Dr. Pepe’s Diploma Casebook: Case 45 – SOLVED!
Dear Friends,
Today I am presenting the case of a 73-year-old woman who had preoperative radiographs for haemorrhoid treatment.
Check the two images below and leave me your comments and diagnosis in the comments. Come back on Friday for the answer!
Diagnosis:
1. Cyanotic heart disease
2. Acyanotic heart disease
3. No heart disease
4. None of the above

73-year-old woman, PA chest

73-year-old woman, lateralchest
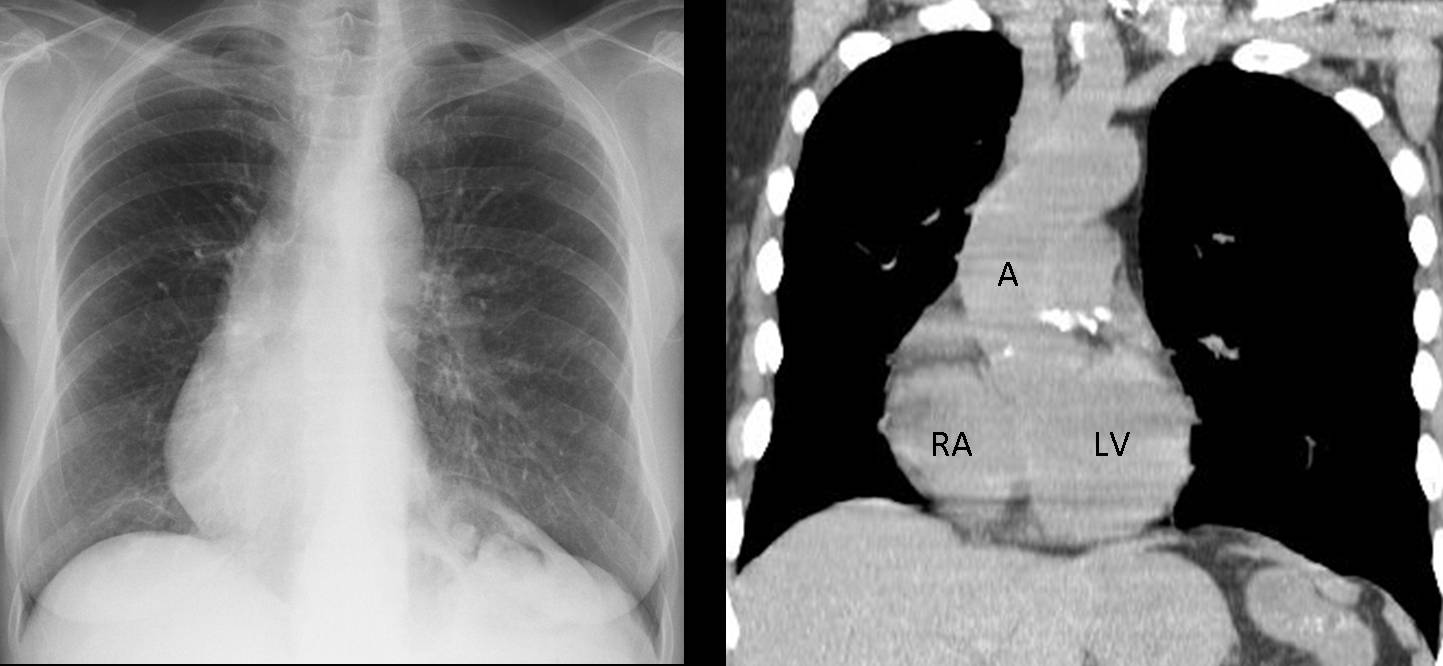
Fig. 1
Findings: PA radiograph shows that most of the heart occupies the right hemithorax. Aorta and gastric fornix are on the left side. On unenhanced coronal CT, the aorta and cardiac chambers are in the normal position (A, aorta; RA, right atrium; LV, left ventricle). Abdominal viscera are in their normal location. EKG and echocardiogram were normal, and there was no clinical evidence of heart disease
Final diagnosis: incomplete rotation of the heart (cardiac dextroversion)
This case is shown to introduce the subject of dextrocardia in adults. For clarity’s sake, I am using dextrocardia as a descriptive term, meaning that most of the cardiac silhouette lies in the right hemithorax, without specifying the cause. If you are like me, the word dextrocardia elicits thoughts of complicated congenital heart disease. However, I realised long ago that these patients undergo surgery in childhood and arrive at adulthood with a clinical history and telltale surgical changes that allow you to recognise them easily (Fig. 2)

Fig. 2
Fig. 2 (above): a 35-year-old woman with dextrocardia and transposition of great vessels, corrected at eight years of age. Note the post-surgical changes in sternum.
Furthermore, I have found that the great majority of non-operated adults with dextrocardia do not have intrinsic heart disease. The anomalous position of the heart is due either to changes in the rotation of the heart or to causes related to the neighboring structures. This ‘innocuous’ dextrocardia is the subject of this presentation and should be recognised as such, to avoid taking the wrong diagnostic path.
The most common types of heart rotation changes in the adult are situs inversus totalis and the above-mentioned cardiac dextroversion.
In situs inversus totalis the organs are a mirror-image of the normal positioning. The incidence is about 1 in 8,500 individuals, and it is usually discovered incidentally. Associated congenital heart disease is seen in about 3% of cases (1% in normal population). About 20% of patients have primary ciliary dyskinesia (Kartagener syndrome).
