Muppet and I are very happy to have reached one hundred cases. We hope you enjoyed them as much as we did. Radiographs of this case belong to a 52-year-old man with vague chest complaints. He was operated on for testicular tumour fifteen years earlier.
Check the images below, leave your thoughts and diagnosis in the comments section, and come back on Friday to find out the answer.
1. Duplication cyst
2. Lymphangioma
3. Metastasis from testicular tumour
4. None of the above
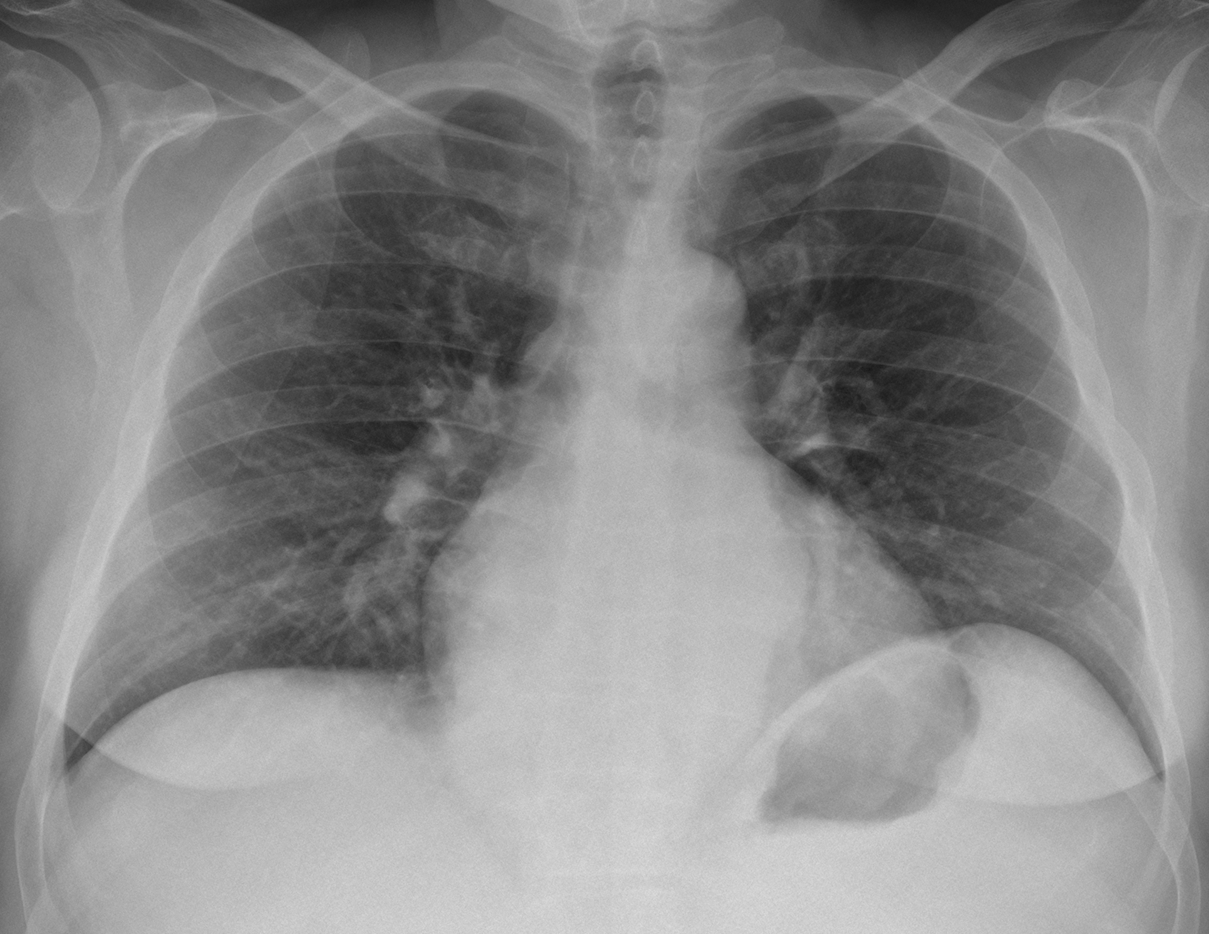
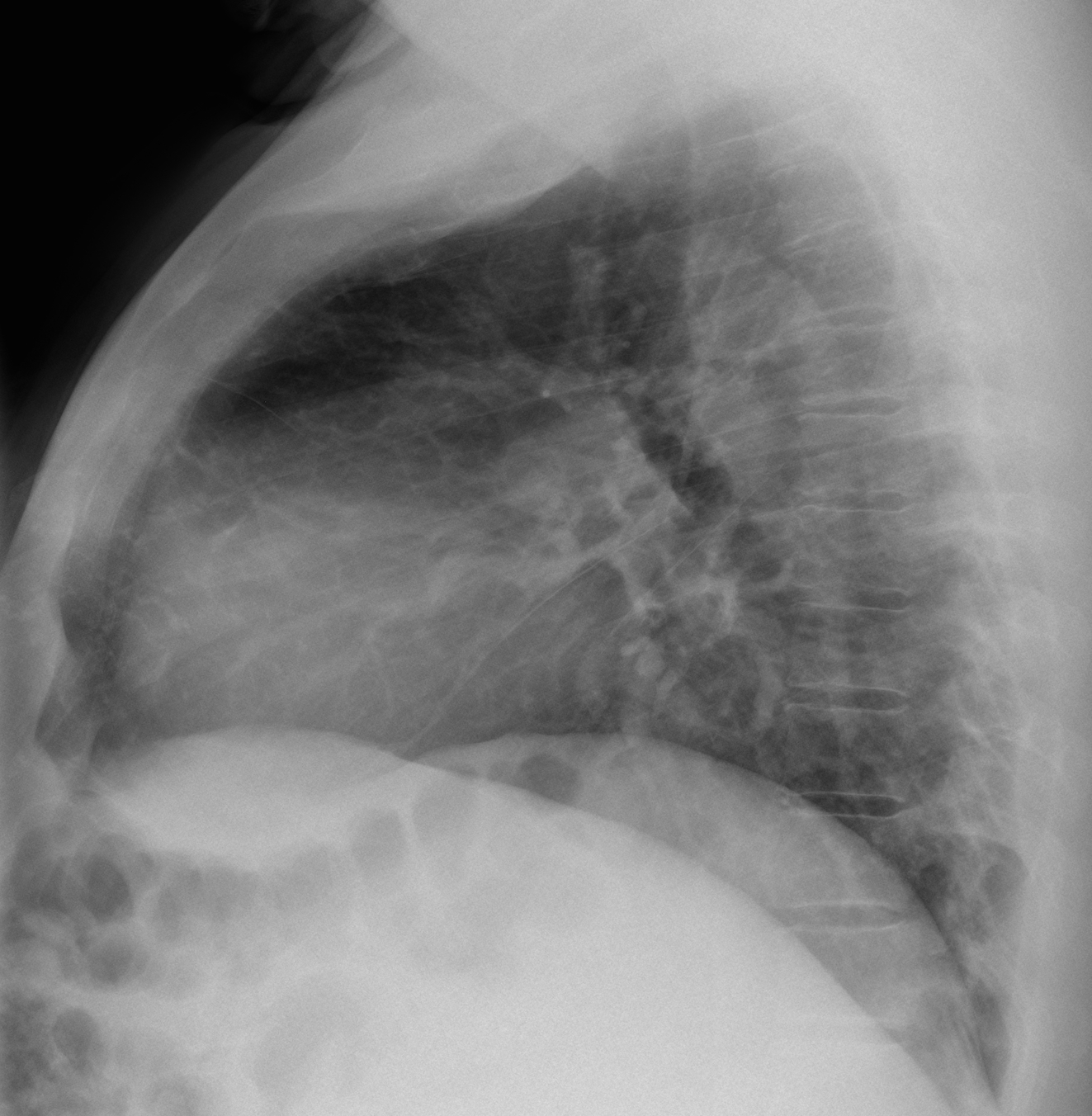
Findings: PA radiograph shows widening of lower mediastinal lines, which are slightly undulated (A, arrows). There is increased density in the left upper quadrant of the abdomen and the lateral wall of the stomach is indented, suggesting splenomegaly. On the lateral view there is increased opacity of the middle lower mediastinum, with a suggestion of tubular structures (B, arrows).
