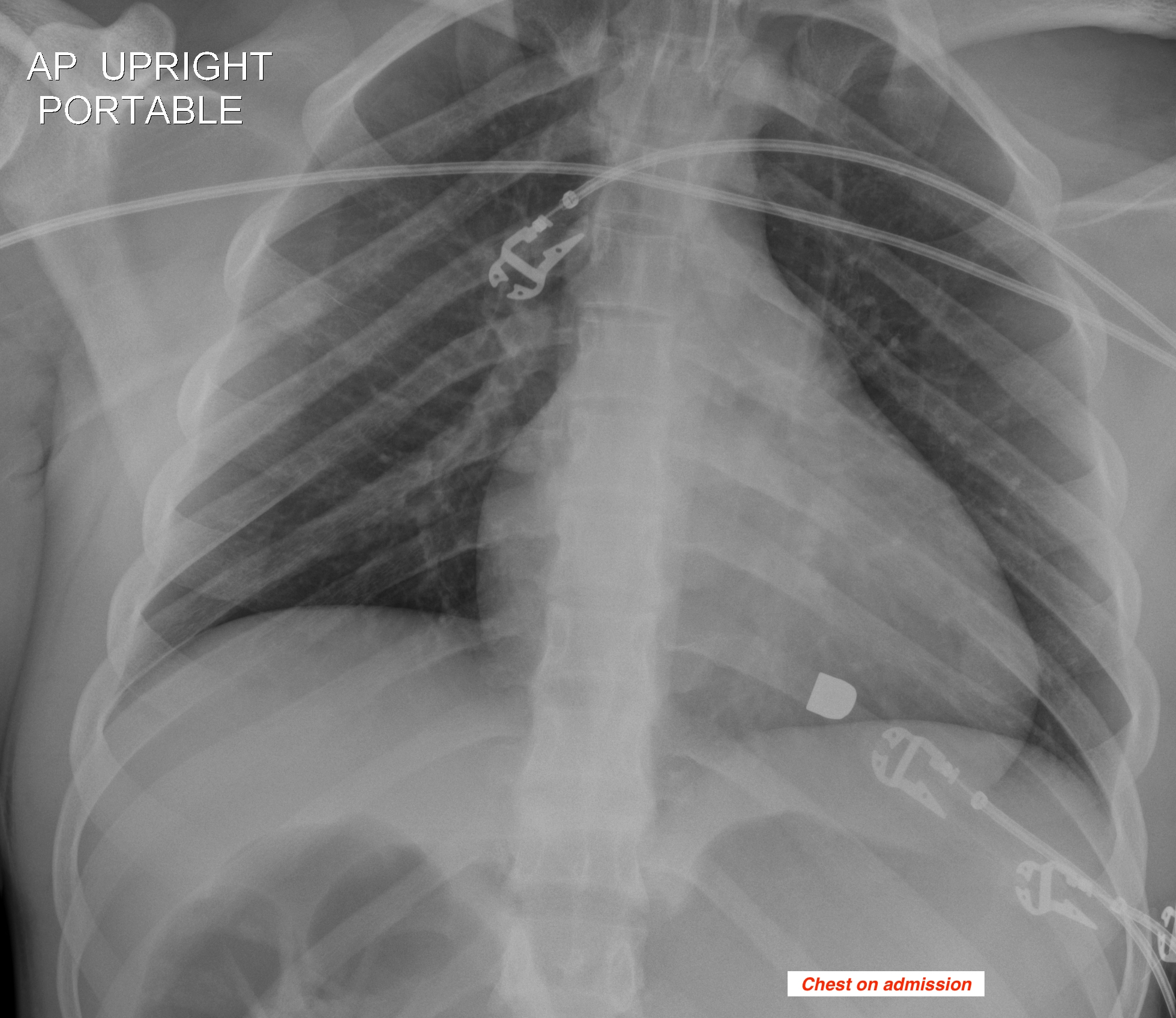
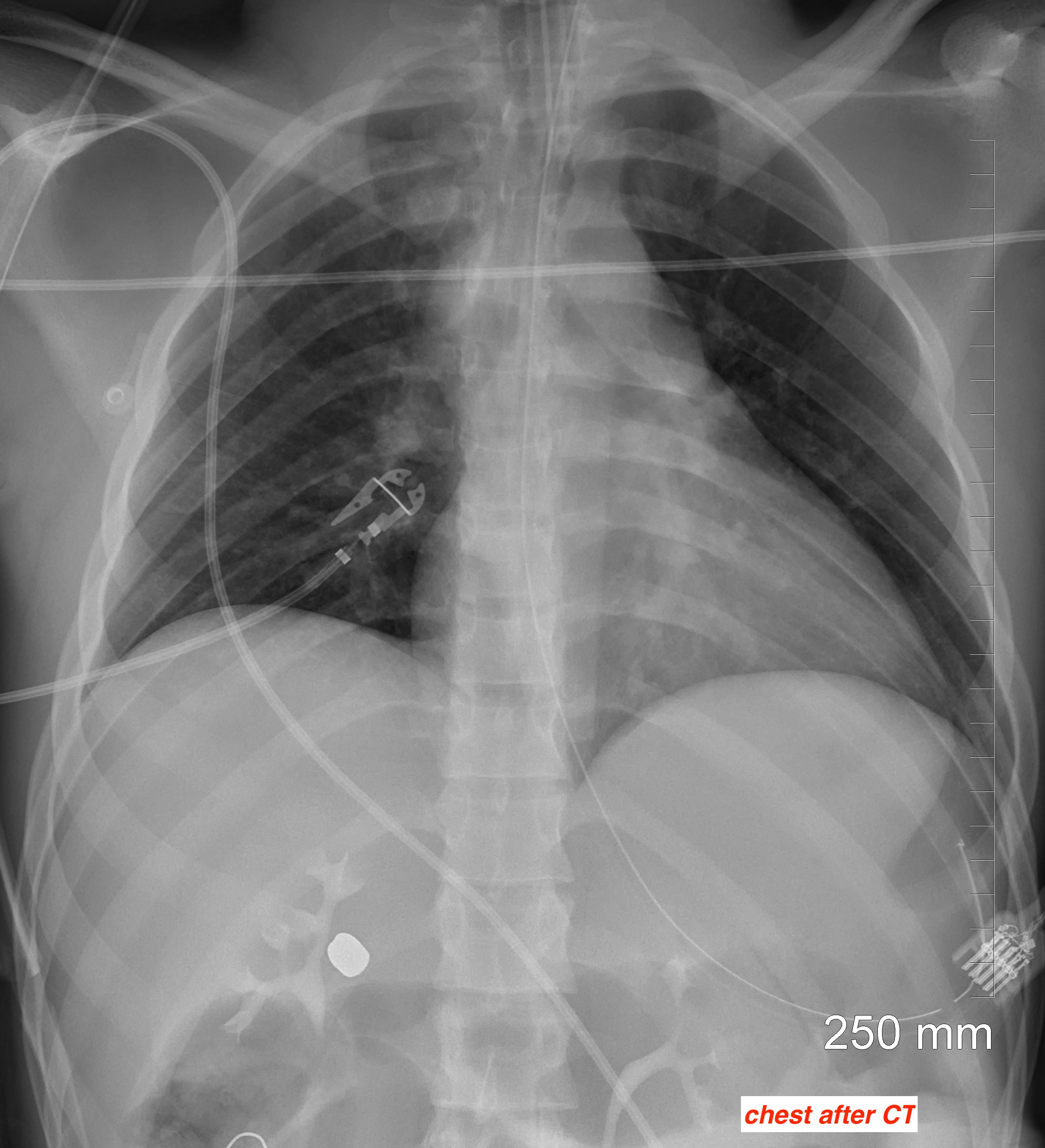
My close friend Larry Goodman, Director of Chest Imaging at the Medical College of Wisconsin, provides the first case. The images are of a 27-year-old male who was shot in the abdomen. I am showing chest radiographs taken on admission and after a CT was performed.