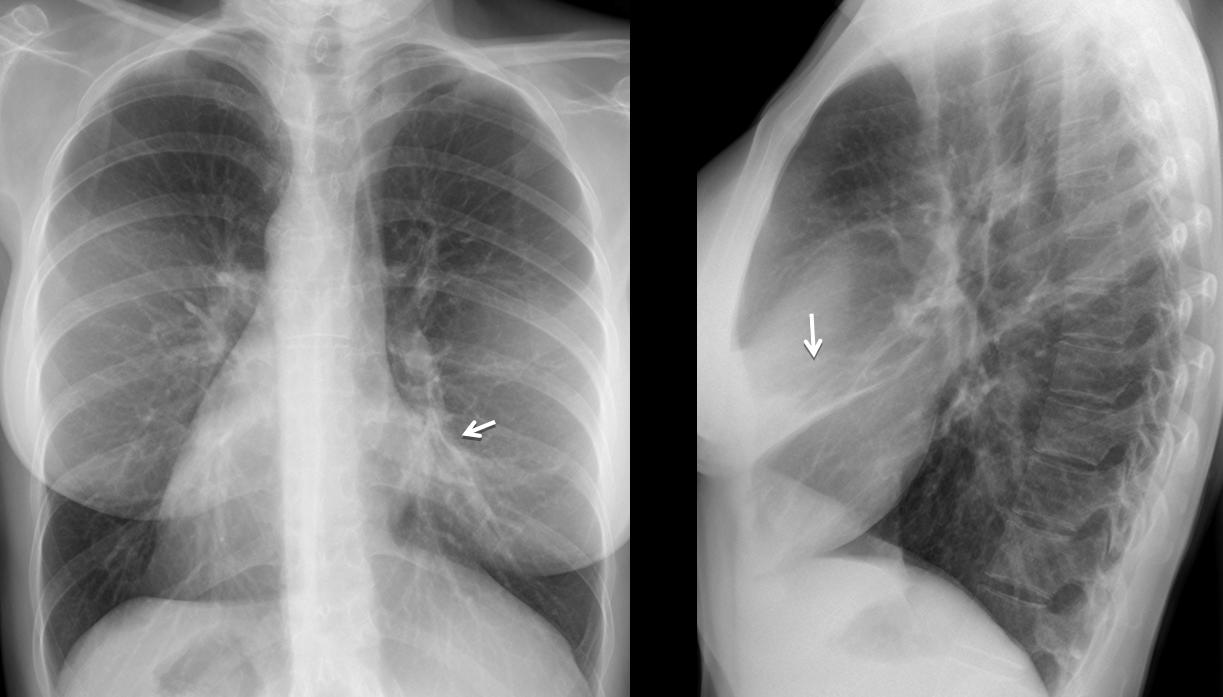
Fig. 3
Fig. 2 (above): 32-year-old woman with situs inversus totalis. PA chest film shows mirror-image dextrocardia. There is chronic disease of the middle lobe (arrows), secondary to bronchiectasis and Kartagener syndrome.
The second most common type of anomalous rotation of the heart is cardiac dextroversion. The rotation of the heart is arrested before completion, and as a consequence, most of the heart silhouette remains in the right hemithorax. Patients are asymptomatic and the incidence of cardiac disease is low. If the patient turns about 20 degrees to the left, the heart silhouette looks normal.
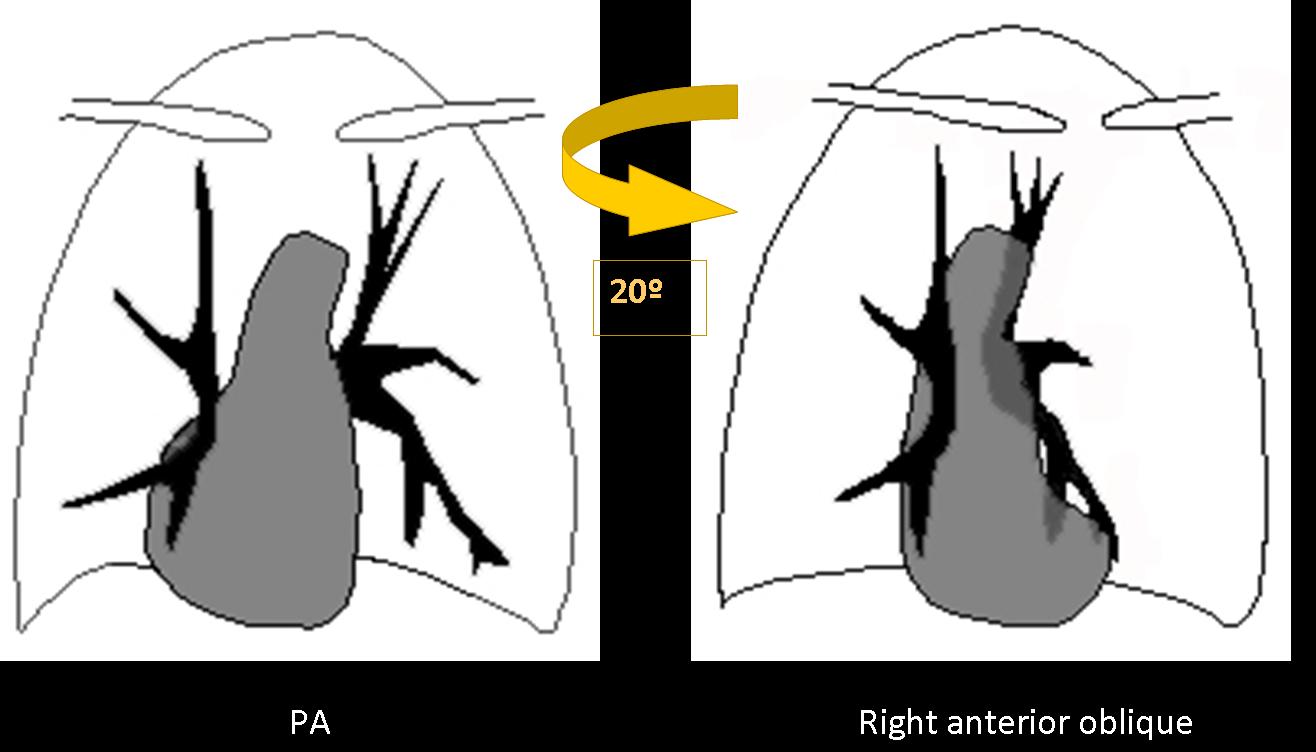
Fig. 4
Diagnosis of uncomplicated dextroversion can be made with reasonable certainty on radiographic evidence of heart in the right hemithorax, aortic knob on the left, normal position of the abdominal viscera, and absence of obvious extracardiac disease to account for the cardiac displacement. Normal EKG and lack of symptoms confirm the diagnosis.