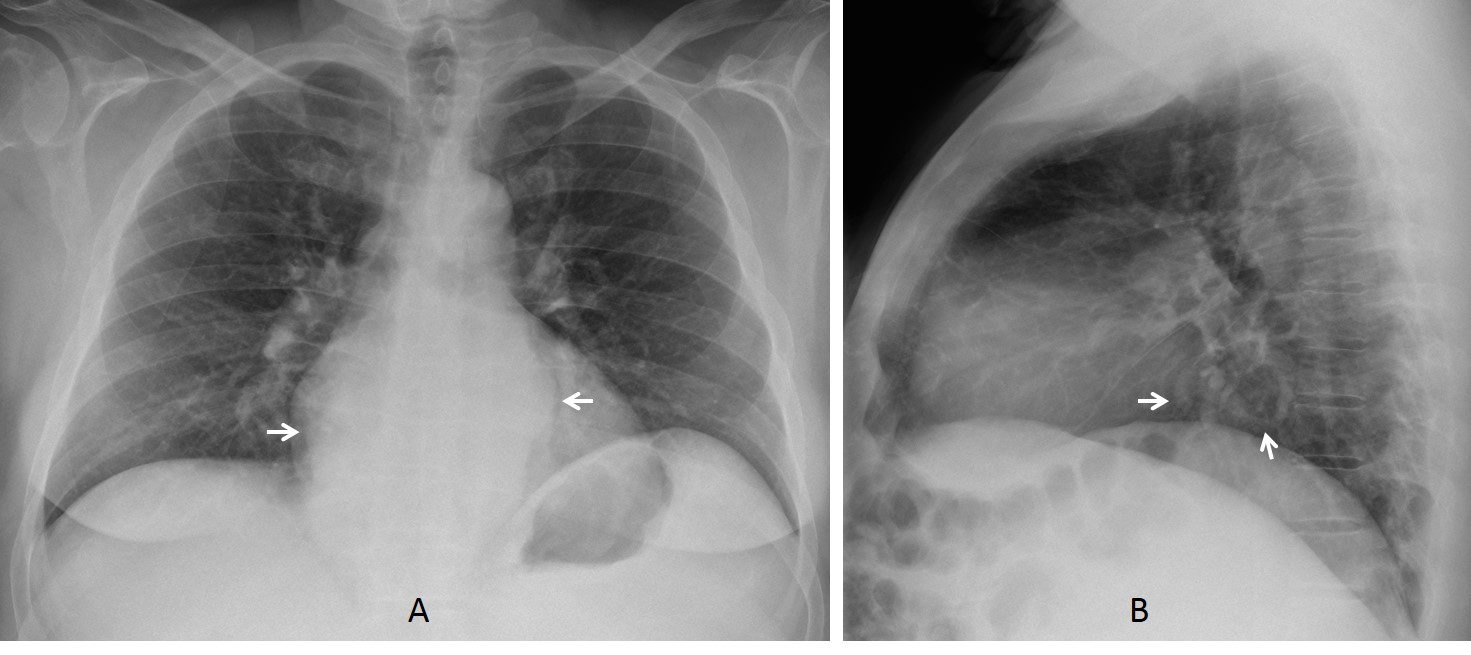
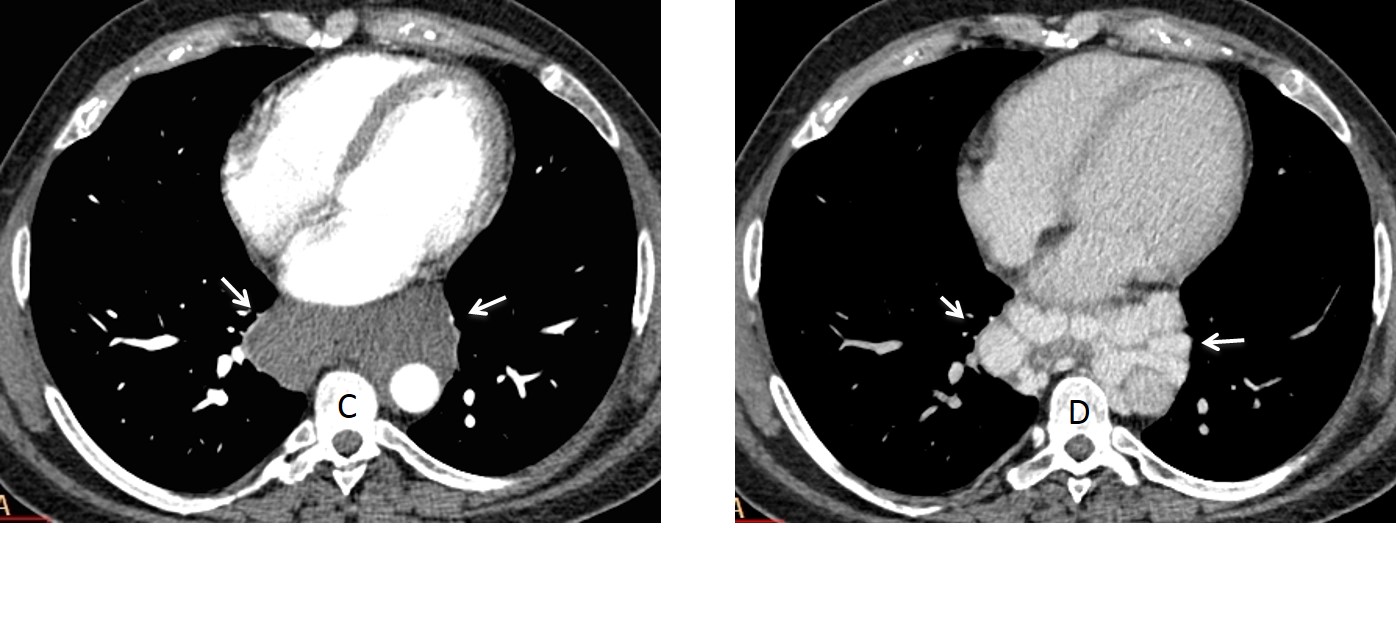
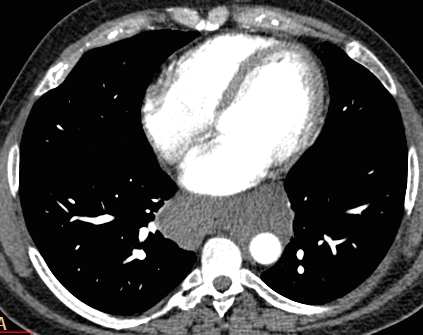
Enhanced axial CT (arterial phase) shows a non-enhancing mass in the middle mediastinum (C, arrows). Venous phase