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
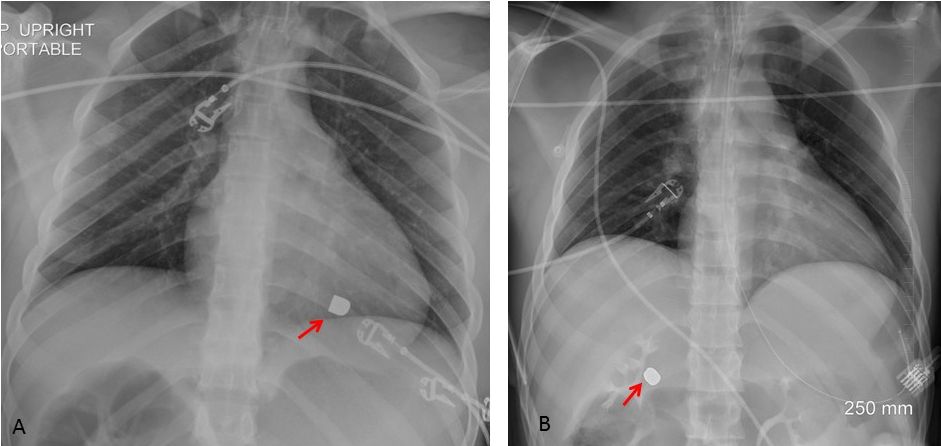
The main finding in the admission chest is a bullet overlying the cardiac shadow (A, arrow). A second chest radiograph after CT shows the bullet in the right upper quadrant of the abdomen (B, arrow). Considering that the patient was shot in the abdomen, it is obvious that the bullet has travelled from the abdomen to the chest and returned to the abdomen
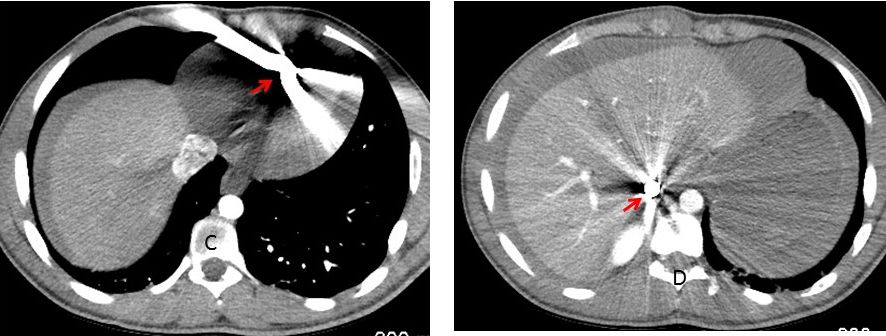
I have received ingenious suggestions regarding the possible paths of the travelling bullet, but the most credible one is that it is travelling through the blood vessels. This is confirmed by CT images, which show the bullet in the right ventricle (C, arrow) and a few seconds later in the IVC (D, arrow).
