Dr. Pepe has eloped to the Bahamas with Miss Piggy and forgot to prepare the Diploma case. Hope he returns happy and suntanned. In the meantime I will show images of a 57-year-old woman with acute chest pain and mild fever. Check the images below, leave your thoughts and diagnosis in the comments section and come back on Friday for the answer.
1. Pneumonia
2. Pulmonary infarct
3. Pleural fluid
4. None of the above
Findings: PA radiograph shows a triangular pulmonary opacity at the right costophrenic angle (A, arrow), with the characteristic appearance of a Hampton hump, suggesting a pulmonary infarct. In addition, a round nodule is visible in the lower aspect of the right hilum (A,B red arrows).
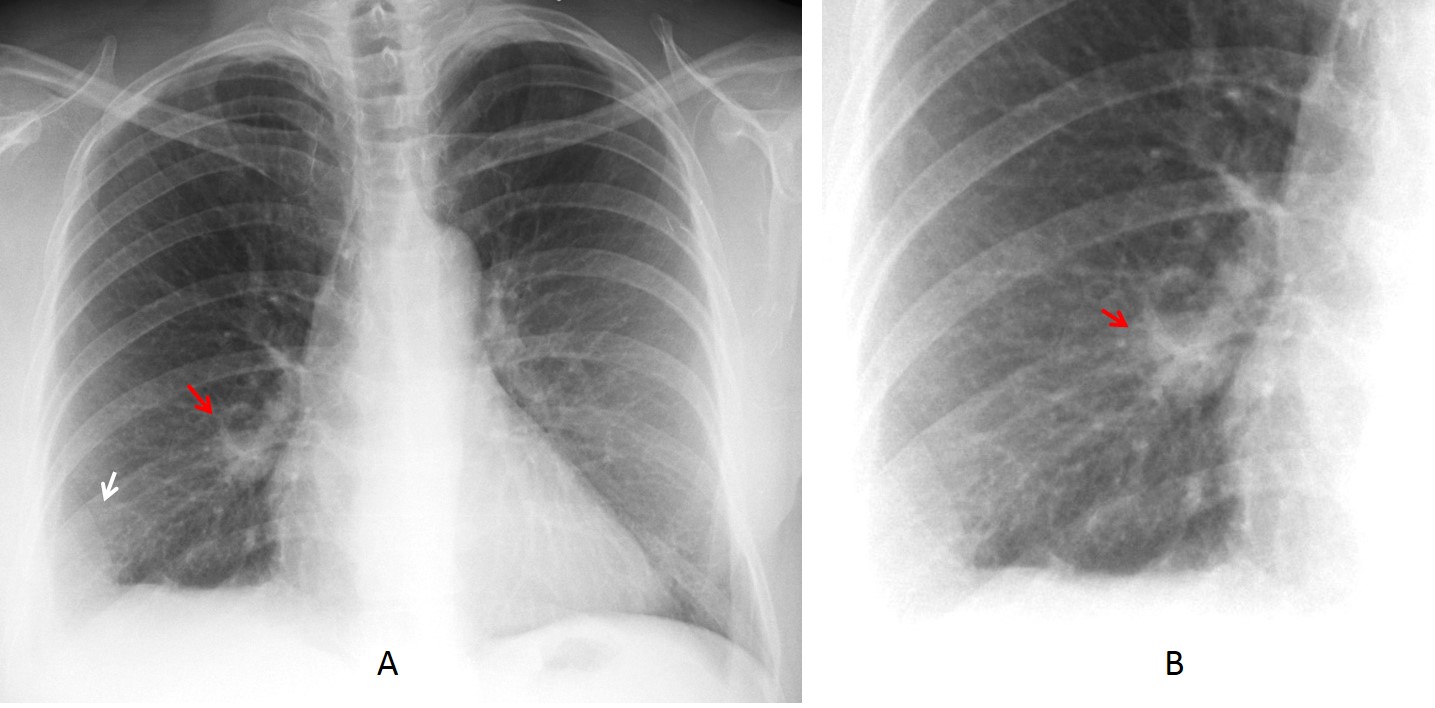
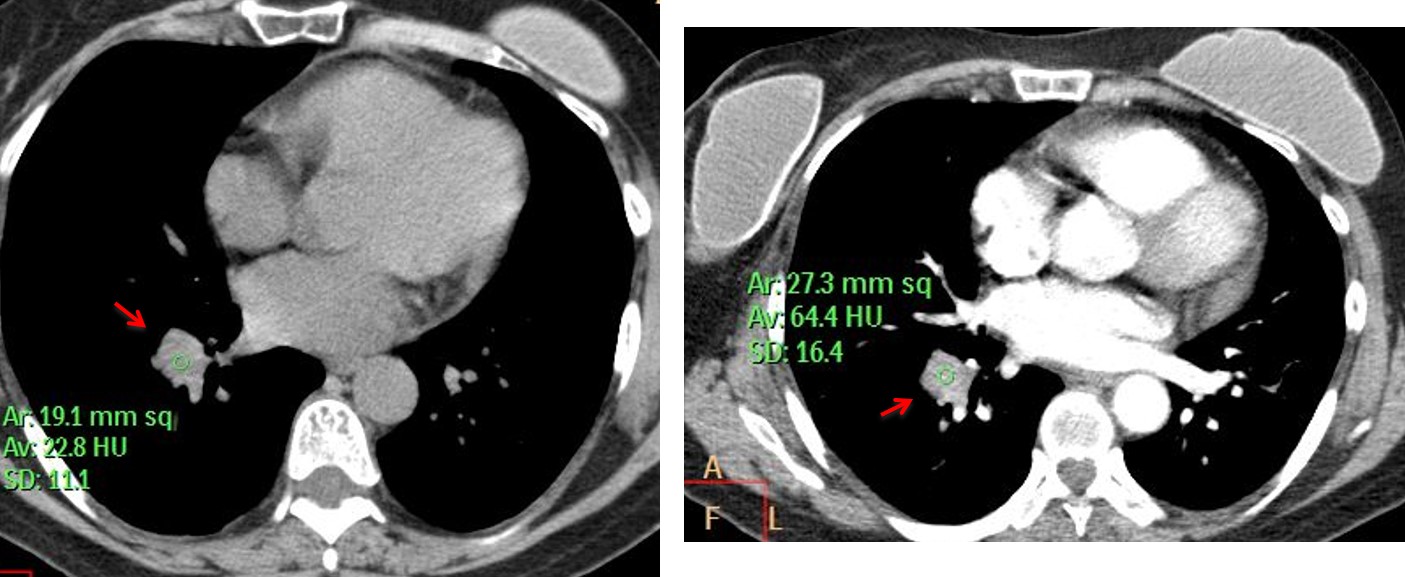
CT confirmed the pulmonary embolism and a RLL mass (C,D arrows) that enhanced 42 H.U. after contrast injection, suggesting malignancy. Needle biopsy confirmed a lung adenocarcinoma.
Final diagnosis: Carcinoma of the lung with pulmonary infarct.
Congratulations to Dr. Prasanna Kulkarni who made the correct diagnosis
Teaching point: remember avoiding satisfaction of search. In this case, it discovered an unsuspected malignancy, which is known to increase the risk of pulmonary embolism.




2. Pulmonary infarct – Hampton hump in right lower lobe.
Second guess – pulmonary sequestration (do I see a feeding vessel in lateral view?)
Think that the infarct is too obvious?
Now that you ask, I have doubts.
And I noticed surgical clips in left axillary region (breast cancer?) that I have missed before, so I stay with first answer – pulmonary infarct.
…evidente amputazione della arteria polmonare dx, con rarefazione del disegno vascolare ed aumento della trasparenza polmonare( vedi il confronto con il lato sx) ..versamento pleurico nello sfondato costo vertebrale posteriore…..D-dimeri. aumentati……tromboembolismo polmonare….buone vacanze!!!!!!
Are you going on vacation again? Congratulations
None of the above. Assymetric lucency of the right lung with ?absent breast shadow. Slightly thickened bronchovascular markings in the right lung as well with interstitial prominence. Mastectomy for breast cancer with lymphangiitis carcinomatosa?
I think Answer is c Plural Fluid Likly encysted
d, none of the above
Axillary surgical clips, with mastectomy, Coarse interstitial markings with septal lines in the left lung- lymphangitis carcinamatosa. Right costophrenic angle – mass like with medial convexity- could represent pleural metastasis from breast carcinoma- but atypical.