shows multiple enhancing veins within the mass (D, arrows).
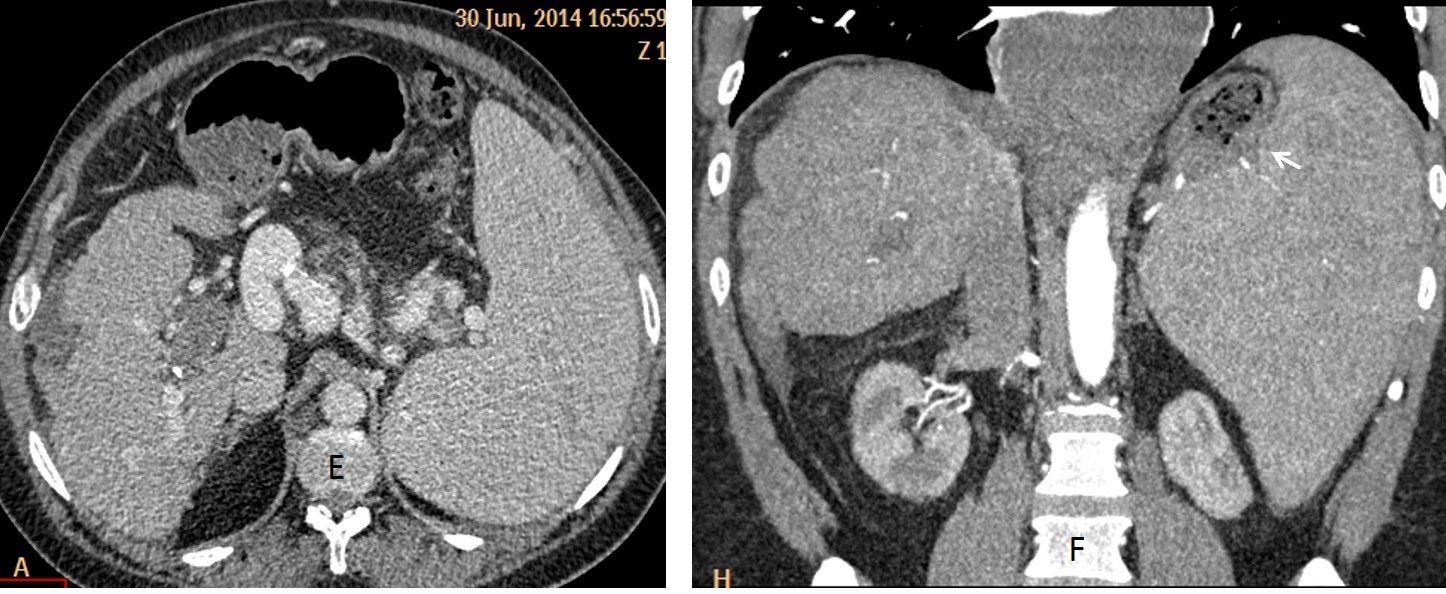
Axial and coronal CT (E, F) show marked liver irregularity and splenomegaly. Note how the enlarged spleen impinges on the stomach (F, arrow).