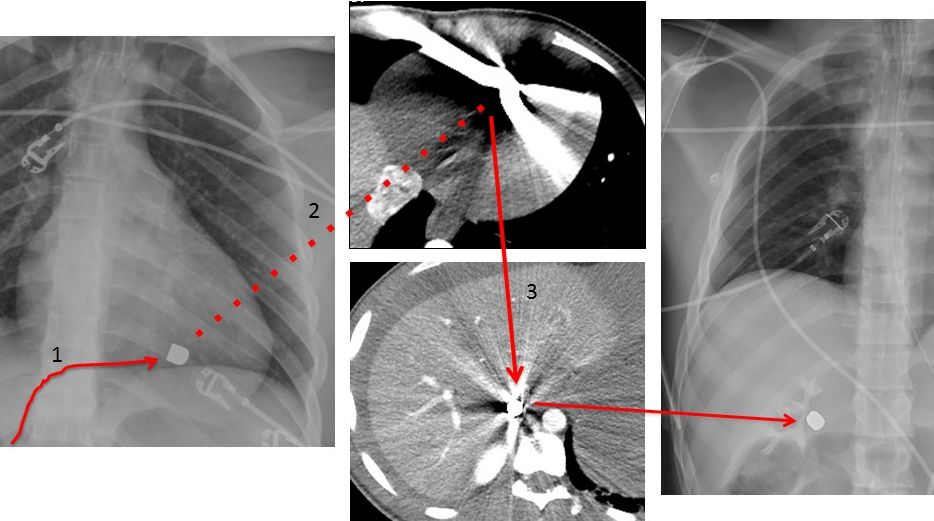
The most likely path is then: departing from the IVC (1), the bullet reaches the RV (2) and then follows a retrograde path to the IVC again (3) as shown below. An alternative explanation would be an intracardiac shunt or a pulmonary AV fistula, but there is no evidence to support this hypothesis.
The patient had a laparotomy where several internal injuries were repaired including a rent in the inferior vena cava. No bullet was found.
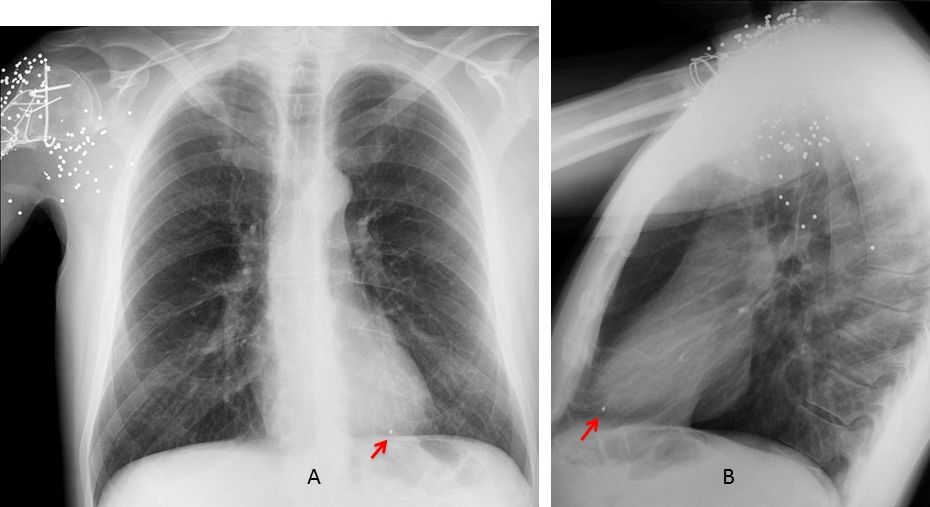
Wandering bullets have been reported previously. In Spain we are more primitive and use shotguns. Radiographs below show a patient shot in the shoulder. A single pellet has emigrated through the veins to the RV (A-B, arrows).
Congratulations to all of you, because it was a hard case. Olena was the first to mention the vascular route and TR brilliantly summarized it.
Teaching point: this is an unusual case and brings to mind the words of Sherlock Holmes: “Once you eliminate the impossible, whatever remains, no matter how improbable, must be the truth”.


Hello after holiday dear professor:)
On second picture I think about deep sulcus sign on left in pneumothorax.
Is that metalic object a bullet? I dont know why its moving – inside gi tract?
Greetings
Welcome back, dear friend. Don’t you think that the bullet in the chest is too high to be in the stomach?
That’s truth it’s above diaphragm. In the absence of hernia or rupture of diaphragm – I can’t see any signs of it – it’s too high to be in the stomach.
Quite strange bullet journey. In clinical history patient was shot in the abdomen – maybe it’s come back by bullet track in chest-abdomen walls?