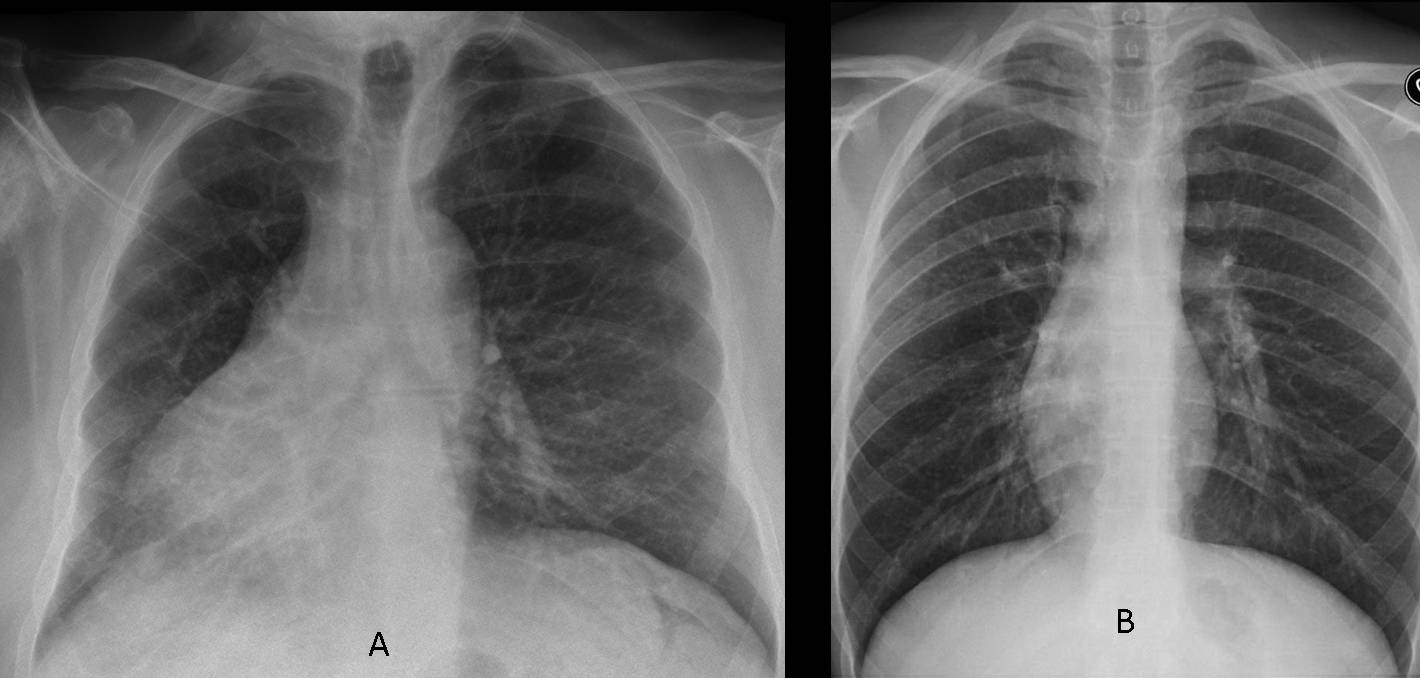
Fig. 5
Fig. 5 (above): the right-sided position of the heart in dextroversion can vary from very obvious (A) to minimal (B). In both cases, unenhanced CT performed for unrelated reasons shows the normal configuration of the cardiac chambers (Fig. 6).