Final diagnosis: paraesophageal varices secondary to liver cirrhosis
I am showing this case as a reminder that vascular structures should always be considered when facing a mediastinal mass. A similar case was presented three years ago (Case #8). The same teaching point applies today.
Teaching point: the mediastinum is composed mainly of vascular structures. When a mediastinal abnormality is present, always rule out a vascular origin (arterial or venous).


1. Duplication cyst
Posterior mediastinal mass surrounding the esophagus with fluid like attenuation.
Option number 4
Do you have any ideas?
It could be mediastinal and retroperitoneal fibrosis caused by the previous malignancy or its treatment.
Metastasis from testicular tumor
This seems like too easy an answer (though maybe you’re messing with us because it’s case 100…), but a subcarinal, well circumscribed, homogenous, non-enhancing, mass-occupying lesion looks like a duplication cyst to me. History of testicular tumor is unrelated.
Incidentally, does he also seem to have pretty minimal thoracic curvature of the spine? (i.e. more straight than normal)
Regarding your comments. 1 Spine is OK; 2. Muppet is an evil character and likes to mess with everybody. And case 100 should be especial, don’t you think?
Growing teratoma syndrome
Interesting answer. Keep thinking.
IT IS INTERESTING CONSIDERATION EXCEPT FOR FOLLOWING POINTS-:
1. THE GROWING TERATOMA SYNDROME USUALLY IS SEEN IN RETROPERITNEUM.
2. IT USUALLY IS CYSTIC BUT SHOULD HACE FEATURE SIMILAR TO MATURE TERATOMA AS IT CONSIST FO ALL THREE LAYERS.
Let’s shoot with benign esophageal wall tumor
If the patient was younger I would consider lymphatic malformation…
The mass seen on ct looks “soft” so should’nt We rule out malignancy? Does it continue from subcarinal area- meaning it can originate from medial mediastinum…
I think I can see a small bubble of air in the center of mass on ct suggesting it originates from oesophagus…
Did You perform upper GI with oral contrast?
Maybe achalasia should be considered with uniform fluid like content
Esophageal duplication cyst
Bronchogenic cyst
Cystic sequestation in uncommon location?
Sorry, I liked your first diagnosis better. Look at the lateral chest
Estimado profesor:
Pienso que se trata de un quiste de duplicacion, aunque conociendo sus casos no creo que sea tan facil. La otra posibilidad es el Sindrome del Teratoma creciente que se produce despues de la terapia de un tumor no seminomatoso.
Gracias por sus estupendos casos
Hay otras posibilidades. Revisa el caso #41 del Dr Pepe
On the lateral view i think there is at least two masses one subcarinal and one in posterior mediastinum that we can see on CT.that makes the possibility of bronchogenic cyst or esophageal duplication cyst unusual.
it looks like benign mass, i think is not involvement of the heart , aorta or the spine.
i can’t see dilatation of esophagus. the mass just displace the heart infront and the main bronchus posterior.
can you tell us professor the mass HU?
23 HU. See my comment below
I will give you all a hint: review Dr. Pepe’s Diploma case 41, which gives basic advice about mediastinal masses
….la “densità” della massa è sovrapponibile a quella dei muscoli della parete toracica e non prende C.E. …essa è localizzata nella doccia vertebrale e non ha caratteri “aggressivi” perchè l’aorta è regolarmente rappresentata ed opacizzata….in LL del torace sembrerebbe vedere delle bozzature retrosternali, senza che il Professore ci faccia vedere il piano di scansione TC a tale livello!….si esclude pertanto la natura “liquida” della stessa: linfangiomi e cisti da duplicazione bronco-enteriche…..metastasi dopo 15 anni?Improbabile …..la sindrome da teratoma crescente è suggestiva , ma perchè anch’essa dopo 15 anni ? Poiche’ penso sempre “controcorrente”, perchè non pensare anche a focolai di eritropoiesi extramidollari ?Cosa ci dice la PET-TC?