Pleural metastases from previous breast cancer.
PA view : mastectomy on the left(surgical clips in axilla and triangular shape of mastectomy in outer border of hemithorax). Although, the right lower lung zone is more lucent than the left one. In addition to the right hilum being lower than normal, i would suspect loss of volume of the right lower lobe.
But in the lateral view the right interlobar fissures seem to be ok.
So, probably the lucency on the right is due to thromboembolism of right pulmonary artery and the opacity in the right costophrenic angle represents associated pulmonary infarct.
The line running craniocaudally in the outer lower part of the right lung in PA view is due to pleural fluid? or is a dermal fissure?
-right pleural based triangular opacity with the apex pointing towards the lung hilum -Hampton’s hump- obstructed pulmonary arteries cause a wedge-shaped infarction, whereas the bronchial arterial circulation is preserved.
-a darkened area distal to the area of embolism that is produced by dilation of the proximal arteries in conjunction with collapse of distal vasculature – Westermark’s sign.
– raised right hemidiaphragm
– enlargement of the ipsilateral pulmonary artery – Fleicher’s sign.
PA view –
inhomogeneous haziness in the right lower zone peripherally, obscuring the right lateral costophrenic angle and lateral aspect of the right hemidiaphragm.
A sharply marginated vertical line in the periphery of the right lower zone paralleling the chest wall and another medailly convex line in the right lower zone – these are likely to represent the displaced major fissure.
A subtle opacity projecting over the inferior aspect of the right hilum, likely to be an endobronchial mass.
Nonvisualization of the right breast outline with resultant hyperlucency in the right lower zone.
Surgical clips in left axilla indicating left axillary exploration.
brocnhovascular prominence in the left lower lobe with Kerley-B lines – lymphangitis carcinomatosis
Lateral View –
Tenting of the right hemidiaphragm, nonvisualization of the anterior third of the right hemidiaphragm and posterior dispalcement of the major fissure – al of them indicating partial collapse in right lower lobe.
Probable diagnosis –
Endobronchial metastasis from Ca breast causing partial collapse of the right lower lobe.
Also depressed right hilum on the PA view