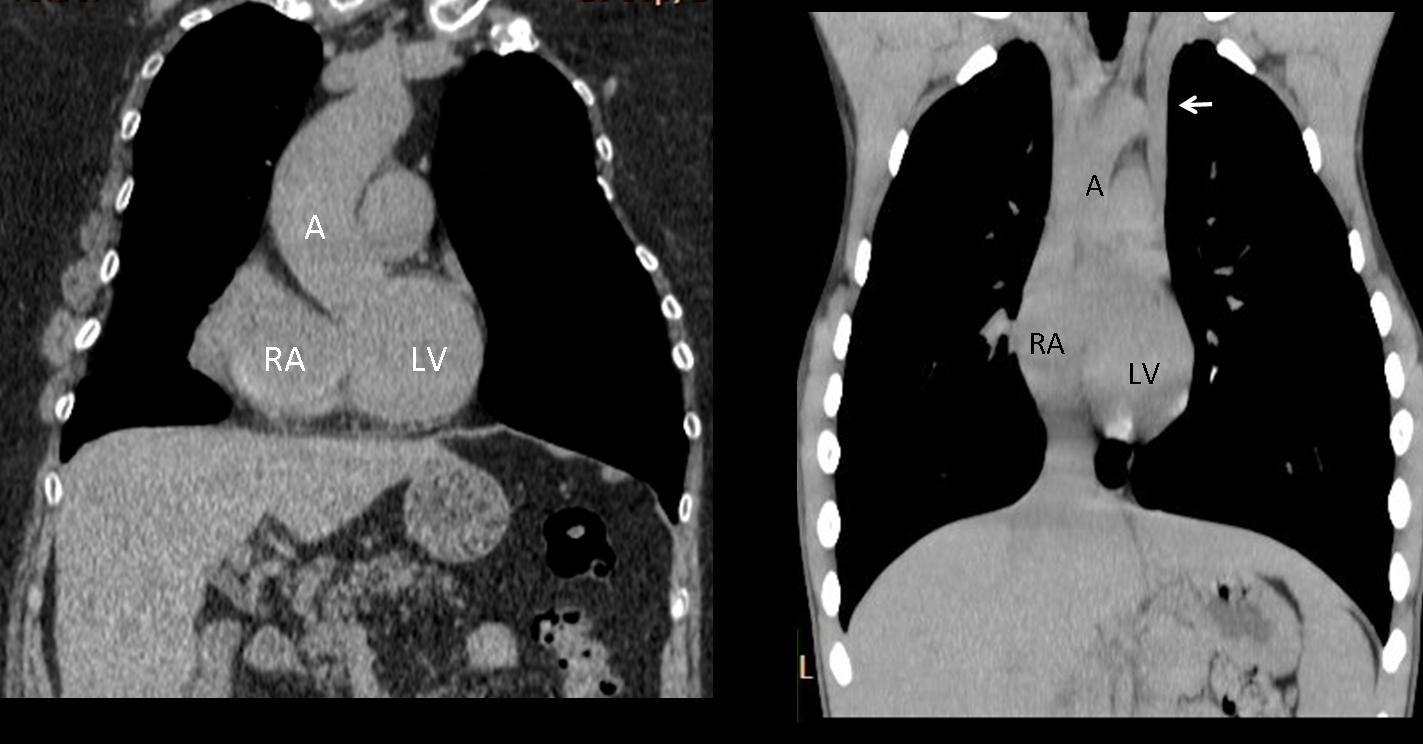
Fig. 6
Fig. 6 (above): unenhanced coronal CT of the previous cases demonstrating normal configuration of the cardiac chambers (A, aorta; RA, right atrium; LV, left ventricle). Note normal location of liver and stomach. A left superior vena cava is visible in B (arrow).
Time for a test. Below you’ll find the PA radiographs of a 27-year-old woman with a moderate cough. What do you think is causing the dextrocardia in this patient?
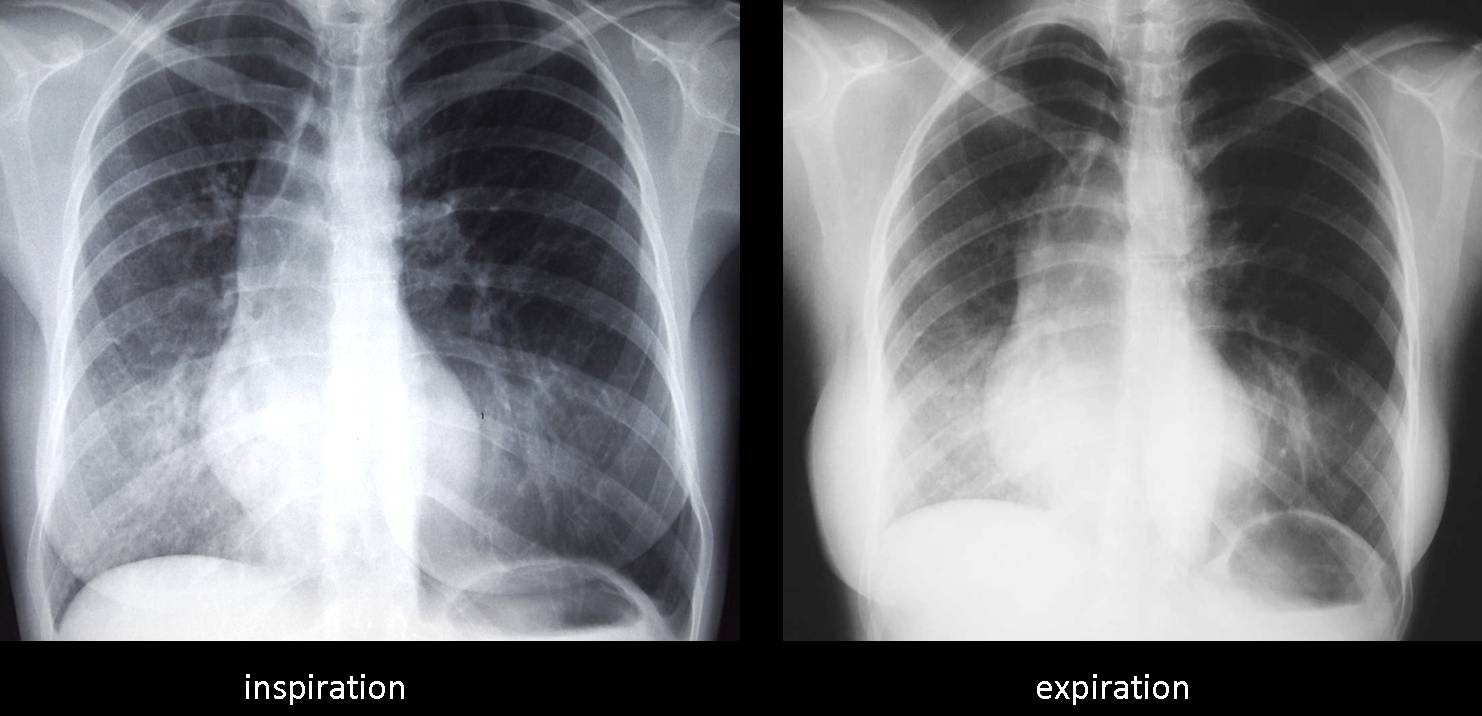
Fig. 7
This case is an example of secondary dextrocardia. In these patients, the heart was originally in its normal location, but it is now visible in the right hemithorax because it has been pushed or pulled towards it. In my experience, secondary dextrocardia is not uncommon and we should look for the coexisting cause rather than be deceived by the position of the heart (Fig. 8).