Good diagnosis, but not the right one. Go to Diploma case #41 to get inspiration.
PET-CT was not done
….ho preso visione del caso 41( dove avevo fatto una diagnosi corretta) ed allora penso a grasso mediastinico in sede posteriore….
Oesophageal diverticulum
Lymphoma.
ok professor the mass is 1 cm infront of the
anterior edge of the vertebral body on the lateral view that means is on middle mediastinum ?
23 HU is not cystic could be solid but no fat.
Hiatal hernia with material???
…il soggetto “maschile” ha un seno ben sviluppato( ginecomastia)…a ciò si aggiunge un pregresso tumore testicolare….se il suo cariotipo ha qualcosa in “piu'( x sovrannumerario), si configura una S. di Klinefelter( il rischio di tumore testicolare è alto)….in più c’è il rischio di tumori a c. germinali del mediastino e/ o linfomi , come appunto in questa Sindrome….vado ancora controcorrente ?
Congratulations Dr Caceres for these 100 so beautiful cases and also please give thank’s on behalf of me to the mupet for his help.Nothing would’ve been the same without him. I was just helping my housband in the garden when I thought the 100th case must be on line and it is. Then I take a look and decided better to do gardering … But as this 100 case is like a birthday I wouldn’t lose this chance of participating. By the way you are invited to see our garden and take a cup of tea or coffe a beer or some vine…
Regarding your leson about extrapulmonary/intrapulmonary I remeber when I was pregnant from one of my children and you gave me book with an inscription about this feature. The aorta seems to be intrapulmonary in relation to the lesion. So could the lesion could be a vascular lesion like a big mural haematoma or a thrombosed aneurysm. However the shape of the aorta is not that these kind of lesions usually have and the symptoms woudn’t be so average in case of an acute aortic haematoma. I agree with pH about a lymphoma a mass that can encase the aorta and can have this appearance, hypodense and can be found in inmunodepressed patients like this could be. Anyway the important think is participate not win as it seems it’s going to happen with some football teams this year.
Wow! that was a long disertation! Thanks for the invitation and for you nice words.
Regarding the football team I image you are referring to Real Madrid.
You came close to the diagnosis. Answer tomorrow.
IN A OPERATED PATIENT, A FLUID ATTENUATION LESION WITH NO TO IMPERCEPTABLE WALL- WE COULD THINK LYMHANGIOMA AS A CONSIDERATION. THE LACK OF SOLID COMPONENT OR THICK WALL ARGUES AGAINST BOTH METS AND ESOPHEGAL DUPLICATION CYST. VASCULAS MASSES ARE EQUALLY UNLIKELY.
LYMHANGIOMA LOOKS LIKE THE BEST GUESS!
Yor reasoning is sound. See the answer today.
….il Bari , anche se di “serie B”, non ci sta a perdere con il Barca !!!!…Simpaticissimo professore, dovevi farci vedere tutti i piani di scansioni, anche quelli più caudali…..inoltre come sospettare una Ipertensione portale se la vena Azygos non è dilata nell’Rx torace standard ?Ancora chi ha fatto l’esame conosceva la condizione clinica del paziente….Quello che ti “salva” è la ginecomastia che si ha nelle epatopatie terminali e che doveva farci capire da che cosa era determinata.. Con stima …ti seguo anche in spagnolo !!!!!
I sort of agree with you, but giving too much information takes away all the diagnostic fun. Also, I had shown a similar case three years ago. And remember the final advice from Dr. Pepe in Case 41:”The great imitators are vascular structures, mediastinal fat, and esophageal disease”
And, who wants to see easy cases…?
Satanic muppet hihihi!!!!!! 🙂
And you ain’t seen nothing yet!
Great case!! I’m a new fan, hoping to follow your cases….and giving answers. Thanks a lot!
Wow, I think that was the hardest case yet. I’m annoyed at myself for wondering about the gynecomastia on the PA, but assuming it was unrelated.
Buenos dias
Creo que son varices esofágicas, en un paciente con hepatopatía crónica, hipertensión portal y trombosis portal.
Un saludo
Diagnóstico correcto; pero demasiado tarde. Tendrás una nueva oportunidad con el caso 101.
GOOD JOB
Thank you