Or drown from soft tissue chest wall into peritoneal cavity?
there are the shadows of ecg electrodes seen on both side
on the right there is a small apical pneumothorax on the first AP chest radiograph on admission
and the “bullet-like” shadow on the left overlaying the shadow oh the posterior part of 9 rib – I suppose this shadow has too smooth and well-defined contours to be a bullet
i suppose the pneumotorax was resolved after CT administration before the second chest X-ray
on the second chest x-ray we can see the contrast in calyces and renal pelvis of both kidneys with further contrast in left ureter. at the same time it seems there is no enhanced the write ureter (ruptured ?) closer to vertebral column on the level of the Th12 on the right side there is seen the probable bullet of oval shape
is this bullet in the kidney?
I am not confirming or denying it. How do you explain it got there?
it will sounds absurdly but maybe the bullet was in the left ventricle and with the blood flow traveled?
the bullet could be small enough
silly, I suppose?
Not silly at all. Let us pause the discussion and return to it tomorrow. In the meantime, think about the bullet
I read about the bullet embolism but from heart to pulmonary vessels – they are big enough.
in this case the only vessel I can think about is right renal vessel but according normal anatomy it is too small – 5-6mm in diameter
Welcome, dear Olena. The bullet is definitely a bullet. While in USA, I saw many of them.
CT did not confirm a pneumohorax, nor did it show any problem with the ureter
soft tissue, lung parenchima look normal
there is no tear of diaphragm and the air in the addomen
no rib fractures
she is intubated and has nasogastral probe
is there a wrong position of the right subclavian cathether (if it is a cathether and not any other external device)?
Welcome Dr. Cáceres!!!
Is it possible that the bullet was outside the body??
Welcome Dr. Cáceres!!!
Is it possible that the bullet was outside the body??
Very good idea. Sorry, bullet is inside the body
In the second X-ray there is an increased convex density under the left diapgrahm that is pushing the stomach (nasogastric tube is displaced laterally) and the kidney. Perhaps there is a postero-inferior haemathoma…..
Greetings,
in the admission radiograph, the bullet can be in three possible locations: inside the heart, posterior or anterior to it, so if it was the inside the heart, then it seems that it has migrated within the great vessels to the abdomen, the renal excretion looks symmetrical?, so there a low possibility that the right renal vessels are affected.
And if it was posterior or anterior to the heart then it has migrated to the abdomen through a diaphragmatic defect, which is expected in this case.
so the bullet has migrated though a diaphragmatic defect or within the great vessels.
thanks
You deserve to know that the bullet was located in the right ventricle in the admission film. This raises two interesting questions:
1. Considering that the patient was shot in the abdomen, how did it get there?
2. How did it travel from the RV back into the abdomen? (second chest film)
Greetings,
there are two possibilities how it reached the RV:
-through the IVC.
-directly through the diaphragm and RV ventricular wall, although no evidence of hemopericarduim, but there is mild widening of the superior mediastinum in the second film compared to the first.
There are two possibilities how it migrated back to the abdomen:
– through the aorta, which makes sense because of the blood flow direction, but in this case a R-L shunt is needed, either congenital or traumatic.
– through the IVC, in this case it must have been regurgitated through the tricuspid valve and the gravity drove it down against the flow direction.
thanks
Ad.2 Could be pushed back by IVC after CPR.
….avevo dimenticato la lunga vacanza….scusa per il ritardo………il tragitto del proiettile è stato dal basso verso l’alto e quindi, attraverso lo stomaco è giunto nel ventricolo dx…..la contrattilità del cuore, evidentemente, lo ha risospinto nello stomaco, perchè probabilmente era rimasto intrappolato nella parete ventricolare, ma non proprio nella cavità—–con cari saluti da Bari.
Welcome, old friend.
Better late than never!
hyper ventilation left upper lobe lung with wide inter costal spaces
Lt sternoclaviular joint not clearly defined ( fructure)