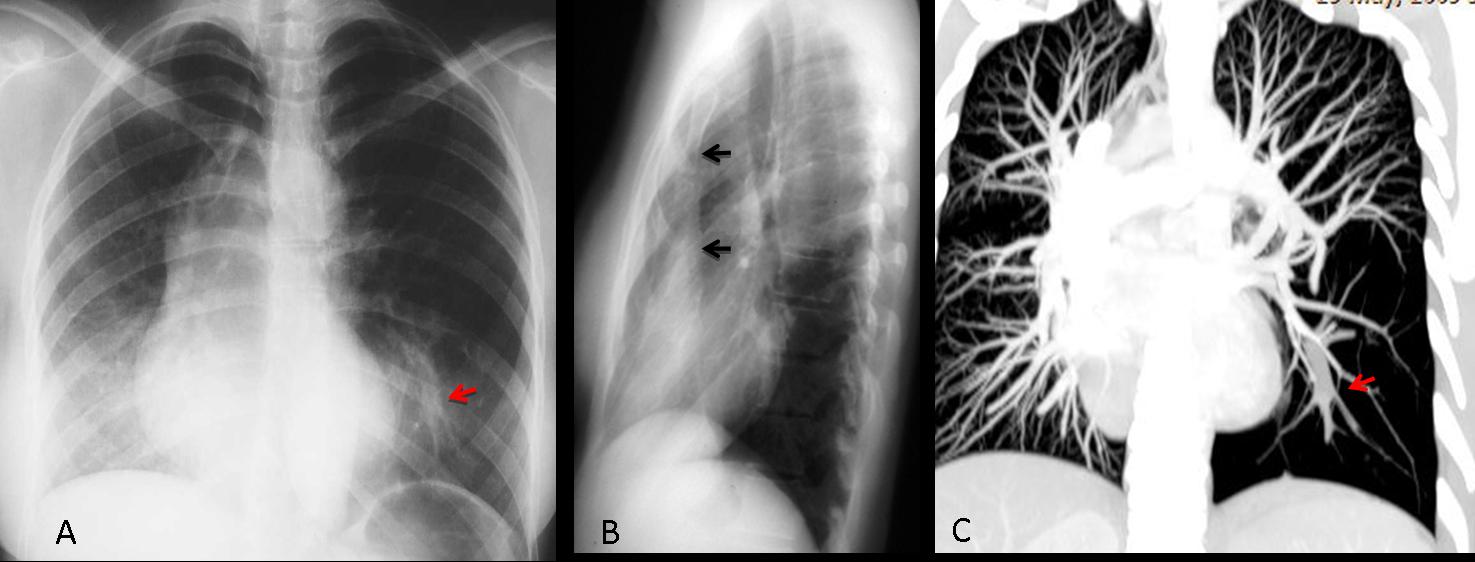
Fig. 8
Fig. 8 (above): the heart is displaced towards the right by a combination of pectus excavatum (B, arrows) and bronchial atresia of LLL, which causes lung overexpansion, pushing the heart towards the right. Note the mucous impaction (A,C, red arrow).
In my experience, secondary dextrocardia is not unusual. The causes include:
Rib cage malformations, mainly scoliosis and rarely, pectus excavatum
Loss of right lung volume, due to previous surgery or hypogenetic lung.
Increased left lung volume, pushing the heart towards the opposite side
Left pleural disease (tension pneumothorax or massive pleural effusion)
Elevation of left hemidiaphragm, displacing the heart towards the right.
Examples of some of these conditions are shown below.
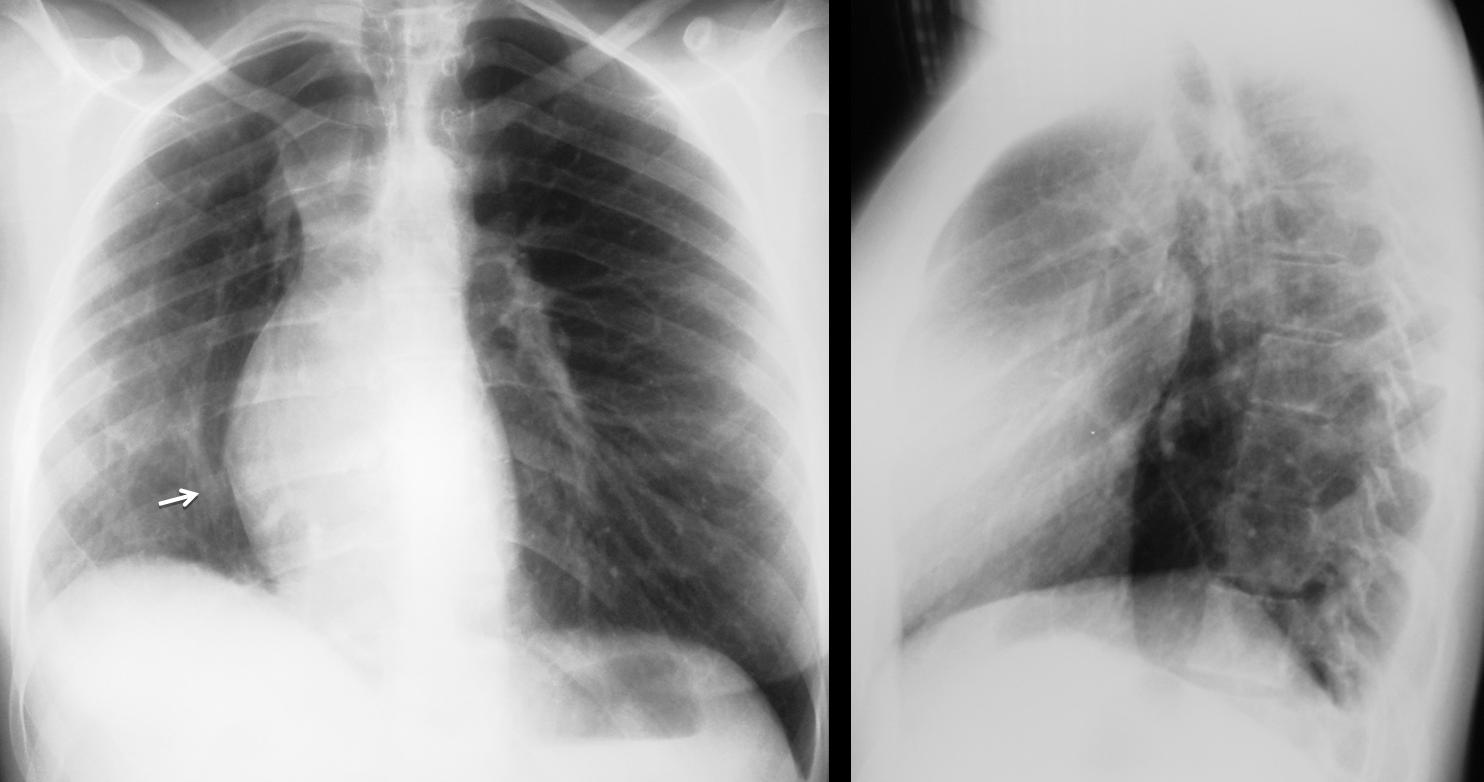
Fig. 9
Fig. 9. Dextrocardia secondary to hypogenetic lung syndrome, a congenital condition in which there is an absence of one or two lobes of the right lung. As a consequence of the volume loss, the heart is drawn towards the right. Note the small hemithorax and the scimitar vein (arrow).
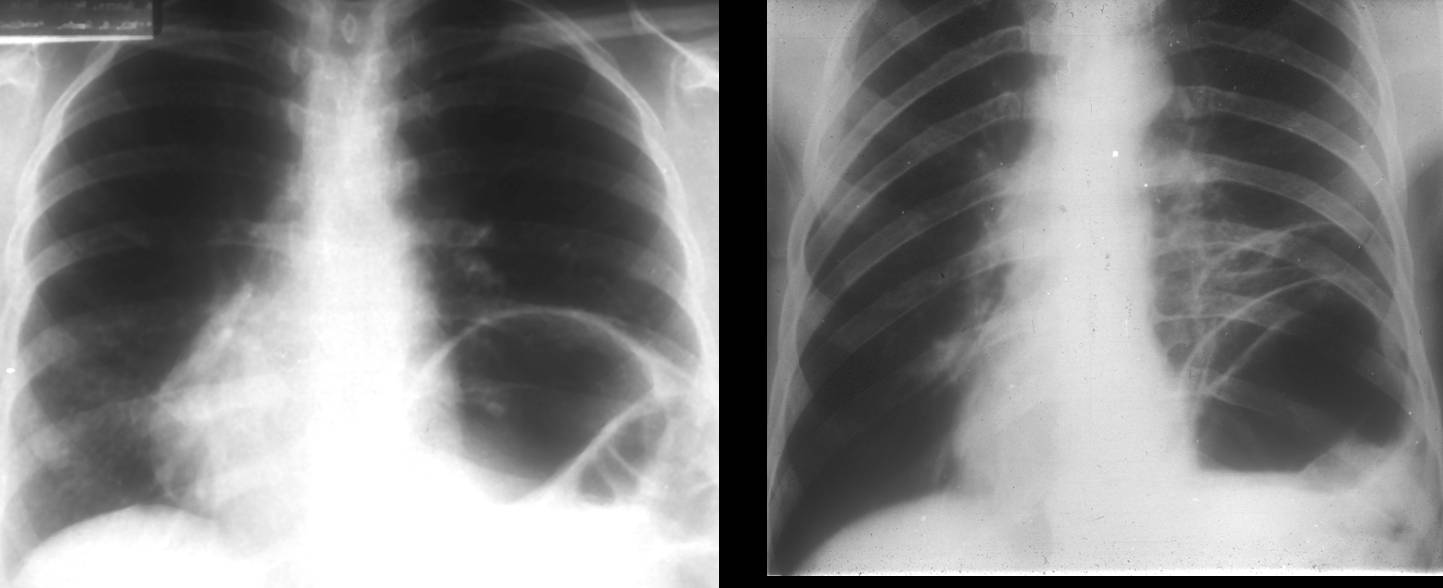
Fig. 10
Fig. 10 (above): two cases of secondary dextrocardia due to elevation of the left hemidiaphragm. Both patients had diaphragmatic paralysis, although eventration and diaphragmatic hernia can produce a similar appearance.
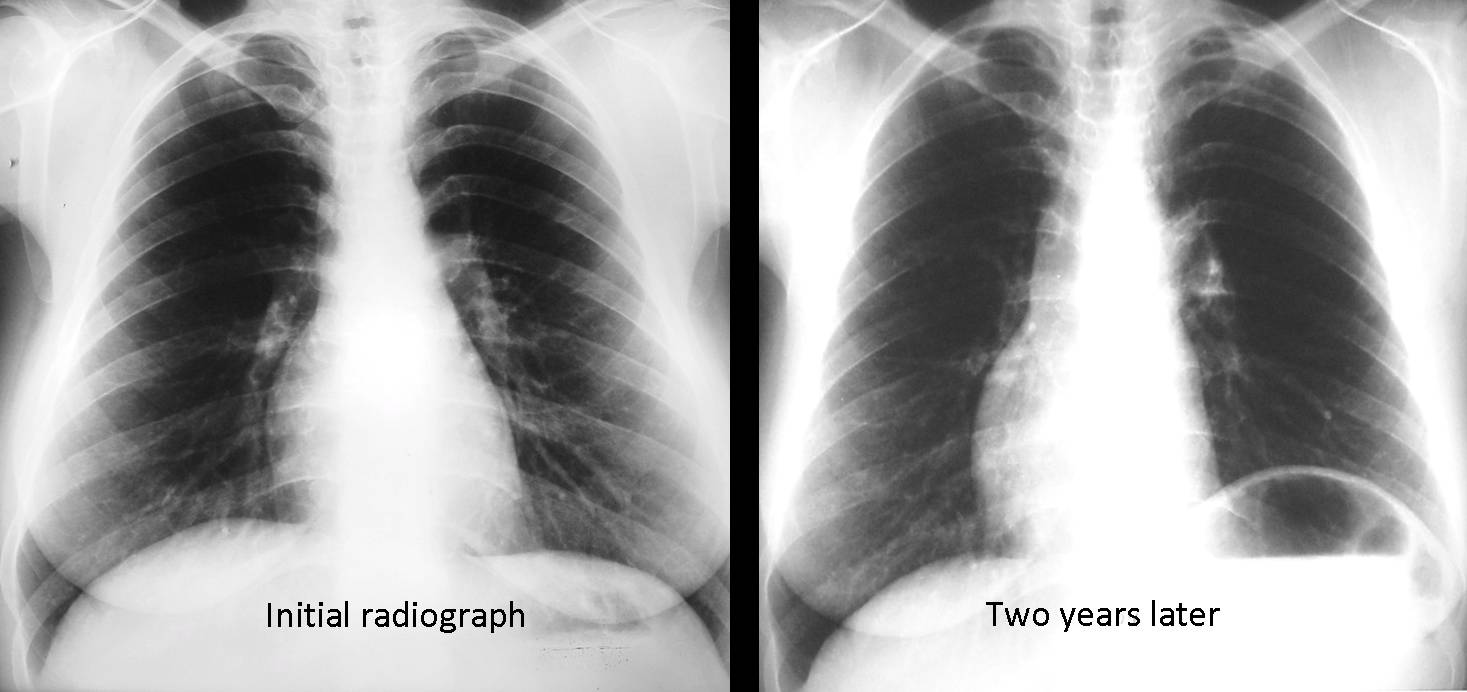
Fig. 11
Fig. 11 (above): illustrative case in which a patient developed phrenic nerve paralysis after radiotherapy for lymphoma. The original film shows the heart in its normal position. Two years later, the heart is displaced to the right due to elevation of the left hemidiaphragm, secondary to the phrenic nerve involvement.
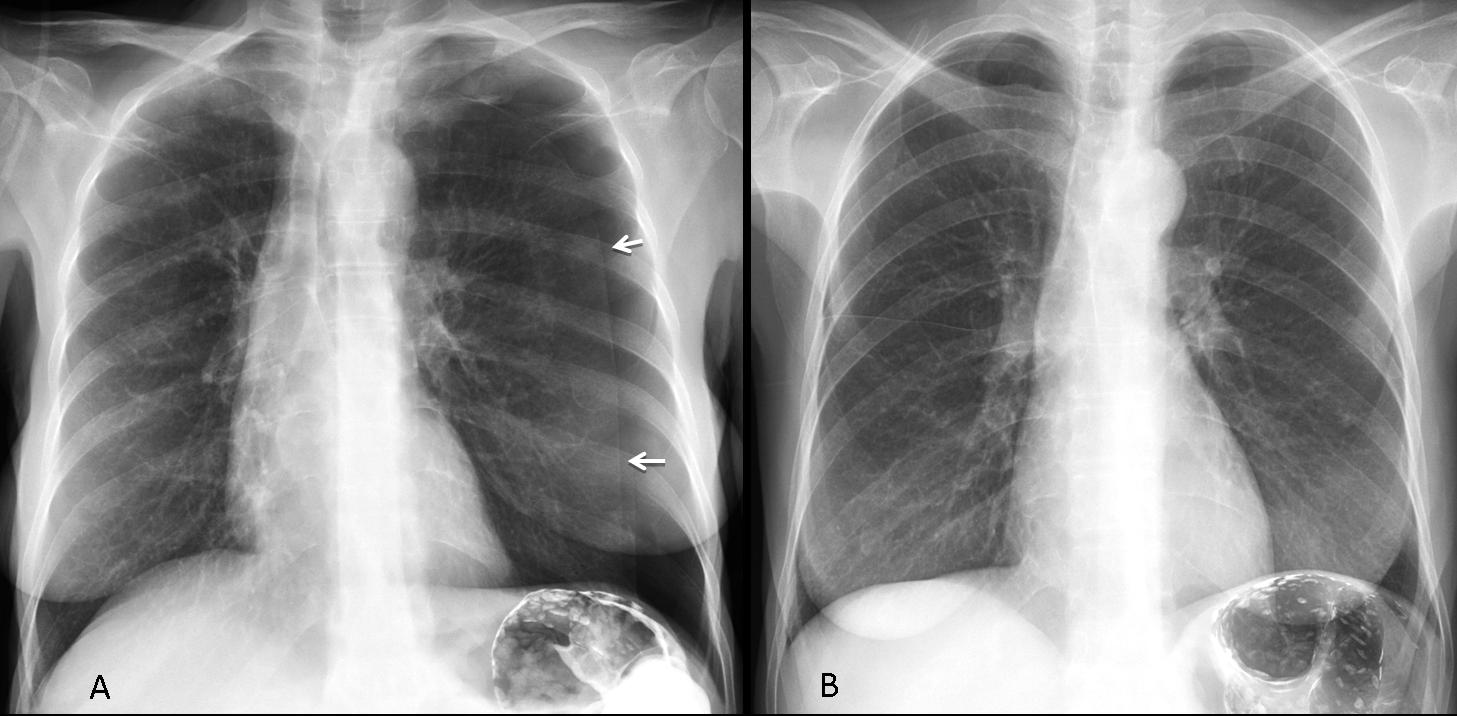
Fig. 12
Fig 12 (above): 57-year-old woman with transient dextrocardia due to left pneumothotax (A, arrows). Three days later (B), after drainage of pneumothorax, the heart has returned to its normal position.

Follow Dr. Pepe’s advice:
Follow Dr. Pepe’s advice:
- Most dextrocardias in adults are innocuous and unrelated to intrinsic heart disease.
- Primary dextrocardia is due to situs inversus totalis or cardiac dextroversion.
- Secondary dextrocardia is due to the heart being displaced by a neighboring pulmonary or pleural condition, or by rib cage malformations.
A detailed description of dextrocardia in adults is beyond the scope of this presentation. You can read the article by P. Maldjian and M. Saric: “Approach to dextrocardia in adults: review” AJR 2007;188:S39-S49


Agenesis or hypoplasia of the right pulmonary artery
ELEVATED R MEDIAL DIAPHRAGM WITH LARGE BAWOL INSIDE complecated with mass effect on heart LOCATED ANTERIOR IN THE LATERAL x ray i suppose morgagni heneria
ELEVATED L MEDIAL DIAPHRAGM WITH LARGE BAWOL INSIDE complecated with mass effect on heart LOCATED ANTERIOR IN THE LATERAL x ray i suppose morgagni heneria
If you cover the cardiac shadow and the equivalent area on the left, vascularization of both lungs is similar. And the right pulmonary artery on the lateral view has a normal size.
destro-posizione cardiaca; area sclerotica ,disomogenea, sul peduncolo vertebrale di D10.
Dextrocardia. Most of the cardiac silouette is located in the right hemithorax. Note the increased radiopacity of the right hemithorax (hyperventilation). Decreased caliber and number of pulmonary vessels of the right lung. Right lung hypoplasia.
Hypoplasia of right pulmonary artery? Is the pulmonary artery truk nirmal? The right pulmonary artery normal?
Dextrocardia. Most of the cardiac silouette is located in the right hemithorax. Note the increased radiopacity of the right hemithorax (hyperventilation). Decreased caliber and number of pulmonary vessels of the right lung. Right lung hypoplasia.
Hypoplasia of right pulmonary artery? Is the pulmonary artery truk normal? The right pulmonary artery normal?
Whet do you think of the right pulmonary artery in the lateral view?
I agree.
Do you agree with me or with Maria?
It looks like prominence of the right cardiac border, ( right atrial enlargement ) but i think is not
-The pulmonary artery is normal
-all mediastinum is shifting to the right exept descending aorta.
-these elevation of right frontal hemidiaphragm could be the key.
i am working on it…
sorry my right is left 🙂
sub diaphragmatic mass?
I think it is a focal pericardial defect
Focal pericardial defects have a normal position of the heart with prominent left atrial appendage. Try again 😉
I see that the shape of the cardiac shadow in the lateral view is abnormal as the posterior border became strait and the cardiac shadow looks like a (( Bell ))
so, I think about that the aorto-pulmonary window is obliterated
…carissimo collega, io avevo parlato appunto di dx-posizione e non di dx-cardia, intendendo così la normale posizione delle camere cardiache e dell’arco aortico:cuore “spostato” a dx.
I know you did and you deserve the credit. You were so early that I didn’t want to spoil the diagnosis for all the others.
Again, congratulations!